
Ambulatory Blood Pressure Monitoring for Diagnosis and Management of Hypertension in Pregnant Women

Abstract
:1. Introduction
2. Out-of-Office Blood Pressure in Hypertension Diagnosis in Pregnant Women
2.1. White-Coat Hypertension
2.2. Masked Hypertension
3. Timeliness of Performing Out-of-Office Blood Pressure Measurements
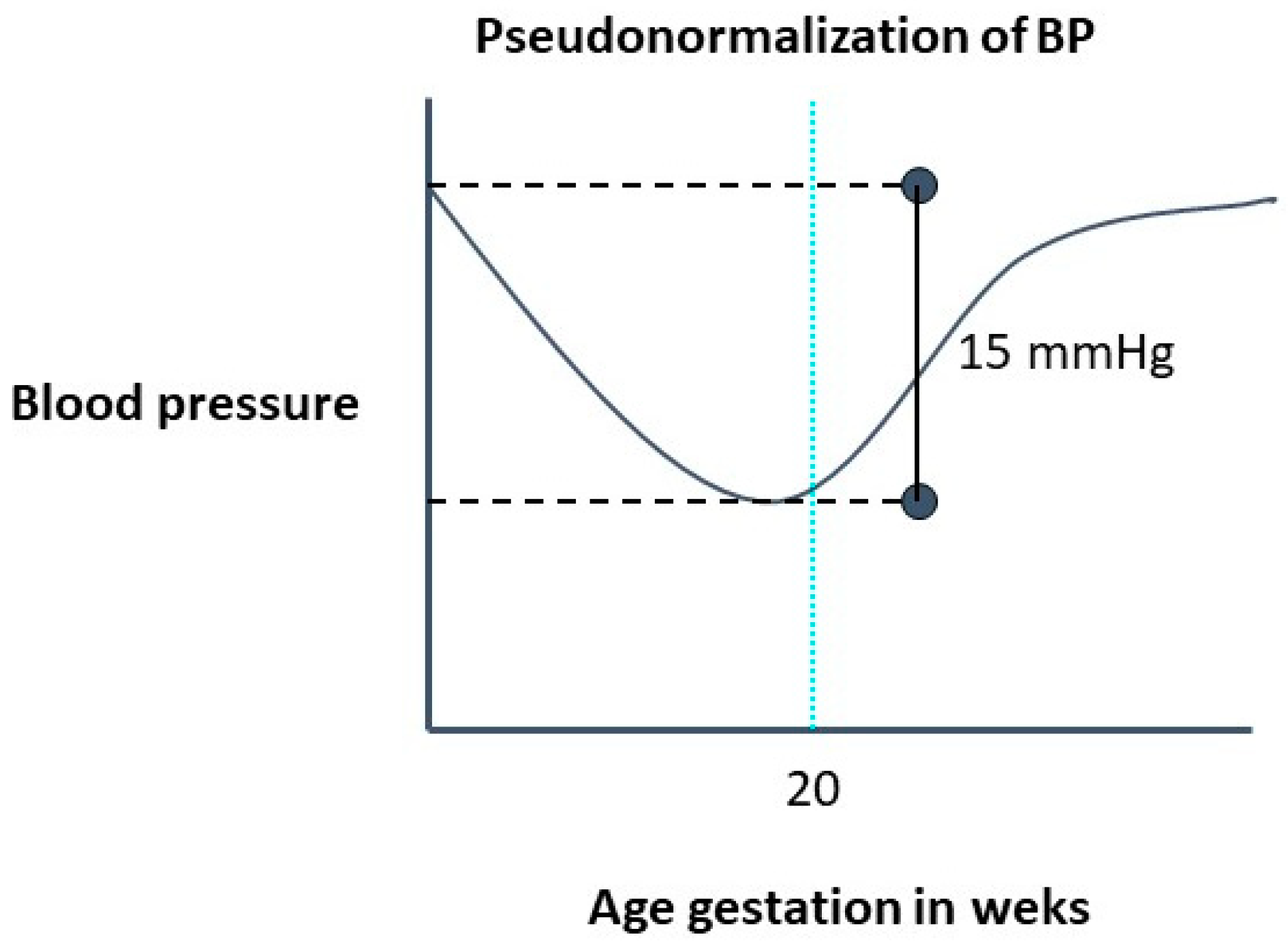
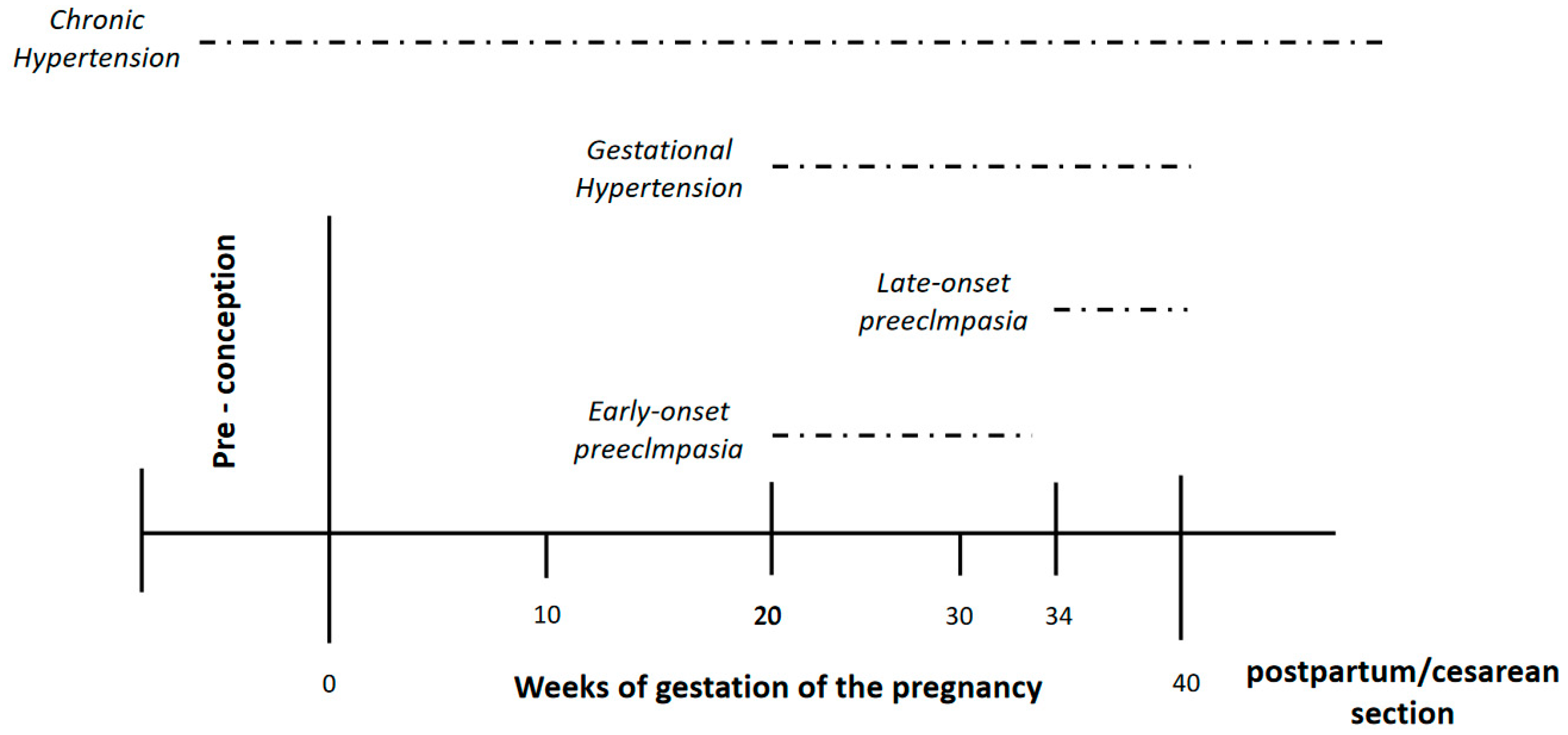
3.1. ABPM before 20 Weeks of Gestation: Identifying Chronic Hypertension
3.2. ABPM after 20 Weeks of Gestation: Identifying Risk of Preeclampsia/Eclampsia
4. Nocturnal Hypertension and Risk for Early Onset Preeclampsia
4.1. Early vs. Late Onset Preeclampsia
4.2. Nocturnal Hypertension and Risk for Early Onset Preeclampsia
5. Hypertension Control in Pregnant Women with Chronic Hypertension
6. Post-Partum Ambulatory Blood Pressure and Long-Term Cardiovascular Risk in Pregnant Women
7. Future Scope and Limitations
- Most evidence comes from observational studies and has inherent limitations, a prospective randomized clinical trial would be necessary to confirm the findings.
