

A Systematic Review of Diagnostic and Prognostic Biomarkers for Head and Neck Cancer of Unknown Primary: An Unmet Clinical Need
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Data Extraction
2.5. Data Extraction
3. Results
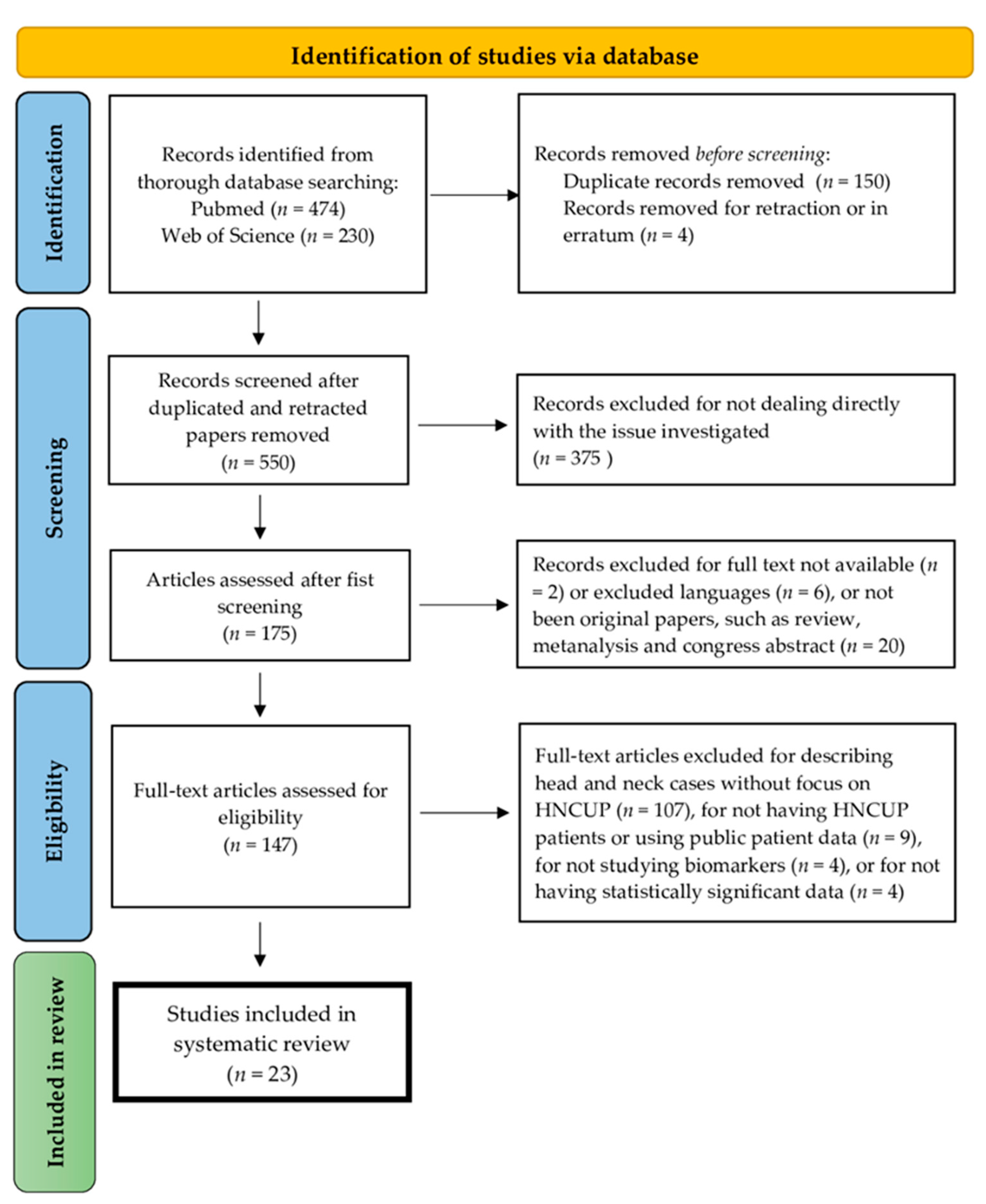
3.1. Study Selection
3.2. Characteristics of the Selected Studies
3.3. HNCUP Biomarkers
3.3.1. Biomarkers Able to Identify H&N Primary Tumor Origin
3.3.2. Head and Neck Cancer of Unknown Primary Diagnostic Biomarkers
- HPV biomarker in HNCUP diagnosis
- EBV biomarkers in HNCUP diagnosis
- Other HNCUP diagnostic biomarkers
- Head and neck cancer of unknown primary prognostic biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, M.S.; Sanoff, H.K. Cancer of unknown primary. BMJ 2020, 371, m4050. [Google Scholar] [CrossRef]
- Maghami, E.; Ismaila, N.; Alvarez, A.; Chernock, R.; Duvvuri, U.; Geiger, J.; Gross, N.; Haughey, B.; Paul, D.; Rodriguez, C.; et al. Diagnosis and Management of Squamous Cell Carcinoma of Unknown Primary in the Head and Neck: ASCO Guideline. J. Clin. Oncol. 2020, 38, 2570–2596. [Google Scholar] [CrossRef]
- Golusinski, P.; Di Maio, P.; Pehlivan, B.; Colley, S.; Nankivell, P.; Kong, A.; Hartley, A.; Mehanna, H. Evidence for the approach to the diagnostic evaluation of squamous cell carcinoma occult primary tumors of the head and neck. Oral Oncol. 2019, 88, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Civantos, F.J.; Vermorken, J.B.; Shah, J.P.; Rinaldo, A.; Suarez, C.; Kowalski, L.P.; Rodrigo, J.P.; Olsen, K.; Strojan, P.; Makitie, A.A.; et al. Metastatic Squamous Cell Carcinoma to the Cervical Lymph Nodes From an Unknown Primary Cancer: Management in the HPV Era. Front. Oncol. 2020, 10, 593164. [Google Scholar] [CrossRef] [PubMed]
- Ye, W.; Arnaud, E.H.; Langerman, A.; Mannion, K.; Topf, M.C. Diagnostic approaches to carcinoma of unknown primary of the head and neck. Eur. J. Cancer Care Engl. 2021, 30, e13459. [Google Scholar] [CrossRef] [PubMed]
- Faisal, M.; Le, N.S.; Grasl, S.; Janik, S.; Simmel, H.; Schratter-Sehn, A.U.; Hamzavi, J.S.; Franz, P.; Erovic, B.M. Carcinoma of Unknown Primary (CUP) versus CUP Turned to Primary Carcinoma of the Head and Neck-An Analysis of Diagnostic Methods and the Impact of Primary Tumor on Clinical Outcome. Diagnostics 2022, 12, 894. [Google Scholar] [CrossRef]
- Pavlidis, N.; Pentheroudakis, G.; Plataniotis, G. Cervical lymph node metastases of squamous cell carcinoma from an unknown primary site: A favourable prognosis subset of patients with CUP. Clin. Transl. Oncol. 2009, 11, 340–348. [Google Scholar] [CrossRef]
