

Categorizing Acute Respiratory Distress Syndrome with Different Severities by Oxygen Saturation Index

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Enrollment
2.2. Data Collection
2.3. Derivation of OI, OSI and Other Indices
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients with ARDS
3.2. Correlation between OI and OSI
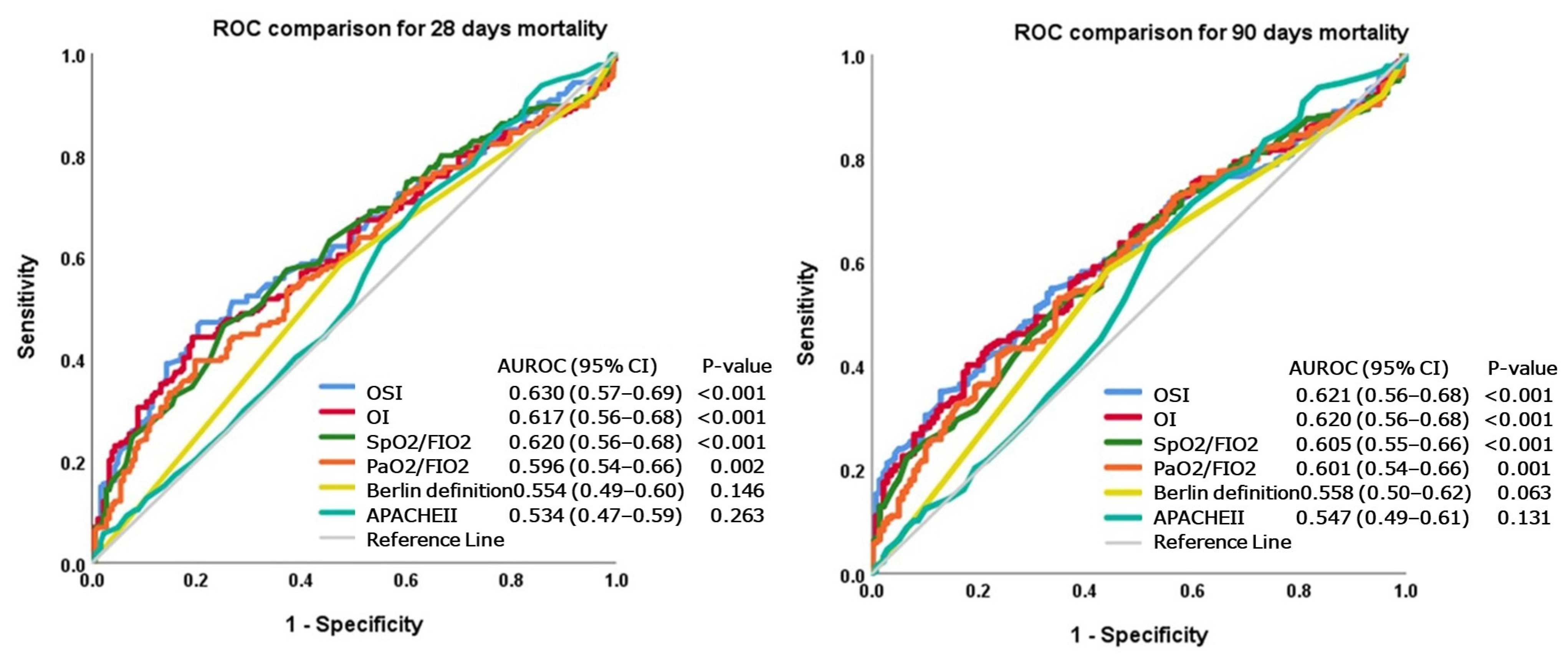
3.3. Comparison of ROC Curves of Commonly Used Indices in the Prediction of Mortality
3.4. Using the OI or OSI Category to Diagnose PaO2/FIO2 Less Than 200 or 100
3.5. Using the OI and OSI Values to Categorize ARDS with Different Severities
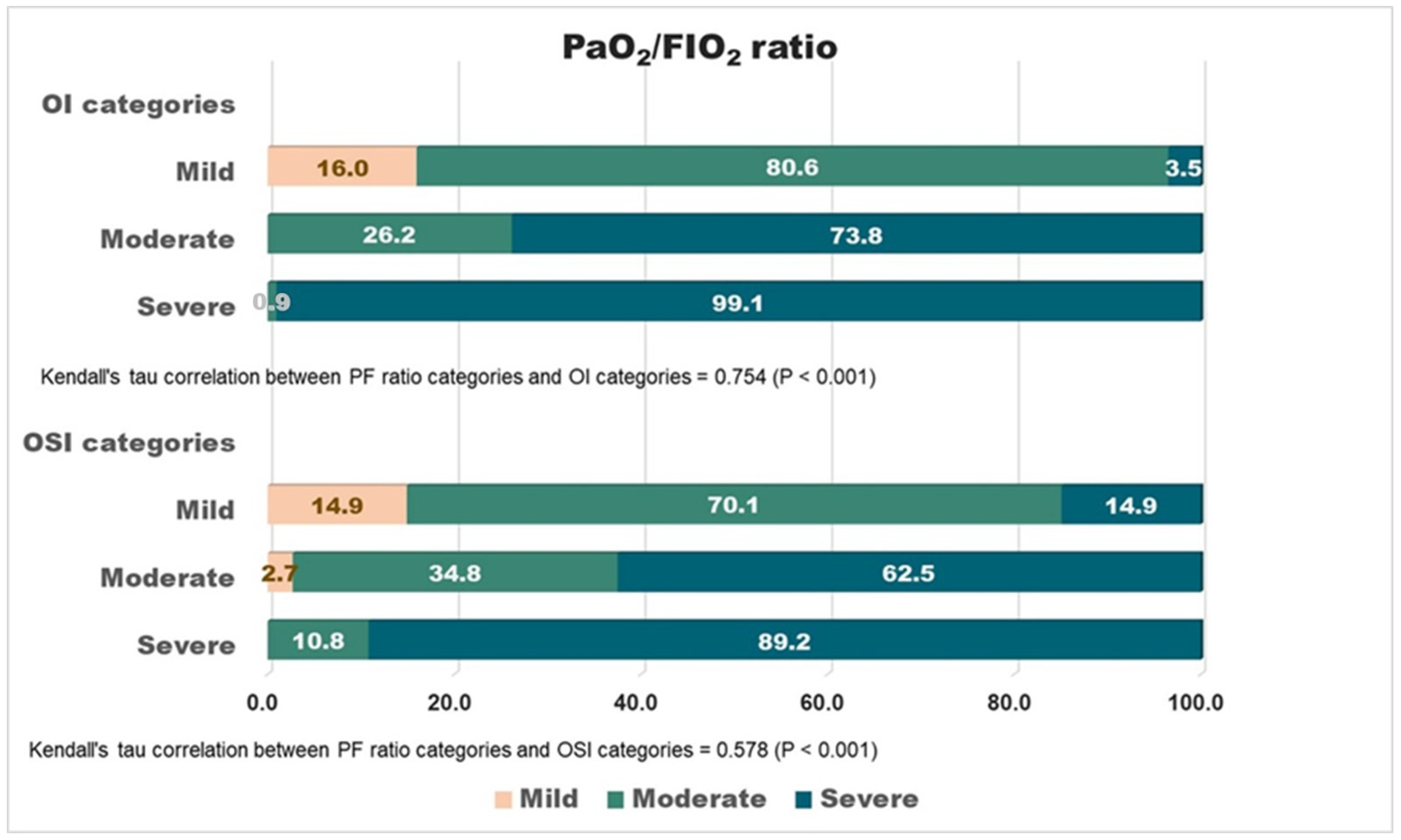
3.6. Correlations between OI/OSI-Based and PaO2/FIO2-Based (Berlin Definition) Categorization
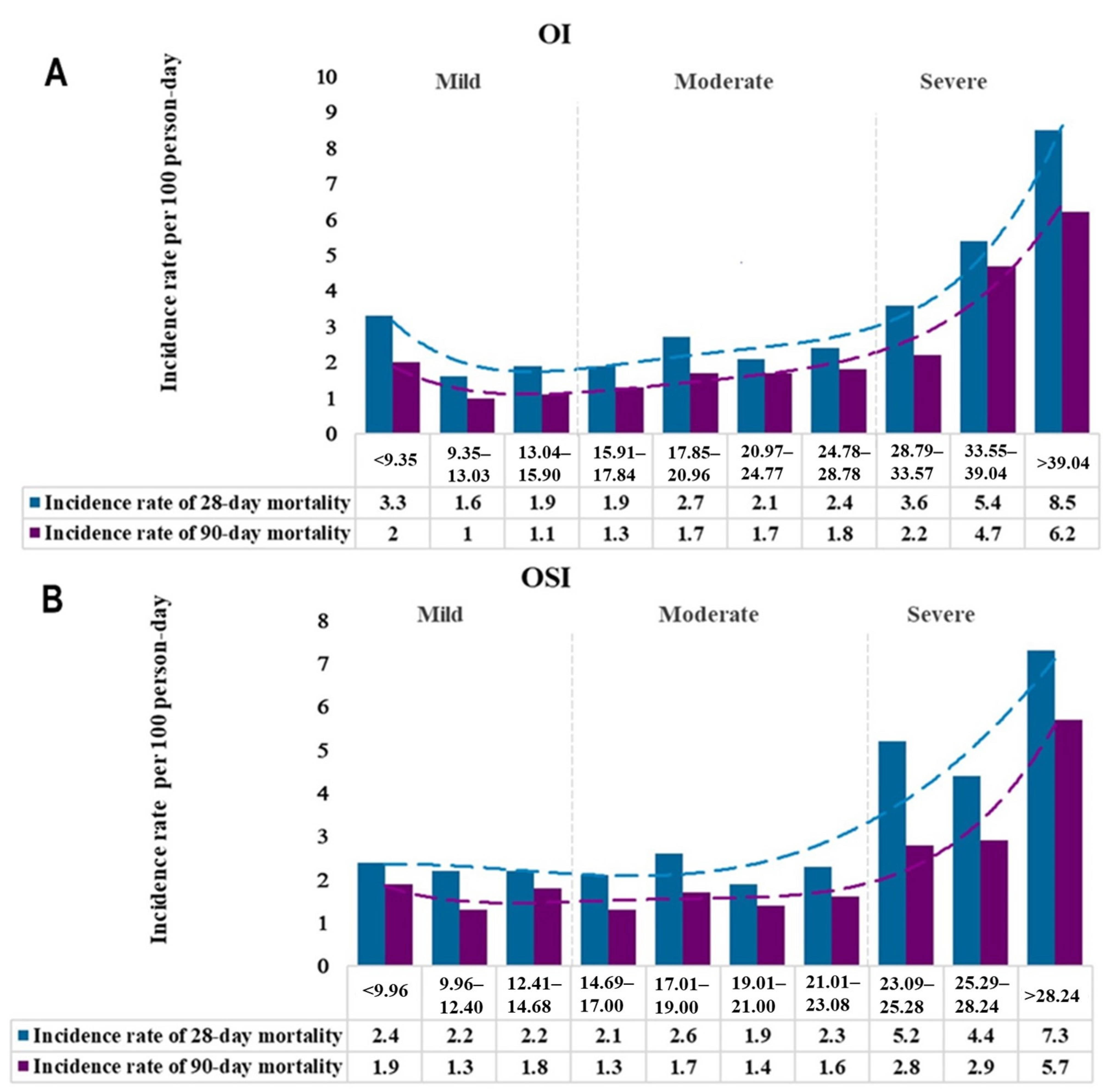
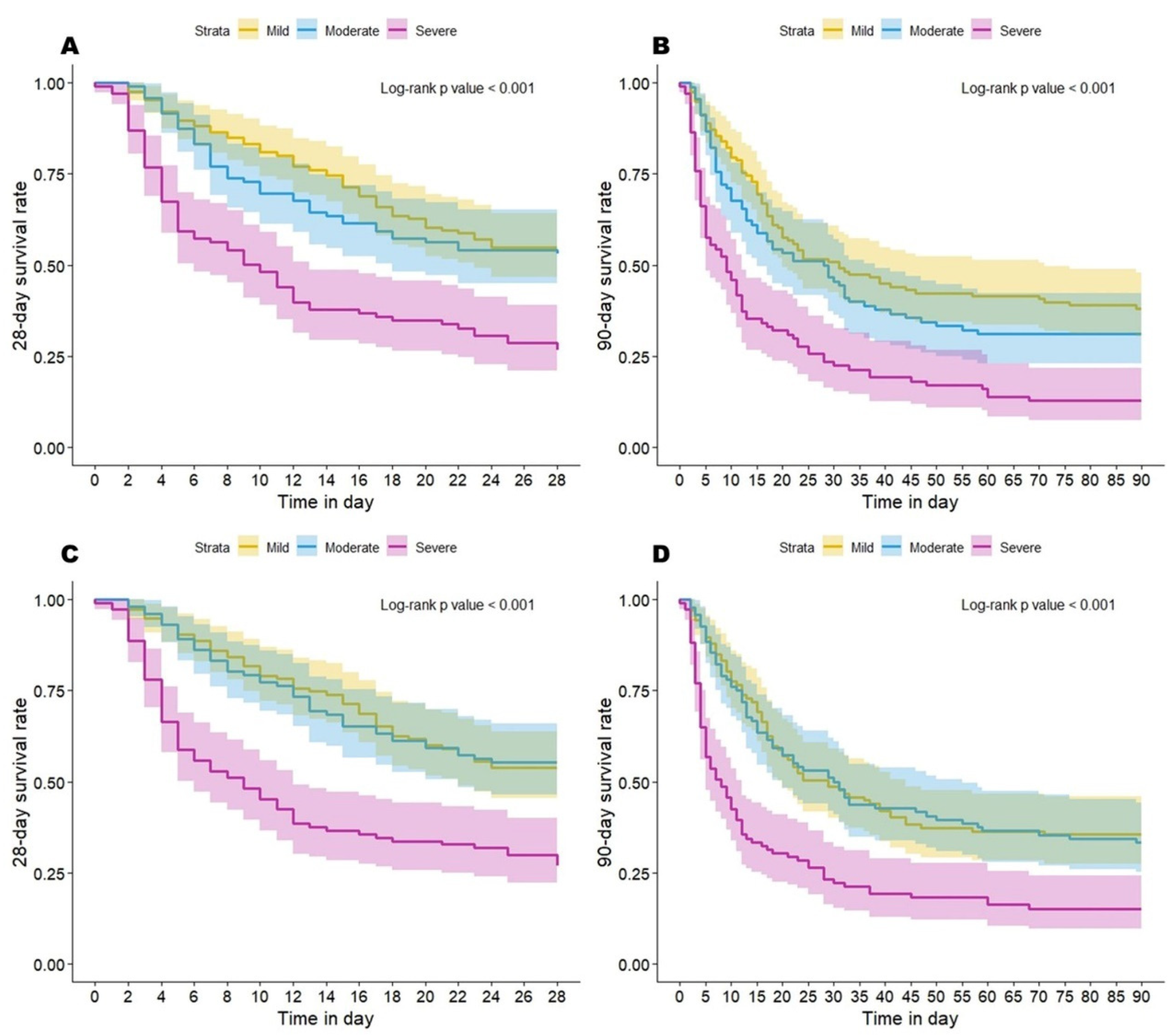
3.7. Mortality of Various OI/OSI-Based Severity Categories
3.8. Univariate Analyses of Variables Associated with Mortality
3.9. Multivariate Cox Proportional Hazard Analyses of Variables Associated with Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. Jama 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Caser, E.B.; Zandonade, E.; Pereira, E.; Gama, A.M.; Barbas, C.S. Impact of distinct definitions of acute lung injury on its incidence and outcomes in Brazilian ICUs: Prospective evaluation of 7133 patients. Crit. Care Med. 2014, 42, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Ware, L.B. Prognostic determinants of acute respiratory distress syndrome in adults: Impact on clinical trial design. Crit. Care Med. 2005, 33, S217–S222. [Google Scholar] [CrossRef] [PubMed]
