
Prognostic Impact of the Get-with-the-Guidelines Heart-Failure Risk Score (GWTG-HF) after Transcatheter Aortic Valve Replacement in Patients with Low-Flow–Low-Gradient Aortic Valve Stenosis
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patient Population
2.2. Definition of Low-Flow–Low-Gradient Aortic Valve Stenosis
2.3. Definition of Endpoints and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Clinical Outcome
3.3. Hemodynamic Performance at Discharge
3.4. GWTG HF Score in LFLG-AS Population
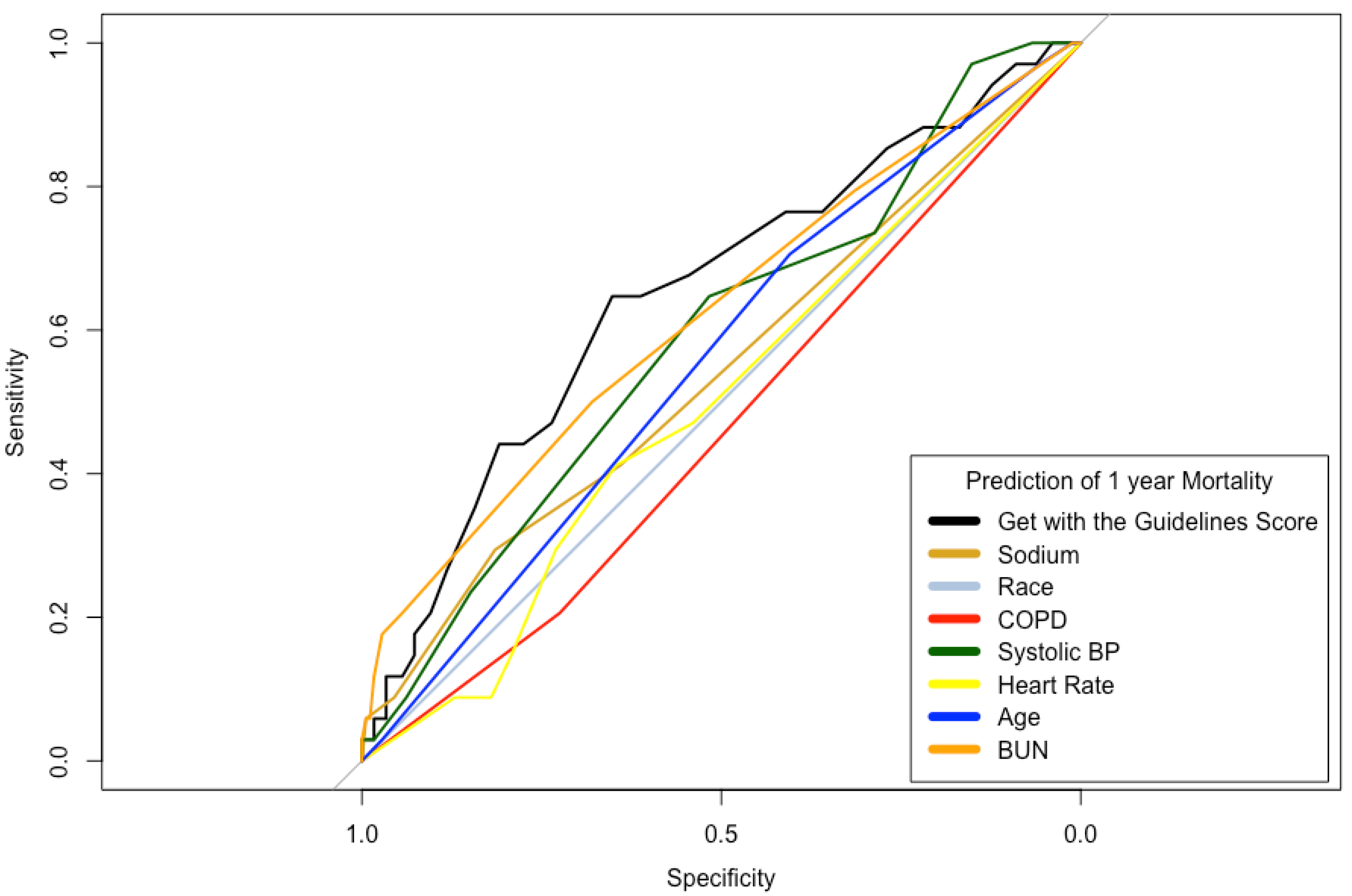
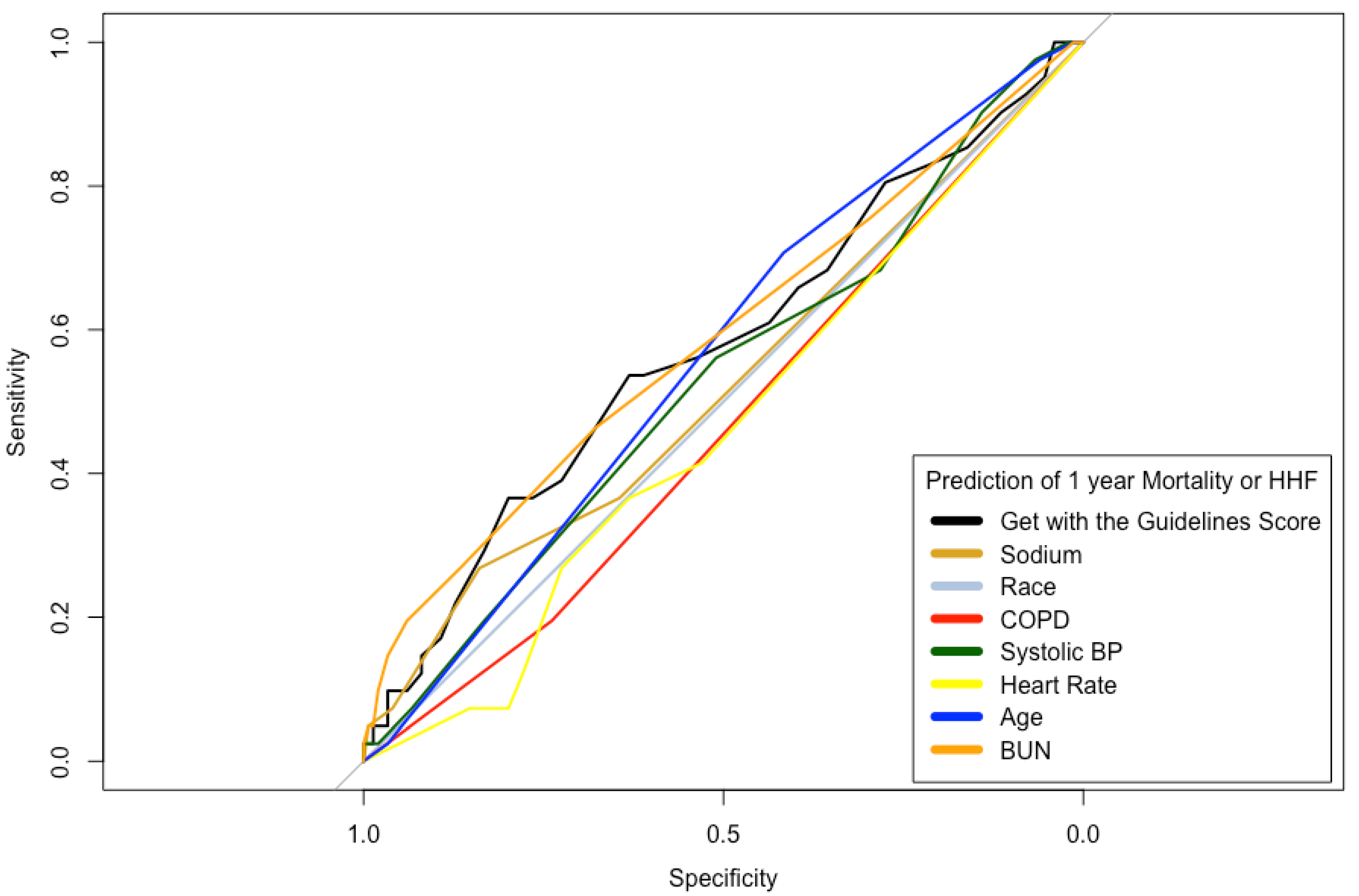
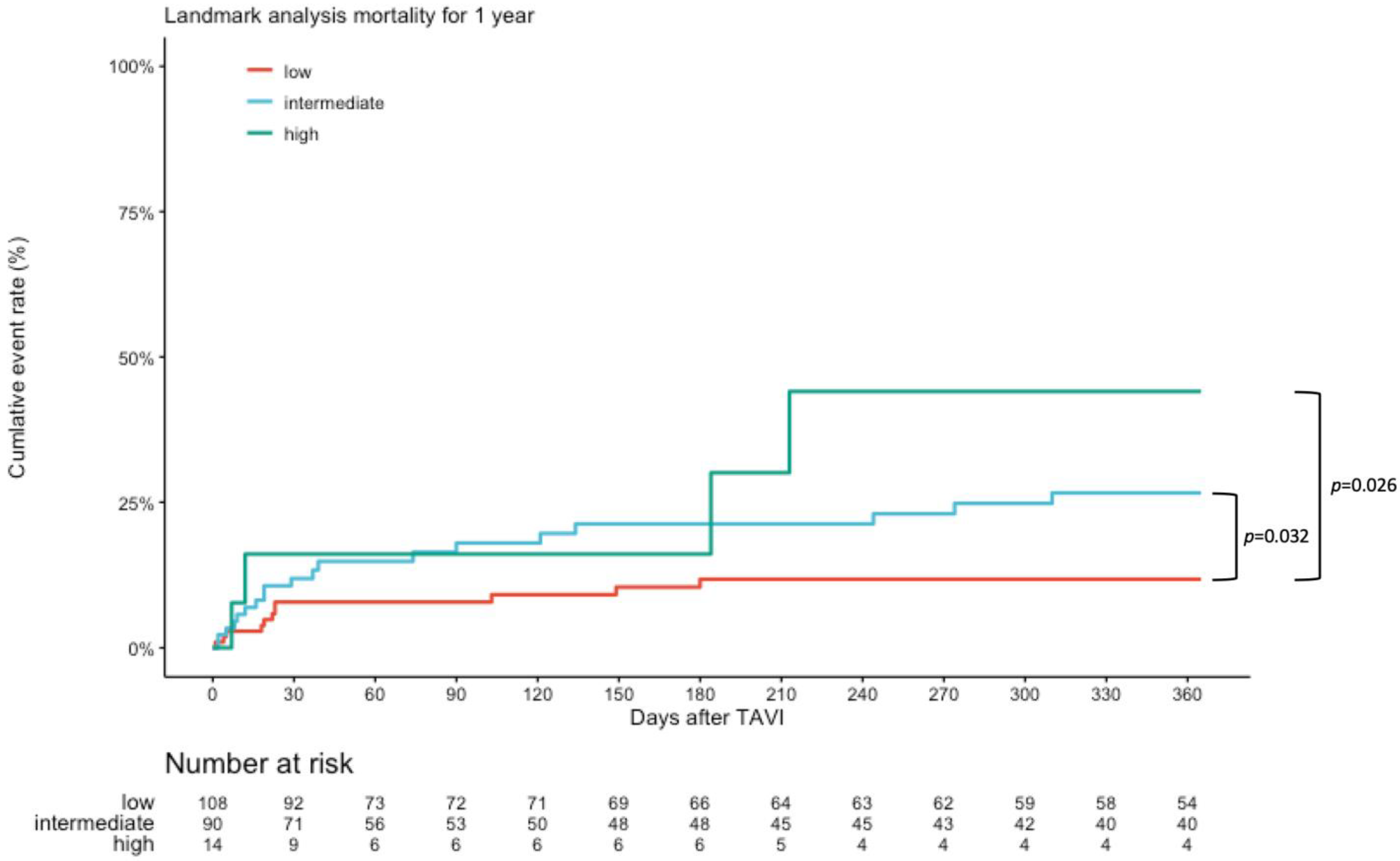
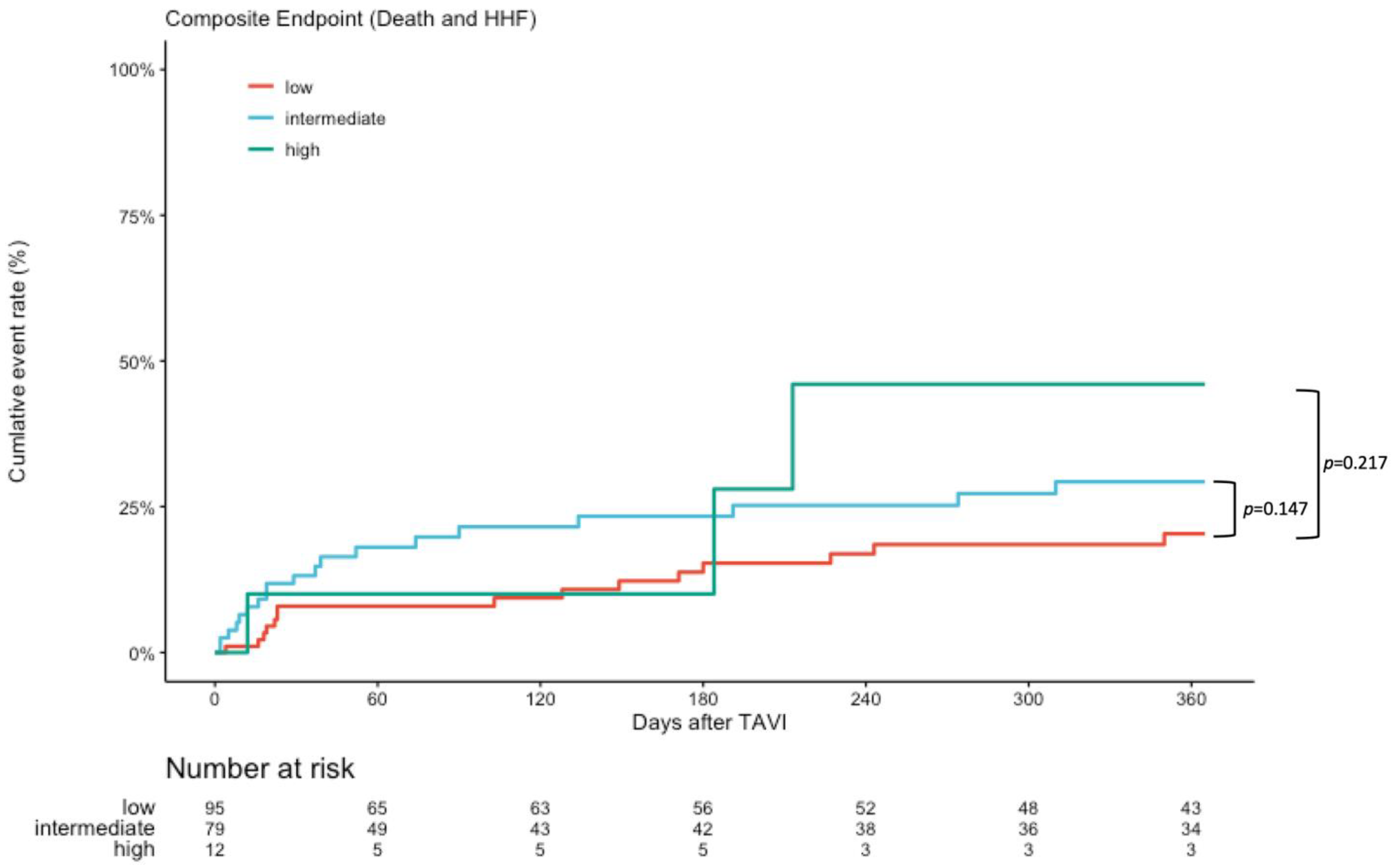
3.5. Outcome at 1 Year Follow-Up
4. Discussion
4.1. Clinical Outcome
4.2. Follow Up at 1 Year
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUC | area under the curve |
| GWTG-HF | get-with-the-guidelines heart-failure |
| HF | heart failure |
| HHF | hospitalization for heart failure |
| LFLG | low-flow–low-gradient |
| PPI | permanent pacemaker implantation |
| PVL | paravalvular regurgitation |
| ROC | receiver operating characteristics |
| TAVI | transcatheter aortic valve implantation |
| THV | transcatheter heart valve |
References
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B. Transcatheter Aortic-Valve Replacement in Low-Risk Patients. N. Engl. J. Med. 2019, 381, 684–685. [Google Scholar] [CrossRef] [PubMed]
- Peterson, P.N.; Rumsfeld, J.S.; Liang, L.; Albert, N.M.; Hernandez, A.F.; Peterson, E.D.; Fonarow, G.C.; Masoudi, F.A.; American Heart Association Get With the Guidelines-Heart Failure Program. A validated risk score for in-hospital mortality in patients with heart failure from the American Heart Association get with the guidelines program. