
A Diagnostic Classifier Based on Circulating miRNA Pairs for COPD Using a Machine Learning Approach


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Pre-Processing
2.2. Construction of miRNA Pair-Based Signature
2.3. Machine Learning Model Development and Evaluation
2.4. Study Subjects
2.5. Quantitative Real-Time Polymerase Chain Reaction (qRT-PCR)
2.6. Statistical Analyses
3. Results
3.1. Dataset Description
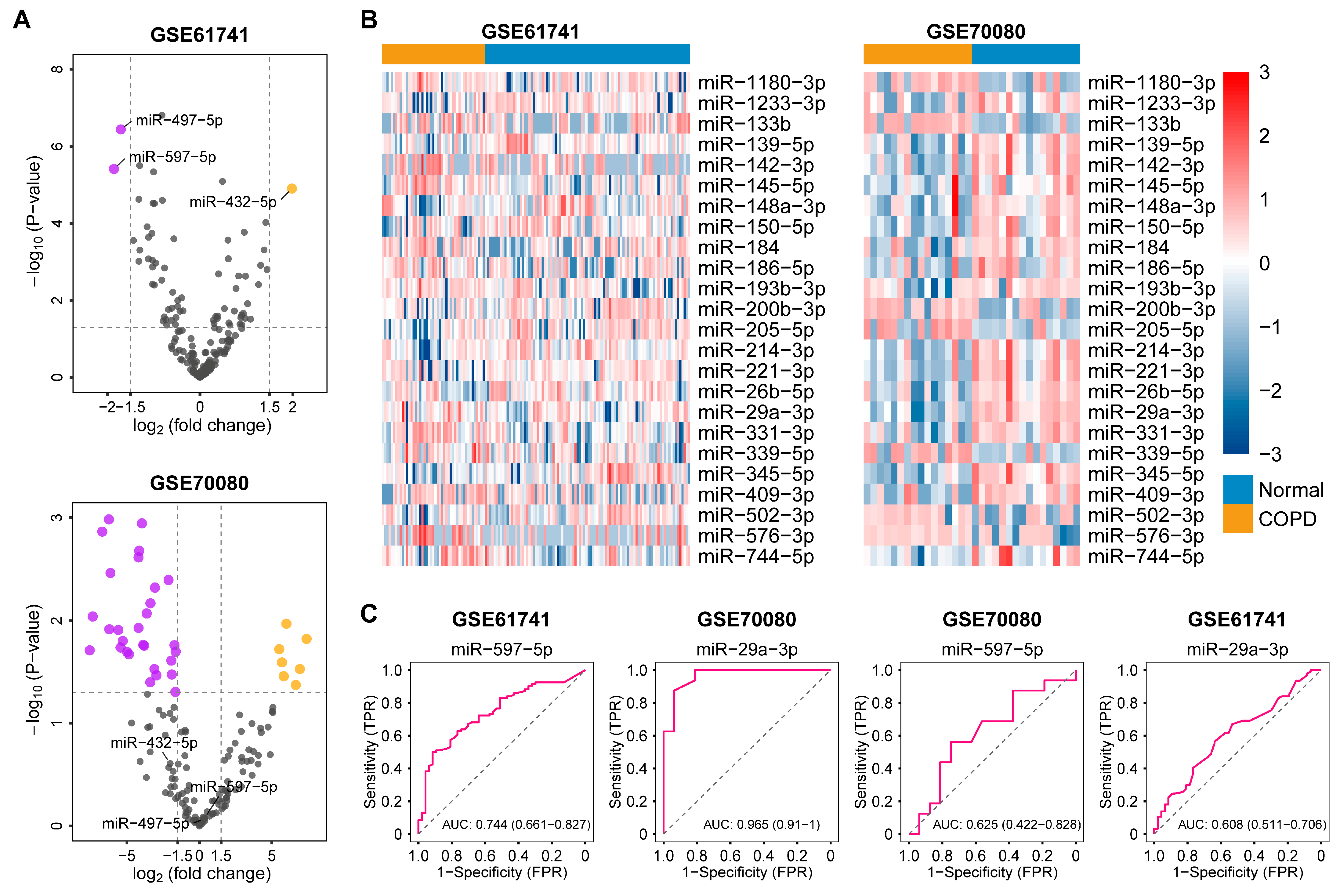
3.2. The Expression of Single miRNAs and miRNA Signature Failed in COPD Diagnosis
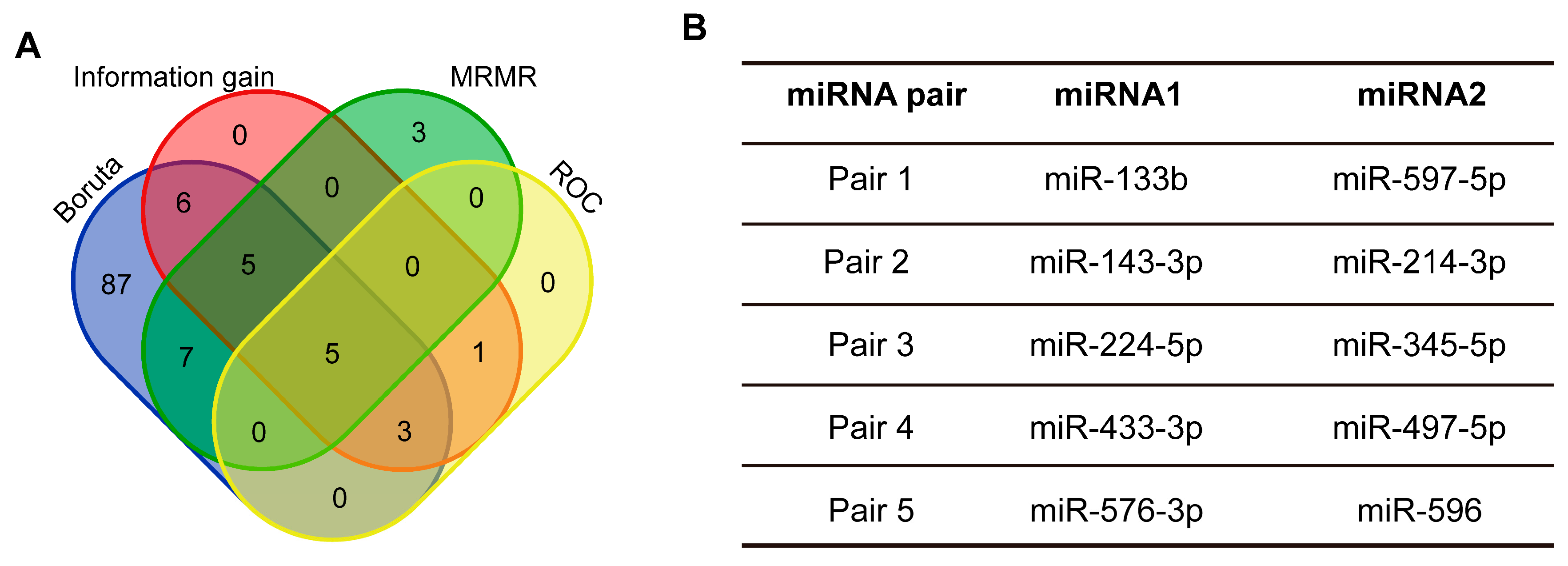
3.3. Construction of miRNA Pairs and Feature Selection
3.4. Machine Learning Model Establishment and Evaluation
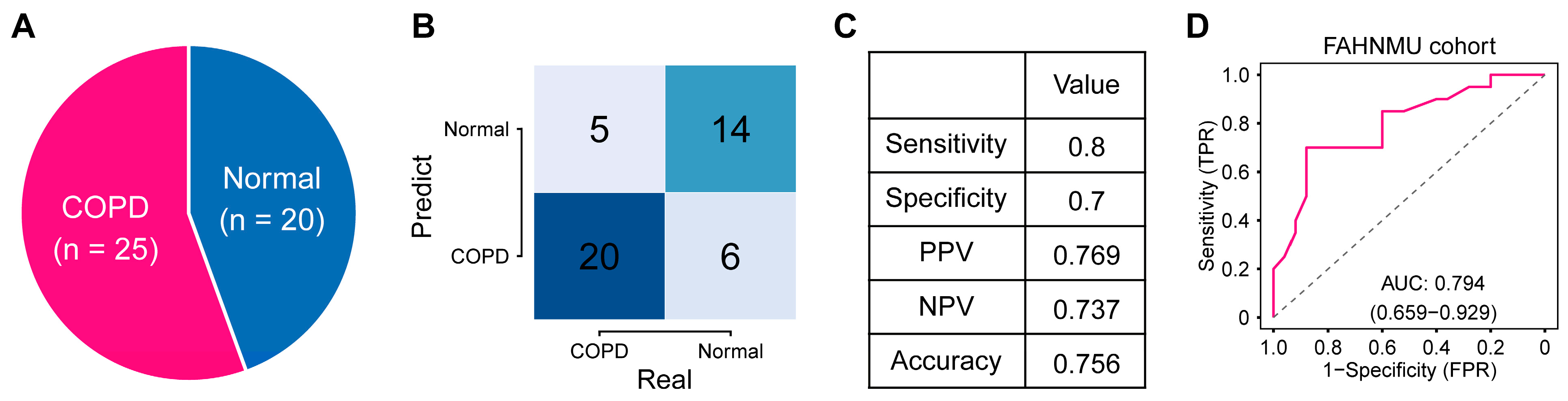
3.5. Validation of the miRNA Pair-Based Model in an External Cohort
3.6. Development of a Web Application for COPD Prediction
3.7. Functional Annotation of the miRNA Pairs in the Model
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Halpin, D.M.G.; Celli, B.R.; Criner, G.J.; Frith, P.; Varela, L.; Salvi, S.; Vogelmeier, C.F.; Chen, R.; Mortimer, K.; Montes de Oca, M. The GOLD Summit on Chronic Obstructive Pulmonary Disease in Low-and Middle-Income Countries. Int. J. Tuberc. Lung Dis. 2019, 23, 1131–1141. [Google Scholar] [CrossRef]
- 2023 GOLD Report. Available online: https://goldcopd.org/2023-gold-report-2/ (accessed on 31 January 2023).
- Vollmer, W.M.; Gíslason, T.; Burney, P.; Enright, P.L.; Gulsvik, A.; Kocabas, A.; Buist, A.S. Comparison of Spirometry Criteria for the Diagnosis of COPD: Results from the BOLD Study. Eur. Respir. J. 2009, 34, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Mizumura, K.; Cloonan, S.; Nakahira, K.; Bhashyam, A.R.; Cervo, M.; Kitada, T.; Glass, K.; Owen, C.A.; Mahmood, A.; Washko, G.R.; et al. Mitophagy-Dependent Necroptosis Contributes to the Pathogenesis of COPD. J. Clin. Investig. 2014, 124, 3987–4003. [Google Scholar] [CrossRef]
- Wadhwa, R.; Aggarwal, T.; Malyla, V.; Kumar, N.; Gupta, G.; Chellappan, D.K.; Dureja, H.; Mehta, M.; Satija, S.; Gulati, M.; et al. Identification of Biomarkers and Genetic Approaches toward Chronic Obstructive Pulmonary Disease. J. Cell. Physiol. 2019, 234, 16703–16723. [Google Scholar] [CrossRef] [PubMed]
- Szymczak, I.; Wieczfinska, J.; Pawliczak, R. Molecular Background of MiRNA Role in Asthma and COPD: An Updated Insight. BioMed Res. Int. 2016, 2016, 7802521. [Google Scholar] [CrossRef]
