
ETISTP: An Enhanced Model for Brain Tumor Identification and Survival Time Prediction
 , , , , and
, , , , and
Abstract
:1. Introduction
- ETISTP enables the improved classification of gliomas with respect to different grades.
- To the best of the authors’ knowledge, this work pioneers the use of tumor volume for survival time prediction.
- This work integrates four different factors to enhance the accuracy of survival time prediction.
- The proposed model reduces the computation time by enabling the parallel execution of tumor volume computation and classification.
2. Related Work
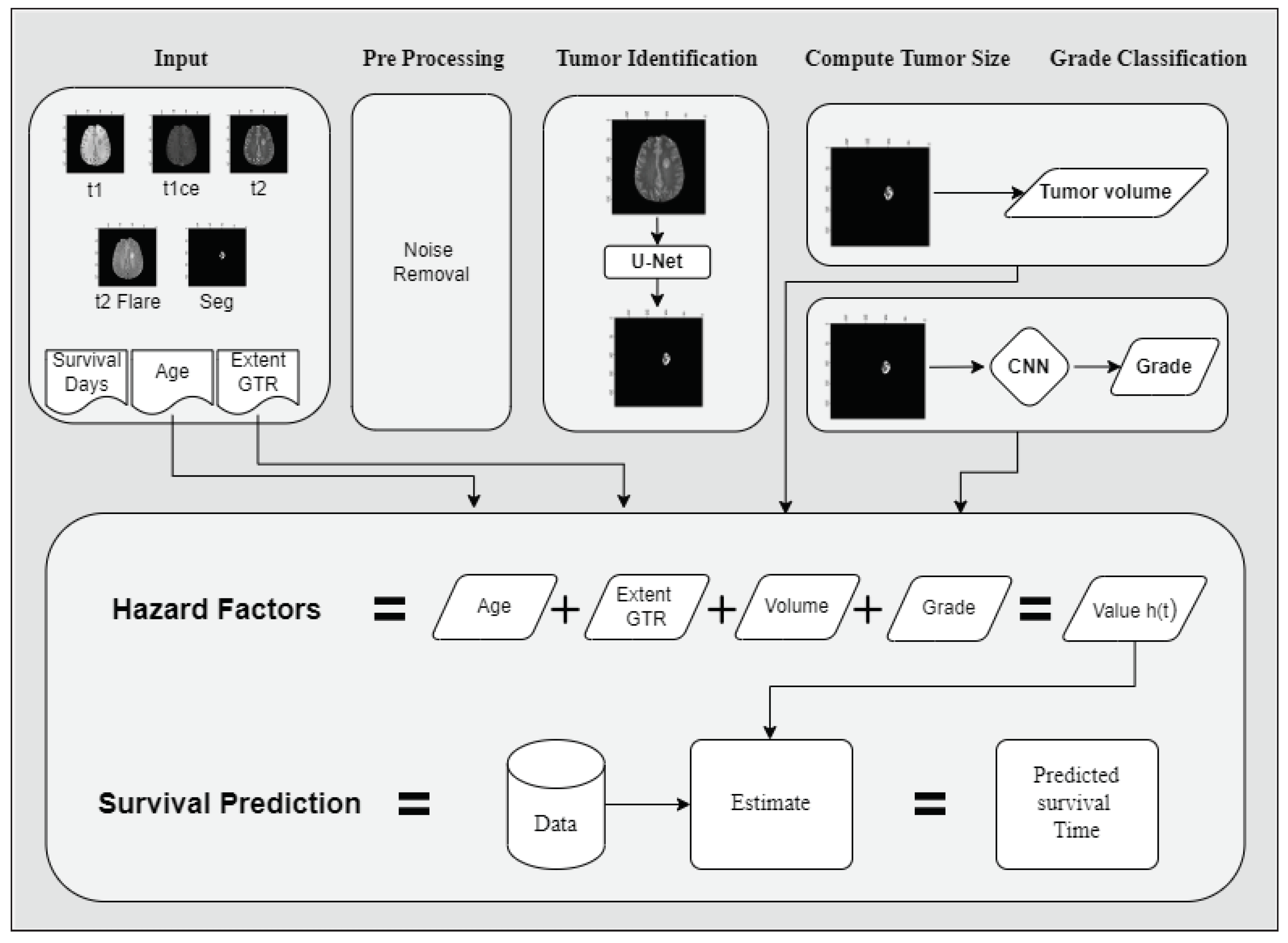
3. The Proposed ETISTP Model
| Algorithm 1 Pseudocode of the proposed ETISTP model. |
|
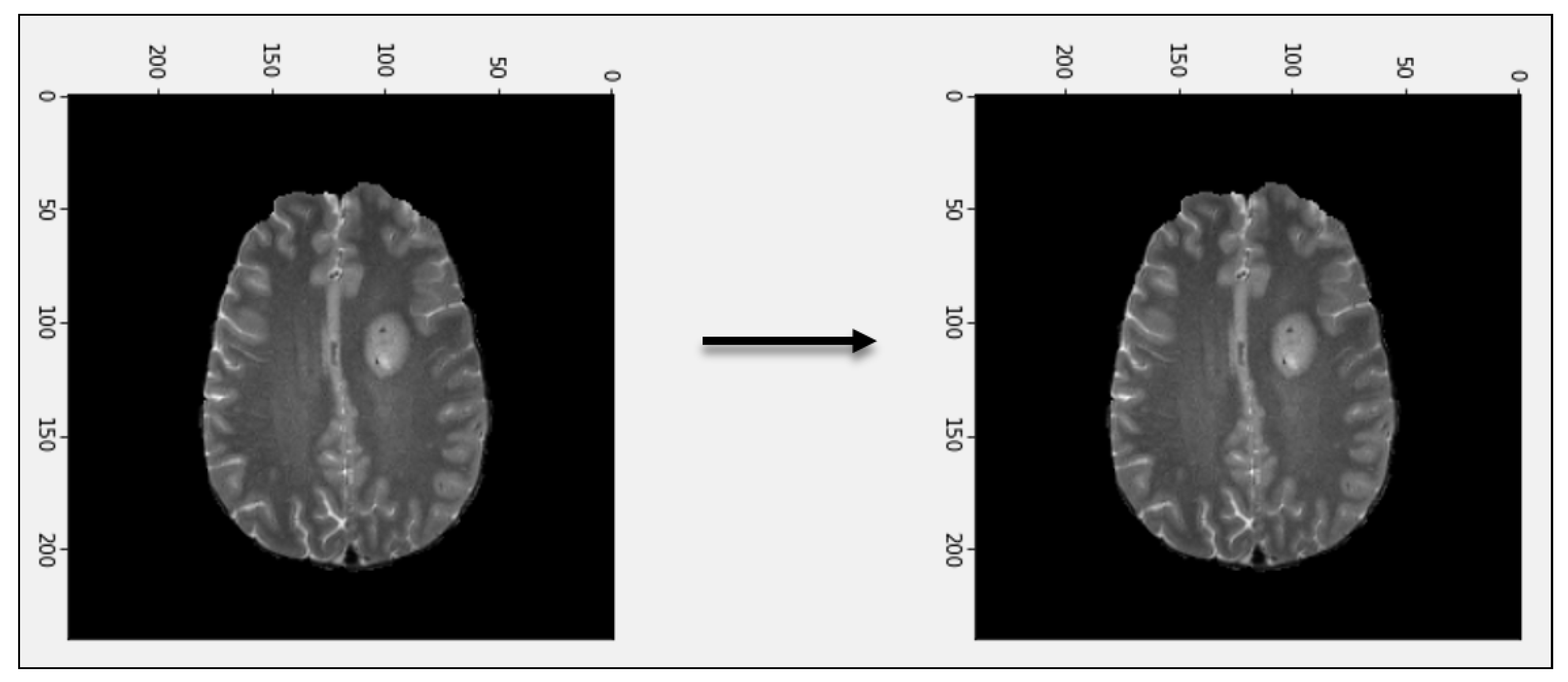
3.1. Pre-Processing
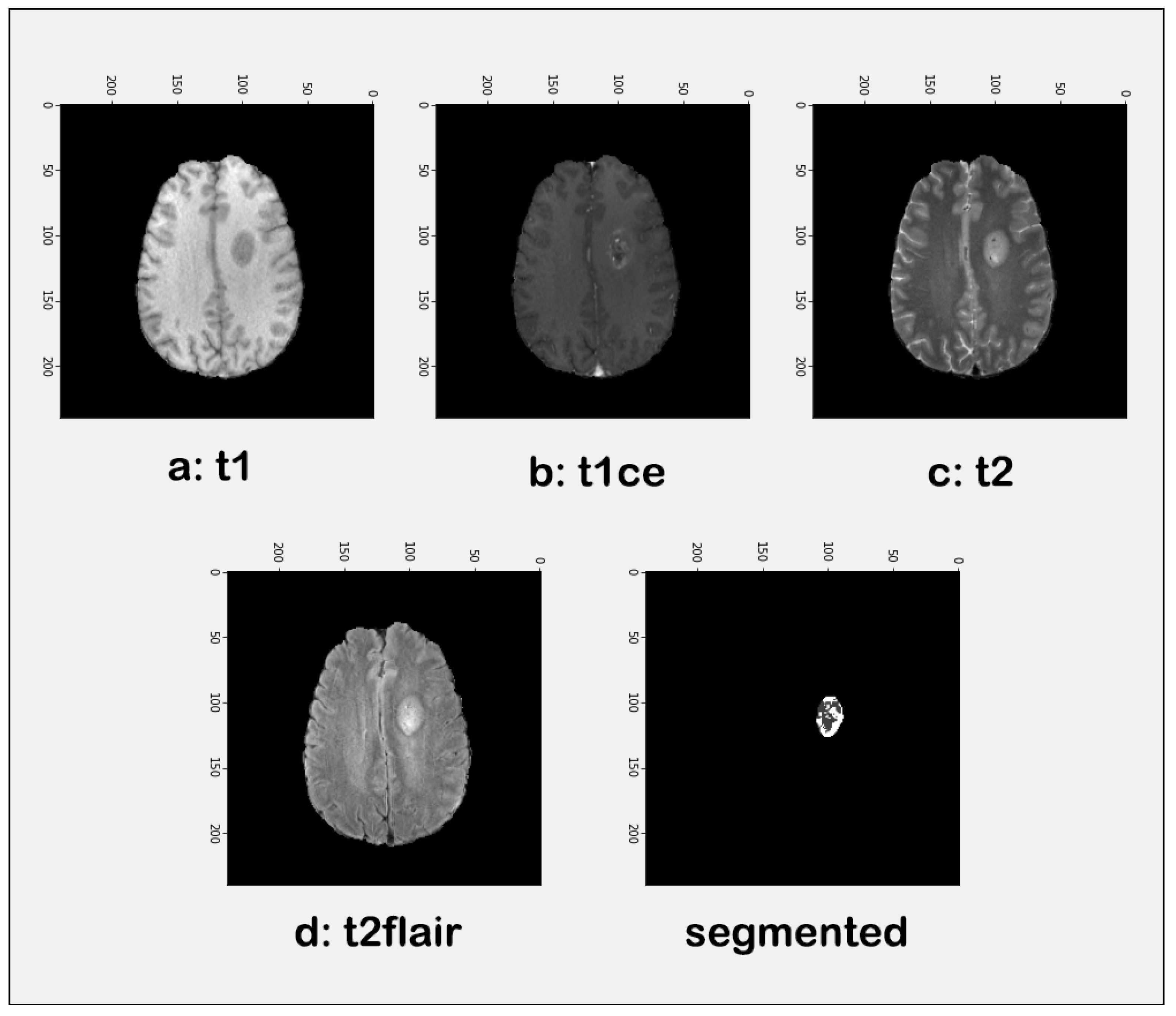
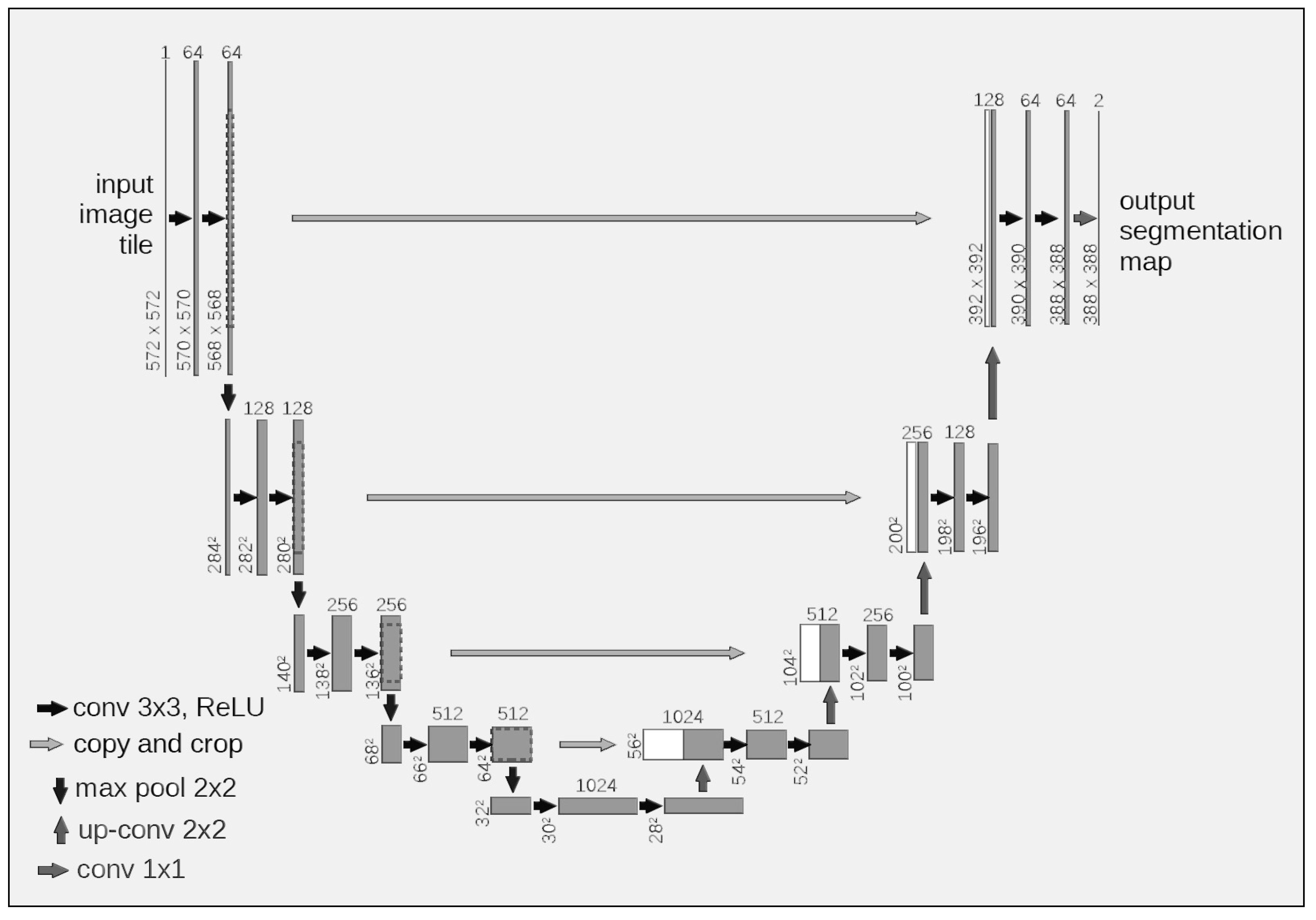
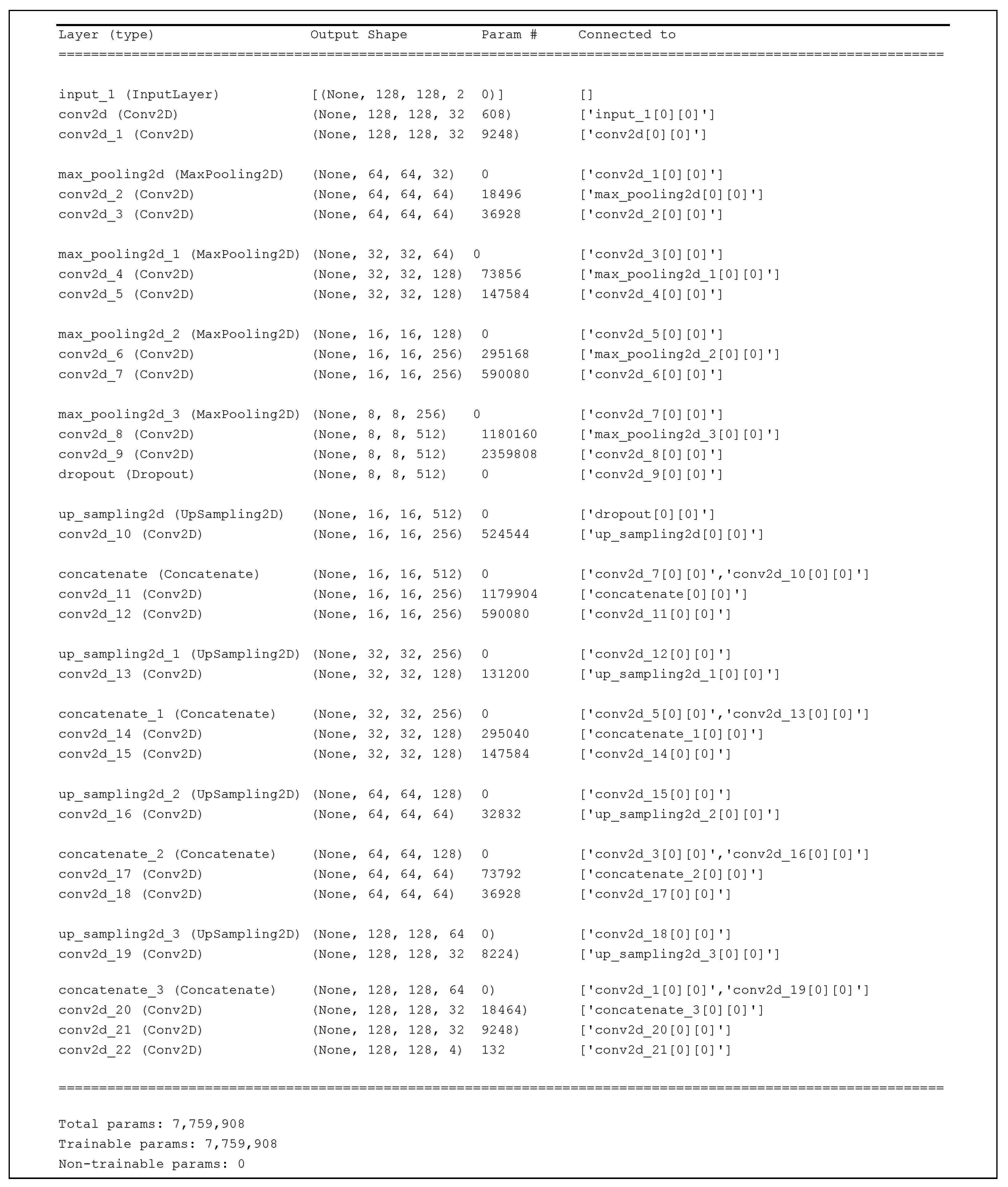
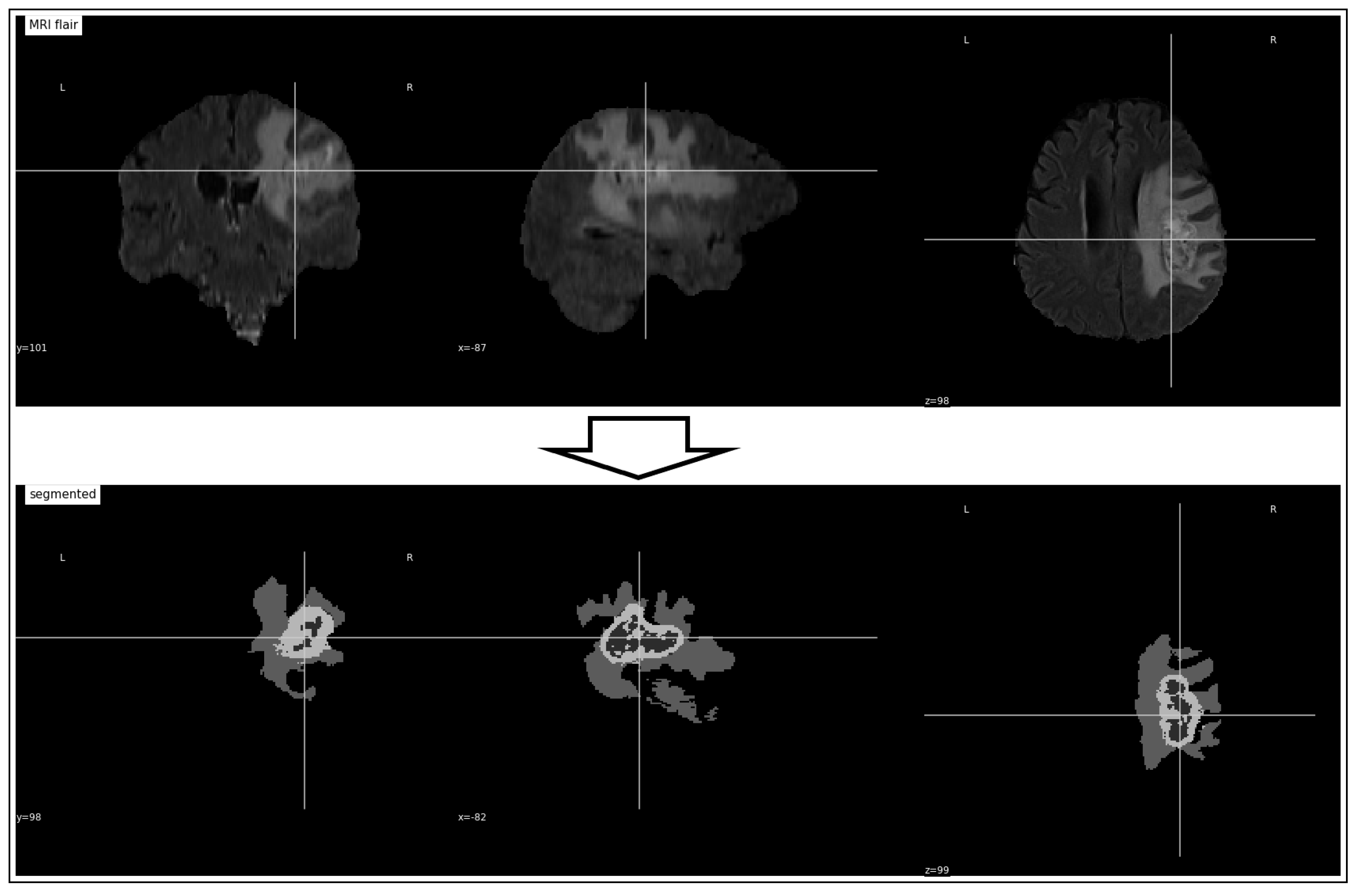