- Venet, C.; Guyomarc’h, S.; Pingat, J.; Michard, C.; Laporte, S.; Bertrand, M.; Gery, P.; Page, D.; Vermesch, R.; Bertrand, J.C.; et al. Prognostic factors in acute respiratory distress syndrome: A retrospective multivariate analysis including prone positioning in management strategy. Intensive Care Med. 2003, 29, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Luhr, O.R.; Karlsson, M.; Thorsteinsson, A.; Rylander, C.; Frostell, C.G. The impact of respiratory variables on mortality in non-ARDS and ARDS patients requiring mechanical ventilation. Intensive Care Med. 2000, 26, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Tsuno, K.; Miura, K.; Takeya, M.; Kolobow, T.; Morioka, T. Histopathologic pulmonary changes from mechanical ventilation at high peak airway pressures. Am. Rev. Respir. Dis. 1991, 143 Pt 1, 1115–1120. [Google Scholar] [CrossRef]
- Kolobow, T.; Moretti, M.P.; Fumagalli, R.; Mascheroni, D.; Prato, P.; Chen, V.; Joris, M. Severe impairment in lung function induced by high peak airway pressure during mechanical ventilation. An experimental study. Am. Rev. Respir. Dis. 1987, 135, 312–315. [Google Scholar] [CrossRef]
- Parker, J.C.; Hernandez, L.A.; Peevy, K.J. Mechanisms of ventilator-induced lung injury. Crit. Care Med. 1993, 21, 131–143. [Google Scholar] [CrossRef]
- Amato, M.B.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef]
- Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef]
- Seeley, E.; McAuley, D.F.; Eisner, M.; Miletin, M.; Matthay, M.A.; Kallet, R.H. Predictors of mortality in acute lung injury during the era of lung protective ventilation. Thorax 2008, 63, 994–998. [Google Scholar] [CrossRef] [PubMed]