- Ezzie, M.E.; Crawford, M.; Cho, J.-H.; Orellana, R.; Zhang, S.; Gelinas, R.; Batte, K.; Yu, L.; Nuovo, G.; Galas, D.; et al. Gene Expression Networks in COPD: MicroRNA and MRNA Regulation. Thorax 2012, 67, 122–131. [Google Scholar] [CrossRef]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating MicroRNAs as Stable Blood-Based Markers for Cancer Detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef]
- Benz, F.; Roy, S.; Trautwein, C.; Roderburg, C.; Luedde, T. Circulating MicroRNAs as Biomarkers for Sepsis. Int. J. Mol. Sci. 2016, 17, 78. [Google Scholar] [CrossRef] [PubMed]
- Greener, J.G.; Kandathil, S.M.; Moffat, L.; Jones, D.T. A Guide to Machine Learning for Biologists. Nat. Rev. Mol. Cell Biol. 2022, 23, 40–55. [Google Scholar] [CrossRef]
- Toh, T.S.; Dondelinger, F.; Wang, D. Looking beyond the Hype: Applied AI and Machine Learning in Translational Medicine. EBioMedicine 2019, 47, 607–615. [Google Scholar] [CrossRef]
- Walsh, J.A.; Rozycki, M.; Yi, E.; Park, Y. Application of Machine Learning in the Diagnosis of Axial Spondyloarthritis. Curr. Opin. Rheumatol. 2019, 31, 362–367. [Google Scholar] [CrossRef]
- Sammut, S.-J.; Crispin-Ortuzar, M.; Chin, S.-F.; Provenzano, E.; Bardwell, H.A.; Ma, W.; Cope, W.; Dariush, A.; Dawson, S.-J.; Abraham, J.E.; et al. Multi-Omic Machine Learning Predictor of Breast Cancer Therapy Response. Nature 2022, 601, 623–629. [Google Scholar] [CrossRef]
- Lee, Y.W.; Choi, J.W.; Shin, E.-H. Machine Learning Model for Predicting Malaria Using Clinical Information. Comput. Biol. Med. 2021, 129, 104151. [Google Scholar] [CrossRef] [PubMed]
- Mayampurath, A.; Ajith, A.; Anderson-Smits, C.; Chang, S.-C.; Brouwer, E.; Johnson, J.; Baltasi, M.; Volchenboum, S.; Devercelli, G.; Ciaccio, C.E. Early Diagnosis of Primary Immunodeficiency Disease Using Clinical Data and Machine Learning. J. Allergy Clin. Immunol. Pract. 2022, 10, 3002–3007.e5. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Leidinger, P.; Vogel, B.; Backes, C.; ElSharawy, A.; Galata, V.; Mueller, S.C.; Marquart, S.; Schrauder, M.G.; Strick, R.; et al. MiRNAs Can Be Generally Associated with Human Pathologies as Exemplified for MiR-144. BMC Med. 2014, 12, 224. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, A.R.; Bjaanæs, M.; LeBlanc, M.; Holm, A.M.; Bolstad, N.; Rubio, L.; Peñalver, J.C.; Cervera, J.; Mojarrieta, J.C.; López-Guerrero, J.A.; et al. A Unique Set of 6 Circulating MicroRNAs for Early Detection of Non-Small Cell Lung Cancer. Oncotarget 2016, 7, 37250–37259. [Google Scholar] [CrossRef]