3.2. Tumor Identification
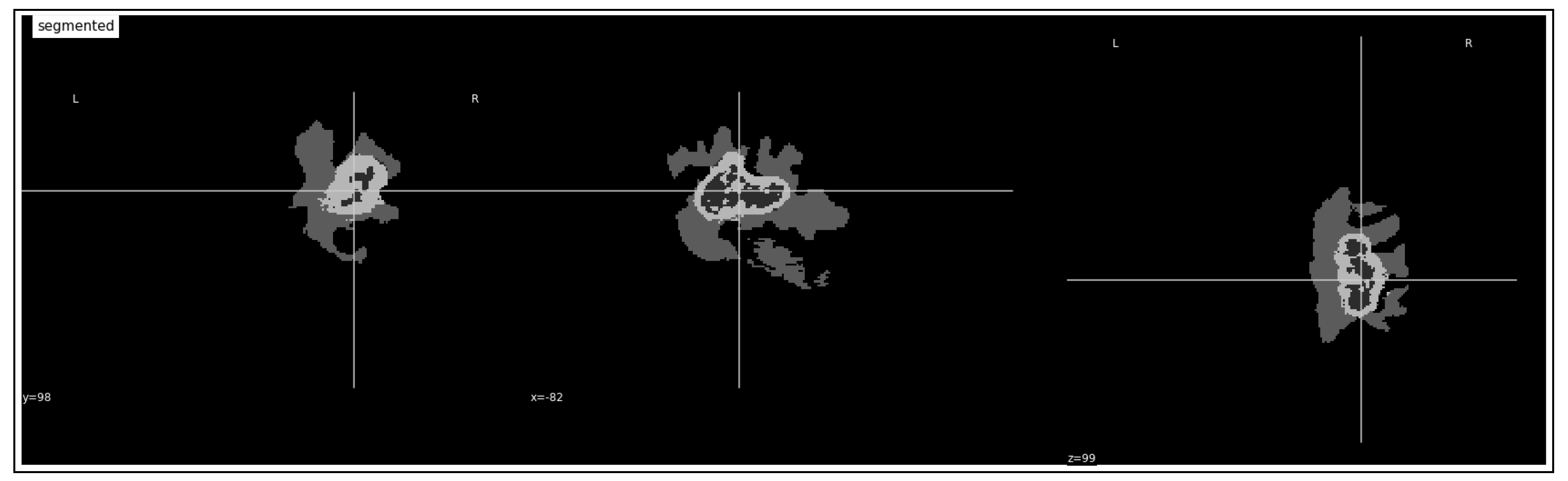
3.3. Tumor Volume Computation
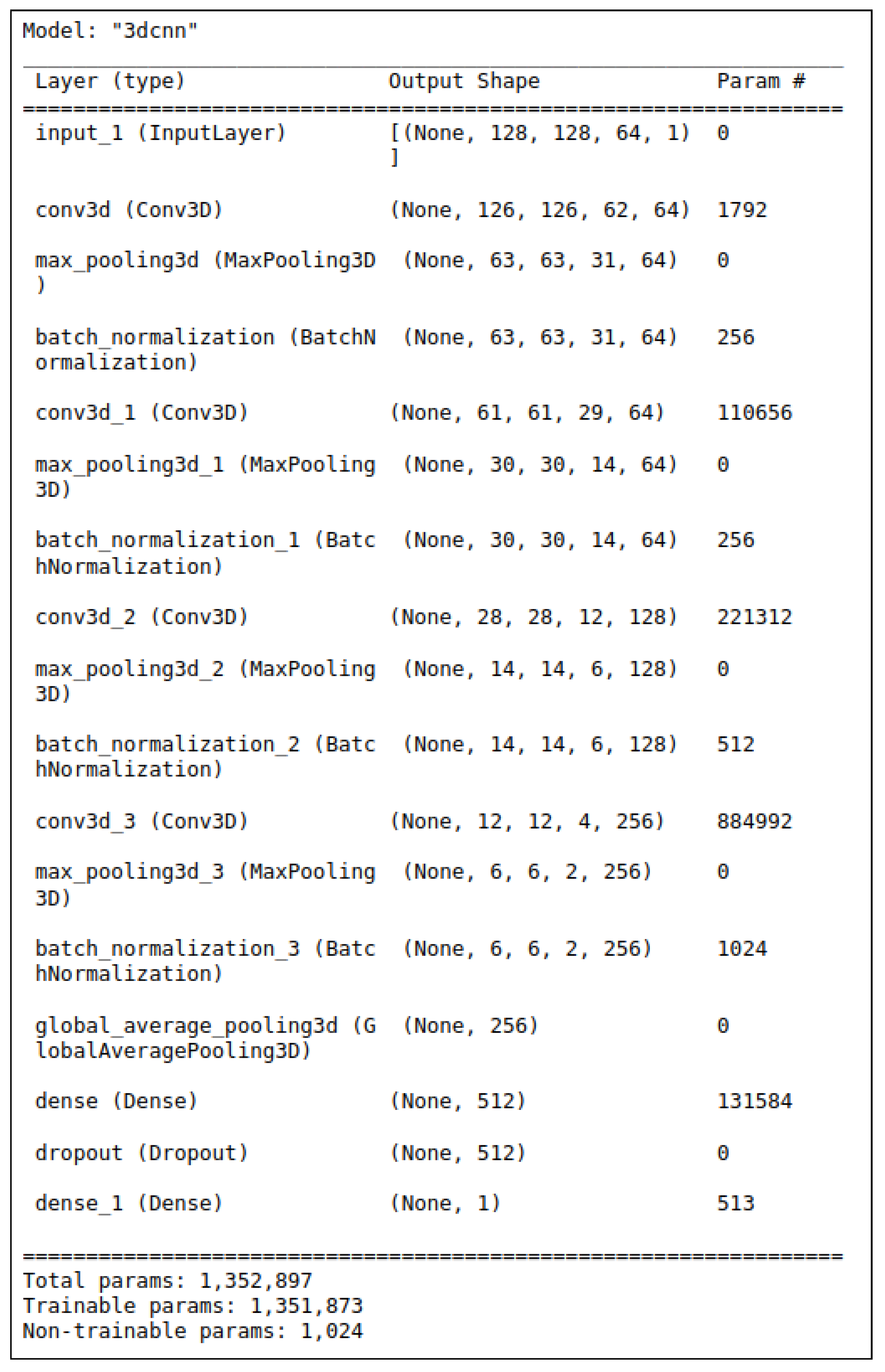
3.4. Tumor Grade Classification
3.5. Survival Time Prediction
- The hazard ratio (HR) is the ratio of the hazard rates of two groups, which in this case is the ratio of the hazard rate of the group with a one-unit increase in the factor to the hazard rate of the group with the reference level of the factor.