- Most evidence comes from studies performed on women with high-risk pregnancies. Therefore, it is not necessarily applicable to normal pregnancies.
- Thresholds for abnormal ABPM in pregnant women have been not defined; values defined for general population are not necessarily appropriate. However, a recently published study of an at-risk pregnant women in a southern Chinese population defined similar ABPM thresholds based in maternal and fetal outcomes [64].
- Therapeutics goals for ABPM have not been defined. Consequently, randomized clinical trials are necessary in order to define clarify this issue.
8. Conclusions
Funding
Conflicts of Interest
References
- Allen, V.M.; Joseph, K.; Murphy, K.E.; Magee, L.A.; Ohlsson, A. The effect of hypertensive disorders in pregnancy on small for gestational age and stillbirth: A population based study. BMC Pregnancy Childbirth 2004, 4, 17. [Google Scholar] [CrossRef] [PubMed]
- Wikström, A.-K.; Gunnarsdottir, J.; Nelander, M.; Simic, M.; Stephansson, O.; Cnattingius, S. Prehypertension in pregnancy and risks of small for gestational age infant and stillbirth. Hypertension 2016, 67, 640–646. [Google Scholar] [CrossRef]
- Steegers, E.A.P.; von Dadelszen, P.; Duvekot, J.J.; Pijnenborg, R. Preeclampsia. Lancet 2010, 376, 631–644. [Google Scholar] [CrossRef] [PubMed]
- Hutcheon, J.A.; Lisonkova, S.; Joseph, K. Epidemiology of preeclampsia and the other hypertensive disorders of pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2011, 25, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Umesawa, M.; Kobashi, G. Epidemiology of hypertensive disorders in pregnancy: Prevalence, risk factors, predictors and prognosis. Hypertens. Res. 2017, 40, 213–220. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 203: Chronic Hypertension in Pregnancy. Obstet. Gynecol. 2019, 133, e26–e50. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- European Society of Gynecology (ESG); Association for European Paediatric Cardiology (AEPC); German Society for Gender Medicine (DGesGM); Regitz-Zagrosek, V.; Lundqvist, C.B.; Borghi, C.; Cifkova, R.; Ferreira, R.; Foidart, J.-M.; Gibbs, J.S.R.; et al. ESC Guidelines on the management of cardiovascular diseases during pregnancy: The Task Force on the Management of Cardiovascular Diseases during Pregnancy of the European Society of Cardiology (ESC). Eur. Heart J. 2011, 32, 3147–3197. [Google Scholar] [CrossRef]
- Butalia, S.; Audibert, F.; Côté, A.-M.; Firoz, T.; Logan, A.G.; Magee, L.A.; Mundle, W.; Rey, E.; Rabi, D.M.; Daskalopoulou, S.S.; et al. Hypertension Canada. Hypertension Canada’s 2018 Guidelines for the Management of Hypertension in Pregnancy. Can. J. Cardiol. 2018, 34, 526–531. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Palatini, P.; Parati, G.; O’brien, E.; Januszewicz, A.; Lurbe, E.; Persu, A.; Mancia, G.; Kreutz, R.; European Society of Hypertension Council and the European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J. Hypertens. 2021, 39, 1293–1302. [Google Scholar] [CrossRef]
- Guias de Manejo, Diagnóstico y Tratamiento de Hipertensión Arterial Intersociedades (FAC-SAC-SAHA). Available online: http://www.saha.org.ar. (accessed on 1 June 2017).