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagu, T.; Pekow, P.S.; Shieh, M.S.; Stefan, M.; Pack, Q.R.; Kashef, M.A.; Atreya, A.R.; Valania, G.; Slawsky, M.T.; Lindenauer, P.K. Validation and Comparison of Seven Mortality Prediction Models for Hospitalized Patients With Acute Decompensated Heart Failure. Circ. Heart Fail. 2016, 9, e002912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef] [PubMed]
- Clavel, M.A.; Magne, J.; Pibarot, P. Low-gradient aortic stenosis. Eur. Heart J. 2016, 37, 2645–2657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kappetein, A.P.; Head, S.J.; Genereux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document (VARC-2). Eur. J. Cardiothorac. Surg. 2012, 42, S45–S60. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Yoshihisa, A.; Sato, Y.; Kanno, Y.; Watanabe, S.; Abe, S.; Sato, T.; Oikawa, M.; Kobayashi, A.; Yamaki, T.; et al. Clinical Significance of Get with the Guidelines-Heart Failure Risk Score in Patients with Chronic Heart Failure after Hospitalization. J. Am. Heart Assoc. 2018, 7, e008316. [Google Scholar] [CrossRef] [PubMed]
- Iliadis, C.; Spieker, M.; Kavsur, R.; Metze, C.; Hellmich, M.; Horn, P.; Westenfeld, R.; Tiyerili, V.; Becher, M.U.; Kelm, M.; et al. “Get with the Guidelines Heart Failure Risk Score” for mortality prediction in patients undergoing MitraClip. Clin. Res. Cardiol. 2021, 110, 1871–1880. [Google Scholar] [CrossRef] [PubMed]
- Kavsur, R.; Hupp-Herschel, H.E.; Sugiura, A.; Tanaka, T.; Ozturk, C.; Weber, M.; Nickenig, G.; Tiyerili, V.; Becher, M.U. Prognostic significance of the get with the guidelines-heart failure (GWTG-HF) risk score in patients undergoing trans-catheter tricuspid valve repair (TTVR). Heart Vessels 2021, 36, 1903–1910. [Google Scholar] [CrossRef] [PubMed]
