
Validation of a Digital Headache Calendar at a Tertiary Referral Center
 , ,
, ,
Abstract
:1. Introduction
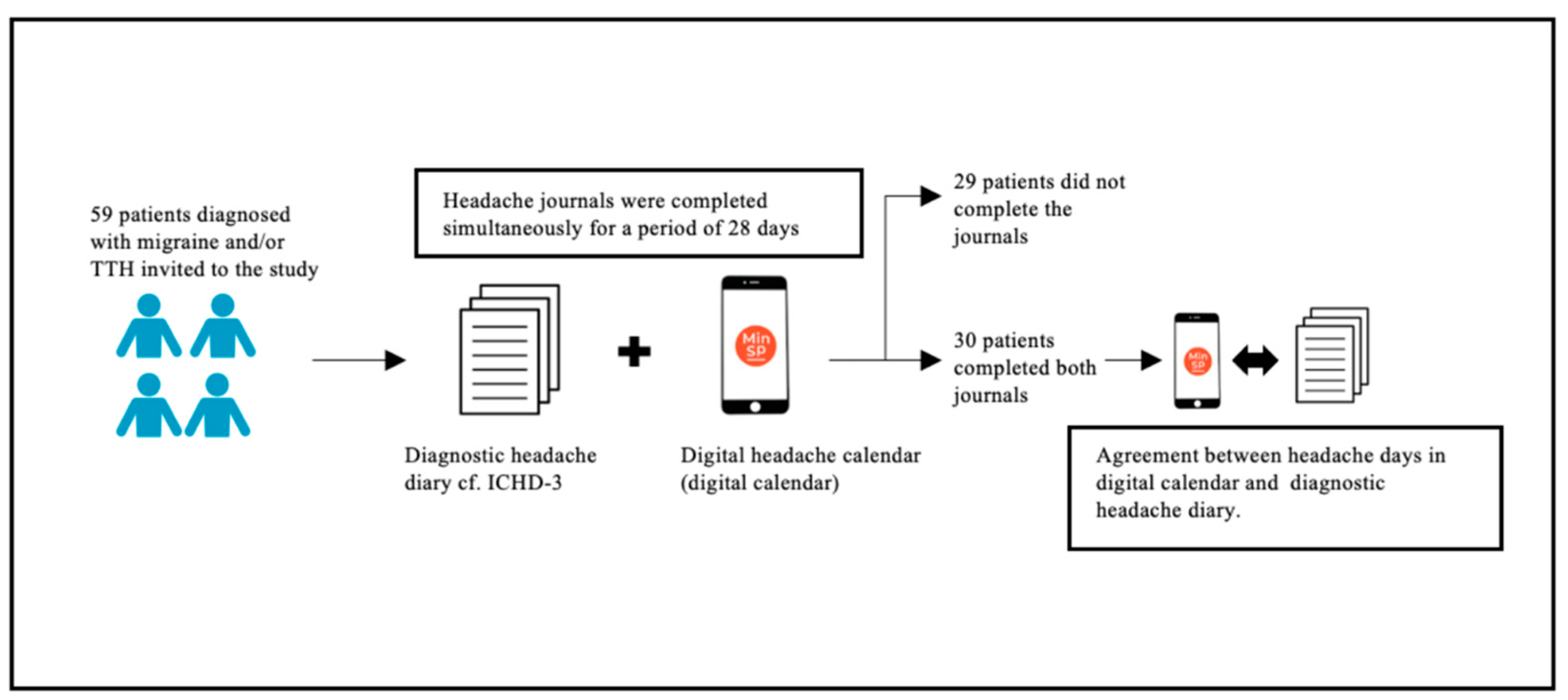
2. Methods
2.1. Study Population and Study Design
2.2. The Diagnostic Headache Diary
2.3. The Digital Headache Calendar (Digital Calendar)
2.4. Validation of Digital Calendar
2.5. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. Validation of Electronic Headache Diary (Digital Calendar)
3.2.1. Migraine Days

{kind=link}
| A | B | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Migraine Days | Migraine Days | ||||||||
| Yes | No | Yes | No | ||||||
| Self-reported migraine days | yes | 173 | 86 | 259 | Self-reported migraine days | yes | 225 | 34 | 259 |
| no | 27 | 143 | 170 | no | 48 | 122 | 170 | ||
| 200 | 229 | 429 | 273 | 156 | 429 | ||||
| Sensitivity: 173/200 = 0.87 | Sensitivity: 225/273 = 0.82 | ||||||||
| Specificity: 143/229 = 0.62 | Specificity: 122/156 = 0.78 | ||||||||
| PPV: 173/259 = 0.67 | PPV: 225/259 = 0.87 | ||||||||
| NPV: 143/170 = 0.84 | NPV: 122/170 = 0.72 | ||||||||
| Unweighted kappa coefficient (κ): 0.49 | Unweighted kappa coefficient (κ): 0.60 | ||||||||
3.2.2. Tension-Type Headache (TTH) Days
| A | B | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| TTH Days | TTH Days | ||||||||
| Yes | No | Yes | No | ||||||
| Self-reported TTH days | yes | 164 | 86 | 250 | Self-reported TTH days | yes | 173 | 77 | 250 |
| no | 27 | 199 | 226 | no | 32 | 194 | 226 | ||
| 191 | 285 | 476 | 205 | 271 | 476 | ||||
| Sensitivity: 164/191 = 0.86 | Sensitivity: 173/205 = 0.84 | ||||||||
| Specificity: 199/285 = 0.70 | Specificity: 194/271 = 0.72 | ||||||||
| PPV: 164/250 = 0.66 | PPV: 173/250 = 0.70 | ||||||||
| NPV: 199/226 = 0.88 | NPV: 194/226 = 0.86 | ||||||||
| Unweighted kappa coefficient (κ): 0.52 | Unweighted kappa coefficient (κ): 0.54 | ||||||||
3.3. Comparison between Patient Groups
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Stovner, L.J.; Hagen, K.; Linde, M.; Steiner, T.J. The global prevalence of headache: An update, with analysis of the influences of methodological factors on prevalence estimates. J. Headache Pain 2022, 23, 34. [Google Scholar] [CrossRef] [PubMed]
- Nappi, G.; Jensen, R.; Nappi, R.E.; Sances, G.; Torelli, P.; Olesen, J. Diaries and calendars for migraine. A review. Cephalalgia 2006, 26, 905–916. [Google Scholar] [CrossRef] [PubMed]