- Garovic, V.D.; Dechend, R.; Easterling, T.; Karumanchi, S.A.; McMurtry Baird, S.; Magee, L.A.; American Heart Association Council on Hypertension; Council on the Kidney in Cardiovascular Disease, Kidney in Heart Disease Science Committee; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Lifestyle and Cardiometabolic Health; et al. Hypertension in Pregnancy: Diagnosis, Blood Pressure Goals, and Pharmacotherapy: A Scientific Statement From the American Heart Association. Hypertension 2022, 79, e21–e41. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S.; et al. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018, 13, 291–310. [Google Scholar] [CrossRef] [PubMed]
- Gillon, T.E.; Pels, A.; Von Dadelszen, P.; MacDonell, K.; Magee, L.A. Hypertensive disorders of pregnancy: A systematic review of international clinical practice guidelines. PLoS ONE 2014, 9, e113715. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Robinson, A.; Jones, M. The white coat effect in hypertensive pregnancy: Much ado about nothing? Br. J. Obstet. Gynaecol. 1999, 106, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Salazar, M.R.; Espeche, W.G.; Balbín, E.; Sisnieguez, C.E.L.; Sisnieguez, B.C.L.; Stavile, R.N.; March, C.; Olano, R.D.; Soria, A.; Yoma, O.; et al. Office blood pressure values and the necessity of out-of-office measurements in high-risk pregnancies. J. Hypertens. 2019, 37, 1838–1844. [Google Scholar] [CrossRef]
- Rodrigues, Â.; Barata, C.; Marques, I.; Almeida, M.C. Diagnosis of white coat hypertension and pregnancy outcomes. Pregnancy Hypertens. 2018, 14, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Mangos, G.; Davis, G.; Homer, C. The natural history of white coat hypertension during pregnancy. BJOG 2005, 112, 601–606. [Google Scholar] [CrossRef]
- Tomitani, N.; Hoshide, S.; Kario, K. Effective out-of-office BP monitoring to detect masked hypertension: Perspectives for wearable BP monitoring. Hypertens. Res. 2023, 46, 523–525. [Google Scholar] [CrossRef]
- Salazar, M.R.; Espeche, W.G.; Sisnieguez, B.C.L.; Balbín, E.; Sisnieguez, C.E.L.; Stavile, R.N.; March, C.E.; Grassi, F.; Santillan, C.; Cor, S.; et al. Significance of masked and nocturnal hypertension in normotensive women coursing a high-risk pregnancy. J. Hypertens. 2016, 34, 2248–2252. [Google Scholar] [CrossRef]
- Salazar, M.R.; Espeche, W.G.; Sisnieguez, C.E.L.; Sisnieguez, B.C.L.; Balbín, E.; Stavile, R.N.; March, C.; Olano, R.D.; Soria, A.; Yoma, O.; et al. Nocturnal hypertension in high-risk mid-pregnancies predict the development of preeclampsia/eclampsia. J. Hypertens. 2019, 37, 182–186. [Google Scholar] [CrossRef]
- Salazar, M.R.; Espeche, W.G.; Sisnieguez, C.E.L.; Juliano, P.L.; Vulcano, M.V.; Caro, L.S.; Minetto, J.; Balbín, E.; Carbajal, H.A. Masked hypertension and neonatal outcome in high-risk pregnancies. J. Hum. Hypertens. 2023, 37, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.-D.; Gao, L.; Huang, O.; Ullah, K.; Guo, M.-X.; Liu, Y.; Zhang, J.; Chen, L.; Fan, J.-X.; Sheng, J.-Z.; et al. Increased Adverse Pregnancy Outcomes Associated With Stage 1 Hypertension in a Low-Risk Cohort: Evidence From 47 874 Cases. Hypertension 2020, 75, 772–780. [Google Scholar] [CrossRef]