- Pinkiewicz, M.; Dorobisz, K.; Zatonski, T. A Systematic Review of Cancer of Unknown Primary in the Head and Neck Region. Cancer Manag. Res. 2021, 13, 7235–7241. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Schroeder, L.; Romeo, S.; Pawlita, M. The prevalence of human papillomavirus in squamous cell carcinoma of unknown primary site metastatic to neck lymph nodes: A systematic review. Clin. Exp. Metastasis 2015, 32, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.H.H.; Channir, H.I.; von Buchwald, C. Human Papillomavirus and Squamous Cell Carcinoma of Unknown Primary in the Head and Neck Region: A Comprehensive Review on Clinical Implications. Viruses 2021, 13, 1297. [Google Scholar] [CrossRef] [PubMed]
- Kennel, T.; Garrel, R.; Costes, V.; Boisselier, P.; Crampette, L.; Favier, V. Head and neck carcinoma of unknown primary. Eur. Ann. Otorhinolaryngol. Head. Neck Dis. 2019, 136, 185–192. [Google Scholar] [CrossRef]
- Oien, K.A. Pathologic evaluation of unknown primary cancer. Semin. Oncol. 2009, 36, 8–37. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Fan, S.; Zhang, X.; Li, S.; Zhou, M.; Xiong, W.; Tan, M.; Zhang, W.; Li, G. Epstein-Barr virus-encoded small RNA 1 (EBER-1) could predict good prognosis in nasopharyngeal carcinoma. Clin. Transl. Oncol. 2016, 18, 206–211. [Google Scholar] [CrossRef]
- Chen, Y.P.; Chan, A.T.C.; Le, Q.T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Taverna, F.; Alfieri, S.; Romano, R.; Campanini, G.; Marceglia, S.; Giardina, F.; Mazzocchi, A.; Comoli, P.; Gloghini, A.; Quattrone, P.; et al. Comparing BamHI-W and CE-marked assays to detect circulating Epstein-Barr Virus (EBV) DNA of nasopharyngeal cancer patients in a non-endemic area. Oral. Oncol. 2022, 135, 106229. [Google Scholar] [CrossRef]
- Ota, I.; Kitahara, T. Cancer of unknown primary in the head and neck: Diagnosis and treatment. Auris Nasus Larynx 2021, 48, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, K.; Watson, M.; Jankowska, P.; Bhide, S.; Simo, R. Investigation and management of the unknown primary with metastatic neck disease: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S170–S175. [Google Scholar] [CrossRef] [PubMed]
- Cabrera Rodriguez, J.; Cacicedo, J.; Giralt, J.; Garcia Miragall, E.; Lloret, M.; Arias, F.; Gonzalez Ruiz, M.A.; Contreras, J. GEORCC recommendations on target volumes in radiotherapy for Head Neck Cancer of Unkown Primary. Crit. Rev. Oncol. Hematol. 2018, 130, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Ghatasheh, H.; Huang, S.H.; Su, J.; Xu, W.; Bratman, S.V.; Cho, J.; Giuliani, M.; Hahn, E.; Hope, A.; Kim, J.; et al. Evaluation of risk-tailored individualized selection of radiation therapy target volume for head and neck carcinoma of unknown primary. Radiother. Oncol. 2022, 175, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Melchardt, T.; Magnes, T.; Hufnagl, C.; Thorner, A.R.; Ducar, M.; Neureiter, D.; Trankenschuh, W.; Klieser, E.; Gaggl, A.; Rosch, S.; et al. Clonal evolution and heterogeneity in metastatic head and neck cancer-An analysis of the Austrian Study Group of Medical Tumour Therapy study group. Eur. J. Cancer 2018, 93, 69–78. [Google Scholar] [CrossRef]