- Lauten, A.; Zahn, R.; Horack, M.; Sievert, H.; Linke, A.; Ferrari, M.; Harnath, A.; Grube, E.; Gerckens, U.; Kuck, K.H.; et al. Transcatheter aortic valve implantation in patients with low-flow, low-gradient aortic stenosis. JACC Cardiovasc. Interv. 2012, 5, 552–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotzmann, M.; Lindstaedt, M.; Bojara, W.; Ewers, A.; Mugge, A. Clinical outcome of transcatheter aortic valve implantation in patients with low-flow, low gradient aortic stenosis. Catheter. Cardiovasc. Interv. 2012, 79, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Fischer-Rasokat, U.; Renker, M.; Liebetrau, C.; van Linden, A.; Arsalan, M.; Weferling, M.; Rolf, A.; Doss, M.; Mollmann, H.; Walther, T.; et al. 1-Year Survival After TAVR of Patients With Low-Flow, Low-Gradient and High-Gradient Aortic Valve Stenosis in Matched Study Populations. JACC Cardiovasc. Interv. 2019, 12, 752–763. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, H.B.; Lerakis, S.; Gilard, M.; Cavalcante, J.L.; Makkar, R.; Herrmann, H.C.; Windecker, S.; Enriquez-Sarano, M.; Cheema, A.N.; Nombela-Franco, L.; et al. Transcatheter Aortic Valve Replacement in Patients With Low-Flow, Low-Gradient Aortic Stenosis: The TOPAS-TAVI Registry. J. Am. Coll. Cardiol. 2018, 71, 1297–1308. [Google Scholar] [CrossRef] [PubMed]