- Kario, K.; Hoshide, S.; Tomitani, N.; Nishizawa, M.; Yoshida, T.; Kabutoya, T.; Fujiwara, T.; Mizuno, H.; Narita, K.; Komori, T.; et al. Inconsistent Control Status of Office, Home, and Ambulatory Blood Pressure All Taken Using the Same Device: The HI-JAMP Study Baseline Data. Am. J. Hypertens. 2023, 36, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.-F.; Yang, W.-Y.; Asayama, K.; Zhang, Z.-Y.; Thijs, L.; Li, Y.; O’brien, E.; Staessen, J.A. Ambulatory Blood Pressure Monitoring to Diagnose and Manage Hypertension. Hypertension 2021, 77, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Stergiou, G.S.; Kario, K.; Kollias, A.; McManus, R.J.; Ohkubo, T.; Parati, G.; Imai, Y. Home blood pressure monitoring in the 21st century. J. Clin. Hypertens. 2018, 20, 1116–1121. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Matsubara, K.; Watanabe, K.; Tanaka, K.; Yamamoto, T.; Nohira, T.; Mimura, K.; Suzuki, H.; Hamada, F.; Makino, S.; et al. A multicenter prospective study of home blood pressure measurement (HBPM) during pregnancy in Japanese women. Hypertens. Res. 2022, 45, 1563–1574. [Google Scholar] [CrossRef]
- Espeche, W.G.; Rojas, C.; Stisman, D.; Fuentes, A.; Fita, M.; Lacunza, C.D.; Marquez, D.; Grosse, P.; Bueno, D.; Zilberman, J.; et al. May Measurement Month 2018: An analysis of blood pressure screening results from Argentinean cohort. Eur. Heart J. Suppl. 2020, 22 (Suppl. H), H11–H13. [Google Scholar] [CrossRef]
- Espeche, W.G.; Salazar, M.R.; Minetto, J.; Sisnieguez, C.E.L.; Cerri, G.; Balbín, E.; Stavile, R.N.; Ramos, P.C.; Soria, A.; Santillan, C.; et al. Hypertension arising after 20 weeks of gestation: Gestational hypertension or masked chronic hypertension? J. Hum. Hypertens. 2022, 12. [Google Scholar] [CrossRef]
- Bakker, R.; Steegers, E.A.P.; Hofman, A.; Jaddoe, V.W.V. Blood pressure in different gestational trimesters, fetal growth, and the risk of adverse birth outcomes: The generation R study. Am. J. Epidemiol. 2011, 174, 797–806. [Google Scholar] [CrossRef]
- Bartsch, E.; Medcalf, K.E.; Park, A.L.; Ray, J.G. High Risk of Pre-eclampsia Identification Group. Clinical risk factors for pre-eclampsia determined in early pregnancy: Systematic review and meta-analysis of large cohort studies. BMJ 2016, 353, i1753. [Google Scholar] [CrossRef]
- Wu, P.; Chew-Graham, C.A.; Maas, A.H.; Chappell, L.C.; Potts, J.E.; Gulati, M.; Jordan, K.P.; Mamas, M.A. Temporal Changes in Hypertensive Disorders of Pregnancy and Impact on Cardiovascular and Obstetric Outcomes. Am. J. Cardiol. 2020, 125, 1508–1516. [Google Scholar] [CrossRef] [PubMed]
- Saudan, P.; Brown, M.A.; Buddle, M.L.; Jones, M. Does gestational hypertension become pre-eclampsia? Br. J. Obstet. Gynaecol. 1998, 105, 1177–1184. [Google Scholar] [CrossRef]
- Davis, G.K.; Mackenzie, C.; Brown, M.A.; Homer, C.S.; Holt, J.; McHugh, L.; Mangos, G. Predicting transformation from gestational hypertension to preeclampsia in clinical practice: A possible role for 24 hour ambulatory blood pressure monitoring. Hypertens. Pregnancy 2007, 26, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Shennan, A.; Hyett, J.A.; Kapur, A.; Hadar, E.; Divakar, H.; McAuliffe, F.; da Silva Costa, F.; von Dadelszen, P.; McIntyre, H.D.; et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia: A pragmatic guide for first-trimester screening and prevention. Int. J. Gynaecol. Obstet. 2019, 145 (Suppl. S1), 1–33. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, T.M.; Walker, S.P.; Hannan, N.J.; Tong, S.; Kaitu’U-Lino, T.J. Clinical tools and biomarkers to predict preeclampsia. EBioMedicine 2022, 75, 103780. [Google Scholar] [CrossRef]