- Machiels, J.P.; Rene Leemans, C.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Park, G.C.; Lee, M.; Roh, J.L.; Yu, M.S.; Choi, S.H.; Nam, S.Y.; Kim, S.Y.; Cho, K.J. Human papillomavirus and p16 detection in cervical lymph node metastases from an unknown primary tumor. Oral Oncol. 2012, 48, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Park, G.C.; Lee, M.; Roh, J.L.; Choi, S.H.; Nam, S.Y.; Kim, S.Y.; Cho, K.J. Phospho-Rb (Ser780) as a biomarker in patients with cervical lymph node metastases from an unknown primary tumour: A retrospective cohort study. Clin. Otolaryngol. 2013, 38, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Cheol Park, G.; Roh, J.L.; Cho, K.J.; Seung Kim, J.; Hyeon Jin, M.; Choi, S.H.; Yuhl Nam, S.; Yoon Kim, S. (18) F-FDG PET/CT vs. human papillomavirus, p16 and Epstein-Barr virus detection in cervical metastatic lymph nodes for identifying primary tumors. Int. J. Cancer 2017, 140, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Raghav, K.; Overman, M.; Poage, G.M.; Soifer, H.S.; Schnabel, C.A.; Varadhachary, G.R. Defining a Distinct Immunotherapy Eligible Subset of Patients with Cancer of Unknown Primary Using Gene Expression Profiling with the 92-Gene Assay. Oncologist 2020, 25, e1807–e1811. [Google Scholar] [CrossRef]
- Karahatay, S.; Thomas, K.; Koybasi, S.; Senkal, C.E.; Elojeimy, S.; Liu, X.; Bielawski, J.; Day, T.A.; Gillespie, M.B.; Sinha, D.; et al. Clinical relevance of ceramide metabolism in the pathogenesis of human head and neck squamous cell carcinoma (HNSCC): Attenuation of C(18)-ceramide in HNSCC tumors correlates with lymphovascular invasion and nodal metastasis. Cancer Lett. 2007, 256, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Werner, J.A.; Gottschlich, S.; Folz, B.J.; Goeroegh, T.; Lippert, B.M.; Maass, J.D.; Rudert, H. p53 serum antibodies as prognostic indicator in head and neck cancer. Cancer Immunol. Immunother. 1997, 44, 112–116. [Google Scholar] [CrossRef]
- Sun, W.; Wu, W.; Wang, Q.; Yao, Q.; Feng, Q.; Wang, Y.; Sun, Y.; Liu, Y.; Lai, Q.; Zhang, G.; et al. Clinical validation of a 90-gene expression test for tumor tissue of origin diagnosis: A large-scale multicenter study of 1417 patients. J. Transl. Med. 2022, 20, 114. [Google Scholar] [CrossRef]
- Rohrbach, M.R.; Britt, C.J.; Schwalbe, M.; Wieland, A.M.; Hartig, G.K. p16 Immunohistochemistry Is a Useful Diagnostic Adjunct in Cases of Metastatic Cervical Carcinoma of Unknown Origin. J. Oral Maxillofac. Surg. 2017, 75, 525–529. [Google Scholar] [CrossRef]