- Wilde, N.; Sugiura, A.; Sedaghat, A.; Becher, M.U.; Kelm, M.; Baldus, S.; Nickenig, G.; Veulemans, V.; Tiyerili, V. Risk of mortality following transcatheter aortic valve replacement for low-flow low-gradient aortic stenosis. Clin. Res. Cardiol. 2021, 110, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, T.H.; De Backer, O.; Gerds, T.A.; Bieliauskas, G.; Svendsen, J.H.; Sondergaard, L. Mortality and Heart Failure Hospitalization in Patients with Conduction Abnormalities after Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2019, 12, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Mangner, N.; Stachel, G.; Woitek, F.; Haussig, S.; Schlotter, F.; Hollriegel, R.; Adam, J.; Lindner, A.; Mohr, F.W.; Schuler, G.; et al. Predictors of Mortality and Symptomatic Outcome of Patients With Low-Flow Severe Aortic Stenosis Undergoing Transcatheter Aortic Valve Replacement. J. Am. Heart Assoc. 2018, 7, e007977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrmann, H.C.; Pibarot, P.; Hueter, I.; Gertz, Z.M.; Stewart, W.J.; Kapadia, S.; Tuzcu, E.M.; Babaliaros, V.; Thourani, V.; Szeto, W.Y.; et al. Predictors of mortality and outcomes of therapy in low-flow severe aortic stenosis: A Placement of Aortic Transcatheter Valves (PARTNER) trial analysis. Circulation 2013, 127, 2316–2326. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low Risk | Intermediate | High Risk | p-Value | |
|---|---|---|---|---|
| n = 108 | n = 90 | n = 14 | ||
| Baseline Characteristics | ||||
| Age, years | 79.0 [75.0; 82.0] | 82.0 [79.2; 84.0] | 86.0 [82.2; 88.8] | <0.001 |
| Gender, female | 39 (36.1%) | 31 (34.4%) | 3 (21.4%) | 0.612 |
| BMI, kg/m2 | 27.6 [24.3; 30.8] | 26.2 [24.0; 29.4] | 24.4 [22.9; 27.8] | 0.036 |
| Log. Euroscore, % | 17.3 [11.6; 25.1] | 21.9 [14.8; 31.8] | 36.0 [20.9; 48.4] | <0.001 |
| Euroscore II, % | 5.5 [3.9; 8.8] | 7.2 [4.9; 11.3] | 9.1 [6.1; 15.9] | 0.004 |
| NYHA class III/IV | 103 (95.4%) | 86 (95.6%) | 12 (85.7%) | 0.284 |