- Gilbert, J.S.; Gilbert, S.A.; Arany, M.; Granger, J.P. Hypertension produced by placental ischemia in pregnant rats is associated with increased soluble endoglin expression. Hypertension 2009, 53, 399–403. [Google Scholar] [CrossRef]
- Lyall, F.; Robson, S.C.; Bulmer, J.N. Spiral artery remodeling and trophoblast invasion in preeclampsia and fetal growth restriction: Relationship to clinical outcome. Hypertension 2013, 62, 1046–1054. [Google Scholar] [CrossRef]
- von Dadelszen, P.; Payne, B.; Li, J.; Ansermino, J.M.; Pipkin, F.B.; Côté, A.-M.; Douglas, M.J.; Gruslin, A.; Hutcheon, J.A.; Joseph, K.; et al. Prediction of adverse maternal outcomes in pre-eclampsia: Development and validation of the full PIERS model. Lancet 2011, 377, 219–227. [Google Scholar] [CrossRef]
- Cnossen, J.S.; Morris, R.K.; ter Riet, G.; Mol, B.W.; van der Post, J.A.; Coomarasamy, A.; Zwinderman, A.H.; Robson, S.C.; Bindels, P.J.; Kleijnen, J.; et al. Use of uterine artery Doppler ultrasonography to predict pre-eclampsia and intrauterine growth restriction: A systematic review and bivariable meta-analysis. CMAJ 2008, 178, 701–711. [Google Scholar] [CrossRef]
- Chaemsaithong, P.; Pooh, R.K.; Zheng, M.; Ma, R.; Chaiyasit, N.; Tokunaka, M.; Shaw, S.W.; Seshadri, S.; Choolani, M.; Wataganara, T.; et al. Prospective evaluation of screening performance of first-trimester prediction models for preterm preeclampsia in an Asian population. Am. J. Obstet. Gynecol. 2019, 221, 650.e1–650.e16. [Google Scholar] [CrossRef]
- Magee, L.A.; Pels, A.; Helewa, M.; Rey, E.; von Dadelszen, P.; Canadian Hypertensive Disorders of Pregnancy (HDP) Working Group. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. Pregnancy Hypertens. 2014, 4, 105–145. [Google Scholar] [CrossRef] [PubMed]
- Bilo, G.; Parati, G. Ambulatory blood pressure monitoring: A mandatory approach in high-risk pregnancy? J. Hypertens. 2016, 34, 2140–2142. [Google Scholar] [CrossRef] [PubMed]
- Ness, R.B.; Roberts, J.M. Heterogeneous causes constituting the single syndrome of preeclampsia: A hypothesis and its implications. Am. J. Obstet. Gynecol. 1996, 175, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- Vatten, L.J.; Skjaerven, R. Is pre-eclampsia more than one disease? BJOG 2004, 111, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Egbor, M.; Ansari, T.; Morris, N.; Green, C.I.; Sibbons, P.D. Morphometric placental villous and vascular abnormalities in early and late-onset pre-eclampsia with and without fetal growth restriction. BJOG 2006, 113, 580–589. [Google Scholar] [CrossRef]
- Moldenhauer, J.S.; Stanek, J.; Warshak, C.; Khoury, J.; Sibai, B. The frequency and severity of placental findings in women with preeclampsia are gestational age dependent. Am. J. Obstet. Gynecol. 2003, 189, 1173–1177. [Google Scholar] [CrossRef]