- Hata, T.; Iga, H.; Imai, S.; Hirokawa, M. Heterotopic salivary gland adenocarcinoma in the cervical region. Int. J. Oral Maxillofac. Surg. 1997, 26, 290–292. [Google Scholar] [CrossRef]
- Gupta, P.; Rajwanshi, A.; Kakkar, N. Metastatic Epithelial-Myoepithelial Carcinoma in a Female Presenting with Neck Mass and Lytic Lesion in Acetabulum: A Diagnostic Challenge on Cytology. Turk. Patoloji Derg. 2021, 37, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Leung, S.Y.; Chung, L.P.; Ho, C.M.; Yuen, S.T.; Wong, M.P.; Kwong, W.K. An Epstein-Barr virus positive undifferentiated carcinoma in the lacrimal sac. Histopathology 1996, 28, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Dictor, M.; Siven, M.; Tennvall, J.; Rambech, E. Determination of nonendemic nasopharyngeal carcinoma by in situ hybridization for Epstein-Barr virus EBER1 RNA: Sensitivity and specificity in cervical node metastases. Laryngoscope 1995, 105, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Desai, P.C.; Jaglal, M.V.; Gopal, P.; Ghim, S.J.; Miller, D.M.; Farghaly, H.; Jenson, A.B. Human papillomavirus in metastatic squamous carcinoma from unknown primaries in the head and neck: A retrospective 7 year study. Exp. Mol. Pathol. 2009, 87, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, B.; Das, P.; Naresh, K.N.; Borges, A.M. Angiogenic ability of metastatic squamous carcinoma in the cervical lymph nodes from unknown primary tumours. J. Clin. Pathol. 2011, 64, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Shan, A.; Rooper, L.M.; Ryan, J.F.; Eisele, D.W.; Fakhry, C. p16 immunohistochemistry for primary tumor detection in HPV-positive squamous cell carcinoma of unknown primary. Am. J. Otolaryngol. 2021, 42, 103015. [Google Scholar] [CrossRef] [PubMed]
- Vent, J.; Haidle, B.; Wedemeyer, I.; Huebbers, C.; Siefer, O.; Semrau, R.; Preuss, S.F.; Klussmann, J. p16 expression in carcinoma of unknown primary: Diagnostic indicator and prognostic marker. Head. Neck 2013, 35, 1521–1526. [Google Scholar] [CrossRef]
- Schroeder, L.; Wichmann, G.; Willner, M.; Michel, A.; Wiesenfarth, M.; Flechtenmacher, C.; Gradistanac, T.; Pawlita, M.; Dietz, A.; Waterboer, T.; et al. Antibodies against human papillomaviruses as diagnostic and prognostic biomarker in patients with neck squamous cell carcinoma from unknown primary tumor. Int. J. Cancer 2018, 142, 1361–1368. [Google Scholar] [CrossRef]
- Sivars, L.; Landin, D.; Grun, N.; Vlastos, A.; Marklund, L.; Nordemar, S.; Ramqvist, T.; Munck-Wikland, E.; Nasman, A.; Dalianis, T. Validation of Human Papillomavirus as a Favourable Prognostic Marker and Analysis of CD8(+) Tumour-infiltrating Lymphocytes and Other Biomarkers in Cancer of Unknown Primary in the Head and Neck Region. Anticancer Res. 2017, 37, 665–673. [Google Scholar] [CrossRef]