- Russell, M.B.; Rasmussen, B.K.; Brennum, J.; Iversen, H.K.; Jensen, R.A.; Olesen, J. Presentation of a New Instrument: The Diagnostic Headache Diary. Cephalalgia 1992, 12, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Tassorelli, C.; Sances, G.; Allena, M.; Ghiotto, N.; Bendtsen, L.; Olesen, J.; Nappi, G.; Jensen, R. The usefulness and applicability of a basic headache diary before first consultation: Results of a pilot study conducted in two centres. Cephalalgia 2018, 28, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, K.D.; Rasmussen, C.; Russell, M.B. The diagnostic headache diary--a headache expert system. Stud Health Technol. Inform. 2000, 78, 149–160. [Google Scholar] [PubMed]
- Kim, K.M.; Kim, A.R.; Lee, W.; Lee, W.; Jang, B.H.; Heo, K.; Chu, M.K. Development and validation of a web-based headache diagnosis questionnaire. Sci. Rep. 2022, 12, 7032. [Google Scholar] [CrossRef] [PubMed]
- Maizels, M.; Wolfe, W.J. An expert system for headache diagnosis: The computerized headache assessment tool (CHAT). Headache 2008, 48, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.; Tassorelli, C.; Rossi, P.; Allena, M.; Osipove, V.; Steiner, T.J.; Sandrini, G.; Olesen, J.; Nappi, G. A basic diagnostic headache diary (BDHD) is well accepted and useful in the diagnosis of headache. A multicentre European and Latin American study. Cephalalgia 2011, 31, 1549–1560. [Google Scholar] [CrossRef]
- Brandes, J.L.; Saper, J.R.; Diamond, M.; Couch, J.R.; Lewis, D.W.; Schmitt, J.; Neto, W.; Schwabe, S.; Jacobs, D. Topiramate for Migraine Prevention: A Randomized Controlled Trial. JAMA 2004, 291, 965–973. [Google Scholar] [CrossRef]
- Diener, H.C.; Tassorelli, C.; Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; Messoud, A.; Becker, W.J.; Ferrari, M.D.; Goadsby, P.J.; Pozo-Rosich, P.; et al. Guidelines of the International Headache Society for controlled trials of preventive treatment of migraine attacks in episodic migraine in adults. Cephalalgia 2020, 40, 1026–1044. [Google Scholar] [CrossRef]
- Bendtsen, L.; Bigal, M.E.; Cerbo, R.; Diener, H.C.; Holroyd, K.; Lampl, C.; Mitsikostas, D.D.; Steiner, T.J.; Tfelt-Hansen, P. Guidelines for controlled trials of drugs in tension-type headache: Second edition. Cephalalgia 2010, 30, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Allena, M.; Cuzzoni, M.G.; Tassorelli, C.; Nappi, G.; Antonica, F. An electronic diary on a palm device for headache monitoring: A preliminary experience. J. Headache Pain 2012, 13, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Raffaelli, B.; Mecklenburg, J.; Overeem, L.H.; Scholler, S.; Dahlem, M.A.; Kurth, T.; Goncalves, A.O.; Reuter, U.; Neeb, L. Determining the Evolution of Headache Among Regular Users of a Daily Electronic Diary via a Smartphone App: Observational Study. JMIR Mhealth Uhealth 2021, 9, e26401. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.A.; Shiffman, S.; Schwartz, J.E.; Broderick, J.E.; Hufford, M.R. Patient compliance with paper and electronic diaries. Control. Clin. Trials 2003, 24, 182–199. [Google Scholar] [CrossRef]