- Burton, G.J.; Redman, C.W.; Roberts, J.M.; Moffett, A. Pre-eclampsia: Pathophysiology and clinical implications. BMJ 2019, 366, l2381. [Google Scholar] [CrossRef]
- Lisonkova, S.; Joseph, K.S. Incidence of preeclampsia: Risk factors and outcomes associated with early- versus late-onset disease. Am. J. Obstet. Gynecol. 2013, 209, 544.e1–544.e12. [Google Scholar] [CrossRef]
- Salazar, M.R.; Espeche, W.G.; Sisnieguez, C.E.L.; Minetto, J.; Balbín, E.; Soria, A.; Yoma, O.; Prudente, M.; Torres, S.; Grassi, F.; et al. Nocturnal hypertension and risk of developing early-onset preeclampsia in high-risk pregnancies. Hypertens. Res. 2021, 44, 1633–1640. [Google Scholar] [CrossRef]
- Hoshide, S.; Kanegae, H.; Kario, K. Nighttime home blood pressure as a mediator of N-terminal pro-brain natriuretic peptide in cardiovascular events. Hypertens. Res. 2021, 44, 1138–1146. [Google Scholar] [CrossRef]
- Hoshide, S. Nocturnal hypertension-solving the puzzle of preeclampsia risk. Hypertens. Res. 2021, 44, 1681–1682. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.N., Jr.; Thigpen, B.D.; Moore, R.C.; Rose, C.H.; Cushman, J.; May, W. Stroke and severe preeclampsia and eclampsia: A paradigm shift focusing on systolic blood pressure. Obstet. Gynecol. 2005, 105, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Housni, B.; Bayad, R.; Cherkab, R.; Salmi, S.; Miguil, M. Brainstem ischemia and preeclampsia. Hypertens. Pregnancy 2004, 23, 269–273. [Google Scholar] [CrossRef]
- Ozkan, D.; Ibanoglu, M.C.; Adar, K.; Ozkan, M.; Tapisiz, O.L.; Engin-Ustun, Y.; Iskender, C.T. Efficacy of blood parameters in predicting the severity of gestational hypertension and preeclampsia. J. Obstet. Gynaecol. 2023, 43, 2144175. [Google Scholar] [CrossRef] [PubMed]
- Magee, L.A.; Singer, J.; von Dadelszen, P.; CHIPS Study Group. Less-tight versus tight control of hypertension in pregnancy. N. Engl. J. Med. 2015, 372, 2366–2368. [Google Scholar] [CrossRef] [PubMed]
- Bánhidy, F.; Ács, N.; Puhó, E.H.; Czeizel, A.E. The efficacy of antihypertensive treatment in pregnant women with chronic and gestational hypertension: A population-based study. Hypertens. Res. 2010, 33, 460–466. [Google Scholar] [CrossRef]
- Tita, A.T.; Szychowski, J.M.; Boggess, K.; Dugoff, L.; Sibai, B.; Lawrence, K.; Hughes, B.L.; Bell, J.; Aagaard, K.; Edwards, R.K.; et al. Chronic Hypertension and Pregnancy (CHAP) Trial Consortium. Treatment for Mild Chronic Hypertension during Pregnancy. N. Engl. J. Med. 2022, 386, 1781–1792. [Google Scholar] [CrossRef]
- Abe, M.; Arima, H.; Yoshida, Y.; Fukami, A.; Sakima, A.; Metoki, H.; Tada, K.; Mito, A.; Morimoto, S.; Shibata, H.; et al. Optimal blood pressure target to prevent severe hypertension in pregnancy: A systematic review and meta-analysis. Hypertens. Res. 2022, 45, 887–899. [Google Scholar] [CrossRef]
- Ueda, A.; Hasegawa, M.; Matsumura, N.; Sato, H.; Kosaka, K.; Abiko, K.; Yoshioka, S.; Yoshida, T.; Tatsumi, K.; Higuchi, T.; et al. Lower systolic blood pressure levels in early pregnancy are associated with a decreased risk of early-onset superimposed preeclampsia in women with chronic hypertension: A multicenter retrospective study. Hypertens. Res. 2021, 45, 135–145. [Google Scholar] [CrossRef]
