
Helicobacter pylori Infection in Children: A Possible Reason for Headache?
 , , , , , ,
, , , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anttila, P.; Metsähonkala, L.; Sillanpää, M. Long-term Trends in the Incidence of Headache in Finnish Schoolchildren. Pediatrics 2006, 117, e1197–e1201. [Google Scholar] [CrossRef]
- Blankenburg, M.; Schroth, M.; Braun, S. Chronic headache in children and adolescents. Klin. Padiatr. 2019, 231, 14–20. [Google Scholar]
- Teleanu, R.I.; Vladacenco, O.; Teleanu, D.M.; Epure, D.A. Treatment of Pediatric Migraine: A Review. Maedica 2016, 11, 136–143. [Google Scholar]
- Bigal, M.E.; Lipton, R.B. The epidemiology, burden, and comorbidities of migraine. Neurol. Clin. 2009, 27, 321–334. [Google Scholar] [CrossRef]
- Wöber-Bingöl, Ç. Epidemiology of Migraine and Headache in Children and Adolescents. Curr. Pain Headache Rep. 2013, 17, 341. [Google Scholar] [CrossRef]
- Nieswand, V.; Richter, M.; Gossrau, G. Epidemiology of Headache in Children and Adolescents—Another Type of Pandemia. Curr. Pain Headache Rep. 2020, 24, 62. [Google Scholar] [CrossRef]
- Gazerani, P. Migraine and Mood in Children. Behav. Sci. 2021, 11, 52. [Google Scholar] [CrossRef]
- Deleu, D.; Hanssens, Y.; Worthing, E.A. Symptomatic and prophylactic treatment of migraine: A critical reappraisal. Clin. Neuropharmacol. 1998, 21, 267–279. [Google Scholar]
- Le Gal, J.; Michel, J.F.; Rinaldi, V.E.; Spiri, D.; Moretti, R.; Bettati, D.; Romanello, S.; Berlese, P.; Lualdi, R.; Boizeau, P.; et al. Association between functional gastrointestinal disorders and migraine in children and adolescents: A case-control study. Lancet Gastroenterol. Hepatol. 2016, 1, 114–121. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Lv, Z.-F.; Zhong, Y.; Liu, D.-S.; Chen, S.-P.; Xie, Y. The internalization of Helicobacter pylori plays a role in the failure of H. pylori eradication. Helicobacter 2016, 22, e12324. [Google Scholar] [CrossRef]
- Pinessi, L.; Savi, L.; Pellicano, R.; Rainero, I.; Valfre, W.; Gentile, S.; Cossotto, D.; Rizzetto, M.; Ponzetto, A. Chronic Helicobacter Pylori Infection and Migraine: A Case-Control Study. Headache 2000, 40, 836–839. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, C.; Machado, J.C.; Yamaoka, Y. Pathogenesis of Helicobacter pylori Infection. Helicobacter 2005, 10, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Pellicano, R.; Ianiro, G.; Fagoonee, S.; Settanni, C.R.; Gasbarrini, A. Review: Extragastric diseases and Helicobacter pylori. Helicobacter 2020, 25, e12741. [Google Scholar] [CrossRef]
- Kountouras, J.; Zavos, C.; Polyzos, S.A.; Deretzi, G. The gut-brain axis: Interactions between Helicobacter pylori and enteric and central nervous systems. Ann. Gastroenterol. 2015, 28, 506. [Google Scholar]
