
Automatic Segmentation of Teeth, Crown–Bridge Restorations, Dental Implants, Restorative Fillings, Dental Caries, Residual Roots, and Root Canal Fillings on Orthopantomographs: Convenience and Pitfalls


Abstract
:1. Introduction
- Individuals with maxillofacial disorders or anatomical variations that are unable to maintain an upward spinal posture;
- Patients with severe Class II or Class III malocclusions (due to the inability to position both jaws within the focal trough at the same time);
- Due to difficulties situating the left and right sides of the face inside the focal trough because of facial skeletal asymmetry, only one side of the face may be clearly seen on the radiograph;
- Patients with moderate or severe periodontitis may find it difficult to bite the groove of the biting block. As mobile teeth have a tendency to tilt/move during biting, a cotton roll might be indicated to be put between the upper and lower incisors. Although this seems to be a solution for their acquisition, artefacts related to increased distance affect image quality;
- Even within the same OPG the image magnification changes, often because of anatomical variations and defects. The horizontal plane exhibits more distortion than the vertical plane, which might affect the interpretation of the OPG;
- The OPG’s diagnostic quality is impacted by the image’s tomographic characteristics. The focal trough measures approximately 20 mm in the lateral regions and 10 mm in the anterior area, and only those structures located inside the focal trough are clearly visible on an OPG. Any structures that will be examined outside of this focal trough might cause underdiagnosis;
- Due to superimpositions, bone loss and carious lesions that are localized at the interproximal areas cannot be demonstrated by OPG images. As those superimpositions are more common and problematic in the premolar region, even tooth segmentations may have lower success;
- Ghost images and double shadows are two of the phenomena of OPG imaging that drastically affect interpretation of radiographs.
2. Materials and Methods
- Presence of motion artefacts;
- Presence of removable dentures;
- Presence of fixed orthodontic appliances;
- Presence of ghost images due to glasses, earrings, piercings, and hearing aids;
- OPGs of edentulous patients;
- OPGs with positioning problems (head tilted downwards/upwards, head twisted to one side, head tipped, etc.).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Orhan, K.; Shamshiev, M.; Ezhov, M.; Plaksin, A.; Kurbanova, A.; Ünsal, G.; Gusarev, M.; Golitsyna, M.; Aksoy, S.; Mısırlı, M.; et al. AI-based automatic segmentation of craniomaxillofacial anatomy from CBCT scans for automatic detection of pharyngeal airway evaluations in OSA patients. Sci. Rep. 2022, 12, 11863. [Google Scholar] [CrossRef] [PubMed]
- Sin Akkaya, N.; Aksoy, S.; Orhan, K.; Öz, U. A deep learning algorithm proposal to automatic pharyngeal airway detection and segmentation on CBCT images. Orthod. Craniofacial Res. 2021, 24, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Willaert, R.; Degrieck, B.; Orhan, K.; Deferm, J.; Politis, C.; Shaheen, E.; Jacobs, R. Semi-automatic magnetic resonance imaging based orbital fat volumetry: Reliability and correlation with computed tomography. Int. J. Oral Maxillofac. Surg. 2021, 50, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Abbasi, M.S.; Zuberi, F.; Qamar, W.; Bin Halim, M.S.; Maqsood, A.; Alam, M.K. Artificial Intelligence Techniques: Analysis, Application, and Outcome in Dentistry—A Systematic Review. BioMed Res. Int. 2021, 2021, 9751564. [Google Scholar] [CrossRef]