- The coefficient (coef) of each factor is the estimated change in the log hazard ratio for a one-unit increase in the factor, holding other factors constant.
- The exponentiated coefficient (exp (coef)) is the estimated change in the hazard ratio for a one-unit increase in the factor, holding other factors constant.
- The standard error (se) of the coefficient is the estimated standard deviation of the coefficient.
- The 95% confidence interval (CI) of the coefficient provides a range of values for the coefficient that is likely to contain the true value of the coefficient with a 95% probability.
- The 95% CI of the exponentiated coefficient provides a range of values for the hazard ratio that is likely to contain the true value of the hazard ratio with a 95% probability.
- The z-value is the coefficient divided by the standard error and indicates the significance of the coefficient.
- The p-value is the probability of observing a z-value that is as extreme as (or more extreme than) the observed z-value under the assumption that the null hypothesis, which states that the coefficient is zero, is true.
- The −log2(p) is the negative logarithm (base 2) of the p-value and it indicates the strength of evidence against the null hypothesis.
- Age: The coefficient of age is 0.04, indicating that the hazard ratio of survival time increases by 4% for a one-year increase in age, assuming that all other factors remain constant. This effect is statistically significant (). The 95% confidence interval (CI) of the hazard ratio ranges from 1.02 to 1.05, indicating that the hazard ratio is likely to increase between 2% and 5% for a one-year increase in age.
- GTR: The coefficient of GTR is 0.04, which means that the hazard ratio of survival time increases by 4% for GTR, holding other factors constant. However, this effect is not statistically significant (). The 95% CI of the hazard ratio is 0.90 to 1.19, which means that the hazard ratio can decrease by 10% or increase by 19% for GTR, but the uncertainty is high.