- Monchi, M.; Bellenfant, F.; Cariou, A.; Joly, L.M.; Thebert, D.; Laurent, I.; Dhainaut, J.F.; Brunet, F. Early predictive factors of survival in the acute respiratory distress syndrome. A multivariate analysis. Am. J. Respir. Crit. Care Med. 1998, 158, 1076–1081. [Google Scholar] [CrossRef] [PubMed]
- Pisani, L.; Roozeman, J.P.; Simonis, F.D.; Giangregorio, A.; van der Hoeven, S.M.; Schouten, L.R.; Horn, J.; Neto, A.S.; Festic, E.; Dondorp, A.M.; et al. Risk stratification using SpO(2)/FiO(2) and PEEP at initial ARDS diagnosis and after 24 h in patients with moderate or severe ARDS. Ann. Intensive Care 2017, 7, 108. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Janz, D.R.; Shaver, C.M.; Bernard, G.R.; Bastarache, J.A.; Ware, L.B. Clinical Characteristics and Outcomes Are Similar in ARDS Diagnosed by Oxygen Saturation/Fio2 Ratio Compared with Pao2/Fio2 Ratio. Chest 2015, 148, 1477–1483. [Google Scholar] [CrossRef] [PubMed]
- Bashar, F.R.; Vahedian-Azimi, A.; Farzanegan, B.; Goharani, R.; Shojaei, S.; Hatamian, S.; Mosavinasab, S.M.M.; Khoshfetrat, M.; Khatir, M.A.K.; Tomdio, A.; et al. Comparison of non-invasive to invasive oxygenation ratios for diagnosing acute respiratory distress syndrome following coronary artery bypass graft surgery: A prospective derivation-validation cohort study. J. Cardiothorac. Surg. 2018, 13, 123. [Google Scholar] [CrossRef] [PubMed]
- Babu, S.; Abhilash, K.P.; Kandasamy, S.; Gowri, M. Association between SpO(2)/FiO(2) Ratio and PaO(2)/FiO(2) Ratio in Different Modes of Oxygen Supplementation. Indian J. Crit. Care Med. 2021, 25, 1001–1005. [Google Scholar] [CrossRef] [PubMed]
- Khemani, R.G.; Smith, L.S.; Zimmerman, J.J.; Erickson, S. Pediatric acute respiratory distress syndrome: Definition, incidence, and epidemiology: Proceedings from the Pediatric Acute Lung Injury Consensus Conference. Pediatr. Crit. Care Med. 2015, 16 (Suppl. S1), S23–S40. [Google Scholar] [CrossRef] [PubMed]