- Carrillo-Perez, F.; Pecho, O.E.; Morales, J.C.; Paravina, R.D.; Della Bona, A.; Ghinea, R.; Pulgar, R.; Pérez, M.D.M.; Herrera, L.J. Applications of artificial intelligence in dentistry: A comprehensive review. J Esthet Restor Dent. 2022, 34, 259–280. [Google Scholar] [CrossRef]
- Chen, Y.-W.; Stanley, K.; Att, W. Artificial intelligence in dentistry: Current applications and future perspectives. Quintessence Int. 2020, 51, 248–257. [Google Scholar]
- Hung, K.; Montalvao, C.; Tanaka, R.; Kawai, T.; Bornstein, M.M. The use and performance of artificial intelligence applications in dental and maxillofacial radiology: A systematic review. Dentomaxillofacial Radiol. 2020, 49, 20190107. [Google Scholar] [CrossRef]
- Issa, J.; Olszewski, R.; Dyszkiewicz-Konwińska, M. The Effectiveness of Semi-Automated and Fully Automatic Segmentation for Inferior Alveolar Canal Localization on CBCT Scans: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 560. [Google Scholar] [CrossRef]
- Wiederhold, G.; McCarthy, J. Arthur Samuel: Pioneer in Machine Learning. IBM J. Res. Dev. 1992, 36, 329–331. [Google Scholar] [CrossRef]
- Hsu, K.; Yuh, D.-Y.; Lin, S.-C.; Lyu, P.-S.; Pan, G.-X.; Zhuang, Y.-C.; Chang, C.-C.; Peng, H.-H.; Lee, T.-Y.; Juan, C.-H.; et al. Improving performance of deep learning models using 3.5D U-Net via majority voting for tooth segmentation on cone beam computed tomography. Sci. Rep. 2022, 12, 19809. [Google Scholar] [CrossRef]
- Ariji, Y.; Gotoh, M.; Fukuda, M.; Watanabe, S.; Nagao, T.; Katsumata, A.; Ariji, E. A preliminary deep learning study on automatic segmentation of contrast-enhanced bolus in videofluorography of swallowing. Sci. Rep. 2022, 12, 18754. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Jeon, K.J.; Kim, Y.H.; Ha, E.-G.; Lee, C.; Han, S.-S. Deep learning-based fully automatic segmentation of the maxillary sinus on cone-beam computed tomographic images. Sci. Rep. 2022, 12, 14009. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Kim, S.; Zhou, J.; Metaxas, D.; Rajagopal, G.; Yue, N. 3D Meshless Prostate Segmentation and Registration in Image Guided Radiotherapy. Med. Image Comput. Comput. Assist. Interv. 2009, 12, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Aliaga, I.; Vera, V.; Vera, M.; García, E.; Pedrera, M.; Pajares, G. Automatic computation of mandibular indices in dental panoramic radiographs for early osteoporosis detection. Artif. Intell. Med. 2020, 103, 101816. [Google Scholar] [CrossRef]
- van Ginneken, B.; Katsuragawa, S.; Romeny, B.T.H.; Doi, K.; Viergever, M. Automatic detection of abnormalities in chest radiographs using local texture analysis. IEEE Trans. Med. Imaging 2002, 21, 139–149. [Google Scholar] [CrossRef]
- Rueda, S.; Gil, J.A.; Pichery, R.; Alcaniz, M. Automatic Segmentation of Jaw Tissues in CT Using Active Appearance Models and Semi-automatic Landmarking. Med. Image Comput. Comput. Assist. Interv. 2006, 9, 167–174. [Google Scholar] [CrossRef]
- Chifor, R.; Hotoleanu, M.; Marita, T.; Arsenescu, T.; Socaciu, M.A.; Badea, I.C.; Chifor, I. Automatic Segmentation of Periodontal Tissue Ultrasound Images with Artificial Intelligence: A Novel Method for Improving Dataset Quality. Sensors 2022, 22, 7101. [Google Scholar] [CrossRef]
- Nogueira-Reis, F.; Morgan, N.; Nomidis, S.; Van Gerven, A.; Oliveira-Santos, N.; Jacobs, R.; Tabchoury, C.P.M. Three-dimensional maxillary virtual patient creation by convolutional neural network-based segmentation on cone-beam computed tomography images. Clin. Oral Investig. 2022, 27, 1133–1141. [Google Scholar] [CrossRef]