- Class: The coefficient of ’class’ is -0.64, which means that the hazard ratio of survival time decreases by 47% for class, holding other factors constant. This effect is marginally significant (), indicating weak evidence against the null hypothesis. The 95% CI of the hazard ratio is 0.26 to 1.08, which means that the hazard ratio can decrease by 74% or increase by 8% for class, but the uncertainty is high.
- Volume: The coefficient of volume is 0.00, which means that the hazard ratio of survival time does not change for volume, holding other factors constant. This effect is not statistically significant (). The 95% CI of the hazard ratio is 1.00 to 1.00, which means that the hazard ratio is likely to remain the same for volume. However, the upper bound of the CI is 1.08, indicating that there is a small possibility that the hazard ratio can increase by up to 8% for a one-unit increase in volume, but the uncertainty is high.
4. Performance Evaluation
4.1. Simulation Setup
4.2. Performance Evaluation Criteria
4.3. Results and Discussion
4.3.1. Tumor Identification
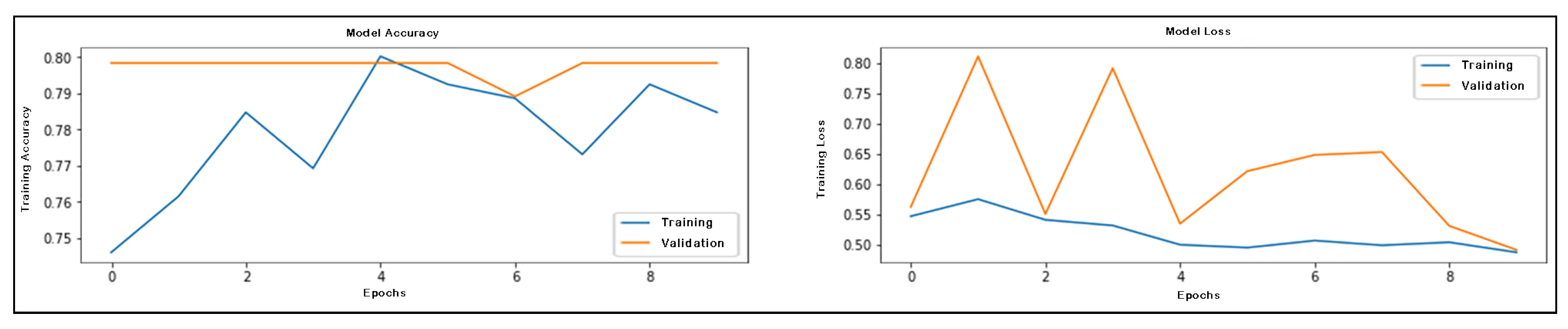
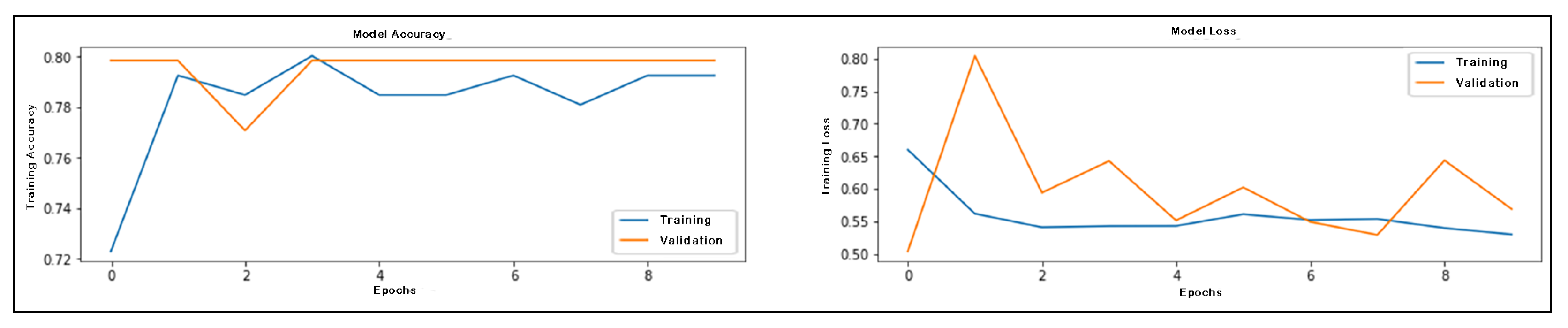
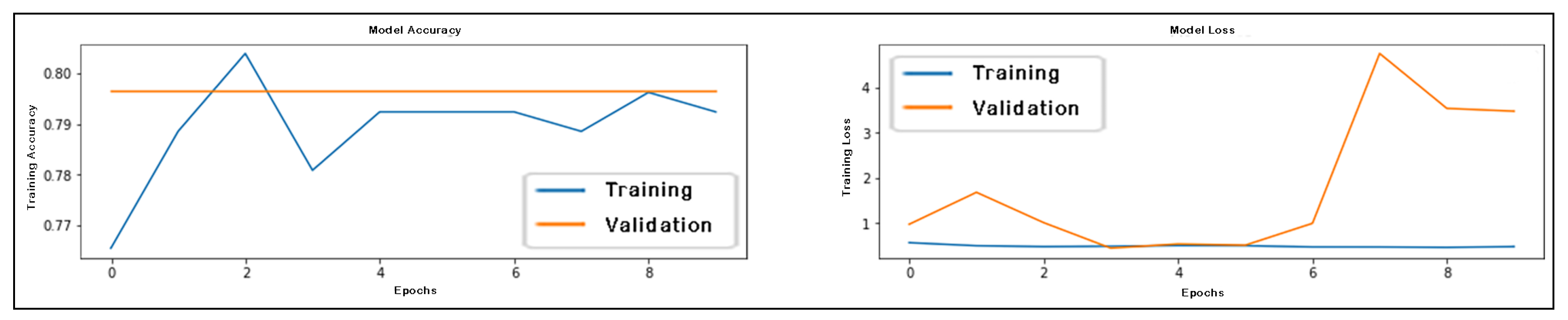
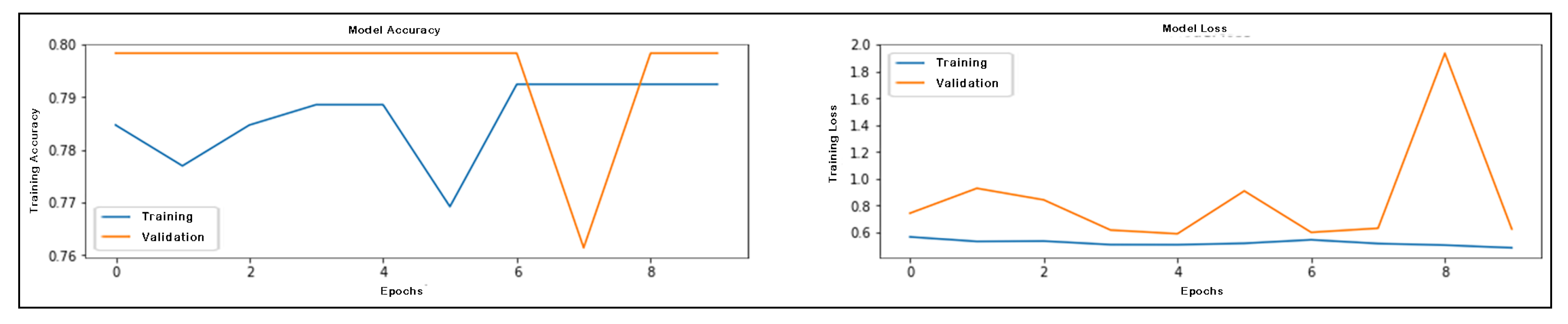
4.3.2. Classification
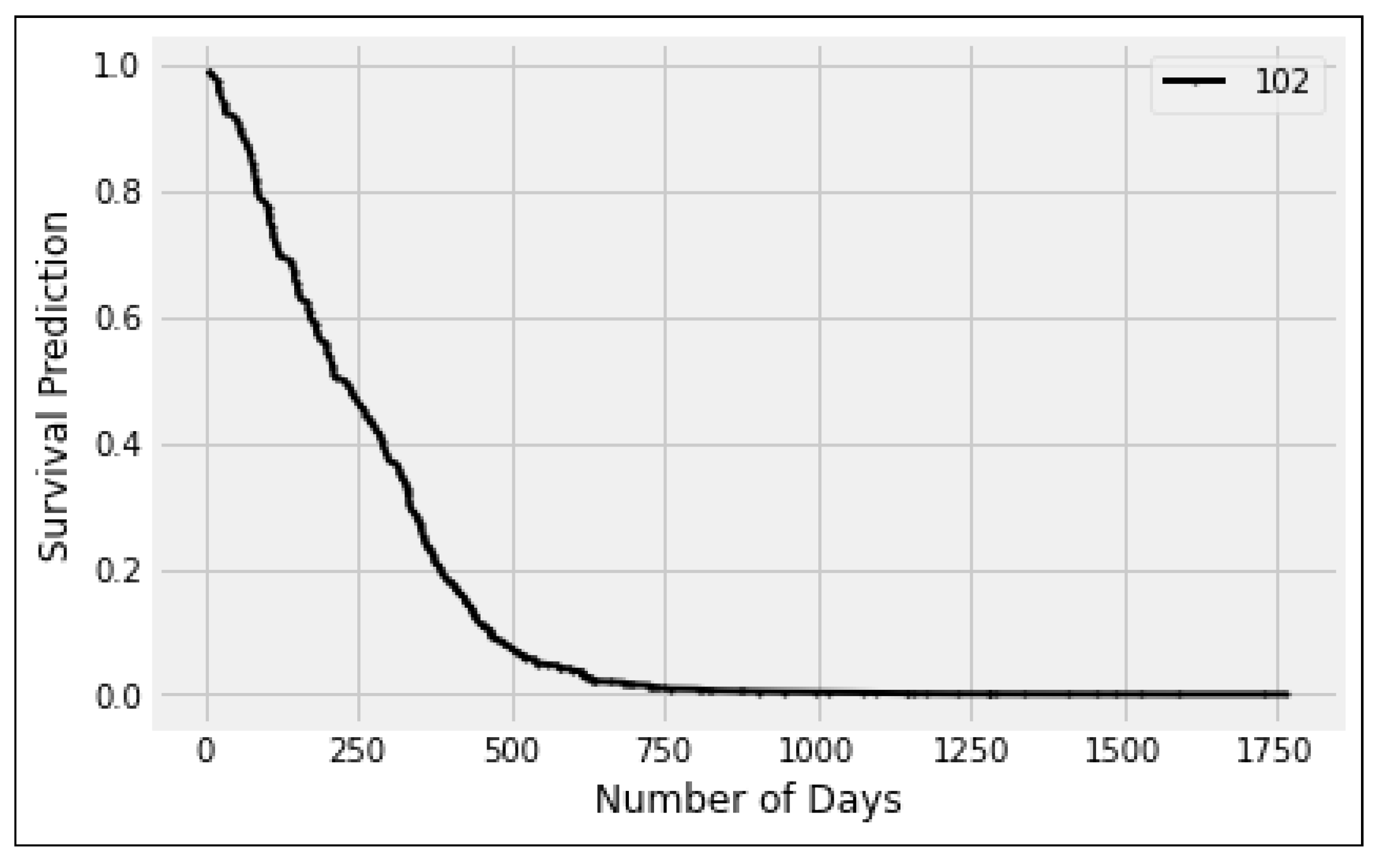
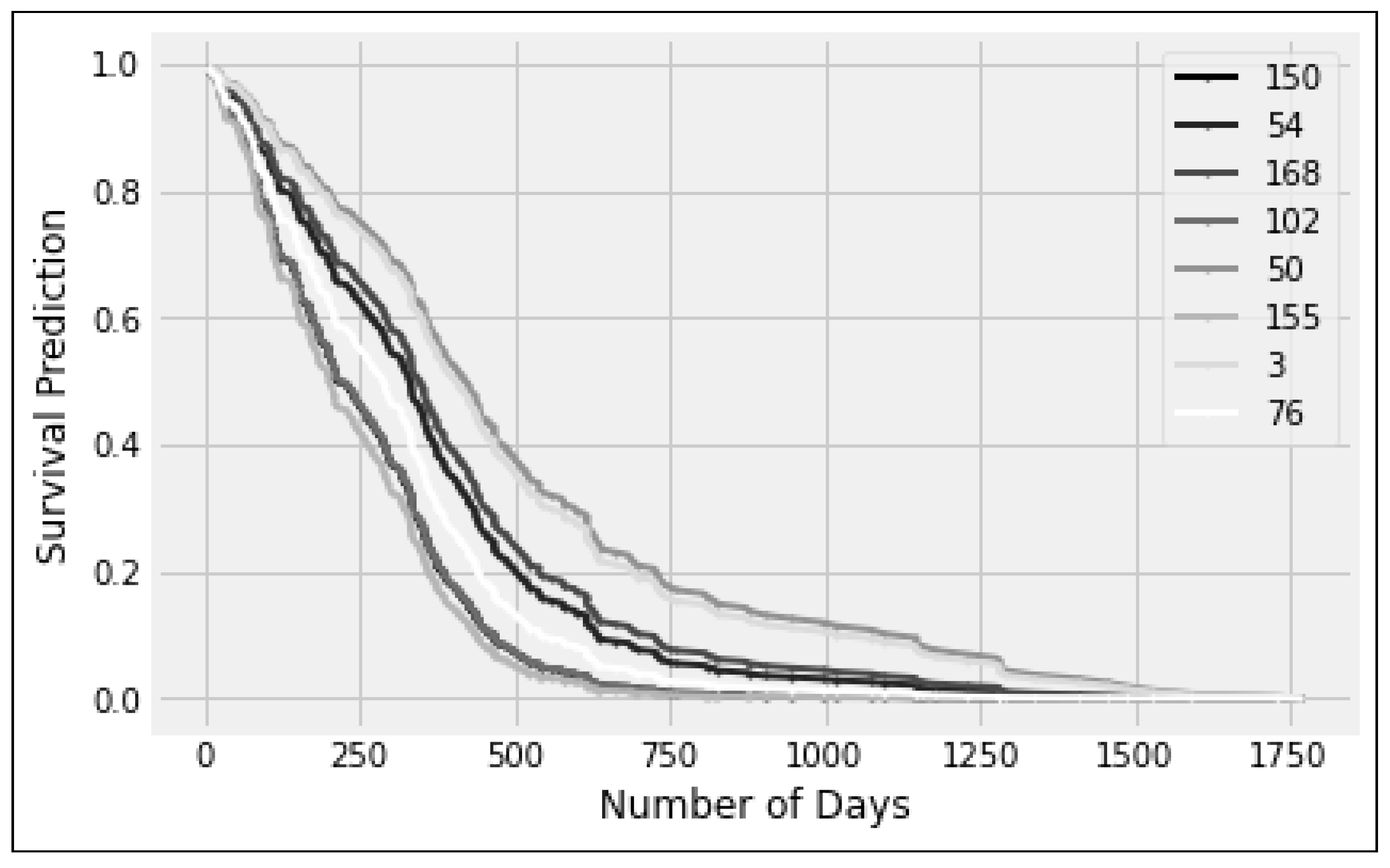
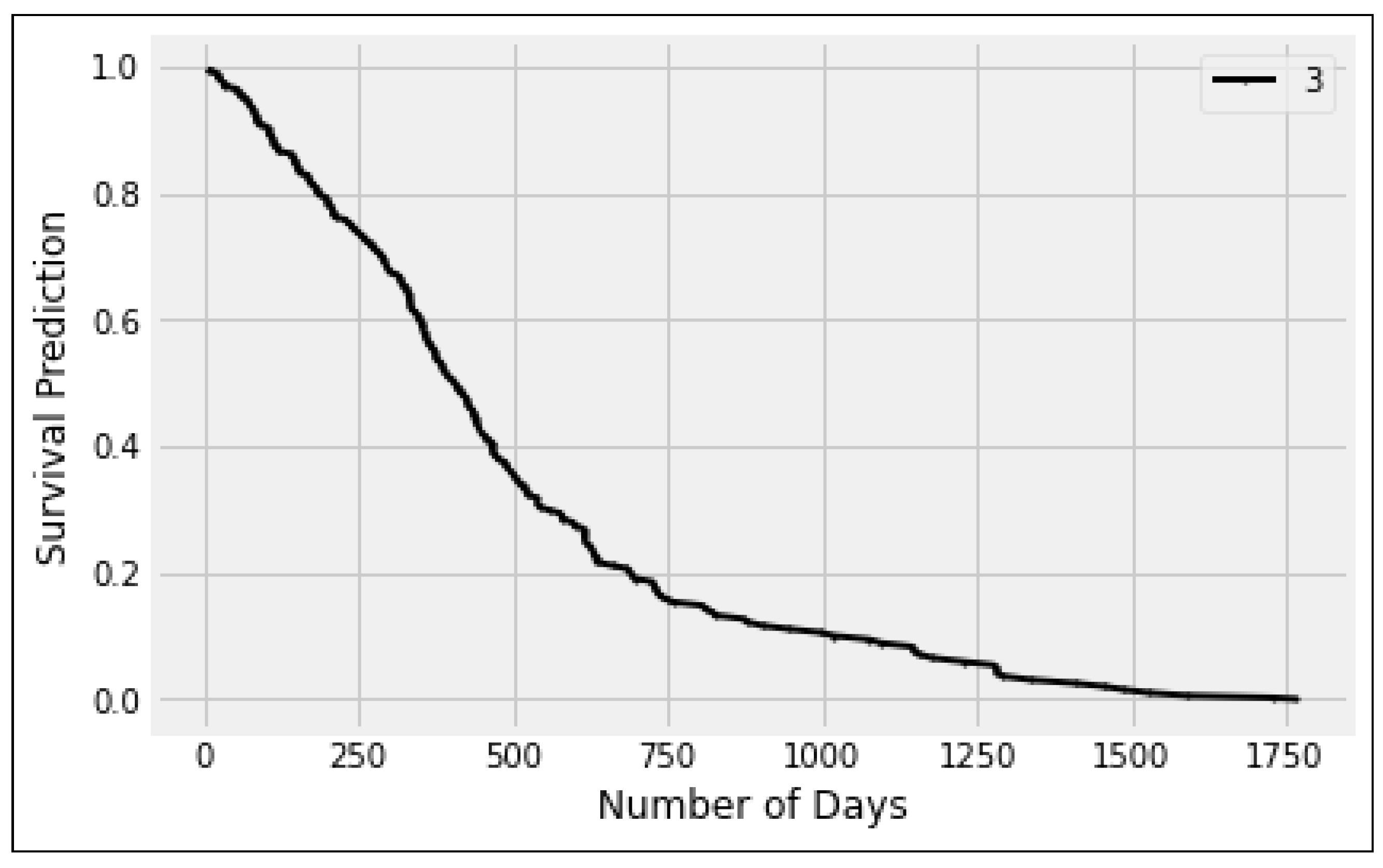
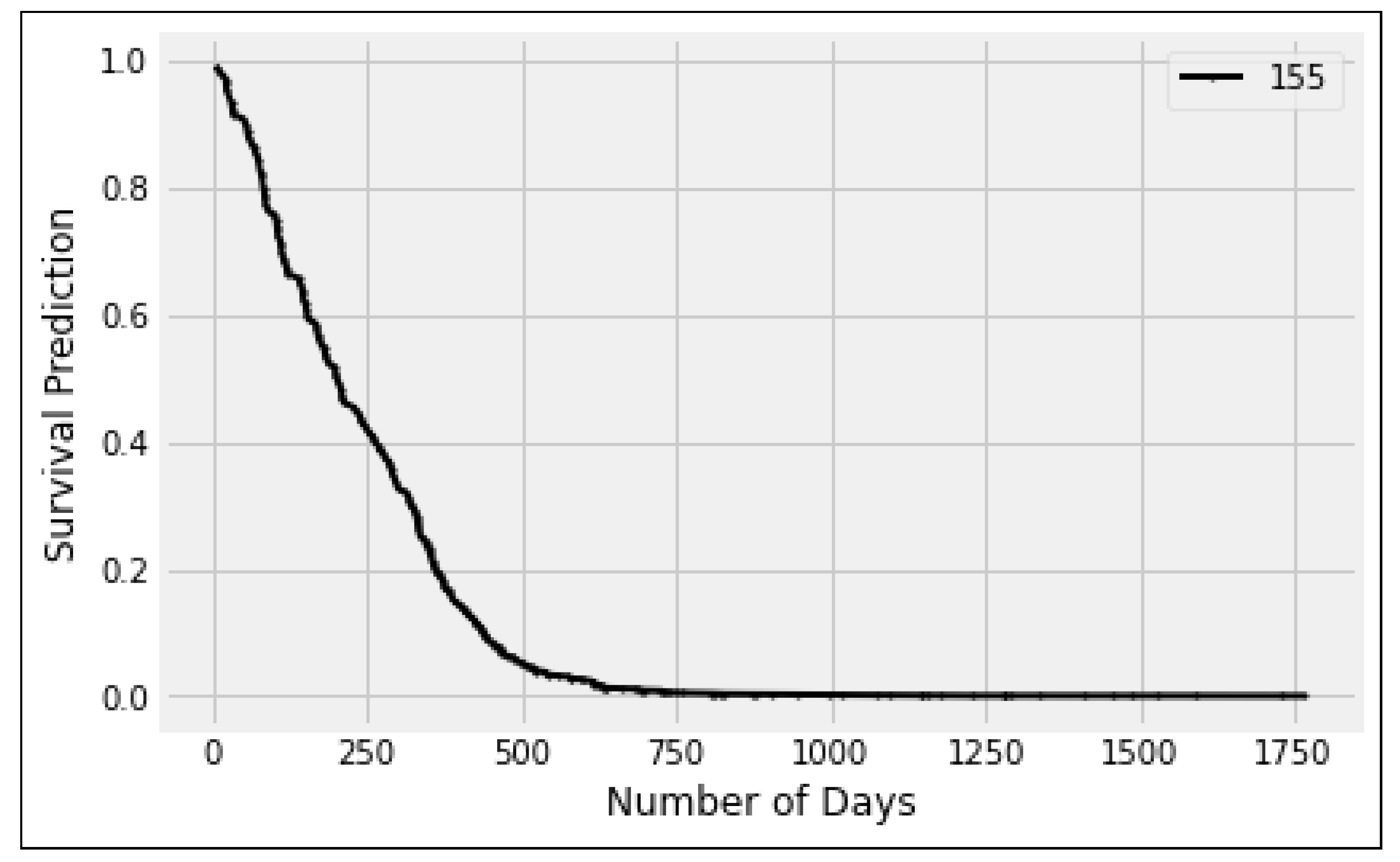
4.3.3. Survival Time Prediction
4.4. Computational Efficiency
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rajinikanth, V.; Kadry, S.; Damasevicius, R.; Sujitha, R.A.; Balaji, G.; Mohammed, M.A. Glioma/Glioblastoma Detection in Brain MRI using Pre-trained Deep-Learning Scheme. In Proceedings of the 2022 3rd International Conference on Intelligent Computing, Instrumentation and Control Technologies: Computational Intelligence for Smart Systems, ICICICT 2022, Kannur, India, 11–12 August 2022; pp. 987–990. [Google Scholar]