- Kobayashi, K.; Saito, Y.; Omura, G.; Ando, M.; Sakamoto, T.; Yamasoba, T.; Asakage, T. Clinical features of human papilloma virus-related head and neck squamous cell carcinoma of an unknown primary site. ORL J. Otorhinolaryngol. Relat. Spec. 2014, 76, 137–146. [Google Scholar] [CrossRef]
- Dixon, P.R.; Au, M.; Hosni, A.; Perez-Ordonez, B.; Weinreb, I.; Xu, W.; Song, Y.; Huang, S.H.; O’Sullivan, B.; Goldstein, D.P.; et al. Impact of p16 expression, nodal status, and smoking on oncologic outcomes of patients with head and neck unknown primary squamous cell carcinoma. Head Neck 2016, 38, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Keller, L.M.; Galloway, T.J.; Holdbrook, T.; Ruth, K.; Yang, D.; Dubyk, C.; Flieder, D.; Lango, M.N.; Mehra, R.; Burtness, B.; et al. p16 status, pathologic and clinical characteristics, biomolecular signature, and long-term outcomes in head and neck squamous cell carcinomas of unknown primary. Head Neck 2014, 36, 1677–1684. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, L.; Boscolo-Rizzo, P.; Dal Cin, E.; Romeo, S.; Baboci, L.; Dyckhoff, G.; Hess, J.; Lucena-Porcel, C.; Byl, A.; Becker, N.; et al. Human papillomavirus as prognostic marker with rising prevalence in neck squamous cell carcinoma of unknown primary: A retrospective multicentre study. Eur. J. Cancer 2017, 74, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Nakao, K.; Yuge, T.; Mochiki, M.; Nibu, K.; Sugasawa, M. Detection of Epstein-Barr virus in metastatic lymph nodes of patients with nasopharyngeal carcinoma and a primary unknown carcinoma. Arch. Otolaryngol. Head Neck Surg. 2003, 129, 338–340. [Google Scholar] [CrossRef] [PubMed]
- Szymonowicz, K.A.; Chen, J. Biological and clinical aspects of HPV-related cancers. Cancer Biol. Med. 2020, 17, 864–878. [Google Scholar] [CrossRef]
- Lewis, J.S., Jr.; Khan, R.A.; Masand, R.P.; Chernock, R.D.; Zhang, Q.; Al-Naief, N.S.; Muller, S.; McHugh, J.B.; Prasad, M.L.; Brandwein-Gensler, M.; et al. Recognition of nonkeratinizing morphology in oropharyngeal squamous cell carcinoma-a prospective cohort and interobserver variability study. Histopathology 2012, 60, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Gronhoj Larsen, C.; Gyldenlove, M.; Jensen, D.H.; Therkildsen, M.H.; Kiss, K.; Norrild, B.; Konge, L.; von Buchwald, C. Correlation between human papillomavirus and p16 overexpression in oropharyngeal tumours: A systematic review. Br. J. Cancer 2014, 110, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Stephen, J.K.; Divine, G.; Chen, K.M.; Chitale, D.; Havard, S.; Worsham, M.J. Significance of p16 in Site-specific HPV Positive and HPV Negative Head and Neck Squamous Cell Carcinoma. Cancer Clin. Oncol. 2013, 2, 51–61. [Google Scholar] [CrossRef]