- Budzyński, J. Brain-gut axis in the pathogenesis of Helicobacter pylori infection. World J. Gastroenterol. 2014, 20, 5212–5225. [Google Scholar] [CrossRef]
- Baj, J.; Forma, A.; Flieger, W.; Morawska, I.; Michalski, A.; Buszewicz, G.; Sitarz, E.; Portincasa, P.; Garruti, G.; Flieger, M.; et al. Helicobacter pylori Infection and Extragastric Diseases—A Focus on the Central Nervous System. Cells 2021, 10, 2191. [Google Scholar] [CrossRef]
- Savi, L.; Ribaldone, D.; Fagoonee, S.; Pellicano, R. Is Helicobacter pylori the infectious trigger for headache?: A review. Infect. Disord.—Drug Targets 2014, 13, 313–317. [Google Scholar] [CrossRef] [Green Version]
- Tsai, H.-F.; Hsu, P.-N. Interplay between Helicobacter pylori and immune cells in immune pathogenesis of gastric inflammation and mucosal pathology. Cell. Mol. Immunol. 2010, 7, 255–259. [Google Scholar] [CrossRef] [Green Version]
- Arzani, M.; Jahromi, S.R.; Ghorbani, Z.; Vahabizad, F.; Martelletti, P.; Ghaemi, A.; Sacco, S.; Togha, M.; On behalf of the School of Advanced Studies of the European Headache Federation (EHF-SAS). Gut-brain Axis and migraine headache: A comprehensive review. J. Headache Pain 2020, 21, 15. [Google Scholar] [CrossRef] [Green Version]
- Mayer, E.A.; Tillisch, K.; Bradesi, S. Review article: Modulation of the brain–gut axis as a therapeutic approach in gastrointestinal disease. Aliment. Pharmacol. Ther. 2006, 24, 919–933. [Google Scholar] [CrossRef]
- Sticlaru, L.; Stăniceanu, F.; Cioplea, M.; Nichita, L.; Bastian, A.; Micu, G.; Popp, C. Dangerous Liaison: Helicobacter pylori, Ganglionitis, and Myenteric Gastric Neurons: A Histopathological Study. Anal. Cell. Pathol. 2019, 2019, 3085181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasbarrini, A.; Gabrielli, M.; Fiore, G.; Candelli, M.; Bartolozzi, F.; De Luca, A.; Cremonini, F.; Franceschi, F.; Di Campli, C.; Armuzzi, A.; et al. Association Between Helicobacter Pylori Cytotoxic Type I Caga-Positive Strains and Migraine with Aura. Cephalalgia 2000, 20, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Ranjbar, R.; Behzadi, P.; Farshad, S. Advances in diagnosis and treatment of Helicobacter pylori infection. Acta Microbiol. et Immunol. Hung. 2017, 64, 273–292. [Google Scholar] [CrossRef] [Green Version]
- Corojan, A.L.; Dumitrașcu, D.; Ciobanca, P.; Leucuta, D. Prevalence of Helicobacter pylori infection among dyspeptic patients in Northwestern Romania: A decreasing epidemiological trend in the last 30 years. Exp. Ther. Med. 2020, 20, 3488–3492. [Google Scholar] [CrossRef]