- Xu, T.; Su, N.; Liu, L.; Zhang, J.; Wang, H.; Zhang, W.; Gui, J.; Yu, K.; Li, J.; Le, T.D. MiRBaseConverter: An R/Bioconductor Package for Converting and Retrieving MiRNA Name, Accession, Sequence and Family Information in Different Versions of MiRBase. BMC Bioinform. 2018, 19, 514. [Google Scholar] [CrossRef]
- Odhiambo Omuya, E.; Onyango Okeyo, G.; Waema Kimwele, M. Feature Selection for Classification Using Principal Component Analysis and Information Gain. Expert Syst. Appl. 2021, 174, 114765. [Google Scholar] [CrossRef]
- Ding, C.; Peng, H. Minimum Redundancy Feature Selection from Microarray Gene Expression Data. J. Bioinform. Comput. Biol. 2005, 3, 185–205. [Google Scholar] [CrossRef]
- Kursa, M.B.; Rudnicki, W.R. Feature Selection with the Boruta Package. J. Stat. Softw. 2010, 36, 1–13. [Google Scholar] [CrossRef]
- Ritchie, M.E.; Phipson, B.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. Limma Powers Differential Expression Analyses for RNA-Sequencing and Microarray Studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhou, B.; Pache, L.; Chang, M.; Khodabakhshi, A.H.; Tanaseichuk, O.; Benner, C.; Chanda, S.K. Metascape Provides a Biologist-Oriented Resource for the Analysis of Systems-Level Datasets. Nat. Commun. 2019, 10, 1523. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-Y.; Lin, Y.-C.-D.; Cui, S.; Huang, Y.; Tang, Y.; Xu, J.; Bao, J.; Li, Y.; Wen, J.; Zuo, H.; et al. MiRTarBase Update 2022: An Informative Resource for Experimentally Validated MiRNA–Target Interactions. Nucleic Acids Res. 2022, 50, D222–D230. [Google Scholar] [CrossRef]
- Mathers, C.D.; Loncar, D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed]
- Christenson, S.A.; Smith, B.M.; Bafadhel, M.; Putcha, N. Chronic Obstructive Pulmonary Disease. Lancet Lond. Engl. 2022, 399, 2227–2242. [Google Scholar] [CrossRef]
- Grasedieck, S.; Schöler, N.; Bommer, M.; Niess, J.H.; Tumani, H.; Rouhi, A.; Bloehdorn, J.; Liebisch, P.; Mertens, D.; Döhner, H.; et al. Impact of Serum Storage Conditions on MicroRNA Stability. Leukemia 2012, 26, 2414–2416. [Google Scholar] [CrossRef]