- Riviello, E.D.; Kiviri, W.; Twagirumugabe, T.; Mueller, A.; Banner-Goodspeed, V.M.; Officer, L.; Novack, V.; Mutumwinka, M.; Talmor, D.S.; Fowler, R.A. Hospital Incidence and Outcomes of the Acute Respiratory Distress Syndrome Using the Kigali Modification of the Berlin Definition. Am. J. Respir. Crit. Care Med. 2016, 193, 52–59. [Google Scholar] [CrossRef]
- Matthay, M.A.; Arabi, Y.; Arroliga, A.C.; Bernard, G.; Bersten, A.D.; Brochard, L.J.; Calfee, C.S.; Combes, A.; Daniel, B.M.; Ferguson, N.D.; et al. A New Global Definition of Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2023. published online ahead of print. [Google Scholar] [CrossRef]
- DesPrez, K.; McNeil, J.B.; Wang, C.; Bastarache, J.A.; Shaver, C.M.; Ware, L.B. Oxygenation Saturation Index Predicts Clinical Outcomes in ARDS. Chest 2017, 152, 1151–1158. [Google Scholar] [CrossRef]
- Chen, W.L.; Lin, W.T.; Kung, S.C.; Lai, C.C.; Chao, C.M. The Value of Oxygenation Saturation Index in Predicting the Outcomes of Patients with Acute Respiratory Distress Syndrome. J. Clin. Med. 2018, 7, 205. [Google Scholar] [CrossRef] [PubMed]
- Otekeiwebia, A.; Ajao, O.; Ingrid, P.; Foreman, M. 668: Performance of Oxygen Saturation Index among Adults with Type I Respiratory Failure. Crit. Care Med. 2014, 42, A1521. [Google Scholar] [CrossRef]
- Needham, D.M.; Colantuoni, E.; Mendez-Tellez, P.A.; Dinglas, V.D.; Sevransky, J.E.; Dennison Himmelfarb, C.R.; Desai, S.V.; Shanholtz, C.; Brower, R.G.; Pronovost, P.J. Lung protective mechanical ventilation and two year survival in patients with acute lung injury: Prospective cohort study. Bmj 2012, 344, e2124. [Google Scholar] [CrossRef] [PubMed]