| Previous COPD | 23 (21.3%) | 27 (30.0%) | 6 (42.9%) | 0.130 |
| Previous aHT | 104 (96.3%) | 83 (92.2%) | 12 (85.7%) | 0.125 |
| Syst. RR, mmHg | 138 [130; 146] | 120 [108; 127] | 101 [93; 120] | <0.001 |
| Diabetes | 45 (41.7%) | 42 (46.7%) | 5 (35.7%) | 0.651 |
| Previous Dialysis | 3 (2.8%) | 5 (5.6%) | 2 (14.3%) | 0.127 |
| Previous PAD | 30 (27.8%) | 18 (20.0%) | 6 (42.9%) | 0.140 |
| Previous Stroke | 24 (22.2%) | 12 (13.3%) | 1 (7.1%) | 0.186 |
| Previous CAD | 80 (74.1%) | 67 (74.4%) | 10 (71.4%) | 0.939 |
| Previous MI | 15 (13.9%) | 12 (13.3%) | 3 (21.4%) | 0.666 |
| Previous PCI | 55 (50.9%) | 38 (42.2%) | 7 (50.0%) | 0.463 |
| Previous CABG | 16 (14.8%) | 14 (15.6%) | 0 (0.0%) | 0.359 |
| Echocardiographic Characteristics | ||||
| LVEF, % | 36.0 [28.8; 40.0] | 33.0 [25.2; 39.0] | 33.5 [28.2; 40.0] | 0.085 |
| AVA, cm2 | 0.8 [0.6; 0.9] | 0.7 [0.6; 0.9] | 0.7 [0.6; 0.8] | 0.050 |
| SV, mL | 55.0 [44.0; 64.2] | 48.0 [39.2; 55.8] | 47.5 [38.8; 51.0] | 0.001 |
| SVi, mL/m2 | 28.2 [23.9; 32.1] | 25.8 [20.0; 29.0] | 25.0 [21.8; 28.2] | 0.004 |
| Pmean, mmHg | 26.5 [21.0; 32.0] | 25.0 [18.0; 31.0] | 24.5 [22.2; 31.2] | 0.265 |
| Pmax, mmHg | 45.0 [36.5; 50.0] | 42.0 [31.0; 50.0] | 43.0 [38.5; 50.0] | 0.471 |
| MR ( ≥ III) | 3 (2.8%) | 2 (2.2%) | 0 (0.0%) | 1.000 |
| TR ( ≥ III) | 0 (0.0%) | 1 (1.1%) | 1 (7.1%) | 0.060 |
| pAH 1 | 5 (4.6%) | 7 (8.0%) | 1 (7.1%) | 0.515 |
| Electrocardiographic Characteristics | ||||
| Atrial fibrillation | 55 (50.9%) | 53 (58.9%) | 9 (64.3%) | 0.415 |
| Heart rate, bpm | 72.0 [64.8; 81.2] | 82.0 [70.5; 99.5] | 99.5 [88.5; 112.0] | <0.001 |
| LBBB | 17 (15.7%) | 16 (18.0%) | 2 (14.3%) | 0.914 |