- Allegra, A.; Alonci, A.; Campo, S.; Penna, G.; Petrungaro, A.; Gerace, D.; Musolino, C. Circulating MicroRNAs: New Biomarkers in Diagnosis, Prognosis and Treatment of Cancer (Review). Int. J. Oncol. 2012, 41, 1897–1912. [Google Scholar] [CrossRef] [PubMed]
- Backes, C.; Meese, E.; Keller, A. Specific MiRNA Disease Biomarkers in Blood, Serum and Plasma: Challenges and Prospects. Mol. Diagn. Ther. 2016, 20, 509–518. [Google Scholar] [CrossRef]
- Rajasekaran, S.; Rajaguru, P.; Sudhakar Gandhi, P.S. MicroRNAs as Potential Targets for Progressive Pulmonary Fibrosis. Front. Pharmacol. 2015, 6, 254. [Google Scholar] [CrossRef]
- Rajasekaran, S.; Pattarayan, D.; Rajaguru, P.; Sudhakar Gandhi, P.S.; Thimmulappa, R.K. MicroRNA Regulation of Acute Lung Injury and Acute Respiratory Distress Syndrome. J. Cell. Physiol. 2016, 231, 2097–2106. [Google Scholar] [CrossRef]
- Hassan, T.; Carroll, T.P.; Buckley, P.G.; Cummins, R.; O’Neill, S.J.; McElvaney, N.G.; Greene, C.M. MiR-199a-5p Silencing Regulates the Unfolded Protein Response in Chronic Obstructive Pulmonary Disease and A1-Antitrypsin Deficiency. Am. J. Respir. Crit. Care Med. 2014, 189, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Leuenberger, C.; Schuoler, C.; Bye, H.; Mignan, C.; Rechsteiner, T.; Hillinger, S.; Opitz, I.; Marsland, B.; Faiz, A.; Hiemstra, P.S.; et al. MicroRNA-223 Controls the Expression of Histone Deacetylase 2: A Novel Axis in COPD. J. Mol. Med. Berl. Ger. 2016, 94, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Christenson, S.A.; Brandsma, C.-A.; Campbell, J.D.; Knight, D.A.; Pechkovsky, D.V.; Hogg, J.C.; Timens, W.; Postma, D.S.; Lenburg, M.; Spira, A. MiR-638 Regulates Gene Expression Networks Associated with Emphysematous Lung Destruction. Genome Med. 2013, 5, 114. [Google Scholar] [CrossRef]
- Latorre, I.; Leidinger, P.; Backes, C.; Domínguez, J.; Souza-Galvão, M.L.; de Maldonado, J.; Prat, C.; Ruiz-Manzano, J.; Sánchez, F.; Casas, I.; et al. A Novel Whole-Blood MiRNA Signature for a Rapid Diagnosis of Pulmonary Tuberculosis. Eur. Respir. J. 2015, 45, 1173–1176. [Google Scholar] [CrossRef]
- Schwarzenbach, H.; Milde-Langosch, K.; Steinbach, B.; Müller, V.; Pantel, K. Diagnostic Potential of PTEN-Targeting MiR-214 in the Blood of Breast Cancer Patients. Breast Cancer Res. Treat. 2012, 134, 933–941. [Google Scholar] [CrossRef]