- Rao, C.S.; Karunakara, K. Efficient detection and classification of brain tumor using kernel based SVM for MRI. Multimed. Tools Appl. 2022, 81, 7393–7417. [Google Scholar] [CrossRef]
- Koong, K.; Preda, V.; Jian, A.; Liquet-Weiland, B.; Di Ieva, A. Application of artificial intelligence and radiomics in pituitary neuroendocrine and sellar tumors: A quantitative and qualitative synthesis. Neuroradiology 2021, 64, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Narmatha, C.; Eljack, S.M.; Tuka, A.A.R.M.; Manimurugan, S.; Mustafa, M. A hybrid fuzzy brain-storm optimization algorithm for the classification of brain tumor MRI images. J. Ambient. Intell. Humaniz. Comput. 2020, 1–9. [Google Scholar] [CrossRef]
- Papic, V.; Lasica, N.; Jelaca, B.; Vuckovic, N.; Kozic, D.; Djilvesi, D.; Fimic, M.; Golubovic, J.; Pajicic, F.; Vulekovic, P. Primary intraparenchymal meningiomas: A case report and a systematic review. World Neurosurg. 2021, 153, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Rehman, M.U.; Cho, S.; Kim, J.H.; Chong, K.T. Bu-net: Brain tumor segmentation using modified u-net architecture. Electronics 2020, 9, 2203. [Google Scholar] [CrossRef]
- Öksüz, C.; Urhan, O.; Güllü, M.K. Brain tumor classification using the fused features extracted from expanded tumor region. Biomed. Signal Process. Control 2022, 72, 103356. [Google Scholar] [CrossRef]
- Park, J.H.; de Lomana, A.L.G.; Marzese, D.M.; Juarez, T.; Feroze, A.; Hothi, P.; Cobbs, C.; Patel, A.P.; Kesari, S.; Huang, S.; et al. A systems approach to brain tumor treatment. Cancers 2021, 13, 3152. [Google Scholar] [CrossRef]
- Nazir, M.; Shakil, S.; Khurshid, K. Role of deep learning in brain tumor detection and classification (2015 to 2020): A review. Comput. Med. Imaging Graph. 2021, 91, 101940. [Google Scholar] [CrossRef] [PubMed]
- Cancer.Net Editorial Board, “Brain Tumor,” ASCO.org, Alexandria, VA, United States of America (USA). 2023. Available online: https://www.cancer.net/cancer-types/brain-tumor/statistics (accessed on 1 March 2023).
