
Role of Changes in Driving Pressure and Mechanical Power in Predicting Mortality in Patients with Acute Respiratory Distress Syndrome
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Procedure
2.2. Disease Definitions
2.3. Ventilator Strategy and Intensive Management
2.4. Data Records
2.5. Calculation of MP
2.6. Statistical Analyses
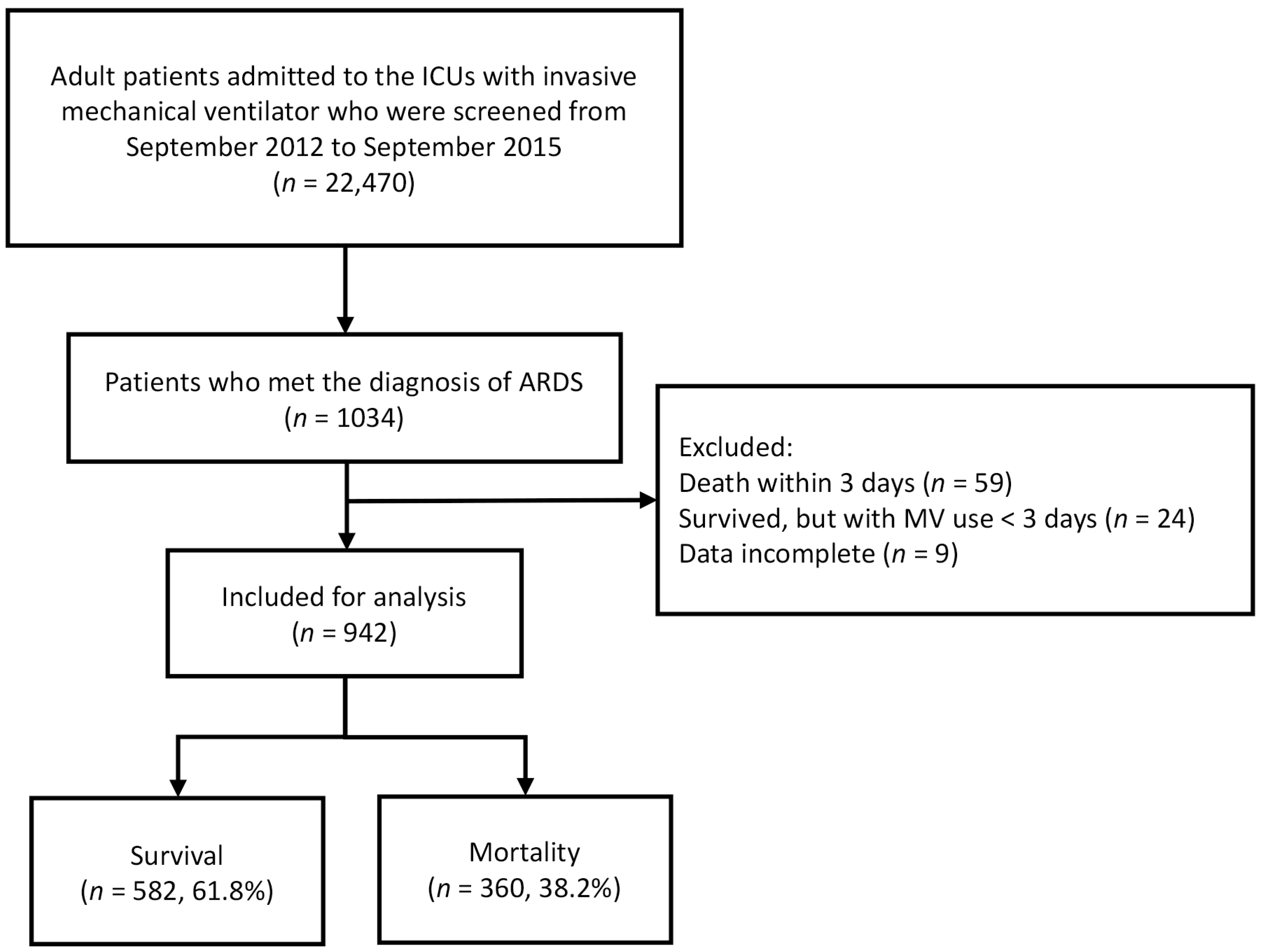
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.B.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.C.; Ho, C.H.; Kung, S.C.; Chen, W.L.; Wang, C.M.; Cheng, K.C.; Liu, W.L.; Hsu, H.S. Maintenance of low driving pressure in patients with early acute respiratory distress syndrome significantly affects outcomes. Respir. Res. 2021, 22, 313. [Google Scholar] [CrossRef]
- Zhang, Z.; Zheng, B.; Liu, N.; Ge, H.; Hong, Y. Mechanical power normalized to predicted body weight as a predictor of mortality in patients with acute respiratory distress syndrome. Intensive Care Med. 2019, 45, 856–864. [Google Scholar] [CrossRef]
- Parhar, K.K.S.; Zjadewicz, K.; Soo, A.; Sutton, A.; Zjadewicz, M.; Doig, L.; Lam, C.; Ferland, A.; Niven, D.J.; Fiest, K.M.; et al. Epidemiology, Mechanical Power, and 3-Year Outcomes in Acute Respiratory Distress Syndrome Patients Using Standardized Screening. An Observational Cohort Study. Ann. Am. Thorac. Soc. 2019, 16, 1263–1272. [Google Scholar] [CrossRef]
- Chiu, L.C.; Hu, H.C.; Hung, C.Y.; Chang, C.H.; Tsai, F.C.; Yang, C.T.; Huang, C.C.; Wu, H.P.; Kao, K.C. Dynamic driving pressure associated mortality in acute respiratory distress syndrome with extracorporeal membrane oxygenation. Ann. Intensive Care 