- Leidinger, P.; Backes, C.; Deutscher, S.; Schmitt, K.; Mueller, S.C.; Frese, K.; Haas, J.; Ruprecht, K.; Paul, F.; Stähler, C.; et al. A Blood Based 12-MiRNA Signature of Alzheimer Disease Patients. Genome Biol. 2013, 14, R78. [Google Scholar] [CrossRef]
- Zampetaki, A.; Kiechl, S.; Drozdov, I.; Willeit, P.; Mayr, U.; Prokopi, M.; Mayr, A.; Weger, S.; Oberhollenzer, F.; Bonora, E.; et al. Plasma MicroRNA Profiling Reveals Loss of Endothelial MiR-126 and Other MicroRNAs in Type 2 Diabetes. Circ. Res. 2010, 107, 810–817. [Google Scholar] [CrossRef]
- Wang, X.; Sundquist, J.; Zöller, B.; Memon, A.A.; Palmér, K.; Sundquist, K.; Bennet, L. Determination of 14 Circulating MicroRNAs in Swedes and Iraqis with and without Diabetes Mellitus Type 2. PLoS ONE 2014, 9, e86792. [Google Scholar] [CrossRef]
- Sapre, N.; Hong, M.K.H.; Macintyre, G.; Lewis, H.; Kowalczyk, A.; Costello, A.J.; Corcoran, N.M.; Hovens, C.M. Curated MicroRNAs in Urine and Blood Fail to Validate as Predictive Biomarkers for High-Risk Prostate Cancer. PLoS ONE 2014, 9, e91729. [Google Scholar] [CrossRef]
- Leek, J.T.; Scharpf, R.B.; Bravo, H.C.; Simcha, D.; Langmead, B.; Johnson, W.E.; Geman, D.; Baggerly, K.; Irizarry, R.A. Tackling the Widespread and Critical Impact of Batch Effects in High-Throughput Data. Nat. Rev. Genet. 2010, 11, 733–739. [Google Scholar] [CrossRef]
- Qi, L.; Chen, L.; Li, Y.; Qin, Y.; Pan, R.; Zhao, W.; Gu, Y.; Wang, H.; Wang, R.; Chen, X.; et al. Critical Limitations of Prognostic Signatures Based on Risk Scores Summarized from Gene Expression Levels: A Case Study for Resected Stage I Non-Small-Cell Lung Cancer. Brief. Bioinform. 2016, 17, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Lightbody, G.; Haberland, V.; Browne, F.; Taggart, L.; Zheng, H.; Parkes, E.; Blayney, J.K. Review of Applications of High-Throughput Sequencing in Personalized Medicine: Barriers and Facilitators of Future Progress in Research and Clinical Application. Brief. Bioinform. 2019, 20, 1795–1811. [Google Scholar] [CrossRef] [PubMed]
- Van Peer, G.; Lefever, S.; Anckaert, J.; Beckers, A.; Rihani, A.; Van Goethem, A.; Volders, P.-J.; Zeka, F.; Ongenaert, M.; Mestdagh, P.; et al. MiRBase Tracker: Keeping Track of MicroRNA Annotation Changes. Database 2014, 2014, bau080. [Google Scholar] [CrossRef]