- Han, S.; Tay, J.K.; Loh, C.J.L.; Chu, A.J.M.; Yeong, J.P.S.; Lim, C.M.; Toh, H.C. Epstein-Barr Virus Epithelial Cancers-A Comprehensive Understanding to Drive Novel Therapies. Front. Immunol. 2021, 12, 734293. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Chen, G.; Gong, X.; Wang, Y.; Zheng, Y.; Liao, X.; Liao, W.; Song, L.; Xu, J.; Zhang, X. The diagnostic value of EBV-DNA and EBV-related antibodies detection for nasopharyngeal carcinoma: A meta-analysis. Cancer Cell. Int. 2021, 21, 164. [Google Scholar] [CrossRef]
- Huang, S.H.; O’Sullivan, B. Overview of the 8th Edition TNM Classification for Head and Neck Cancer. Curr. Treat. Options Oncol. 2017, 18, 40. [Google Scholar] [CrossRef] [PubMed]
- Durante, G.; Broseghini, E.; Comito, F.; Naddeo, M.; Milani, M.; Salamon, I.; Campione, E.; Dika, E.; Ferracin, M. Circulating microRNA biomarkers in melanoma and non-melanoma skin cancer. Expert. Rev. Mol. Diagn. 2022, 22, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Cocks, A.; Martinez-Rodriguez, V.; Del Vecchio, F.; Schukking, M.; Broseghini, E.; Giannakopoulos, S.; Fabbri, M. Diverse roles of EV-RNA in cancer progression. Semin. Cancer Biol. 2021, 75, 127–135. [Google Scholar] [CrossRef]
- Del Vecchio, F.; Martinez-Rodriguez, V.; Schukking, M.; Cocks, A.; Broseghini, E.; Fabbri, M. Professional killers: The role of extracellular vesicles in the reciprocal interactions between natural killer, CD8+ cytotoxic T-cells and tumour cells. J. Extracell. Vesicles 2021, 10, e12075. [Google Scholar] [CrossRef] [PubMed]
- Conway, A.M.; Mitchell, C.; Kilgour, E.; Brady, G.; Dive, C.; Cook, N. Molecular characterisation and liquid biomarkers in Carcinoma of Unknown Primary (CUP): Taking the ‘U’ out of ‘CUP’. Br. J. Cancer 2019, 120, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Riefolo, M.; Porcellini, E.; Dika, E.; Broseghini, E.; Ferracin, M. Interplay between small and long non-coding RNAs in cutaneous melanoma: A complex jigsaw puzzle with missing pieces. Mol. Oncol. 2019, 13, 74–98. [Google Scholar] [CrossRef]
- Broseghini, E.; Filippini, D.M.; Fabbri, L.; Leonardi, R.; Abeshi, A.; Dal Molin, D.; Fermi, M.; Ferracin, M.; Fernandez, I.J. Diagnostic and Prognostic Value of microRNAs in Patients with Laryngeal Cancer: A Systematic Review. Noncoding RNA 2023, 9, 9. [Google Scholar] [CrossRef]
- Laprovitera, N.; Riefolo, M.; Porcellini, E.; Durante, G.; Garajova, I.; Vasuri, F.; Aigelsreiter, A.; Dandachi, N.; Benvenuto, G.; Agostinis, F.; et al. MicroRNA expression profiling with a droplet digital PCR assay enables molecular diagnosis and prognosis of cancers of unknown primary. Mol. Oncol. 2021, 15, 2732–2751. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Case Description | ||
|---|---|---|