- Melloni, C.; Berger, J.S.; Wang, T.Y.; Gunes, F.; Stebbins, A.; Pieper, K.S.; Dolor, R.J.; Douglas, P.S.; Mark, D.B.; Newby, L.K. Representation of women in randomized clinical trials of cardiovascular disease prevention. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 135–142. [Google Scholar] [CrossRef]
- Jameson, J.L.; Fauci, A.; Kasper, D.; Hauser, S.; Longo, D.; Loscalzo, J. Principios de Medicina Interna, 20th ed.; Mac Graw Hill Education: New York, NY, USA, 2019; Volume 1, pp. 256–257. ISBN 9781456264864. [Google Scholar]
- Benschop, L.; Duvekot, J.J.; Versmissen, J.; Van Broekhoven, V.; Steegers, E.A.; Van Lennep, J.E.R. Blood Pressure Profile 1 Year After Severe Preeclampsia. Hypertension 2018, 71, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Lv, L.; Ji, W.; Wu, L.; Miao, J.; Wen, J.; Lei, Q.; Duan, D.; Chen, H.; Hirst, J.E.; Henry, A.; et al. Thresholds for Ambulatory Blood Pressure Monitoring Based on Maternal and Neonatal Outcomes in Late Pregnancy in a Southern Chinese Population. J. Am. Heart Assoc. 2019, 8, e012027. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Office BP (mmHg) | Absolute Risk | Unadjusted Relative Risk | Adjusted Relative Risk * | |||
|---|---|---|---|---|---|---|
| Mean ± SD | (%) | OR | 95% CI | OR | 95% CI | |
| SBP quartiles | ||||||
| 91.0–115.7 mmHg | 108.7 ± 5.4 | 8.8 | 1 | 1 | ||
| 116.0–124.7 mmHg | 120.4 ± 2.8 | 13.4 | 1.60 | 0.63–4.08 | 1.35 | 0.52–3.51 |
| 125.0–132.7 mmHg | 128.9 ± 2.2 | 19.6 | 2.52 | 1.04–6.14 | 2.17 | 0.87–5.43 |
| 133.0–165.0 mmHg | 143.6 ± 8.1 | 32.3 | 4.94 | 2.12–11.51 | 3.99 | 1.66–9.56 |
| p < 0.001 | p for trend = 0.001 | p for trend = 0.004 | ||||
| DBP quartiles | ||||||
| 48.7–69.3 mmHg | 63.8 ± 4.5 | 6.5 | 1 | 1 | ||
| 69.7–75.7 mmHg | 72.7 ± 1.7 | 13.7 | 2.30 | 0.83–6.33 | 2.13 | 0.76–5.97 |
| 76.0–81.7 mmHg | 78.9 ± 1.7 | 19.6 | 3.53 | 1.33–9.34 | 3.08 | 1.14–8.31 |
| 82.0–108.3 mmHg | 88.8 ± 5.6 | 34.4 | 7.61 | 3.00–19.31 | 6.47 | 2.49–16.82 |
| p < 0.001 | p for trend < 0.001 | p for trend < 0.001 | ||||
| Period of Gestation | Indications | Aims |
|---|---|---|
| First half | All women with office BP > 125/75 mmHg | To make an appropriate diagnose of chronic hypertension identifying white coat hypertension and masked hypertension. |
| Second half | Women with high-risk pregnancy | To identify women with high risk for preeclampsia. |
| Post-partum (3–6 months after the delivery) | Women who developed preeclampsia | To evaluate long-term cardiovascular prognosis identifying masked and nocturnal hypertension. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espeche, W.G.; Salazar, M.R. Ambulatory Blood Pressure Monitoring for Diagnosis and Management of Hypertension in Pregnant Women. Diagnostics 2023, 13, 1457. https://doi.org/10.3390/diagnostics13081457
Espeche WG, Salazar MR. Ambulatory Blood Pressure Monitoring for Diagnosis and Management of Hypertension in Pregnant Women. Diagnostics. 2023; 13(8):1457. https://doi.org/10.3390/diagnostics13081457
Chicago/Turabian StyleEspeche, Walter G., and Martin R. Salazar. 2023. "Ambulatory Blood Pressure Monitoring for Diagnosis and Management of Hypertension in Pregnant Women" Diagnostics 13, no. 8: 1457. https://doi.org/10.3390/diagnostics13081457