- Yuan, C.; Adeloye, D.; Luk, T.T.; Huang, L.; He, Y.; Xu, Y.; Ye, X.; Yi, Q.; Song, P.; Rudan, I.; et al. The global prevalence of and factors associated with Helicobacter pylori infection in children: A systematic review and meta-analysis. Lancet Child Adolesc. Health 2022, 6, 185–194. [Google Scholar] [CrossRef]
- Jones, N.L.; Koletzko, S.; Goodman, K.; Bontems, P.; Cadranel, S.; Casswall, T.; Czinn, S.; Gold, B.D.; Guarner, J.; Elitsur, Y.; et al. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016). J. Pediatr. Gastroenterol. Nutr. 2017, 64, 991–1003. [Google Scholar] [CrossRef] [PubMed]
- Lupu, A.; Miron, I.C.; Cianga, A.L.; Cernomaz, A.T.; Lupu, V.V.; Munteanu, D.; Ghica, D.C.; Fotea, S. The Relationship between Anemia and Helicobacter Pylori Infection in Children. Children 2022, 9, 1324. [Google Scholar] [CrossRef]
- Lupu, A.; Miron, I.C.; Cianga, A.L.; Cernomaz, A.T.; Lupu, V.V.; Gavrilovici, C.; Stârcea, I.M.; Tarca, E.; Ghica, D.C.; Fotea, S. The Prevalence of Liver Cytolysis in Children with Helicobacter pylori Infection. Children 2022, 9, 1498. [Google Scholar] [CrossRef] [PubMed]
- Lupu, A.; Miron, I.C.; Cernomaz, A.T.; Gavrilovici, C.; Lupu, V.V.; Starcea, I.M.; Cianga, A.L.; Stana, B.; Tarca, E.; Fotea, S. Epidemiological Characteristics of Helicobacter pylori Infection in Children in Northeast Romania. Diagnostics 2023, 13, 408. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J. The international classification of headache disorders, 2nd edn (ICDH-II). J. Neurol. Neurosurg. Psychiatry 2004, 75, 808–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, W.F.; Lipton, R.B.; Celentano, D.D.; Reed, M.L. Prevalence of migraine headache in the United States. Relation to age, income, race, and other sociodemographic factors. JAMA 1992, 267, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Holtmann, G.; Goebell, H.; Holtmann, M.; Talley, N.J. Dyspepsia in healthy blood donors: Pattern of symptoms and association with Helicobacter pylori. Dig. Dis. Sci. 1994, 39, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Imanieh, M.H.; Dehghani, S.M.; Haghighat, M.; Irani, M.; Yousefi, M. Migraine headache and acid peptic diseases in children. Iran. Red Crescent Med. J. 2009, 11, 181–183. [Google Scholar]
- Pacifico, L.; Anania, C.; Osborn, J.F.; Ferraro, F.; Chiesa, C. Consequences of Helicobacter pylori infection in children. World J. Gastroenterol. 2010, 16, 5181–5194. [Google Scholar] [CrossRef]
- Panconesi, A.; Sicuteri, R. Headache induced by serotonergic agonists—A key to the interpretation of migraine pathogenesis? Cephalalgia 1997, 17, 3–14. [Google Scholar] [CrossRef]