- Wick, K.D.; Matthay, M.A.; Ware, L.B. Pulse oximetry for the diagnosis and management of acute respiratory distress syndrome. Lancet Respir. Med. 2022, 10, 1086–1098. [Google Scholar] [CrossRef]
- Schenck, E.J.; Hoffman, K.L.; Oromendia, C.; Sanchez, E.; Finkelsztein, E.J.; Hong, K.S.; Kabariti, J.; Torres, L.K.; Harrington, J.S.; Siempos, I.I.; et al. A Comparative Analysis of the Respiratory Subscore of the Sequential Organ Failure Assessment Scoring System. Ann. Am. Thorac. Soc. 2021, 18, 1849–1860. [Google Scholar] [CrossRef]
- Tonetti, T.; Vasques, F.; Rapetti, F.; Maiolo, G.; Collino, F.; Romitti, F.; Camporota, L.; Cressoni, M.; Cadringher, P.; Quintel, M.; et al. Driving pressure and mechanical power: New targets for VILI prevention. Ann. Transl. Med. 2017, 5, 286. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Value | |
|---|---|
| Age (year), mean ± SD | 64 ± 16 |
| Male, No. (%) | 262 (69) |
| BMI, median (IQR), (Kg/m2) | 23 (20–26) |
| APACHE II Score, median (IQR) | 24 (18–30) |
| SOFA score, median (IQR) | 7 (5–10) |
| Lung injury score, median (IQR) | 11 (10–12) |
| Severity by Berlin definition | |
| Mild, No. (%) | 23 (6) |
| Moderate, No. (%) | 145 (38) |
| Severe, No. (%) | 189 (50) |
| Missing, No. (%) | 22 (6) |
| Comorbidity | |
| Chronic obstructive pulmonary disease, No. (%) | 126 (33) |
| Diabetes mellitus, No. (%) | 137 (36) |
| Hypertension, No. (%) | 178 (47) |
| Chronic kidney disease, No. (%) | 50 (13) |
| Heart failure, No. (%) | 117 (31) |
| Cerebral vascular accident, No. (%) | 90 (24) |
| Liver cirrhosis, No. (%) | 44 (12) |