| Frequency * | Percentage | |
| General features | ||
| Publication Date | ||
| Before 2000 | 4 | 17.4 |
| 2000–2010 | 3 | 13 |
| 2011–2019 | 12 | 52.2 |
| After 2020 | 4 | 17.4 |
| Total | 23 | 100 |
| Country | ||
| Canada | 1 | 4.4 |
| China | 2 | 8.7 |
| Germany | 3 | 13 |
| India | 1 | 4.4 |
| Korea | 3 | 13 |
| Japan | 3 | 13 |
| Sweden | 2 | 8.7 |
| US | 7 | 30.4 |
| Multicenter (Germany, Italy and Spain) | 1 | 4.4 |
| Total | 23 | 100 |
| Study type | ||
| Prospective | 2 | 8.7 |
| Retrospective | 15 | 65.2 |
| Case report | 4 | 17.4 |
| Prospective and retrospective | 2 | 8.7 |
| Total | 23 | 100 |
| Frequency * | Percentage | |
|---|---|---|
| Biological sample | ||
| Histologic tumor tissue | 19 | 82.5 |
| Cytologic tumor tissue | 1 | 4.4 |
| Histologic and cytologic tumor tissue | 1 | 4.4 |
| Peripheral blood | 2 | 8.7 |
| Total | 23 | 100 |
| Quantification methods | ||
| Next generation sequencing or microarray | 1 | 3 |
| Real time quantitative PCR | 9 | 27.3 |
| Immunohistochemical staining | 13 | 39.4 |
| In situ hybridization (ISH) or fluorescent ISH (FISH) | 7 | 21.2 |
| Western blot or antibodies | 3 | 9.1 |
| Total ** | 33 | 100 |
| Type of molecular biomarkers | ||
| DNA | 9 | 25 |
| RNA | 7 | 19.4 |
| Protein | 20 | 55.6 |
| Total ** | 36 | 100 |
| Biomarkers list | ||
| p16 | 11 | 33.4 |
| HPV DNA | 7 | 21.2 |
| HPV RNA | 1 | 3 |
| Circulating HPV protein | 1 | 3 |
| EBV DNA/RNA | 4 | 12.2 |
| p53/p53 antibodies | 2 | 6.1 |
| Genetic panel assay | 2 | 6.1 |
| Ceramides (n = 4) | 1 | 3 |
| Salivary mRNA | 1 | 3 |
| VEGF | 1 | 3 |
| Rb | 1 | 3 |
| GATA 3 | 1 | 3 |
| Total ** | 33 | 100 |
| Biomarker | Disease-Free Survival | Overall Survival | RT Response | Chemo Response | Immunotherapy | Number of Paper(s) | Refs. |
|---|---|---|---|---|---|---|---|
| 92-gene assay | - | - | - | - | 1 ↑ | 1 | [26] |
| p53 antibodies | 1 ↓ | 1 ↓ | 1 ↓ | 1 | [28] | ||
| C(18)-ceramide | 1 ↓ | - | - | - | 1 | [27] |
| Biomarker | Sample Size | Diagnostic Association N° | Over-Expressed N° (%) | Down Regulated N° (%) | Refs * |
|---|---|---|---|---|---|
| p16 | 167/391 | 5/9 | 5/9 (55.5) | 0/9 | [23,25,30,37,41] |
| HPV DNA/RNA | 200/495 | 4/7 | 4/7 (57.1) | 0/7 | [23,25,35,38] |
| EBV DNA/RNA | 79/79 | 4/4 | 3/4 (75) | 1/4 (25) | [25,33,34,45] |
| P53/p53 antibodies | 63/63 | 2/2 | 1/2 (50) | 1/2 (50) | [23,28] |
| Genetic panel assay | 1214/1214 | 2/2 | - | - | [26,29] |
| Ceramides | 8/8 | 4/4 | 3/4 (75) | 1/4 (25) | [27] |
| Salivary mRNA | 1/1 | 1/1 | 1/1 (100) | 0 | [31] |
| VEGF | 50/50 | 1/1 | 0 | 1/1 (100) | [36] |
| Other | 1/ 37 | 2/2 | 1/2 (50) | 1/2 (50) | [24,32] |
| TOTAL | 1783 | 25/32 | 18/32 | 5/32 |
| Biomarker | Sample Size | Prognostic Association | Recurrence N° | OS N° | RT Response | Chemo Response | Refs. * |