- Reddy, S.; Tatiparti, K.; Sau, S.; Iyer, A.K. Recent advances in nano delivery systems for blood-brain barrier (BBB) penetration and targeting of brain tumors. Drug Discov. Today 2021, 26, 1944–1952. [Google Scholar] [CrossRef]
- Muzammil, S.R.; Maqsood, S.; Haider, S.; Damaševičius, R. CSID: A novel multimodal image fusion algorithm for enhanced clinical diagnosis. Diagnostics 2020, 10, 904. [Google Scholar] [CrossRef]
- Woźniak, M.; Siłka, J.; Wieczorek, M. Deep neural network correlation learning mechanism for CT brain tumor detection. Neural Comput. Appl. 2021, 1–16. [Google Scholar] [CrossRef]
- Khan, M.A.; Ashraf, I.; Alhaisoni, M.; Damaševičius, R.; Scherer, R.; Rehman, A.; Bukhari, S.A.C. Multimodal brain tumor classification using deep learning and robust feature selection: A machine learning application for radiologists. Diagnostics 2020, 10, 565. [Google Scholar] [CrossRef] [PubMed]
- Jansson, D.; Dieriks, V.B.; Rustenhoven, J.; Smyth, L.C.; Scotter, E.; Aalderink, M.; Feng, S.; Johnson, R.; Schweder, P.; Mee, E.; et al. Cardiac glycosides target barrier inflammation of the vasculature, meninges and choroid plexus. Commun. Biol. 2021, 4, 1–17. [Google Scholar] [CrossRef]
- Thayumanavan, M.; Ramasamy, A. An efficient approach for brain tumor detection and segmentation in MR brain images using random forest classifier. Concurr. Eng. 2021, 29, 266–274. [Google Scholar] [CrossRef]
- Muhammad, K.; Khan, S.; Del Ser, J.; De Albuquerque, V.H.C. Deep learning for multigrade brain tumor classification in smart healthcare systems: A prospective survey. IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 507–522. [Google Scholar] [CrossRef] [PubMed]
- Chahal, P.K.; Pandey, S.; Goel, S. A survey on brain tumor detection techniques for MR images. Multimed. Tools Appl. 2020, 79, 21771–21814. [Google Scholar] [CrossRef]
- Tiwari, A.; Srivastava, S.; Pant, M. Brain tumor segmentation and classification from magnetic resonance images: Review of selected methods from 2014 to 2019. Pattern Recognit. Lett. 2020, 131, 244–260. [Google Scholar] [CrossRef]
- Amian, M.; Soltaninejad, M. Multi-resolution 3D CNN for MRI brain tumor segmentation and survival prediction. In Proceedings of the International MICCAI Brainlesion Workshop, Shenzhen, China, 17 October 2019; pp. 221–230. [Google Scholar]
- Benzekry, S.; Lamont, C.; Beheshti, A.; Tracz, A.; Ebos, J.M.; Hlatky, L.; Hahnfeldt, P. Classical mathematical models for description and prediction of experimental tumor growth. PLoS Comput. Biol. 2014, 10, e1003800. [Google Scholar] [CrossRef]
- Bakas, S.; Reyes, M.; Jakab, A.; Bauer, S.; Rempfler, M.; Crimi, A.; Shinohara, R.T.; Berger, C.; Ha, S.M.; Rozycki, M.; et al. Identifying the best machine learning algorithms for brain tumor segmentation, progression assessment, and overall survival prediction in the BRATS challenge. arXiv 2018, arXiv:1811.02629. [Google Scholar]
- Jeong, J.J.; Tariq, A.; Adejumo, T.; Trivedi, H.; Gichoya, J.W.; Banerjee, I. Systematic review of generative adversarial networks (gans) for medical image classification and segmentation. J. Digit. Imaging 2022, 35, 137–152. [Google Scholar] [CrossRef]
- Ilhan, A.; Sekeroglu, B.; Abiyev, R. Brain tumor segmentation in MRI images using nonparametric localization and enhancement methods with U-net. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Saba, T. Recent advancement in cancer detection using machine learning: Systematic survey of decades, comparisons and challenges. J. Infect. Public Health 2020, 13, 1274–1289. [Google Scholar] [CrossRef] [PubMed]
- Lavanyadevi, R.; Machakowsalya, M.; Nivethitha, J.; Kumar, A.N. Brain tumor classification and segmentation in MRI images using PNN. In Proceedings of the 2017 IEEE International Conference on Electrical, Instrumentation and Communication Engineering (ICEICE), Karur, Tamilnadu, India, 27–28 April 2017; pp. 1–6. [Google Scholar]
- AlJame, M.; Ahmad, I.; Imtiaz, A.; Mohammed, A. Ensemble learning model for diagnosing COVID-19 from routine blood tests. Inform. Med. Unlocked 2020, 21, 100449. [Google Scholar] [CrossRef] [PubMed]
- Ge, C.; Gu, I.Y.H.; Jakola, A.S.; Yang, J. Enlarged training dataset by pairwise gans for molecular-based brain tumor classification. IEEE Access 2020, 8, 22560–22570. [Google Scholar] [CrossRef]
- Çinarer, G.; Emiroğlu, B.G.; Yurttakal, A.H. Prediction of glioma grades using deep learning with wavelet radiomic features. Appl. Sci. 2020, 10, 6296. [Google Scholar] [CrossRef]
- Rajinikanth, V.; Kadry, S.; Nam, Y. Convolutional-neural-network assisted segmentation and svm classification of brain tumor in clinical mri slices. Inf. Technol. Control 2021, 50, 342–356. [Google Scholar] [CrossRef]
- Badjie, B.; Deniz Ülker, E. A Deep Transfer Learning Based Architecture for Brain Tumor Classification Using MR Images. Inf. Technol. Control 2022, 51, 332–344. [Google Scholar] [CrossRef]
- Kurdi, S.Z.; Ali, M.H.; Jaber, M.M.; Saba, T.; Rehman, A. Brain Tumor Classification Using Meta-Heuristic Optimized Convolutional Neural Networks. J. Pers. Med. 2023, 13, 181. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, L.W.; Zile, M.; Bennett, T.D.; Kueffer, F.J.; Jessup, M.L.; Adamson, P.; Abraham, W.T.; Manda, V.; Bourge, R.C. Chronic ambulatory intracardiac pressures and future heart failure events. Circ. Heart Fail. 2010, 3, 580–587. [Google Scholar] [CrossRef]
- Husain, H.; Thamrin, S.A.; Tahir, S.; Mukhlisin, A.; Apriani, M.M. The application of extended Cox proportional hazard method for estimating survival time of breast cancer. In Proceedings of the Journal of Physics: Conference Series, Makassar, Indonesia, 2–3 November 2017; Volume 979, p. 012087. [Google Scholar]
- Islam, M.; Wijethilake, N.; Ren, H. Glioblastoma multiforme prognosis: MRI missing modality generation, segmentation and radiogenomic survival prediction. Comput. Med. Imaging Graph. 2021, 91, 101906. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, A.; Ali, S.; Shah, I. Online disease risk monitoring using DEWMA control chart. Expert Syst. Appl. 2021, 180, 115059. [Google Scholar] [CrossRef]
- Yeganeh, A.; Shadman, A.; Shongwe, S.C.; Abbasi, S.A. Employing evolutionary artificial neural network in risk-adjusted monitoring of surgical performance. Neural Comput. Appl. 2023, 1–17. [Google Scholar] [CrossRef]
- Nguyen, D.; Nguyen, H.; Ong, H.; Le, H.; Ha, H.; Duc, N.T.; Ngo, H.T. Ensemble learning using traditional machine learning and deep neural network for diagnosis of Alzheimer’s disease. IBRO Neurosci. Rep. 2022, 13, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Wang, X.; Zhang, X.; Zhang, C.; Zhang, Z.; Zhang, K.; Wang, S. A Novel Attention-Mechanism Based Cox Survival Model by Exploiting Pan-Cancer Empirical Genomic Information. Cells 2022, 11, 1421. [Google Scholar] [CrossRef] [PubMed]
- Moradmand, H.; Aghamiri, S.M.R.; Ghaderi, R.; Emami, H. The role of deep learning-based survival model in improving survival prediction of patients with glioblastoma. Cancer Med. 2021, 10, 7048–7059. [Google Scholar] [CrossRef]
- Hao, J.; Kosaraju, S.C.; Tsaku, N.Z.; Song, D.H.; Kang, M. PAGE-Net: Interpretable and integrative deep learning for survival analysis using histopathological images and genomic data. In Proceedings of the Pacific Symposium on Biocomputing, Kohala Coast, HI, USA, 3–7 January 2020; pp. 355–366. [Google Scholar]
- Senders, J.T.; Staples, P.; Mehrtash, A.; Cote, D.J.; Taphoorn, M.J.; Reardon, D.A.; Gormley, W.B.; Smith, T.R.; Broekman, M.L.; Arnaout, O. An online calculator for the prediction of survival in glioblastoma patients using classical statistics and machine learning. Neurosurgery 2020, 86, E184–E192. [Google Scholar] [CrossRef]
- Dong, W.; Zeng, H.; Peng, Y.; Gao, X.; Peng, A. A deep learning approach with data augmentation for median filtering forensics. Multimed. Tools Appl. 2022, 81, 11087–11105. [Google Scholar] [CrossRef]