- Alqahtani, K.A.; Jacobs, R.; Smolders, A.; Van Gerven, A.; Willems, H.; Shujaat, S.; Shaheen, E. Deep convolutional neural network-based automated segmentation and classification of teeth with orthodontic brackets on cone-beam computed-tomographic images: A validation study. Eur. J. Orthod. 2022, 45, 169–174. [Google Scholar] [CrossRef]
- Cho, H.-N.; Gwon, E.; Kim, K.-A.; Baek, S.-H.; Kim, N.; Kim, S.-J. Accuracy of convolutional neural networks-based automatic segmentation of pharyngeal airway sections according to craniofacial skeletal pattern. Am. J. Orthod. Dentofac. Orthop. 2022, 162, e53–e62. [Google Scholar] [CrossRef]
- Morgan, N.; Van Gerven, A.; Smolders, A.; Vasconcelos, K.D.F.; Willems, H.; Jacobs, R. Convolutional neural network for automatic maxillary sinus segmentation on cone-beam computed tomographic images. Sci. Rep. 2022, 12, 7523. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Kittaka, M.; He, Y.; Zhang, Y.; Ueki, Y.; Kihara, D. OC_Finder: Osteoclast Segmentation, Counting, and Classification Using Watershed and Deep Learning. Front. Bioinform. 2022, 2, 819570. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Fang, Y.; Mei, L.; Zhang, B.; Yu, B.; Liu, J.; Jiang, C.; Sun, Y.; Ma, L.; Huang, J.; et al. A fully automatic AI system for tooth and alveolar bone segmentation from cone-beam CT images. Nat. Commun. 2022, 13, 2096. [Google Scholar] [CrossRef]
- Adışen, M.Z.; Aydoğdu, M. Comparison of mastoid air cell volume in patients with or without a pneumatized articular tubercle. Imaging Sci. Dent. 2022, 52, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, J.-E. Evaluating the Precision of Automatic Segmentation of Teeth, Gingiva and Facial Landmarks for 2D Digital Smile Design Using Real-Time Instance Segmentation Network. J. Clin. Med. 2022, 11, 852. [Google Scholar] [CrossRef]
- Dot, G.; Schouman, T.; Dubois, G.; Rouch, P.; Gajny, L. Fully automatic segmentation of craniomaxillofacial CT scans for computer-assisted orthognathic surgery planning using the nnU-Net framework. Eur. Radiol. 2022, 32, 3639–3648. [Google Scholar] [CrossRef]
- Nozawa, M.; Ito, H.; Ariji, Y.; Fukuda, M.; Igarashi, C.; Nishiyama, M.; Ogi, N.; Katsumata, A.; Kobayashi, K.; Ariji, E. Automatic segmentation of the temporomandibular joint disc on magnetic resonance images using a deep learning technique. Dentomaxillofacial Radiol. 2022, 51, 20210185. [Google Scholar] [CrossRef]
- Ararat, E.; Yalcin, E.D. Morphometric and volumetric evaluation of maxillary sinus in patients with chronic obstructive pulmonary disease using cone-beam CT. Oral Radiol. 2022, 38, 261–268. [Google Scholar] [CrossRef]
- Jang, T.J.; Kim, K.C.; Cho, H.C.; Seo, J.K. A fully automated method for 3D individual tooth identification and segmentation in dental CBCT. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 44, 6562–6568. [Google Scholar] [CrossRef]
- Kwak, G.H.; Kwak, E.-J.; Song, J.M.; Park, H.R.; Jung, Y.-H.; Cho, B.-H.; Hui, P.; Hwang, J.J. Automatic mandibular canal detection using a deep convolutional neural network. Sci. Rep. 2020, 10, 5711. [Google Scholar] [CrossRef]
- Schneider, L.; Arsiwala-Scheppach, L.; Krois, J.; Meyer-Lueckel, H.; Bressem, K.; Niehues, S.; Schwendicke, F. Benchmarking Deep Learning Models for Tooth Structure Segmentation. J. Dent. Res. 2022, 101, 1343–1349. [Google Scholar] [CrossRef] [PubMed]
- Moses, D.A. Deep learning applied to automatic disease detection using chest X-rays. J. Med. Imaging Radiat. Oncol. 2021, 65, 498–517. [Google Scholar] [CrossRef]