- Hundert, A.S.; Huguet, A.; McGrath, P.J.; Stinson, J.N.; Wheaton, M. Commercially Available Mobile Phone Headache Diary Apps: A Systematic Review. JMIR Mhealth Uhealth 2014, 2, e3452. [Google Scholar] [CrossRef]
- Roesch, A.; Dahlem, M.A.; Neeb, L.; Kurth, T. Validation of an algorithm for automated classification of migraine and tension-type headache attacks in an electronic headache diary. J. Headache Pain 2020, 21, 75. [Google Scholar] [CrossRef]
- Kikuchi, H.; Yoshiuchi, K.; Miyasaka, N.; Ohashi, K.; Yamamoto, Y.; Kumano, H.; Kuboki, T.; Akabayashi, A. Reliability of recalled self-report on headache intensity: Investigation using ecological momentary assessment technique. Cephalalgia 2006, 26, 1335–1343. [Google Scholar] [CrossRef]
- McKenzie, J.A.; Cutrer, F.M. How Well Do Headache Patients Remember? A Comparison of Self-Report Measures of Headache Frequency and Severity in Patients with Migraine. Headache J. Head Face Pain 2009, 49, 669–672. [Google Scholar] [CrossRef]
- Miller, V.E.; Faurot, K.R.; Palssson, O.S.; Macintosh, B.A.; Suchindran, C.; Honvoh, G.; Gaylord, S.; Ramsden, C.E.; Mann, J.D. Comparing prospective headache diary and retrospective four-week headache questionnaire over 20 weeks: Secondary data analysis from a randomized controlled trial. Cephalalgia 2020, 40, 1523–1531. [Google Scholar] [CrossRef]
- Van Casteren, D.S.; Verhagen, I.E.; Boer, I.D.; Lentsch, S.V.; Fronczek, R.; Zwet, E.W.; MaassenVanDenBrink, A.; Terwindt, G.M. E-diary use in clinical headache practice: A prospective observational study. Cephalalgia 2021, 41, 1161–1171. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.; Amin, F.M.; Ashima, M.; Bendtsen, L.; Deligianni, C.L.; Gil-Gouveia, R.; Katsarava, Z.; MaassenVanDenBrink, A.; Martelletti, P.; Mitsikostas, D.D.; et al. European Headache Federation guideline on the use of monoclonal antibodies targeting the calcitonin gene related peptide pathway for migraine prevention—2022 update. J. Headache Pain 2022, 23, 67. [Google Scholar] [CrossRef] [PubMed]
- The Danish Medicines Agency Webpage: Medicinraadet. Medicinrådets samling af Vurdering af anti-CGRP-Antistoffer til Behandling af Kronisk Migræne, Herunder Kriterier for Opstart, Monitorering og Seponering. Available online: https://medicinraadet.dk (accessed on 25 May 2023).