- Tunca, A.; Turkay, C.; Tekin, O.; Kargili, A.; Erbayrak, M. Is Helicobacter pylori infection a risk factor for migraine? A case-control study. Acta Neurol. Belg. 2004, 104, 161–164. [Google Scholar]
- Bradbeer, L.; Thakkar, S.; Liu, A.; Nanan, R. Childhood headache and H. pylori: A possible association. Aust. Fam. Physician 2013, 42, 134–136. [Google Scholar] [PubMed]
- Kikui, S.; Chen, Y.; Ikeda, K.; Hasebe, M.; Asao, K.; Takeshima, T. Comorbidities in patients with migraine in Japan: A cross-sectional study using data from National Health and Wellness Survey. BMJ Open 2022, 12, e065787. [Google Scholar] [CrossRef]
- Cavestro, C.; Prandi, G.; Manildo, M.; Martini, S.; Genovesi, C.; Premoli, A.; Fraire, F.; Neri, L.; Mandrino, S.; Ferrero, M.; et al. A cross-sectional study on the association between Helicobacter pylori infection and headache. Neurol. Sci. 2022, 43, 6031–6038. [Google Scholar] [CrossRef]
- Yiannopoulou, K.G.; Efthymiou, A.; Karydakis, K.; Arhimandritis, A.; Bovaretos, N.; Tzivras, M. Helicobacter pylori infection as an environmental risk factor for migraine without aura. J. Headache Pain 2007, 8, 329–333. [Google Scholar] [CrossRef] [Green Version]
- Hosseinzadeh, M.; Khosravi, A.; Saki, K.; Ranjbar, R. Evaluation of Helicobacter pylori infection in patients with common migraine headache. Arch. Med. Sci. 2011, 5, 844–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faraji, F.; Zarinfar, N.; Zanjani, A.T.; Morteza, A. The effect of Helicobacter pylori eradication on migraine: A randomized, double blind, controlled trial. Pain Physician 2012, 15, 495–498. [Google Scholar] [PubMed]
- Karkelis, S.; Papadaki-Papandreou, O.; Lykogeorgou, M.; Papandreou, T.; Lianou, L.; Panayotou, I.; Roma, E.; Chrousos, G. 667 Helicobacter Pylori Infection and Headache in Children and Adolescents. Pediatr. Res. 2010, 68, 340. [Google Scholar] [CrossRef] [Green Version]
- Gasbarrini, A.; De Luca, A.; Fiore, G.; Gambrielli, M.; Franceschi, F.; Ojetti, V.; Torre, E.S.; Gasbarrini, G.; Pola, P.; Giacovazzo, M. Beneficial effects of Helicobacter pylori eradication on migraine. Hepato-Gastroenterology 1998, 45, 765–770. [Google Scholar] [PubMed]
- Gasbarrini, A.; De Luca, A.; Fiore, G.; Franceschi, F.; Ojetti, V.; Torre, E.S.; Di Campli, C.; Candelli, M.; Pola, M.S.R.; Tondi, P.; et al. Primary Headache and Helicobacter Pylori. Int. J. Angiol. 1998, 7, 310–312. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.; Mehany, D.; Eldin, H.G.; Abdelghaffar, M.; Abdelbaky, H.A.; Kamal, Y.S.; Hussein, M. Helicobacter pylori infection in migraine headache: A true association or an innocent bystander? Int. J. Neurosci. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Su, J.; Zhou, X.Y.; Zhang, G.X. Association between helicobacter pylori infection and migraine: A meta-analysis. World J. Gastroenterol. 2014, 20, 14965–14972. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Lee, J.J.; Kwon, Y.; Kim, J.H.; Sohn, J.H. Clinical Implications of Associations between Headache and Gastrointestinal Disorders: A Study Using the Hallym Smart Clinical Data Warehouse. Front. Neurol. 2017, 8, 526. [Google Scholar] [CrossRef] [Green Version]