- Bakas, S.; Akbari, H.; Sotiras, A.; Bilello, M.; Rozycki, M.; Kirby, J.S.; Freymann, J.B.; Farahani, K.; Davatzikos, C. Advancing the cancer genome atlas glioma MRI collections with expert segmentation labels and radiomic features. Sci. Data 2017, 4, 1–13. [Google Scholar] [CrossRef]
- Menze, B.; Isensee, F.; Wiest, R.; Wiestler, B.; Maier-Hein, K.; Reyes, M.; Bakas, S. Analyzing magnetic resonance imaging data from glioma patients using deep learning. Comput. Med. Imaging Graph. 2021, 88, 101828. [Google Scholar] [CrossRef]
- Khan, M.A.; Khan, A.; Alhaisoni, M.; Alqahtani, A.; Alsubai, S.; Alharbi, M.; Malik, N.A. Multimodal brain tumor detection and classification using deep saliency map and improved dragonfly optimization algorithm. Int. J. Imaging Syst. Technol. 2022, 33, 572–587. [Google Scholar] [CrossRef]
- Maqsood, S.; Damaševičius, R.; Maskeliūnas, R. Multi-Modal Brain Tumor Detection Using Deep Neural Network and Multiclass SVM. Medicina 2022, 58, 1090. [Google Scholar] [CrossRef] [PubMed]
- Kheradmandi, N.; Mehranfar, V. A critical review and comparative study on image segmentation-based techniques for pavement crack detection. Constr. Build. Mater. 2022, 321, 126162. [Google Scholar] [CrossRef]
- Dubey, R.; Hanmandlu, M.; Gupta, S.; Gupta, S. Region growing for MRI brain tumor volume analysis. Indian J. Sci. Technol. 2009, 2, 26–31. [Google Scholar] [CrossRef]
- Rohera, D.; Shethna, H.; Patel, K.; Thakker, U.; Tanwar, S.; Gupta, R.; Hong, W.C.; Sharma, R. A Taxonomy of Fake News Classification Techniques: Survey and Implementation Aspects. IEEE Access 2022, 10, 30367–30394. [Google Scholar] [CrossRef]
- Tulbure, A.A.; Tulbure, A.A.; Dulf, E.H. A review on modern defect detection models using DCNNs–Deep convolutional neural networks. J. Adv. Res. 2022, 35, 33–48. [Google Scholar] [CrossRef]
- Maqsood, S.; Damasevicius, R.; Shah, F.M. An efficient approach for the detection of brain tumor using fuzzy logic and U-NET CNN classification. In Proceedings of the International Conference on Computational Science and Its Applications, Cagliari, Italy, 13–16 September 2021; pp. 105–118. [Google Scholar]
- Fauziah, A.; Safitri, D.; Meiza, A. Survival analysis with the Cox Proportional Hazard Method to determine the factors that affect how long the Large-Scale Social Distancing (LSSD) will applied in various areas affected by the COVID-19 pandemic. In Proceedings of the Journal of Physics: Conference Series, Bandar Lampung, Indonesia, 3–4 September 2020; Volume 1751, p. 012004. [Google Scholar]
- Rehman, M.U.; Cho, S.; Kim, J.; Chong, K.T. BrainSeg-Net: Brain tumor MR image segmentation via enhanced encoder–decoder network. Diagnostics 2021, 11, 169. [Google Scholar] [CrossRef] [PubMed]
- Al-Saffar, Z.A.; Yildirim, T. A hybrid approach based on multiple eigenvalues selection (MES) for the automated grading of a brain tumor using MRI. Comput. Methods Programs Biomed. 2021, 201, 105945. [Google Scholar] [CrossRef]
- Jin, H.; Chollet, F.; Song, Q.; Hu, X. AutoKeras: An AutoML Library for Deep Learning. J. Mach. Learn. Res. 2023, 24, 1–6. [Google Scholar]
- Bilic, P.; Christ, P.; Li, H.B.; Vorontsov, E.; Ben-Cohen, A.; Kaissis, G.; Szeskin, A.; Jacobs, C.; Mamani, G.E.H.; Chartrand, G.; et al. The liver tumor segmentation benchmark (lits). Med. Image Anal. 2023, 84, 102680. [Google Scholar] [CrossRef]
- Chang, Y.; Zheng, Z.; Sun, Y.; Zhao, M.; Lu, Y.; Zhang, Y. Dpafnet: A residual dual-path attention-fusion convolutional neural network for multimodal brain tumor segmentation. Biomed. Signal Process. Control 2023, 79, 104037. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Minimum | Maximum |
|---|---|---|
| Age | 18.975 | 86.652 |
| Survival Days | 5 | 1767 |
| GTR Status | 1 (N/A) | 3 (GTR) |
| Tumor Volume | 7.285 | 227.126 |
| Tumor Class | 76 (LGG) | 293 (HGG) |
| Dice Coef | Accuracy | Precision | Sensitivity | Specificity |
|---|---|---|---|---|
| 0.25 | 0.96 | 0.95 | 0.90 | 0.99 |
| Modality | Accuracy | Precision | F1 Score |
|---|---|---|---|
| T1 | 94.00 | 93.81 | 95.77 |
| T1ce | 94.00 | 93.81 | 95.77 |
| T2 | 94.38 | 93.62 | 95.65 |
| Flair | 93.23 | 93.81 | 95.77 |
| Segmented | 94.38 | 93.81 | 95.77 |
| Average | 94.20% | 93.77% | 95.75% |
| Model | lifeline.CoxPHFitter |
|---|---|
| Duration Column | days |
| Event Column | event |
| Baseline Estimation | Breslow |
| Number of observations | 228 |
| Number of events observed | 228 |
| Partial log-likelihood | −994.44 |
| Factor | Coef | Exp (Coef) | Se (Coef) | Coef Lower 95% | Coef Upper 95% | Exp (Coef) Lower 95% | Exp (Coef) Upper 95% | z | p | −log2(p) |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 0.04 | 1.04 | 0.01 | 0.02 | 0.05 | 1.02 | 1.05 | 5.45 | <0.005 | 24.26 |
| GTR | 0.04 | 1.04 | 0.07 | −0.10 | 0.17 | 0.90 | 1.19 | 0.52 | 0.60 | 0.73 |
| Class | −0.64 | 0.53 | 0.37 | −1.36 | 0.08 | 0.26 | 1.08 | −1.75 | 0.08 | 3.63 |
| Volume | 0.00 | 1.00 | 0.00 | −0.00 | 0.08 | 1.00 | 1.00 | −1.73 | 0.08 | 3.58 |
| Concordance | 0.74 |
| Partial AIC | 1999.20 |
| Log-likelihood ratio test | 38.17 on 4 df |
| −log2(p) of ll-ratio test | 23.20 |
| Risk Factor | Coefficients | Exp (Coef) |
|---|---|---|
| Tumor Volume | 0.01 | 1.00 |
| Tumor Type | 0.15 | 1.16 |
| Patient’s Age | 0.03 | 1.04 |
| Extent of GTR | 0.04 | 1.04 |
| Patient’s No. | Age (Years) | GTR | Tumor Class | Volume |
|---|---|---|---|---|
| 102 | 85.942 | 1 | HGG | 58.208 |
| Patient’s No. | Age | GTR | Class | Volume |
|---|---|---|---|---|
| 150 | 63.805 | 3 | 1 | 095.391 |
| 054 | 66.510 | 3 | 2 | 118.394 |
| 168 | 64.378 | 3 | 2 | 099.624 |
| 102 | 85.942 | 1 | 2 | 058.208 |
| 050 | 52.348 | 3 | 2 | 121.570 |
| 155 | 81.112 | 3 | 2 | 162.623 |
| 003 | 39.068 | 1 | 1 | 103.496 |
| 076 | 79.211 | 1 | 2 | 050.183 |
| Patient’s No. | Age (Years) | GTR | Tumor Class | Volume |
|---|---|---|---|---|
| 3 | 39.068 | 1 | LGG | 103.496 |
| 155 | 81.112 | 3 | HGG | 162.623 |
| S No. | Author(s) | Dice Score |
|---|---|---|
| 1. | Rehman et al. [54] | 0.790 |
| 2. | Rehman et al. [6] | 0.837 |
| 3. | Amian et al. [20] | 0.840 |
| 4. | Ilhan et al. [24] | 0.880 |
| 5. | Islam et al. [35] | 0.899 |
| 6. | The proposed ETISTP model | 0.902 |
| S No. | Author(s) | Accuracy | Precision | F1 Score |
|---|---|---|---|---|
| 1. | Chenjie et al. [28] | 88.22% | 86.76% | 85.18% |
| 2. | Zahraa et al. [55] | 91.02% | 87.07% | 88.44% |
| 3. | Attique et al. [14] | 92.50% | 88.37% | 89.12% |
| 4. | Narmatha et al. [4] | 93.85% | 94.77% | 95.42% |
| 5. | The proposed ETISTP model | 94.20% | 95.77% | 95.75% |
| S No. | Author(s) | Method(s) | Concordance | p-Value |
|---|---|---|---|---|
| 1. | Moradmand et al. [40] | CoxPH | 0.58 | 0.006 |
| 2. | Hao et al. [41] | PAGE-Net | 0.64 | 0.007 |
| 3. | Senders et al. [42] | Statistical machine learning algorithm | 0.69 | 0.008 |
| 4. | Meng et al. [39] | SAVAE-COX | 0.71 | 0.009 |
| 5. | The proposed ETISTP model | CoxPH using the integrated parameters | 0.74 | 0.050 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussain, S.; Haider, S.; Maqsood, S.; Damaševičius, R.; Maskeliūnas, R.; Khan, M. ETISTP: An Enhanced Model for Brain Tumor Identification and Survival Time Prediction. Diagnostics 2023, 13, 1456. https://doi.org/10.3390/diagnostics13081456
Hussain S, Haider S, Maqsood S, Damaševičius R, Maskeliūnas R, Khan M. ETISTP: An Enhanced Model for Brain Tumor Identification and Survival Time Prediction. Diagnostics. 2023; 13(8):1456. https://doi.org/10.3390/diagnostics13081456
Chicago/Turabian StyleHussain, Shah, Shahab Haider, Sarmad Maqsood, Robertas Damaševičius, Rytis Maskeliūnas, and Muzammil Khan. 2023. "ETISTP: An Enhanced Model for Brain Tumor Identification and Survival Time Prediction" Diagnostics 13, no. 8: 1456. https://doi.org/10.3390/diagnostics13081456