- Jing, J.; FengSen, L.; Zheng, L.; Dan, X.; Jing, J.; Jing, W. Effects of yiqi gubiao pills on expressions of miRNA of low FFMI COPD patients. Chin. J. Inf. Tradit. Chin. Med. 2019, 26, 16–22. [Google Scholar]
- Gharbi, S.; Khateri, S.; Soroush, M.R.; Shamsara, M.; Naeli, P.; Najafi, A.; Korsching, E.; Mowla, S.J. MicroRNA expression in serum samples of sulfur mustard veterans as a diagnostic gateway to improve care. PLoS ONE 2018, 13, e0194530. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Ye, M.; Wang, J.; Ye, L.; Jin, M. Construction of Potential MiRNA–MRNA Regulatory Network in COPD Plasma by Bioinformatics Analysis. Int. J. Chronic Obstruct. Pulm. Dis. 2020, 15, 2135–2145. [Google Scholar] [CrossRef]
- Shen, Y.; Wang, L.; Wu, Y.; Ou, Y.; Lu, H.; Yao, X. A Novel Diagnostic Signature Based on Three Circulating Exosomal MircoRNAs for Chronic Obstructive Pulmonary Disease. Exp. Ther. Med. 2021, 22, 717. [Google Scholar] [CrossRef]
- Ong, J.; Timens, W.; Rajendran, V.; Algra, A.; Spira, A.; Lenburg, M.E.; Campbell, J.D.; van den Berge, M.; Postma, D.S.; van den Berg, A.; et al. Identification of transforming growth factor-beta-regulated microRNAs and the microRNA-targetomes in primary lung fibroblasts. PLoS ONE 2017, 12, e0183815. [Google Scholar] [CrossRef]
- Zhou, L.; Wu, B.; Yang, J.; Wang, B.; Pan, J.; Xu, D.; Du, C. Knockdown of CircFOXO3 Ameliorates Cigarette Smoke-Induced Lung Injury in Mice. Respir. Res. 2021, 22, 294. [Google Scholar] [CrossRef]
- Singh, K.P.; Maremanda, K.P.; Li, D.; Rahman, I. Exosomal MicroRNAs Are Novel Circulating Biomarkers in Cigarette, Waterpipe Smokers, E-Cigarette Users and Dual Smokers. BMC Med. Genom. 2020, 13, 128. [Google Scholar] [CrossRef]
- Krauskopf, J.; Caiment, F.; van Veldhoven, K.; Chadeau-Hyam, M.; Sinharay, R.; Chung, K.F.; Cullinan, P.; Collins, P.; Barratt, B.; Kelly, F.J.; et al. The Human Circulating MiRNome Reflects Multiple Organ Disease Risks in Association with Short-Term Exposure to Traffic-Related Air Pollution. Environ. Int. 2018, 113, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Opitz, B.; van Laak, V.; Eitel, J.; Suttorp, N. Innate Immune Recognition in Infectious and Noninfectious Diseases of the Lung. Am. J. Respir. Crit. Care Med. 2010, 181, 1294–1309. [Google Scholar] [CrossRef] [PubMed]