- Morgan, N.; Shujaat, S.; Jazil, O.; Jacobs, R. Three-dimensional quantification of skeletal midfacial complex symmetry. Int. J. Comput. Assist. Radiol. Surg. 2022, 18, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Kajor, M.; Kucharski, D.; Grochala, J.; Loster, J.E. New Methods for the Acoustic-Signal Segmentation of the Temporomandibular Joint. J. Clin. Med. 2022, 11, 2706. [Google Scholar] [CrossRef]
- Li, C.; Chen, H.; Wang, Y.; Sun, Y.C. Labelling, segmentation and application of neural network based on machine learning of three-dimensional intraoral anatomical features. Zhonghua Kou Qiang Yi Xue Za Zhi 2022, 57, 540–546. [Google Scholar]
- Xu, J.; Liu, J.; Zhang, D.; Zhou, Z.; Zhang, C.; Chen, X. A 3D segmentation network of mandible from CT scan with combination of multiple convolutional modules and edge supervision in mandibular reconstruction. Comput. Biol. Med. 2021, 138, 104925. [Google Scholar] [CrossRef]
- Giudice, A.L.; Ronsivalle, V.; Spampinato, C.; Leonardi, R. Fully automatic segmentation of the mandible based on convolutional neural networks (CNNs). Orthod. Craniofacial Res. 2021, 24, 100–107. [Google Scholar] [CrossRef]
- Kim, Y.H.; Shin, J.Y.; Lee, A.; Park, S.; Han, S.-S.; Hwang, H.J. Automated cortical thickness measurement of the mandibular condyle head on CBCT images using a deep learning method. Sci. Rep. 2021, 11, 14852. [Google Scholar] [CrossRef]
- Leonardi, R.; Giudice, A.L.; Farronato, M.; Ronsivalle, V.; Allegrini, S.; Musumeci, G.; Spampinato, C. Fully automatic segmentation of sinonasal cavity and pharyngeal airway based on convolutional neural networks. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 824–835.e1. [Google Scholar] [CrossRef]
- Islam, N.M.; Laughter, L.; Sadid-Zadeh, R.; Smith, C.; Dolan, T.A.; Crain, G.; Squarize, C.H. Adopting artificial intelligence in dental education: A model for academic leadership and innovation. J. Dent. Educ. 2022, 86, 1545–1551. [Google Scholar] [CrossRef]
- Schwendicke, F.; Chaurasia, A.; Wiegand, T.; Uribe, S.E.; Fontana, M.; Akota, I.; Tryfonos, O.; Krois, J. Artificial intelligence for oral and dental healthcare: Core education curriculum. J. Dent. 2023, 128, 104363. [Google Scholar] [CrossRef] [PubMed]
- Saghiri, M.A.; Bs, J.V.; Nadershahi, N. Scoping review of artificial intelligence and immersive digital tools in dental education. J. Dent. Educ. 2021, 86, 736–750. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.; Noguchi, N.; Matsuka, Y.; Shinohara, C.; Kimura, T.; Oka, K.; Okura, K.; Rodis, O.M.M.; Kawano, F. Educational effects using a robot patient simulation system for development of clinical attitude. Eur. J. Dent. Educ. 2017, 22, e327–e336. [Google Scholar] [CrossRef] [PubMed]
- Abouzeid, H.L.; Chaturvedi, S.; Abdelaziz, K.M.; Alzahrani, F.A.; AlQarni, A.A.S.; Alqahtani, N.M. Role of Robotics and Artificial Intelligence in Oral Health and Preventive Dentistry—Knowledge, Perception and Attitude of Dentists. Oral Health Prev. Dent 2021, 19, 353–363. [Google Scholar]
- Khanagar, S.B.; Al-Ehaideb, A.; Maganur, P.C.; Vishwanathaiah, S.; Patil, S.; Baeshen, H.A.; Sarode, S.C.; Bhandi, S. Developments, application, and performance of artificial intelligence in dentistry—A systematic review. J. Dent. Sci. 2021, 16, 508–522. [Google Scholar] [CrossRef]
- Seguin, D.; Pac, S.; Wang, J.; Nicolson, R.; Martinez-Trujillo, J.; Duerden, E.G. Amygdala subnuclei development in adolescents with autism spectrum disorder: Association with social communication and repetitive behaviors. Brain Behav. 2021, 11, e2299. [Google Scholar] [CrossRef]
- Cheng, B.; Wang, W. Dental hard tissue morphological segmentation with sparse representation-based classifier. Med. Biol. Eng. Comput. 2019, 57, 1629–1643. [Google Scholar] [CrossRef]