|---|---|---|---|---|---|---|---|
| p16 | 336/358 | Yes 6/8 | 4 ↑ | 4 ↑ | 0 | 0 | [23,25,40,42,43,44] |
| HPV DNA/RNA | 353/495 | Yes 4/7 | 3 ↑ | 4 ↑ | 0 | 0 | [23,39,40,44] |
| EBV DNA/RNA | 0/79 | No 0/4 | 0 | 0 | 0 | 0 | |
| P53/p53 antibodies | 63/63 | Yes 2/2 | 1 ↓ | 1 ↓ | 1 ↓ | 1 ↓ | [23,28] |
| Genetic panel assay | 1183/1214 | Yes (predictive) 1/2 | 1 ↑ | - | 0 | 1 ↑ | [26] |
| Ceramides | 2/8 | Yes 1/4 | 0 | 1 ↓ | 0 | 0 | [27] |
| Salivary mRNA | 0/1 | No 0/1 | 0 | 0 | 0 | 0 | |
| VEGF | 0/50 | No 0/1 | 0 | 0 | 0 | 0 | |
| Other | 1/37 | Yes 1/2 | 1 ↓ | 1 ↓ | 0 | 0 | [24] |
| TOTAL | 790 | 14/31 | 9 | 11 | 1 | 2 |
| Marker | Sample Size | Oropharynx N (%) | Nasopharynx | Salivary Gland | Head and Neck (Generic) | Two or More Head and Neck Subsites | p Value |
|---|---|---|---|---|---|---|---|
| p16 | 167/391 | 5/9 (55.6) | 0 | 0 | 0 | 0 | 0.031 |
| HPV | 200/495 | 3/7 (42.8) | 0 | 0 | 0 | 1/7 (14.3) | 0.327 |
| EBV | 79/79 | 0 | 2/4 (50.0) | 0 | 2/4 (50.0) | 0 | <0.001 |
| p53/p53 antibodies | 63/63 | 1/2 (50.0) | 0 | 0 | 1/2 (50.0) | 0 | 0.477 |
| Genetic panel assay | 1214 /1214 | 0 | 0 | 0 | 2/2 (100) | 0 | - |
| Ceramides | 8/8 | 0 | 0 | 0 | 4/4 (100) | 0 | - |
| Salivary mRNA | 1/1 | 0 | 0 | 1/1 (100) | 0 | 0 | 0.053 |
| VEGF | 50/50 | 0 | 0 | 0 | 1/1 (100) | 0 | - |
| other | 1/1 | 0 | 0 | 1/2 (50.0) | 0 | 0 | - |
| Biomarker | Head and Neck Subsite | p Value | Odds Ratio (95% CI) |
|---|---|---|---|
| HPV-related biomarkers | Oropharynx | 0.015 | 2.71 (0.46–4.97) |
| EBV-related biomarkers | Nasopharynx | 0.012 | 4.04 (0.74–7.64) |
| Salivary-gland-related biomarkers | Salivary gland | 0.002 | 5.72 (1.59–9.84) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filippini, D.M.; Broseghini, E.; Carosi, F.; Molin, D.D.; Riefolo, M.; Fabbri, L.; Abeshi, A.; Fernandez, I.J.; Ferracin, M. A Systematic Review of Diagnostic and Prognostic Biomarkers for Head and Neck Cancer of Unknown Primary: An Unmet Clinical Need. Diagnostics 2023, 13, 1492. https://doi.org/10.3390/diagnostics13081492
Filippini DM, Broseghini E, Carosi F, Molin DD, Riefolo M, Fabbri L, Abeshi A, Fernandez IJ, Ferracin M. A Systematic Review of Diagnostic and Prognostic Biomarkers for Head and Neck Cancer of Unknown Primary: An Unmet Clinical Need. Diagnostics. 2023; 13(8):1492. https://doi.org/10.3390/diagnostics13081492
Chicago/Turabian StyleFilippini, Daria Maria, Elisabetta Broseghini, Francesca Carosi, Davide Dal Molin, Mattia Riefolo, Laura Fabbri, Andi Abeshi, Ignacio Javier Fernandez, and Manuela Ferracin. 2023. "A Systematic Review of Diagnostic and Prognostic Biomarkers for Head and Neck Cancer of Unknown Primary: An Unmet Clinical Need" Diagnostics 13, no. 8: 1492. https://doi.org/10.3390/diagnostics13081492