- Ansari, B.; Basiri, K.; Meamar, R.; Chitsaz, A.; Nematollahi, S. Association of Helicobacter pylori antibodies and severity of migraine attack. Iran. J. Neurol. 2015, 14, 125–129. [Google Scholar]
- Kang, J.W.; Shin, Y.I. The role of interleukin 10 in the associations between migraine and Helicobacter pylori infection. Pain Physician 2013, 16, E450. [Google Scholar] [CrossRef]
- Munno, I.; Marinaro, M.; Bassi, A.; Cassiano, M.; Causarano, V.; Centonze, V. Immunological aspects in migraine: Increase of IL-10 plasma levels during attack. Headache 2001, 41, 764–767. [Google Scholar] [CrossRef]
- Mavromichalis, I.; Zaramboukas, T.; Giala, M.M. Migraine of gastrointestinal origin. Eur. J. Pediatr. 1995, 154, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Ciancarelli, I.; Di Massimo, C.; Ciancarelli, M.G.T.; De Matteis, G.; Marini, C.; Carolei, A. Helicobacter Pylori Infection and Migraine. Cephalalgia 2002, 22, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Öcal, S.; Öcal, R.; Suna, N. Relationship between Helicobacter pylori infection and white matter lesions in patients with migraine. BMC Neurol. 2022, 22, 187. [Google Scholar] [CrossRef]
- Welander, N.Z.; Olivo, G.; Pisanu, C.; Rukh, G.; Schiöth, H.B.; Mwinyi, J. Migraine and gastrointestinal disorders in middle and old age: A UK Biobank study. Brain Behav. 2021, 11, e2291. [Google Scholar] [CrossRef]
- Cámara-Lemarroy, C.R.; Rodriguez-Gutierrez, R.; Monreal-Robles, R.; Marfil-Rivera, A. Gastrointestinal disorders associated with migraine: A comprehensive review. World J. Gastroenterol. 2016, 22, 8149–8160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hormati, A.; Akbari, N.; Sharifipour, E.; Hejazi, S.A.; Jafari, F.; Alemi, F.; Mohammadbeigi, A. Migraine and gastric disorders: Are they associated? J. Res. Med. Sci. 2019, 24, 60. [Google Scholar] [CrossRef] [PubMed]
- Akbari, N.; Hormati, A.; Sharifipour, E.; Hejazi, S.A.; Jafari, F.; Mousavi-Aghdas, S.A.; Golzari, S.E. Migraine, dyspepsia, and Helicobacter pylori: Zeroing in on the culprit. Iran. J. Neurol. 2019, 18, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Martin, B.C.; Dorfman, J.H.; McMillan, J.A.; McMillan, C.A. Prevalence of migraine headache and association with sex, age, race, and rural/urban residence: A population-based study of Georgia Medicaid recipients. Clin. Ther. 1994, 16, 855–872. [Google Scholar]