| Headache Patients (n = 30) | |
|---|---|
| Age, years mean ± SD | 41 ± 12 |
| Women, n (%) | 26 (87%) |
| Diagnosis by physician at headache clinic 1, n (%) | |
| Episodic migraine | 9 (30%) |
| Episodic TTH | 14 (47%) |
| Chronic migraine | 19 (63%) |
| Chronic TTH | 4 (13%) |
| Years with diagnosis from headache center, n (%) | |
| ≤1 year | 12 (40%) |
| 2 years | 4 (13%) |
| 3 years | 5 (17%) |
| 4 years | 5 (17%) |
| 5 years | 4 (13%) |
| Headache days in a month (28 days), median (IQR) | 15.5 (9.25–21.75) |
| ⇒ Migraine days/month | 8.5 (4.75–13.0) |
| ⇒ TTH days/month | 10.5 (7.25–15.25) |
| Days using analgesics 2, mean ± SD | 7.0 ± 3.4 |
| Number of headache days reported in digital calendar per use, median (IQR) | 2.9 (1.7–5.7) |
| Correctly Identified Headache Attacks, % | |||
|---|---|---|---|
| ≥75% | <75% | p value | |
| Headache patients (n = 30) (%) | 14 (47) | 16 (53) | |
| Age, years mean ± SD | 39.1 ± 13.5 | 42.9 ± 10.9 | 0.40 |
| Women, n (%) | 14 (100%) | 12 (75%) | 0.10 |
| Diagnosis by physician at headache clinic, n (%) | |||
| Episodic migraine | 3 (15%) | 6 (23%) | 0.71 |
| Episodic TTH | 6 (30%) | 8 (31%) | 0.96 |
| Chronic migraine | 9 (45%) | 10 (38%) | 0.66 |
| Chronic TTH | 2 (10%) | 2 (8%) | 1.00 |
| Years with diagnosis, n (%) | |||
| ≤1 year | 6 (43%) | 6 (38%) | 0.75 |
| 2–4 years | 5 (36%) | 9 (56%) | 0.22 |
| 5 years | 3 (21%) | 1 (6%) | 0.96 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kjerrumgaard, A.; Hvedstrup, J.; Carlsen, L.N.; Dyre, K.; Schytz, H. Validation of a Digital Headache Calendar at a Tertiary Referral Center. Diagnostics 2024, 14, 21. https://doi.org/10.3390/diagnostics14010021
Kjerrumgaard A, Hvedstrup J, Carlsen LN, Dyre K, Schytz H. Validation of a Digital Headache Calendar at a Tertiary Referral Center. Diagnostics. 2024; 14(1):21. https://doi.org/10.3390/diagnostics14010021
Chicago/Turabian StyleKjerrumgaard, Amalie, Jeppe Hvedstrup, Louise Ninett Carlsen, Kristine Dyre, and Henrik Schytz. 2024. "Validation of a Digital Headache Calendar at a Tertiary Referral Center" Diagnostics 14, no. 1: 21. https://doi.org/10.3390/diagnostics14010021