| Malignancy, No. (%) | 88 (23) |
| Surgical ICU Admission, No. (%) | 57 (15) |
| Treatment received during ARDS period | |
| Sedation, No. (%) | 350 (92) |
| Muscle relaxant, No. (%) | 356 (94) |
| Vasopressor, No. (%) | 294 (78) |
| Total parenteral nutrition, No. (%) | 75 (20) |
| Systemic steroid, No. (%) | 320 (84) |
| Prone position, No. (%) | 42 (11) |
| Hemodialysis, No. (%) | 50 (13) |
| Continuous hemofiltration, No. (%) | 126 (33) |
| Oxygenation index, median (IQR) | 21 (15–31) |
| Oxygen saturation index, median (IQR) | 19 (14–24) |
| VT/PBW 1 (mL/Kg), median (IQR) | 9 (8–10) |
| PaO2/FIO2 ratio, median (IQR) | 96 (71–133) |
| CRS 2 (mL/cmH2O), median (IQR) | 26 (22–31) |
| Plateau Pressure 3 (cmH2O), median (IQR) | 32 (30–35) |
| PEEP (cmH2O), median (IQR) | 10 (10–12) |
| Driving Pressure 3 (cmH2O), median (IQR) | 21 (19–24) |
| 28-day Mortality, No. (%) | 186 (49) |
| 90-day Mortality, No. (%) | 233 (61) |
| Ventilator-free days, day 1–28 4, median (IQR) | 16 (6–22) |
| Survival | Death | HR (95% CI) | p-Value | |
|---|---|---|---|---|
| Age (year), mean ± SD | 62.4 ± 16.6 | 65.3 ± 15 | 1.00 (0.99–1.01) | 0.40 |
| Male, No. (%) | 126 (65) | 136 (73) | 1.37 (0.99–1.90) | 0.06 |
| BMI, median (IQR), (Kg/m2) | 23 (21–27) | 23 (20–26) | 0.97 (0.94–1.00) | 0.07 |
| APACHE II Score, median (IQR) | 24 (18–30) | 24 (19–29) | 1.00 (0.99–1.02) | 0.57 |
| SOFA score, median (IQR) | 7 (5–10) | 7 (5–10) | 1.02 (0.98–1.06) | 0.29 |
| Lung injury score, median (IQR) | 11 (10–12) | 11 (10–12) | 1.01 (0.94–1.09) | 0.82 |
| Severity by Berlin definition | ||||
| Mild, No. (%) | 9 (5) | 14 (8) | 1 | 1 |
| Moderate, No. (%) | 87 (48) | 58 (33) | 0.58 (0.33–1.05) | 0.07 |