| RBBB | 12 (11.1%) | 8 (9.0%) | 4 (28.6%) | 0.122 |
| New pacemaker | 35 (32.4%) | 24 (26.7%) | 1 (7.1%) | 0.131 |
| Multisliced Computed Tomography Data (MSCT) | ||||
| Area cm2 | 5.0 [4.4; 5.7] | 5.3 [4.6; 6.0] | 4.8 [4.6; 5.6] | 0.262 |
| Diameter min., mm | 22.4 [20.5; 24.0] | 23.0 [21.3; 24.5] | 21.7 [21.0; 23.8] | 0.132 |
| Diameter max., mm | 28.7 [27.2; 30.9] | 29.3 [27.6; 31.2] | 29.1 [27.2; 30.9] | 0.362 |
| Eccentricity | 0.2 [0.2; 0.3] | 0.2 [0.2; 0.3] | 0.2 [0.2; 0.3] | 0.800 |
| Calcification, AU | 1927 [1163; 2807] | 2089 [1474; 2908] | 2316 [1553; 3155] | 0.376 |
| Laboratory Characteristics | ||||
| eGFR, mL/min | 58.5 [43.0; 77.0] | 46.5 [35.0; 59.0] | 33.5 [22.0; 47.0] | <0.001 |
| Sodium, mmol/L | 139 [137; 141] | 140 [137; 141] | 139 [135; 141] | 0.405 |
| BUN, mg/dL | 21.1 [16.8; 26.1] | 29.6 [23.1; 37.5] | 44.9 [32.9; 68.1] | <0.001 |
| CRP, mg/dL | 5.8 [1.8; 12.7] | 9.4 [4.0; 17.3] | 9.5 [6.0; 30.2] | 0.027 |
| Haemoglobin, g/dL | 12.7 [11.7; 13.8] | 12.2 [11.3; 13.3] | 11.4 [10.1; 13.0] | 0.043 |
| Low Risk | Intermediate Risk | High Risk | p-Value | |
|---|---|---|---|---|
| n = 108 | n = 90 | n = 14 | ||
| Device Failure 1 | 6 (5.6%) | 6 (6.8%) | 1 (7.7%) | 0.731 |
| Procedural-related death * | 1 (0.5%) | 0 (0.0%) | 0 (0.0%) | 1.000 |
| Intended performance | 106 (99.1%) | 86 (95.6%) | 14 (100.0%) | 0.325 |
| Significant PVL 2 | 2 (1.9%) | 4 (4.5%) | 1 (7.1%) | 0.281 |
| Elevated gradient 3 | 2 (1.9%) | 1 (1.1%) | 0 (0.0%) | 1.000 |
| Multiple valves | 1 (0.9%) | 2 (2.2%) | 0 (0.0%) | 0.669 |
| Conversion to sternotomy * | 1 (0.9%) | 2 (2.2%) | 0 (0.0%) | 0.668 |
| Low Risk | Intermediate | High Risk | p-Value | |
|---|---|---|---|---|
| n = 108 | n = 90 | n = 14 | ||