- Lileikytė, V.; Brasas, K.; Vaitkus, A.; Žvirblienė, A. Is vestibular migraine really a separate form of migraine? Med. Hypotheses 2022, 165, 110880. [Google Scholar] [CrossRef]
- Martami, F.; Ghorbani, Z.; Abolhasani, M.; Togha, M.; Meysamie, A.; Sharifi, A.; Jahromi, S.R. Comorbidity of gastrointestinal disorders, migraine, and tension-type headache: A cross-sectional study in Iran. Neurol. Sci. 2017, 39, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Urits, I.; Yilmaz, M.; Bahrun, E.; Merley, C.; Scoon, L.; Lassiter, G.; An, D.; Orhurhu, V.; Kaye, A.D.; Viswanath, O. Utilization of B12 for the treatment of chronic migraine. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 479–491. [Google Scholar] [CrossRef] [PubMed]
- Fila, M.; Chojnacki, J.; Pawlowska, E.; Szczepanska, J.; Chojnacki, C.; Blasiak, J. Kynurenine Pathway of Tryptophan Metabolism in Migraine and Functional Gastrointestinal Disorders. Int. J. Mol. Sci. 2021, 22, 10134. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Infection with H. pylori | % | |
|---|---|---|
| absent | 1215 | 69.2 |
| present | 542 | 30.8 |
| Headache | ||
| absent | 1627 | 92.6 |
| present | 130 | 7.4 |
| Sex | ||
| female | 1210 | 68.9 |
| male | 547 | 31.1 |
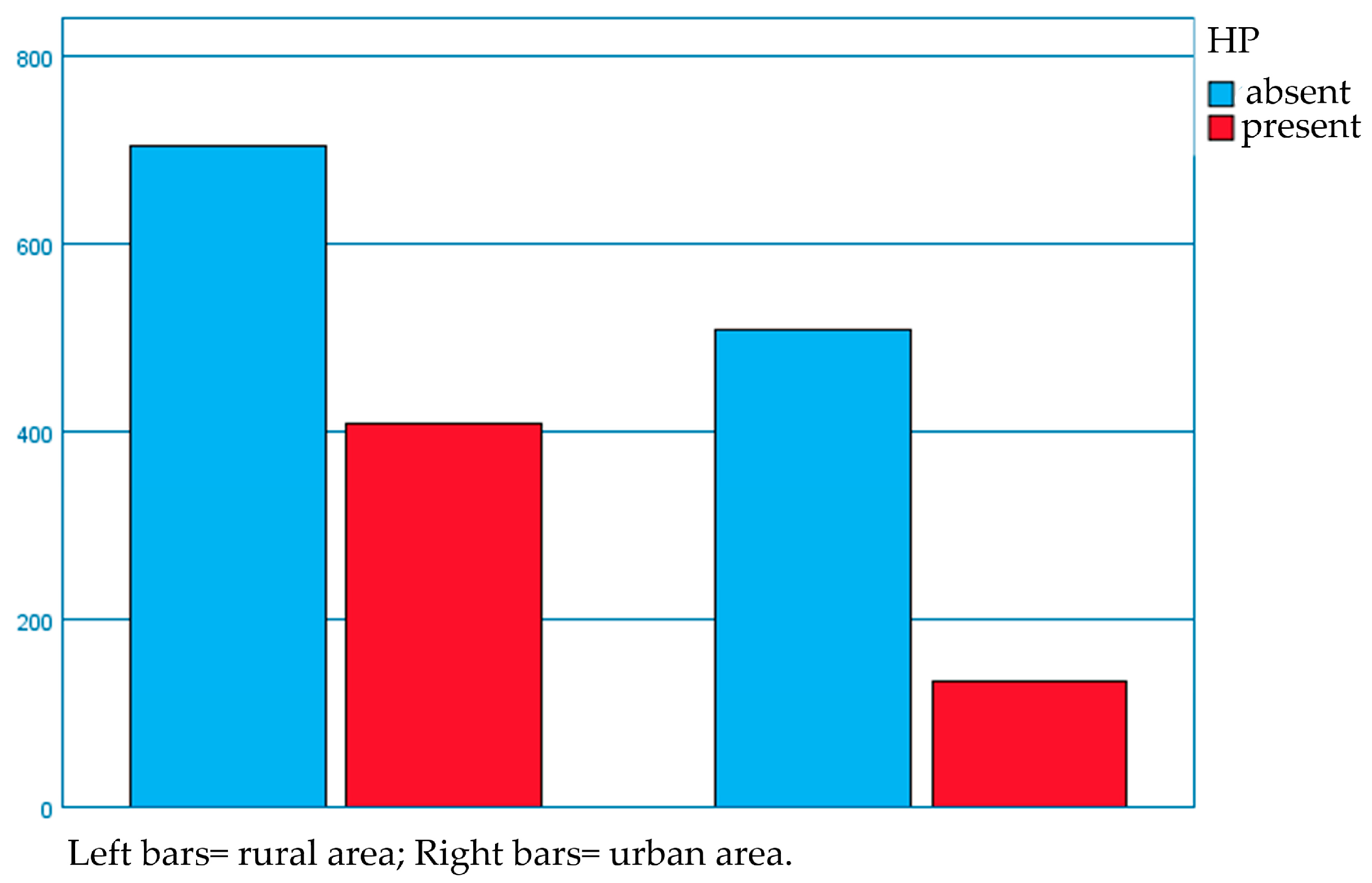
| Area of living | ||
| urban | 643 | 36.6 |
| rural | 1114 | 63.4 |
| Headache (+) | Headache (−) | |
|---|---|---|
| HP (+) | 54 | 488 |
| HP (−) | 76 | 1139 |
| p value = 0.006 |
| HP (+) | HP (−) | Headache (+) | Headache (−) | |
|---|---|---|---|---|
| Sex | ||||
| male | 145 | 402 | 22 | 525 |
| female | 397 | 813 | 108 | 1102 |
| p = 0.0002 chi-squared | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupu, A.; Gavrilovici, C.; Lupu, V.V.; Cianga, A.L.; Cernomaz, A.T.; Starcea, I.M.; Mihai, C.M.; Tarca, E.; Mocanu, A.; Fotea, S. Helicobacter pylori Infection in Children: A Possible Reason for Headache? Diagnostics 2023, 13, 1293. https://doi.org/10.3390/diagnostics13071293
Lupu A, Gavrilovici C, Lupu VV, Cianga AL, Cernomaz AT, Starcea IM, Mihai CM, Tarca E, Mocanu A, Fotea S. Helicobacter pylori Infection in Children: A Possible Reason for Headache? Diagnostics. 2023; 13(7):1293. https://doi.org/10.3390/diagnostics13071293
Chicago/Turabian StyleLupu, Ancuta, Cristina Gavrilovici, Vasile Valeriu Lupu, Anca Lavinia Cianga, Andrei Tudor Cernomaz, Iuliana Magdalena Starcea, Cristina Maria Mihai, Elena Tarca, Adriana Mocanu, and Silvia Fotea. 2023. "Helicobacter pylori Infection in Children: A Possible Reason for Headache?" Diagnostics 13, no. 7: 1293. https://doi.org/10.3390/diagnostics13071293