| Severe, No. (%) | 87 (48) | 102 (59) | 0.95 (0.55–1.67) | 0.87 |
| OI, median (IQR) | 18 (13–27) | 24 (16–35) | 1.03(1.02–1.05) | <0.01 * |
| Mild, No. (%) | 87 (47) | 57 (33) | 1 | |
| Moderate, No. (%) | 62 (34) | 45 (26) | 1.11 (0.75–1.64) | 0.60 |
| Severe, No. (%) | 35 (19) | 72 (41) | 2.45 (1.73–3.47) | <0.01 * |
| OSI, median (IQR) | 18 (13–22) | 21 (14–26) | 1.05 (1.03–1.07) | <0.01 * |
| Mild, No. (%) | 90 (47) | 63 (34) | 1 | |
| Moderate, No. (%) | 67 (35) | 47 (25) | 1.01(0.69–1.47) | 0.96 |
| Severe, No. (%) | 36 (19) | 76 (41) | 2.39 (1.71–3.35) | <0.01 * |
| Comorbidity | ||||
| Hypertension, No. (%) | 98 (51) | 80 (43) | 0.74 (0.55–0.98) | 0.04 * |
| Liver cirrhosis, No. (%) | 15 (8) | 29 (16) | 1.61 (1.08–2.39) | 0.02 * |
| Malignancy, No. (%) | 32 (17) | 56 (30) | 1.54 (1.13–2.11) | 0.01 * |
| Treatment received | ||||
| Vasopressor, No. (%) | 128 (66) | 166 (89) | 3.12 (1.96–4.97) | <0.01 * |
| Hemodialysis, No. (%) | 30 (16) | 20 (11) | 0.61 (0.38–0.97) | 0.04 * |
| Continuous hemofiltration, No. (%) | 42 (22) | 84 (45) | 1.99 (1.49–2.66) | <0.01 * |
| VT/PBW 1 (ml/Kg) | 9 (8–10) | 9 (8–10) | 0.86 (0.8–0.94) | <0.01 * |
| CRS 2 (ml/cmH2O) | 28 (25–33) | 24 (20–28) | 0.94 (0.92–0.96) | <0.01 * |
| PEEP (cmH2O) | 10 (9–12) | 11 (10–13) | 1.13 (1.06–1.22) | <0.01 * |
| Driving pressure 3 (cmH2O) | 20 (18–23) | 22 (20–25) | 1.07 (1.03–1.10) | <0.01 * |
| 28-Day Mortality 1 | 90-Day Mortality 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| aHR 3 (95% CI) | p | aHR (95% CI) | p | aHR (95% CI) | p | aHR (95% CI) | p | |
| OI or OSI as continuous values | ||||||||
| OI | 1.03 (1.01–1.04) | <0.01 | - | - | 1.04 (1.02–1.06) | <0.001 | - | - |
| OSI | - | - | 1.03 (1.01–1.05) | <0.01 | - | - | 1.04 (1.02–1.06) | <0.01 |