- Birch, J.; Anderson, R.K.; Correia-Melo, C.; Jurk, D.; Hewitt, G.; Marques, F.M.; Green, N.J.; Moisey, E.; Birrell, M.A.; Belvisi, M.G.; et al. DNA Damage Response at Telomeres Contributes to Lung Aging and Chronic Obstructive Pulmonary Disease. Am. J. Physiol. Lung Cell. Mol. Physiol. 2015, 309, L1124–L1137. [Google Scholar] [CrossRef]
- Ornatowski, W.; Lu, Q.; Yegambaram, M.; Garcia, A.E.; Zemskov, E.A.; Maltepe, E.; Fineman, J.R.; Wang, T.; Black, S.M. Complex Interplay between Autophagy and Oxidative Stress in the Development of Pulmonary Disease. Redox Biol. 2020, 36, 101679. [Google Scholar] [CrossRef] [PubMed]
- Demedts, I.K.; Demoor, T.; Bracke, K.R.; Joos, G.F.; Brusselle, G.G. Role of Apoptosis in the Pathogenesis of COPD and Pulmonary Emphysema. Respir. Res. 2006, 7, 53. [Google Scholar] [CrossRef]
- Choisy-Rossi, C.; Yonish-Rouach, E. Apoptosis and the Cell Cycle: The P53 Connection. Cell Death Differ. 1998, 5, 129–131. [Google Scholar] [CrossRef]
- Bertoli, C.; Skotheim, J.M.; de Bruin, R.A.M. Control of Cell Cycle Transcription during G1 and S Phases. Nat. Rev. Mol. Cell Biol. 2013, 14, 518–528. [Google Scholar] [CrossRef]
- Puchelle, E.; Zahm, J.-M.; Tournier, J.-M.; Coraux, C. Airway Epithelial Repair, Regeneration, and Remodeling after Injury in Chronic Obstructive Pulmonary Disease. Proc. Am. Thorac. Soc. 2006, 3, 726–733. [Google Scholar] [CrossRef]
- Hisata, S.; Racanelli, A.C.; Kermani, P.; Schreiner, R.; Houghton, S.; Palikuqi, B.; Kunar, B.; Zhou, A.; McConn, K.; Capili, A.; et al. Reversal of Emphysema by Restoration of Pulmonary Endothelial Cells. J. Exp. Med. 2021, 218, e20200938. [Google Scholar] [CrossRef]
- Wiegman, C.H.; Michaeloudes, C.; Haji, G.; Narang, P.; Clarke, C.J.; Russell, K.E.; Bao, W.; Pavlidis, S.; Barnes, P.J.; Kanerva, J.; et al. Oxidative Stress-Induced Mitochondrial Dysfunction Drives Inflammation and Airway Smooth Muscle Remodeling in Patients with Chronic Obstructive Pulmonary Disease. J. Allergy Clin. Immunol. 2015, 136, 769–780. [Google Scholar] [CrossRef]
- Cosio, M.G.; Saetta, M.; Agusti, A. Immunologic Aspects of Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2009, 360, 2445–2454. [Google Scholar] [CrossRef]