- Xu, T.; Tay, F.R.; Gutmann, J.L.; Fan, B.; Fan, W.; Huang, Z.; Sun, Q. Micro–Computed Tomography Assessment of Apical Accessory Canal Morphologies. J. Endod. 2016, 42, 798–802. [Google Scholar] [CrossRef]
- Seipel, S.; Wagner, I.-V.; Koch, S.; Schneider, W. Three-dimensional visualization of the mandible: A new method for presenting the periodontal status and diseases. Comput. Methods Programs Biomed. 1995, 46, 51–57. [Google Scholar] [CrossRef]
- Ma, L.; Wang, Y.; Guo, L.; Zhang, Y.; Wang, P.; Pei, X.; Qian, L.; Jaeger, S.; Ke, X.; Yin, X.; et al. Developing and verifying automatic detection of active pulmonary tuberculosis from multi-slice spiral CT images based on deep learning. J. X-Ray Sci. Technol. 2020, 28, 939–951. [Google Scholar] [CrossRef]
- Zurac, S.; Mogodici, C.; Poncu, T.; Trăscău, M.; Popp, C.; Nichita, L.; Cioplea, M.; Ceachi, B.; Sticlaru, L.; Cioroianu, A.; et al. A New Artificial Intelligence-Based Method for Identifying Mycobacterium Tuberculosis in Ziehl–Neelsen Stain on Tissue. Diagnostics 2022, 12, 1484. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.; Wang, L.; Lin, J.; Xu, J.; Zhang, T.; Qi, J.; Li, X.; Ni, W.; Wu, G.; Huang, J.; et al. A fully automatic artificial intelligence-based CT image analysis system for accurate detection, diagnosis, and quantitative severity evaluation of pulmonary tuberculosis. Eur. Radiol. 2022, 32, 2188–2199. [Google Scholar] [CrossRef] [PubMed]
- Hegde, S.; Ajila, V.; Zhu, W.; Zeng, C. Artificial intelligence in early diagnosis and prevention of oral cancer. Asia-Pacific, J. Oncol. Nurs. 2022, 9, 100133. [Google Scholar] [CrossRef]
- Chen, W.; Zeng, R.; Jin, Y.; Sun, X.; Zhou, Z.; Zhu, C. Artificial Neural Network Assisted Cancer Risk Prediction of Oral Precancerous Lesions. BioMed. Res. Int. 2022, 2022, 7352489. [Google Scholar] [CrossRef] [PubMed]
- Tobias, M.A.S.; Nogueira, B.P.; Santana, M.C.; Pires, R.G.; Papa, J.P.; Santos, P.S. Artificial intelligence for oral cancer diagnosis: What are the possibilities? Oral Oncol. 2022, 134, 106117. [Google Scholar] [CrossRef]
- Kolokythas, A. Can Artificial Intelligence (AI) assist in the diagnosis of oral mucosal lesions and/or oral cancer? Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2022, 134, 413–414. [Google Scholar] [CrossRef]
- Sarode, G.S.; Kumari, N.; Sarode, S.C. Oral cancer histopathology images and artificial intelligence: A pathologist’s perspective. Oral Oncol. 2022, 132, 105999. [Google Scholar] [CrossRef]
- Al-Rawi, N.; Sultan, A.; Rajai, B.; Shuaeeb, H.; Alnajjar, M.; Alketbi, M.; Mohammad, Y.; Shetty, S.R.; Mashrah, M.A. The Effectiveness of Artificial Intelligence in Detection of Oral Cancer. Int. Dent. J. 2022, 72, 436–447. [Google Scholar] [CrossRef]
- Ramezani, K.; Tofangchiha, M. Oral Cancer Screening by Artificial Intelligence-Oriented Interpretation of Optical Coherence Tomography Images. Radiol. Res. Pr. 2022, 2022, 1–10. [Google Scholar] [CrossRef]
- Rai, R.; Vats, R.; Kumar, M. Detecting Oral Cancer: The Potential of Artificial Intelligence. Curr. Med. Imaging. 2022, 18, 919–923. [Google Scholar] [CrossRef]
- Baniulyte, G.; Ali, K. Artificial intelligence—Can it be used to outsmart oral cancer? Evid. Based Dent. 2022, 23, 12–13. [Google Scholar] [CrossRef] [PubMed]
- García-Pola, M.; Pons-Fuster, E.; Suárez-Fernández, C.; Seoane-Romero, J.; Romero-Méndez, A.; López-Jornet, P. Role of Artificial Intelligence in the Early Diagnosis of Oral Cancer. A Scoping Review. Cancers 2021, 13, 4600. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Francesco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253–262. [Google Scholar] [CrossRef]