| Procedural Data | ||||
| Transfemoral Access | 100 (92.6%) | 89 (98.9%) | 13 (92.9%) | 0.064 |
| Pre dilatation | 55 (50.9%) | 50 (56.2%) | 7 (50.0%) | 0.742 |
| Post dilatation | 20 (18.7%) | 9 (10.2%) | 3 (21.4%) | 0.162 |
| Procedural time, min | 57 [45; 75] | 56 [45; 65] | 59 [50; 65] | 0.571 |
| Contrast, mL | 110 [90; 140] | 106 [90; 130] | 110 [100; 130] | 0.434 |
| Conscious sedation | 97 (89.8%) | 80 (88.9%) | 11 (78.6%) | 0.425 |
| Postprocedural echocardiographic outcome | ||||
| AVA, cm2 | 1.9 [1.6; 2.1] | 1.7 [1.5; 2.2] | 1.9 [1.8; 2.2] | 0.518 |
| LVEF | 40 [31; 45] | 36 [30; 45] | 38 [28; 49] | 0.620 |
| Pmean, mmHg | 7.0 [5.0; 9.0] | 7.0 [5.0; 9.0] | 5.0 [4.0; 6.0] | 0.011 |
| Pmax, mmHg | 13.0 [10.0; 17.8] | 13.0 [9.0; 18.0] | 10.0 [9.0; 10.0] | 0.013 |
| Significant PVL 1 | 2 (1.9%) | 4 (4.5%) | 1 (7.1%) | 0.281 |
| Adverse events | ||||
| Major Stroke | 2 (1.9%) | 4 (4.4%) | 0 (0.0%) | 0.613 |
| Major vascular complications | 6 (5.6%) | 3 (3.3%) | 0 (0.0%) | 0.741 |
| Life threatening bleeding | 4 (3.7%) | 1 (1.1%) | 0 (0.0%) | 0.560 |
| Renal failure (≥2) | 5 (5.1%) | 5 (6.0%) | 2 (14.3%) | 0.343 |
| Coronary artery obstruction | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1.000 |
| New permanent pacemaker 2 | 12 (16.44%) | 9 (13.64%) | 3 (23.08%) | 0.631 |
| In hospital | ||||
| Days in hospital | 7.0 [5.0; 9.0] | 7.0 [5.0; 10.0] | 7.0 [6.0; 8.8] | 0.288 |
| Days on intensive care unit | 2.0 [1.0; 3.0] | 2.0 [1.0; 3.0] | 3.0 [2.0; 3.0] | 0.094 |
| In-hospital mortality | 7 (6.5%) | 7 (7.8%) | 2 (14.3%) | 0.390 |
| Predictor | HR (CI 95%) | p-Value |
|---|---|---|
| GWTG-HF Score | 1.07 (1.01–1.14) | 0.030 |