- Barnes, P.J. Inflammatory Mechanisms in Patients with Chronic Obstructive Pulmonary Disease. J. Allergy Clin. Immunol. 2016, 138, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Polverino, F.; Seys, L.J.M.; Bracke, K.R.; Owen, C.A. B Cells in Chronic Obstructive Pulmonary Disease: Moving to Center Stage. Am. J. Physiol. Lung Cell. Mol. Physiol. 2016, 311, L687–L695. [Google Scholar] [CrossRef]
- Wang, C.; Zhou, J.; Wang, J.; Li, S.; Fukunaga, A.; Yodoi, J.; Tian, H. Progress in the Mechanism and Targeted Drug Therapy for COPD. Signal Transduct. Target. Ther. 2020, 5, 248. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-T.; Yin, W.; Nakamichi, Y.; Panza, P.; Grohmann, B.; Buettner, C.; Guenther, S.; Ruppert, C.; Kobayashi, Y.; Guenther, A.; et al. WNT/RYK Signaling Restricts Goblet Cell Differentiation during Lung Development and Repair. Proc. Natl. Acad. Sci. USA 2019, 116, 25697–25706. [Google Scholar] [CrossRef]
- Saito, A.; Horie, M.; Nagase, T. TGF-β Signaling in Lung Health and Disease. Int. J. Mol. Sci. 2018, 19, 2460. [Google Scholar] [CrossRef]
- Hagstad, S.; Bjerg, A.; Ekerljung, L.; Backman, H.; Lindberg, A.; Rönmark, E.; Lundbäck, B. Passive Smoking Exposure Is Associated With Increased Risk of COPD in Never Smokers. Chest 2014, 145, 1298–1304. [Google Scholar] [CrossRef]
- Liu, Y.; Pleasants, R.A.; Croft, J.B.; Wheaton, A.G.; Heidari, K.; Malarcher, A.M.; Ohar, J.A.; Kraft, M.; Mannino, D.M.; Strange, C. Smoking Duration, Respiratory Symptoms, and COPD in Adults Aged ≥45 Years with a Smoking History. Int. J. Chronic Obstruct. Pulm. Dis. 2015, 10, 1409–1416. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.J.; Stout-Delgado, H.W. Aging and Lung Disease. Annu. Rev. Physiol. 2020, 82, 433–459. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xuan, S.; Zhang, J.; Guo, Q.; Zhao, L.; Yao, X. A Diagnostic Classifier Based on Circulating miRNA Pairs for COPD Using a Machine Learning Approach. Diagnostics 2023, 13, 1440. https://doi.org/10.3390/diagnostics13081440
Xuan S, Zhang J, Guo Q, Zhao L, Yao X. A Diagnostic Classifier Based on Circulating miRNA Pairs for COPD Using a Machine Learning Approach. Diagnostics. 2023; 13(8):1440. https://doi.org/10.3390/diagnostics13081440
Chicago/Turabian StyleXuan, Shurui, Jiayue Zhang, Qinxing Guo, Liang Zhao, and Xin Yao. 2023. "A Diagnostic Classifier Based on Circulating miRNA Pairs for COPD Using a Machine Learning Approach" Diagnostics 13, no. 8: 1440. https://doi.org/10.3390/diagnostics13081440