- Bayrakdar, I.S.; Orhan, K.; Çelik, Ö.; Bilgir, E.; Sağlam, H.; Kaplan, F.A.; Görür, S.A.; Odabaş, A.; Aslan, A.F.; Różyło-Kalinowska, I. A U-Net Approach to Apical Lesion Segmentation on Panoramic Radiographs. BioMed. Res. Int. 2022, 2022, 7035367. [Google Scholar] [CrossRef]
- Kim, J.; Hwang, J.J.; Jeong, T.; Cho, B.-H.; Shin, J. Deep learning-based identification of mesiodens using automatic maxillary anterior region estimation in panoramic radiography of children. Dentomaxillofac. Radiol. 2022, 51, 7. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Yu, H.; Zhang, F.; Cao, Z.; Wu, F.; Zhu, F. Automatic segmentation and detection of ectopic eruption of first permanent molars on panoramic radiographs based on nnU-Net. Int. J. Paediatr Dent. 2022, 32, 785–792. [Google Scholar] [CrossRef]
- Sheng, C.; Wang, L.; Huang, Z.; Wang, T.; Guo, Y.; Hou, W.; Xu, L.; Wang, J.; Yan, X. Transformer-Based Deep Learning Network for Tooth Segmentation on Panoramic Radiographs. J. Syst. Sci. Complex. 2022, 36, 257–272. [Google Scholar] [CrossRef]
- Leite, A.F.; Van Gerven, A.; Willems, H.; Beznik, T.; Lahoud, P.; Gaêta-Araujo, H.; Vranckx, M.; Jacobs, R. Artificial intelligence-driven novel tool for tooth detection and segmentation on panoramic radiographs. Clin. Oral Investig. 2020, 25, 2257–2267. [Google Scholar] [CrossRef]
- Giudice, A.L.; Ronsivalle, V.; Gastaldi, G.; Leonardi, R. Assessment of the accuracy of imaging software for 3D rendering of the upper airway, usable in orthodontic and craniofacial clinical settings. Prog. Orthod. 2022, 23, 22. [Google Scholar] [CrossRef]
- Szentimrey, Z.; de Ribaupierre, S.; Fenster, A.; Ukwatta, E. Automated 3D U-net based segmentation of neonatal cerebral ventricles from 3D ultrasound images. Med. Phys. 2021, 49, 1034–1046. [Google Scholar] [CrossRef]
- Groves, L.A.; VanBerlo, B.; Veinberg, N.; Alboog, A.; Peters, T.M.; Chen, E.C.S. Automatic segmentation of the carotid artery and internal jugular vein from 2D ultrasound images for 3D vascular reconstruction. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 1835–1846. [Google Scholar] [CrossRef]
- De Rosa, C.S.; Bergamini, M.L.; Palmieri, M.; Sarmento, D.J.D.S.; de Carvalho, M.O.; Ricardo, A.L.F.; Hasseus, B.; Jonasson, P.; Braz-Silva, P.H.; Costa, A.L.F. Differentiation of periapical granuloma from radicular cyst using cone beam computed tomography images texture analysis. Heliyon 2020, 6, E05194. [Google Scholar] [CrossRef]
- Kim, J.J.; Nam, H.; Kaipatur, N.R.; Major, P.W.; Flores-Mir, C.; Lagravere, M.O.; Romanyk, D.L. Reliability and accuracy of segmentation of mandibular condyles from different three-dimensional imaging modalities: A systematic review. Dentomaxillofac. Radiol. 2020, 49, 20190150. [Google Scholar] [CrossRef]
- Wallner, J.; Schwaiger, M.; Hochegger, K.; Gsaxner, C.; Zemann, W.; Egger, J. A review on multiplatform evaluations of semi-automatic open-source based image segmentation for cranio-maxillofacial surgery. Comput. Methods Programs Biomed. 2019, 182, 105102. [Google Scholar] [CrossRef]
- Xi, T.; Schreurs, R.; Heerink, W.; Bergé, S.J.; Maal, T.J.J. A Novel Region-Growing Based Semi-Automatic Segmentation Protocol for Three-Dimensional Condylar Reconstruction Using Cone Beam Computed Tomography (CBCT). PLoS ONE 2014, 9, e111126. [Google Scholar] [CrossRef]
- Nsal, G.; Orhan, K. Deep Learning and Artificial Intelligence Applications in Dentomaxillofacial Radiology. In Applied Machine Learning and Multi-Criteria, Özşahin, D., Özşahin, I., eds.; Bentham Science Publishers: Sharjah, United Arab Emirates, 2021; pp. 126–140. [Google Scholar]
- Perschbacher, S. Interpretation of panoramic radiographs. Aust. Dent. J. 2012, 57, 40–45. [Google Scholar] [CrossRef]