| CRS | 0.93 (0.91–0.96) | <0.01 | 0.94 (0.92–0.97) | <0.01 | 0.93 (0.90–0.95) | <0.001 | 0.93 (0.91–0.95) | <0.01 |
| VT/PBW | 1.06 (0.95–1.17) | 0.31 | 1.06 (0.96–1.17) | 0.26 | 1.15 (1.04–1.27) | 0.007 | 1.12 (1.01–1.23) | 0.03 |
| OI or OSI as 3 groups | ||||||||
| OI group | ||||||||
| Mild | 1 | - | - | 1 | - | - | ||
| Moderate | 1.05 (0.71–1.57) | 0.80 | - | - | 1.47 (0.95–2.30) | 0.09 | - | - |
| Severe | 2.24 (1.54–3.26) | <0.01 | - | - | 3.03 (1.85–4.95) | <0.01 | - | - |
| OSI group | ||||||||
| Mild | - | - | 1 | - | - | 1 | ||
| Moderate | - | - | 0.98 (0.67–1.44) | 0.94 | - | - | 0.96 (0.66–1.41) | 0.84 |
| Severe | - | - | 2.26 (1.58–3.24) | <0.01 | - | - | 2.15 (1.43–3.24) | <0.01 |
| CRS | 0.93 (0.91–0.96) | <0.01 | 0.93 (0.91–0.96) | <0.01 | 0.93 (0.90–0.95) | <0.01 | 0.93 (0.90–0.95) | <0.01 |
| VT/PBW | 1.07 (0.96–1.19) | 0.22 | 1.06 (0.96–1.17) | 0.25 | 1.16 (1.06–1.28) | 0.01 | 1.15 (1.05–1.26) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, S.-H.; Kor, C.-T.; Chi, S.-H.; Li, C.-Y. Categorizing Acute Respiratory Distress Syndrome with Different Severities by Oxygen Saturation Index. Diagnostics 2024, 14, 37. https://doi.org/10.3390/diagnostics14010037
Wu S-H, Kor C-T, Chi S-H, Li C-Y. Categorizing Acute Respiratory Distress Syndrome with Different Severities by Oxygen Saturation Index. Diagnostics. 2024; 14(1):37. https://doi.org/10.3390/diagnostics14010037
Chicago/Turabian StyleWu, Shin-Hwar, Chew-Teng Kor, Shu-Hua Chi, and Chun-Yu Li. 2024. "Categorizing Acute Respiratory Distress Syndrome with Different Severities by Oxygen Saturation Index" Diagnostics 14, no. 1: 37. https://doi.org/10.3390/diagnostics14010037