| Significant PVL (≥Grade II) | 2.44 (0.37–16.25) | 0.357 |
| Mitral Regurgitation (≥Grade III) | 1.93 (0.24–15.32) | 0.532 |
| Left ventricular ejection fraction (per 1% increase) | 1.02 (0.97–1.08) | 0.352 |
| Stroke volume index (per 1 mL/m2 increase) | 0.90 (0.83–0.97) | 0.006 |
| Post mean transaortic gradient (per 1 mmHg increase) | 0.96 (0.86–1.07) | 0.496 |
| New pacemaker implantation | 3.97 (1.34–11.75) | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eckel, C.; Blumenstein, J.; Husser, O.; Sötemann, D.; Grothusen, C.; Schlüter, J.; Becher, M.; Nef, H.; Elsässer, A.; Nickenig, G.; et al. Prognostic Impact of the Get-with-the-Guidelines Heart-Failure Risk Score (GWTG-HF) after Transcatheter Aortic Valve Replacement in Patients with Low-Flow–Low-Gradient Aortic Valve Stenosis. Diagnostics 2023, 13, 1357. https://doi.org/10.3390/diagnostics13071357
Eckel C, Blumenstein J, Husser O, Sötemann D, Grothusen C, Schlüter J, Becher M, Nef H, Elsässer A, Nickenig G, et al. Prognostic Impact of the Get-with-the-Guidelines Heart-Failure Risk Score (GWTG-HF) after Transcatheter Aortic Valve Replacement in Patients with Low-Flow–Low-Gradient Aortic Valve Stenosis. Diagnostics. 2023; 13(7):1357. https://doi.org/10.3390/diagnostics13071357
Chicago/Turabian StyleEckel, Clemens, Johannes Blumenstein, Oliver Husser, Dagmar Sötemann, Christina Grothusen, Judith Schlüter, Marc Becher, Holger Nef, Albrecht Elsässer, Georg Nickenig, and et al. 2023. "Prognostic Impact of the Get-with-the-Guidelines Heart-Failure Risk Score (GWTG-HF) after Transcatheter Aortic Valve Replacement in Patients with Low-Flow–Low-Gradient Aortic Valve Stenosis" Diagnostics 13, no. 7: 1357. https://doi.org/10.3390/diagnostics13071357