- Różyło-Kalinowska, I. Panoramic radiography in dentistry. Clin. Dent. Rev. 2021, 5, 26. [Google Scholar] [CrossRef]
- Arsiwala-Scheppach, L.T.; Chaurasia, A.; Müller, A.; Krois, J.; Schwendicke, F. Machine Learning in Dentistry: A Scoping Review. J. Clin. Med. 2023, 12, 937. [Google Scholar] [CrossRef]
- Zou, K.H.; Warfield, S.; Bharatha, A.; Tempany, C.M.; Kaus, M.R.; Haker, S.J.; Wells, W.M.; Jolesz, F.A.; Kikinis, R. Statistical validation of image segmentation quality based on a spatial overlap index1: Scientific reports. Acad. Radiol. 2004, 11, 178–189. [Google Scholar] [CrossRef]
- Ye, J. Multicriteria decision-making method using the Dice similarity measure based on the reduct intuitionistic fuzzy sets of interval-valued intuitionistic fuzzy sets. Appl. Math. Model. 2012, 36, 4466–4472. [Google Scholar] [CrossRef]
- Hou, S.; Zhou, T.; Liu, Y.; Dang, P.; Lu, H.; Shi, H. Teeth U-Net: A segmentation model of dental panoramic X-ray images for context semantics and contrast enhancement. Comput. Biol. Med. 2023, 152, 106296. [Google Scholar] [CrossRef]
- Lin, X.; Fu, Y.; Ren, G.; Yang, X.; Duan, W.; Chen, Y.; Zhang, Q. Micro–Computed Tomography–Guided Artificial Intelligence for Pulp Cavity and Tooth Segmentation on Cone-beam Computed Tomography. J. Endod. 2021, 47, 1933–1941. [Google Scholar] [CrossRef]
- Nishitani, Y.; Nakayama, R.; Hayashi, D.; Hizukuri, A.; Murata, K. Segmentation of teeth in panoramic dental X-ray images using U-Net with a loss function weighted on the tooth edge. Radiol. Phys. Technol. 2021, 14, 64–69. [Google Scholar] [CrossRef]
- Shaheen, E.; Leite, A.; Alqahtani, K.A.; Smolders, A.; Van Gerven, A.; Willems, H.; Jacobs, R. A novel deep learning system for multi-class tooth segmentation and classification on cone beam computed tomography. A validation study. J. Dent. 2021, 115, 103865. [Google Scholar] [CrossRef]
- Zhang, J.; Xia, W.; Dong, J.; Tang, Z.; Zhao, Q. Root Canal Segmentation in CBCT Images by 3D U-Net with Global and Local Combination Loss. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Mexico, 1–5 November 2021; pp. 3097–3100. [Google Scholar] [CrossRef]
- Fowler, P. Limitations of the panoramic radiograph’s focal trough: A case report. N Dent. J. 1991, 87, 92–93. [Google Scholar]
- Lopes, L.J.; Gamba, T.O.; Bertinato, J.V.J.; Freitas, D. Comparison of panoramic radiography and CBCT to identify maxillary posterior roots invading the maxillary sinus. Dentomaxillofacial Radiol. 2016, 45, 20160043. [Google Scholar] [CrossRef]
- Ohba, T.; Ogawa, Y.; Shinohara, Y.; Hiromatsu, T.; Uchida, A.; Toyoda, Y. Limitations of panoramic radiography in the detection of bone defects in the posterior wall of the maxillary sinus: An experimental study. Dentomaxillofac. Radiol. 1994, 23, 149–153. [Google Scholar] [CrossRef]
- Nakagawa, Y.; Ishii, H.; Nomura, Y.; Watanabe, N.Y.; Hoshiba, D.; Kobayashi, K.; Ishibashi, K. Third Molar Position: Reliability of Panoramic Radiography. J. Oral Maxillofac. Surg. 2007, 65, 1303–1308. [Google Scholar] [CrossRef]
- Abdalla-Aslan, R.; Yeshua, T.; Kabla, D.; Leichter, I.; Nadler, C. An artificial intelligence system using machine-learning for automatic detection and classification of dental restorations in panoramic radiography. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 593–602. [Google Scholar] [CrossRef]
- Kuwada, C.; Ariji, Y.; Fukuda, M.; Kise, Y.; Fujita, H.; Katsumata, A.; Ariji, E. Deep learning systems for detecting and classifying the presence of impacted supernumerary teeth in the maxillary incisor region on panoramic radiographs. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 464–469. [Google Scholar] [CrossRef]
- Revilla-León, M.; Gómez-Polo, M.; Vyas, S.; Barmak, A.B.; Özcan, M.; Att, W.; Krishnamurthy, V.R. Artificial intelligence applications in restorative dentistry: A systematic review. J. Prosthet. Dent. 2021, 128, 867–875. [Google Scholar] [CrossRef]
- Bayraktar, Y.; Ayan, E. Diagnosis of interproximal caries lesions with deep convolutional neural network in digital bitewing radiographs. Clin. Oral Investig. 2022, 26, 623–632. [Google Scholar] [CrossRef]
- Fontenele, R.C.; Gerhardt, M.D.N.; Pinto, J.C.; Van Gerven, A.; Willems, H.; Jacobs, R.; Freitas, D.Q. Influence of dental fillings and tooth type on the performance of a novel artificial intelligence-driven tool for automatic tooth segmentation on CBCT images—A validation study. J. Dent. 2022, 119, 104069. [Google Scholar] [CrossRef]
- Ying, S.; Wang, B.; Zhu, H.; Liu, W.; Huang, F. Caries segmentation on tooth X-ray images with a deep network. J. Dent. 2022, 119, 104076. [Google Scholar] [CrossRef]
- Eelbode, T.; Bertels, J.; Berman, M.; Vandermeulen, D.; Maes, F.; Bisschops, R.; Blaschko, M.B. Optimization for Medical Image Segmentation: Theory and Practice When Evaluating with Dice Score or Jaccard Index. IEEE Trans. Med. Imaging 2020, 39, 3679–3690. [Google Scholar] [CrossRef]
- Feng, H.; Fu, Z.; Wang, Y.; Zhang, P.; Lai, H.; Zhao, J. Automatic segmentation of thrombosed aortic dissection in post-operative CT-angiography images. Med. Phys. 2022. [Google Scholar] [CrossRef]
- Lei, S.; Zhang, H.; Wang, K.; Su, Z. How Training Data Affect the Accuracy and Robustness of Neural Networks for Image Classification; ICLR: New Orleans, LA, USA, 2019. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structure | DSC |
|---|---|
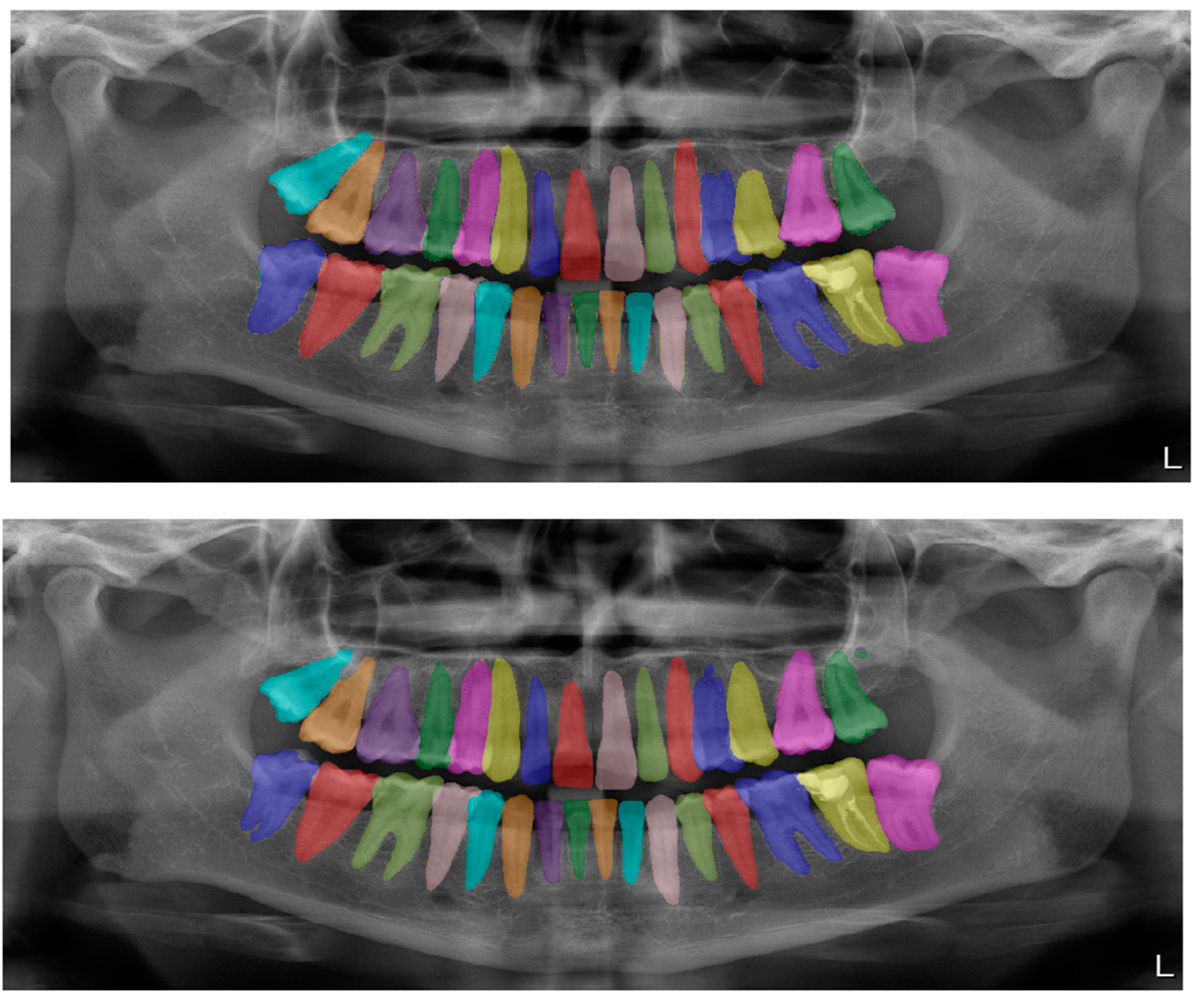
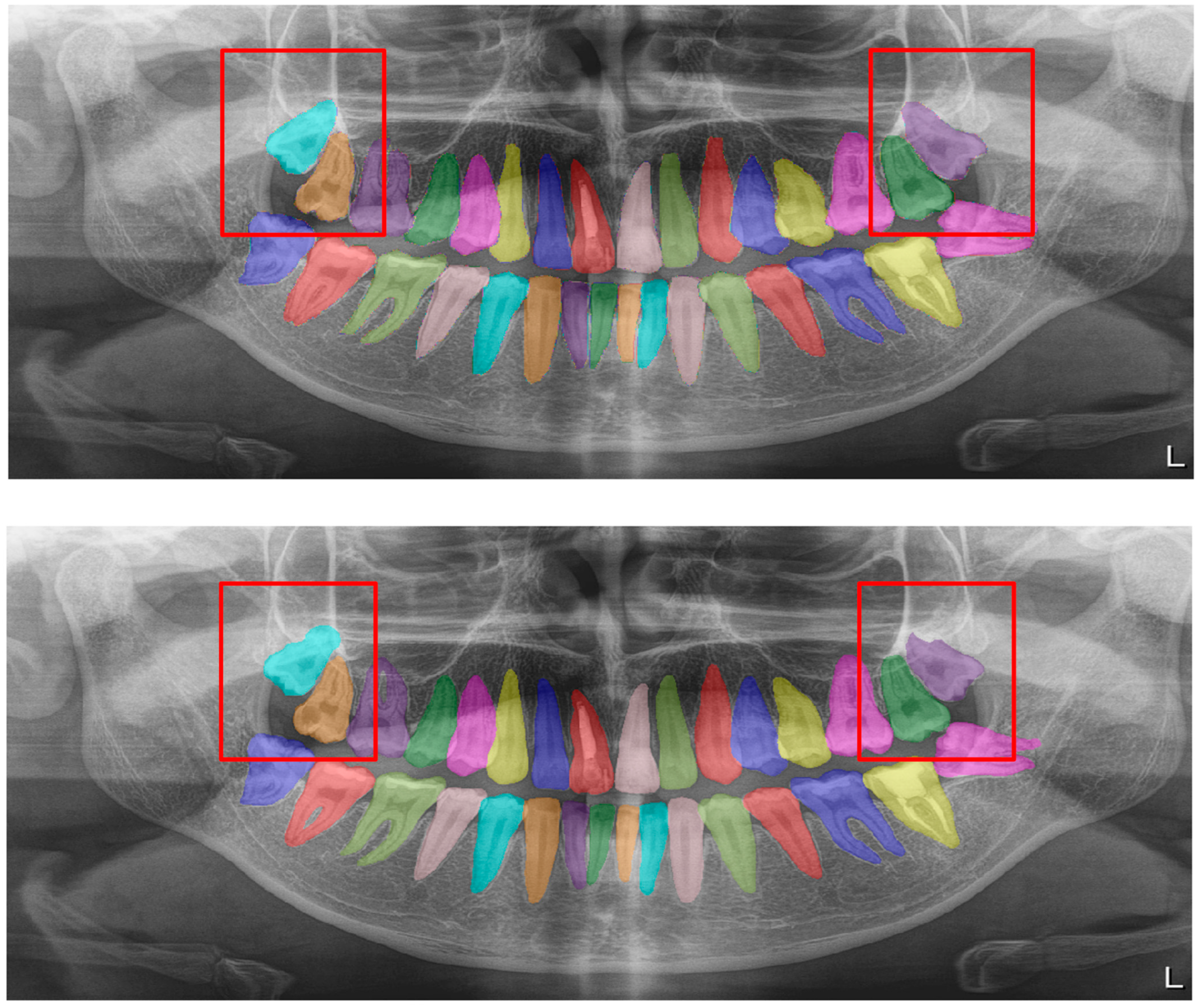
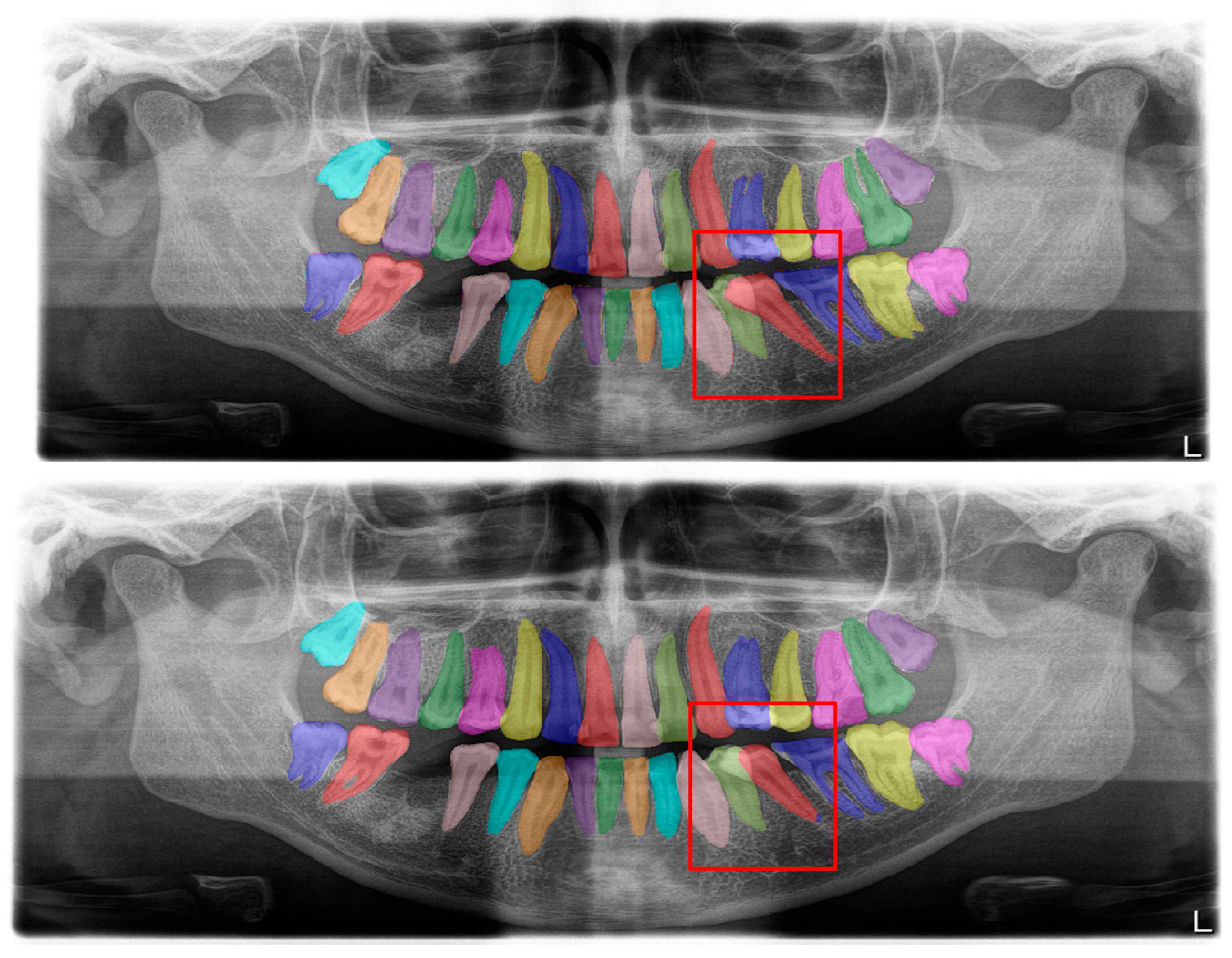
| Tooth segmentation (Figure 2) | 0.95 |
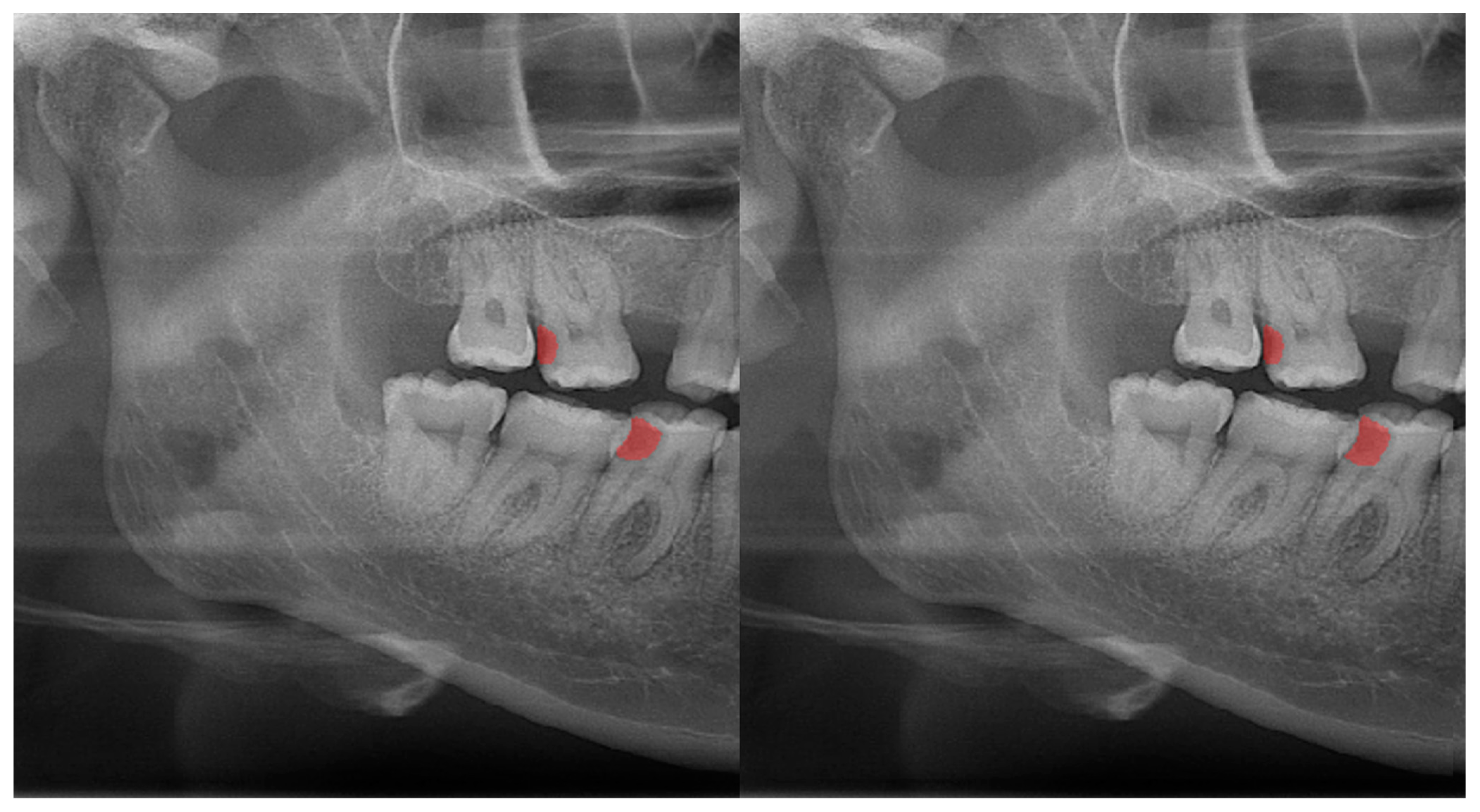
| Dental caries (Figure 3) | 0.88 |
| Dental restoration | 0.87 |
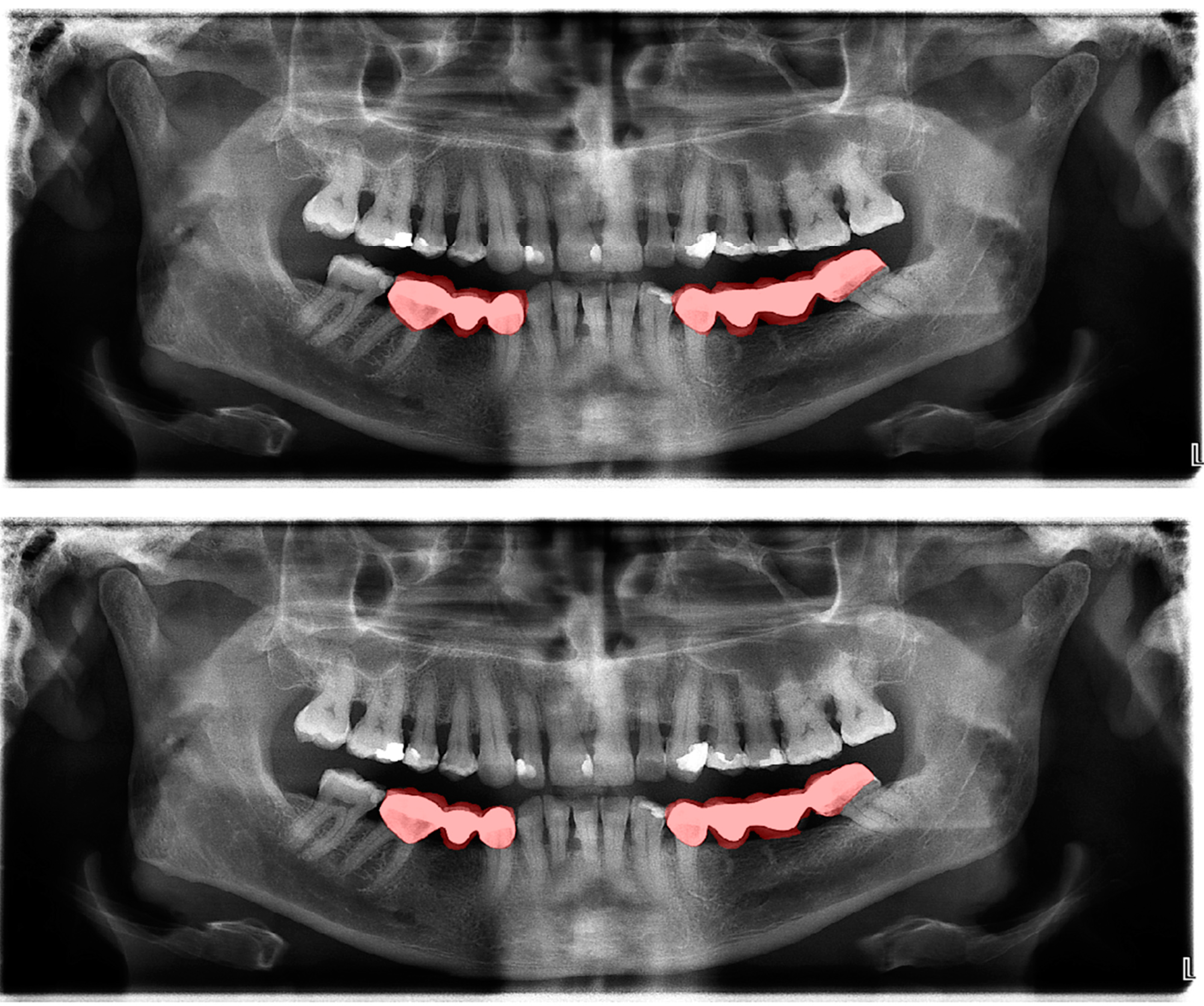
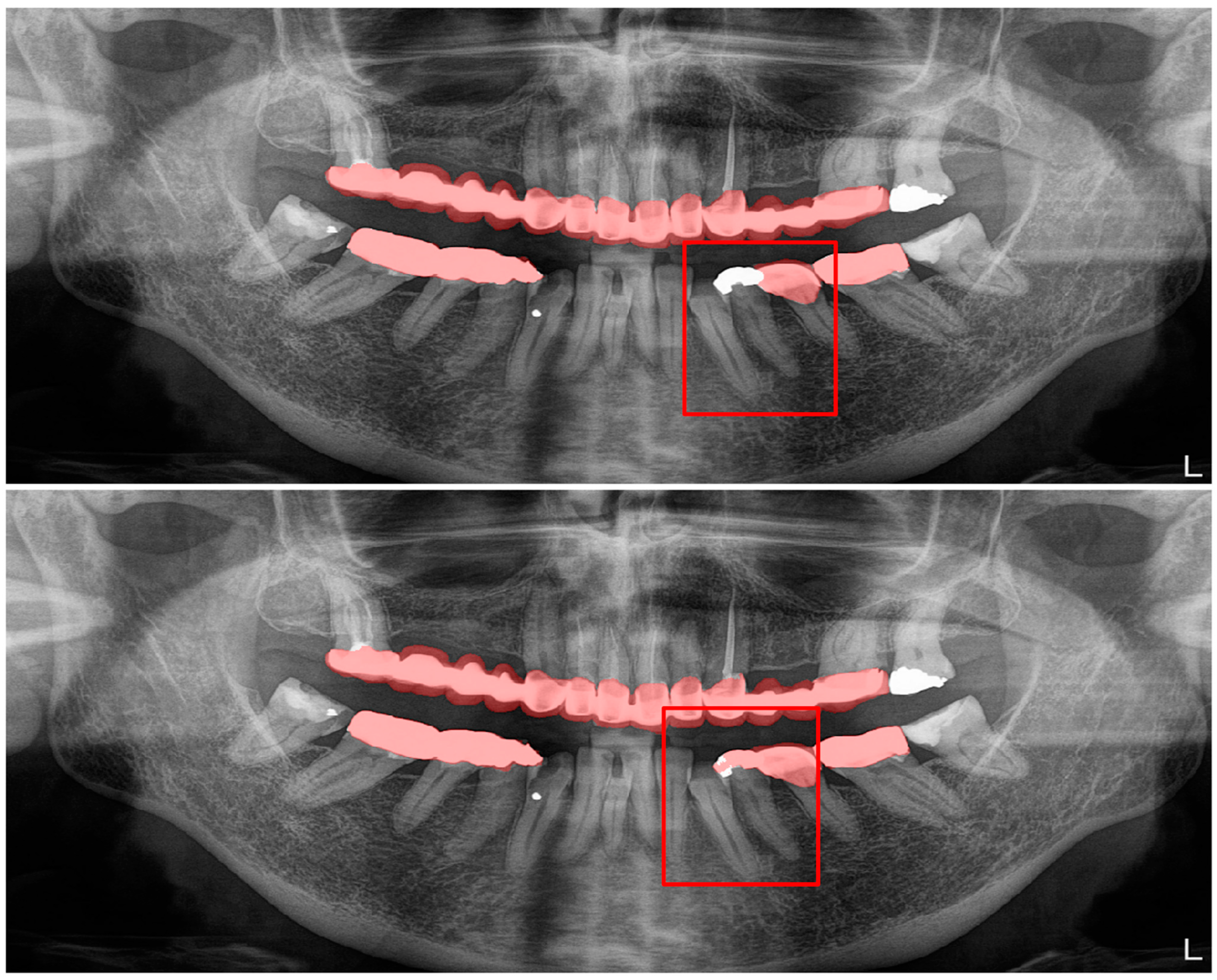
| Crown–bridge restorations (Figure 4) | 0.93 |
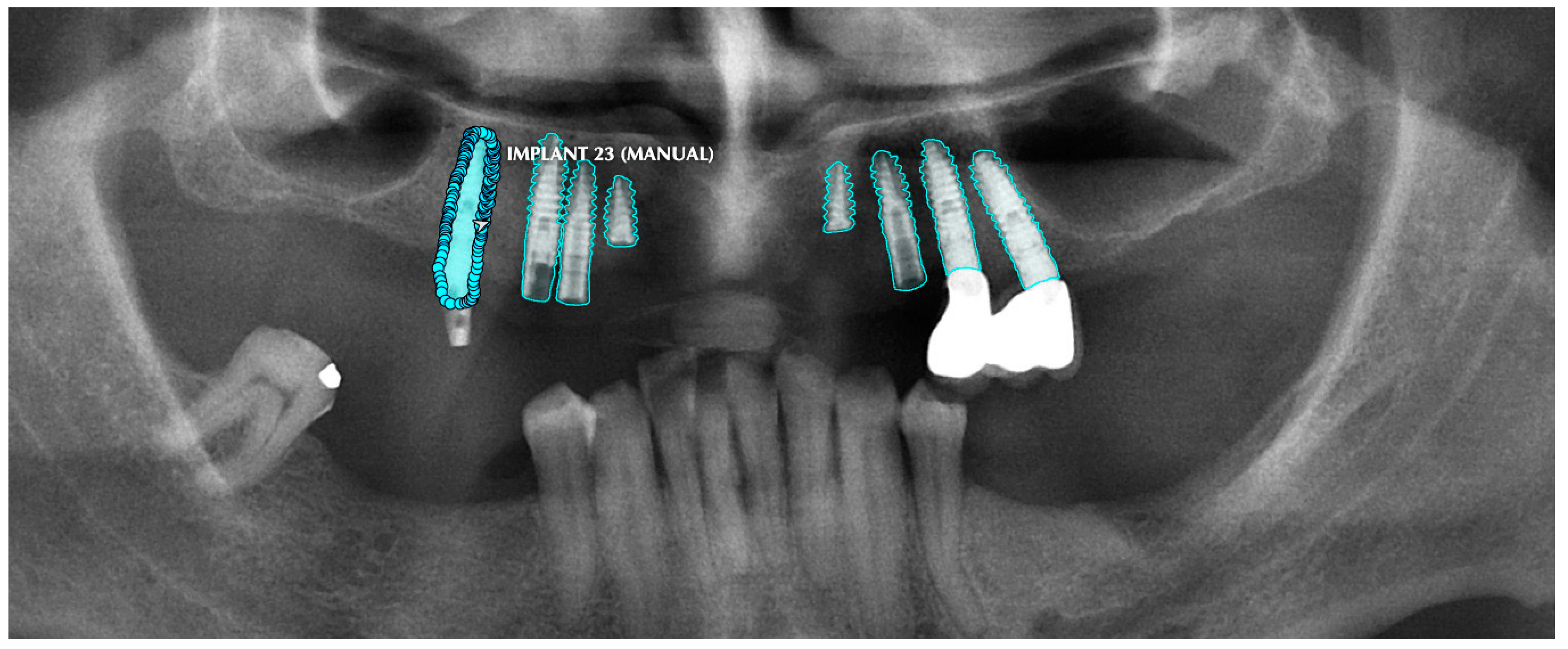
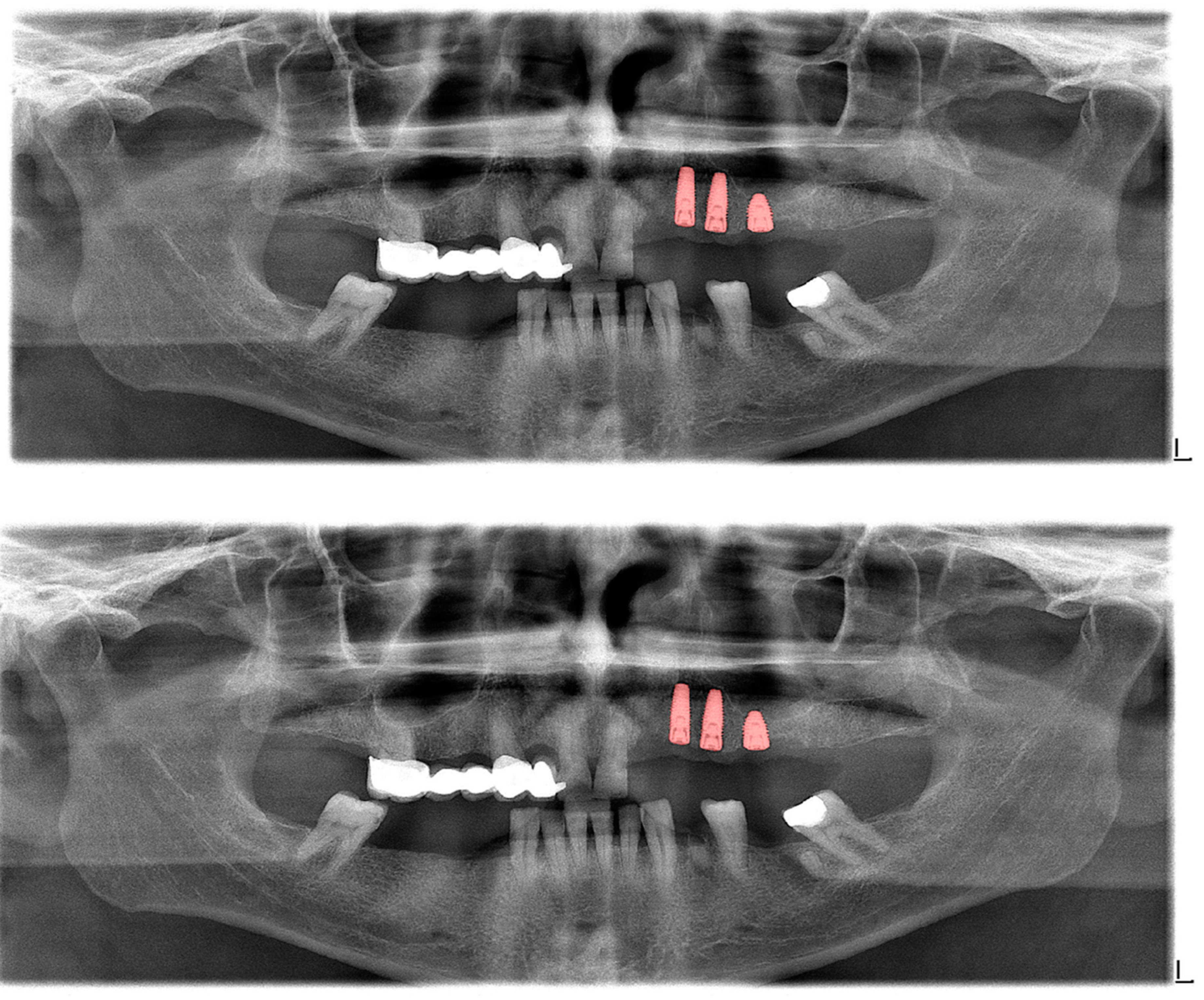
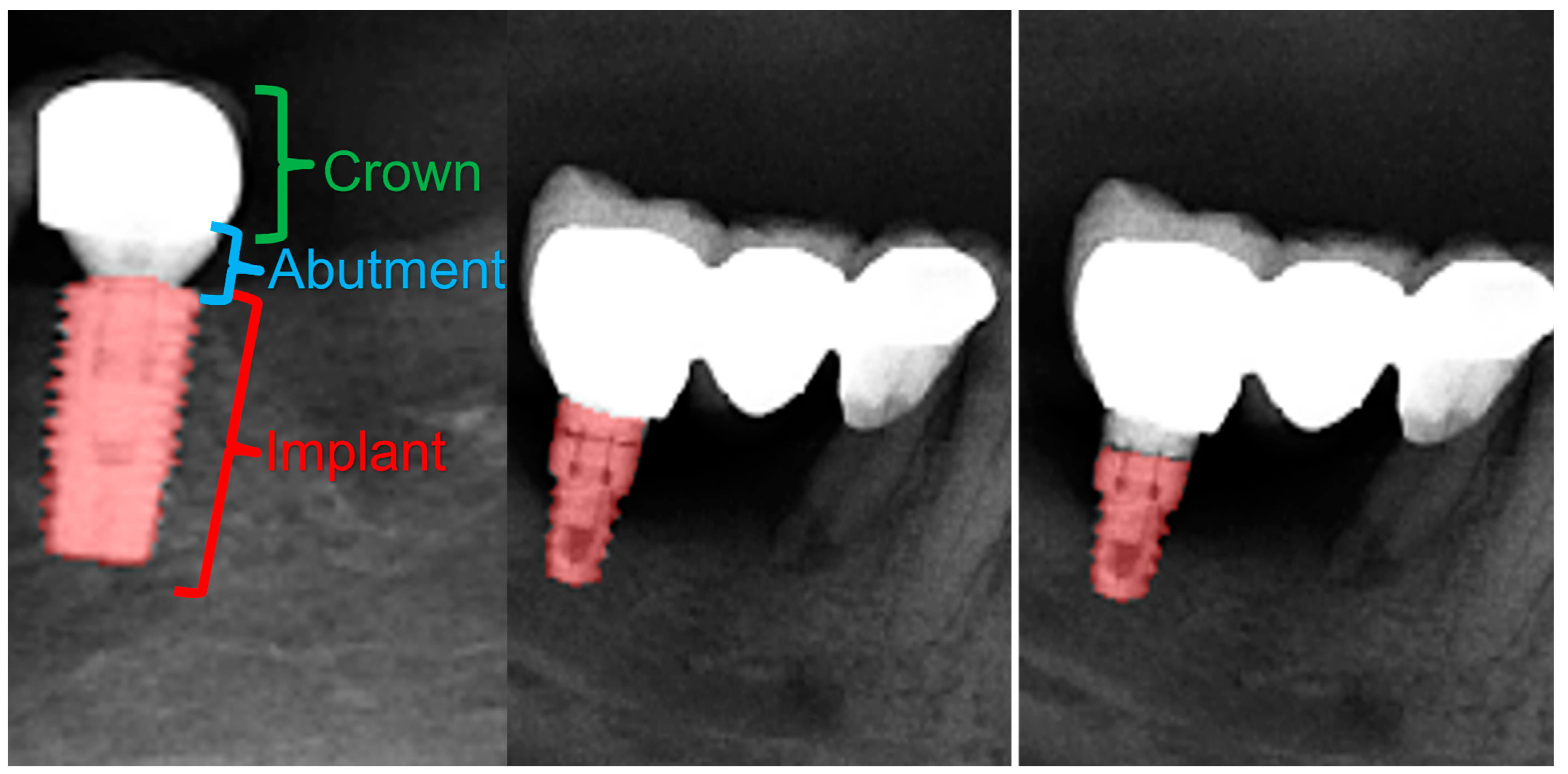
| Dental implants (Figure 5) | 0.94 |
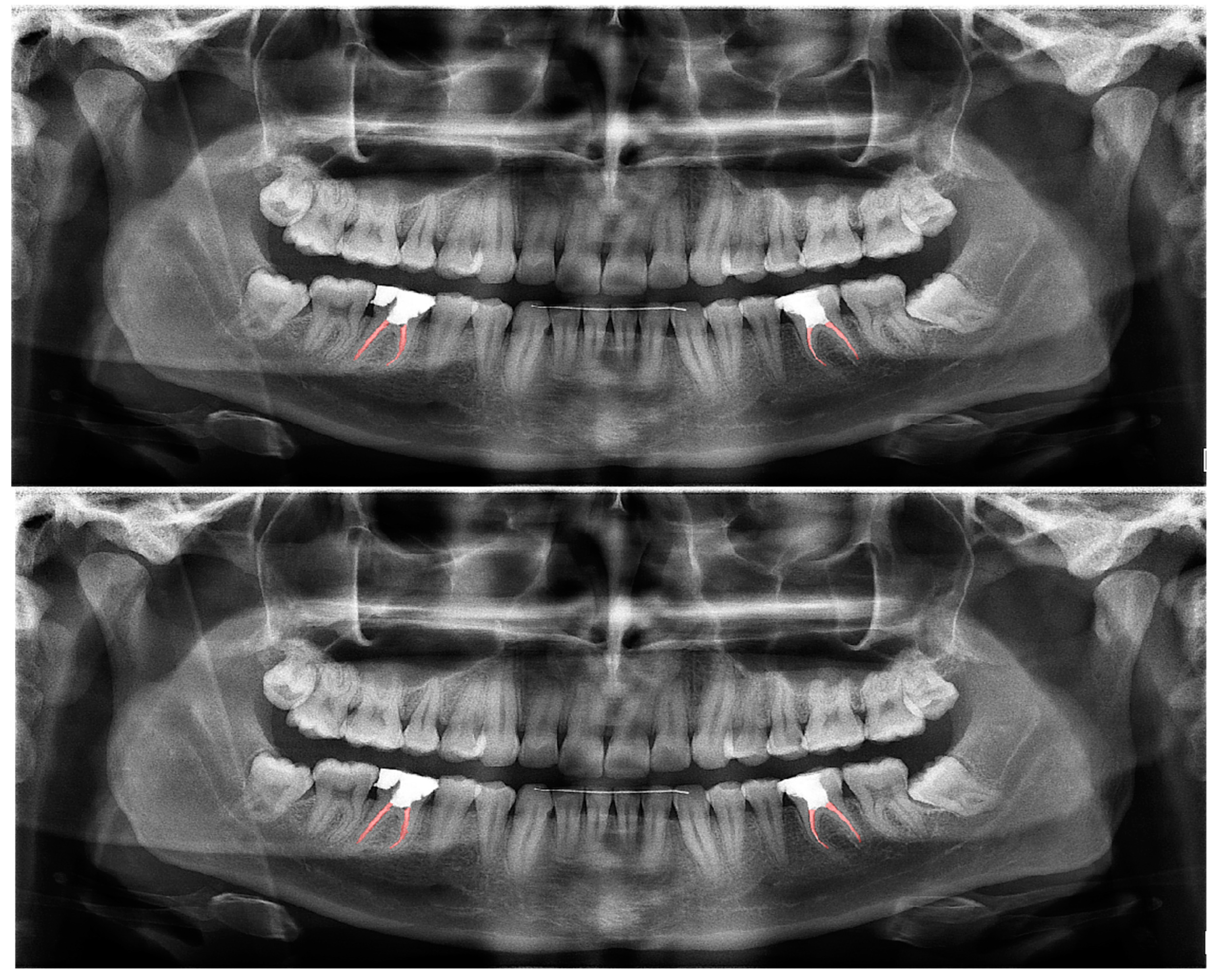
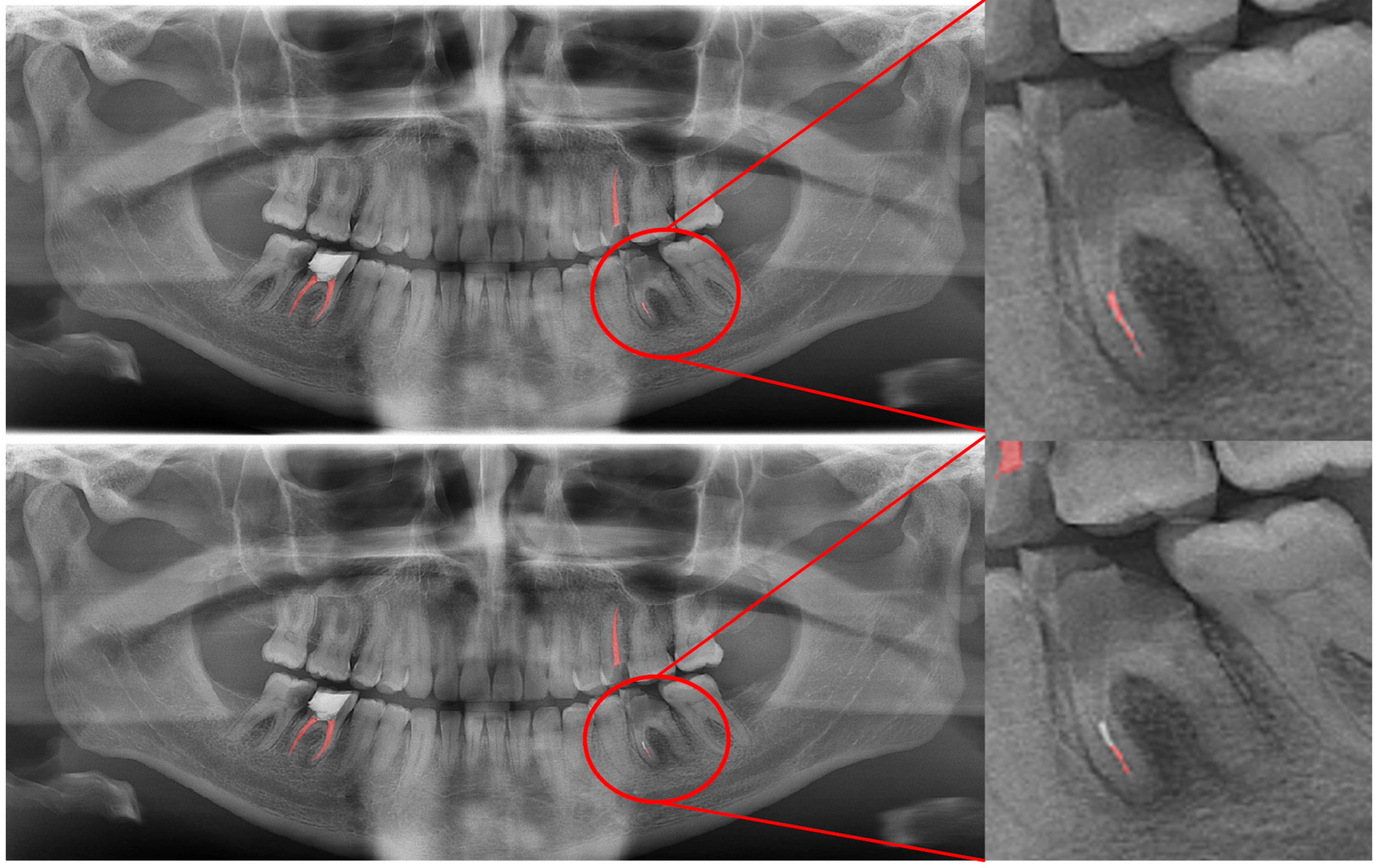
| Root canal fillings (Figure 6) | 0.78 |
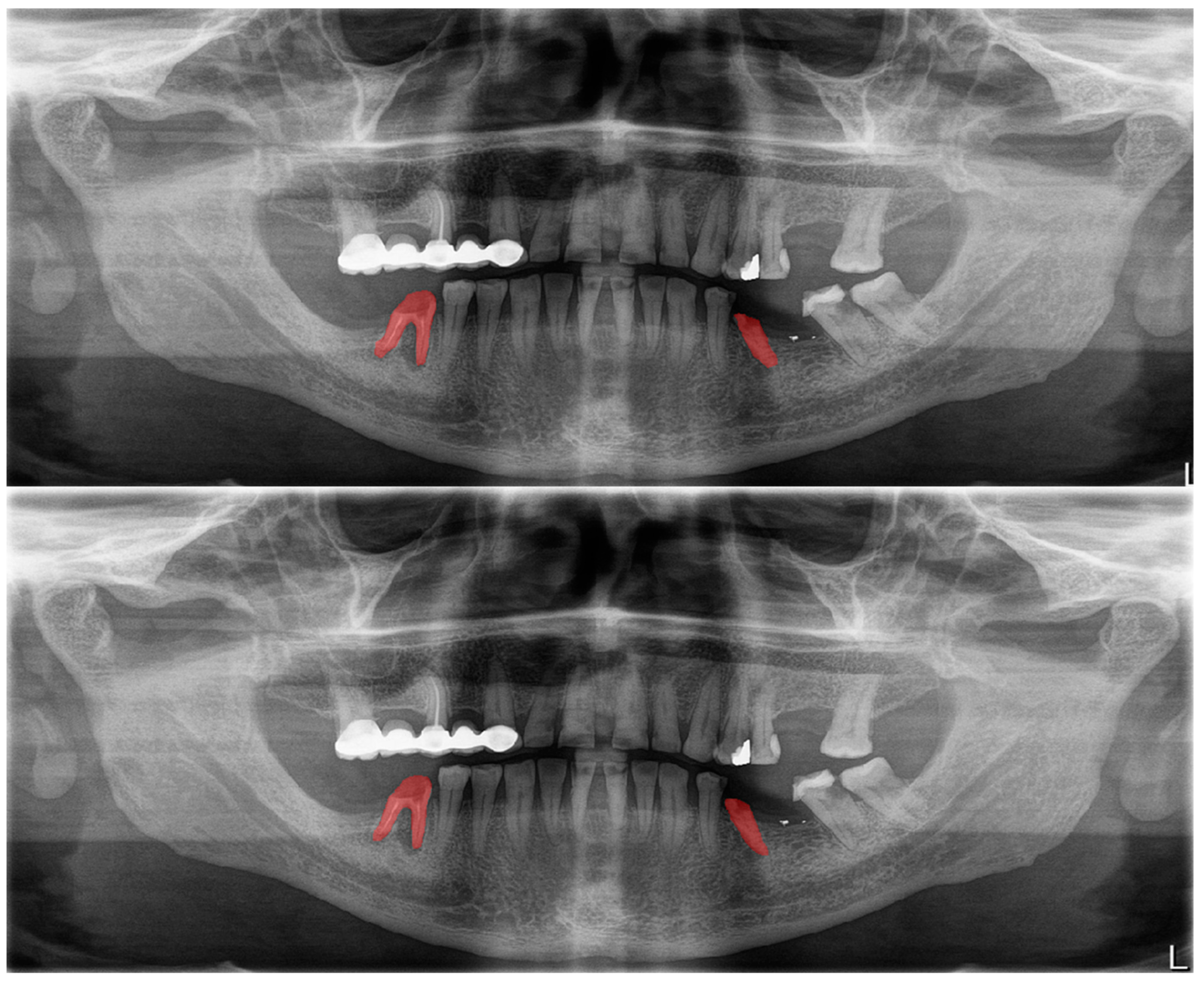
| Residual roots (Figure 7) | 0.78 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gardiyanoğlu, E.; Ünsal, G.; Akkaya, N.; Aksoy, S.; Orhan, K. Automatic Segmentation of Teeth, Crown–Bridge Restorations, Dental Implants, Restorative Fillings, Dental Caries, Residual Roots, and Root Canal Fillings on Orthopantomographs: Convenience and Pitfalls. Diagnostics 2023, 13, 1487. https://doi.org/10.3390/diagnostics13081487
Gardiyanoğlu E, Ünsal G, Akkaya N, Aksoy S, Orhan K. Automatic Segmentation of Teeth, Crown–Bridge Restorations, Dental Implants, Restorative Fillings, Dental Caries, Residual Roots, and Root Canal Fillings on Orthopantomographs: Convenience and Pitfalls. Diagnostics. 2023; 13(8):1487. https://doi.org/10.3390/diagnostics13081487
Chicago/Turabian StyleGardiyanoğlu, Emel, Gürkan Ünsal, Nurullah Akkaya, Seçil Aksoy, and Kaan Orhan. 2023. "Automatic Segmentation of Teeth, Crown–Bridge Restorations, Dental Implants, Restorative Fillings, Dental Caries, Residual Roots, and Root Canal Fillings on Orthopantomographs: Convenience and Pitfalls" Diagnostics 13, no. 8: 1487. https://doi.org/10.3390/diagnostics13081487