2017, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Guerin, C.; Papazian, L.; Reignier, J.; Ayzac, L.; Loundou, A.; Forel, J.M. Effect of driving pressure on mortality in ARDS patients during lung protective mechanical ventilation in two randomized controlled trials. Crit. Care 2016, 20, 384. [Google Scholar] [CrossRef] [Green Version]
- Acute Respiratory Distress Syndrome Network; Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar]
- Mietto, C.; Malbrain, M.L.; Chiumello, D. Transpulmonary pressure monitoring during mechanical ventilation: A bench-to-bedside review. Anaesthesiol. Intensive Ther. 2015, 47, 27–37. [Google Scholar] [CrossRef]
- Cressoni, M.; Gotti, M.; Chiurazzi, C.; Massari, D.; Algieri, I.; Amini, M.; Cammaroto, A.; Brioni, M.; Montaruli, C.; Nikolla, K.; et al. Mechanical Power and Development of Ventilator-induced Lung Injury. Anesthesiology 2016, 124, 1100–1108. [Google Scholar] [CrossRef] [Green Version]
- Santos, R.S.; Maia, L.A.; Oliveira, M.V.; Santos, C.L.; Moraes, L.; Pinto, E.F.; Samary, C.D.S.; Machado, J.A.; Carvalho, A.C.; Fernandes, M.V.S.; et al. Biologic Impact of Mechanical Power at High and Low Tidal Volumes in Experimental Mild Acute Respiratory Distress Syndrome. Anesthesiology 2018, 128, 1193–1206. [Google Scholar] [CrossRef]
- Serpa, N.A.; Deliberato, R.O.; Johnson, A.E.W.; Bos, L.D.; Amorim, P.; Pereira, S.M.; Cazati, D.C.; Cordioli, R.L.; Correa, T.D.; Pollard, T.J.; et al. Mechanical power of ventilation is associated with mortality in critically ill patients: An analysis of patients in two observational cohorts. Intensive Care Med. 2018, 44, 1914–1922. [Google Scholar] [CrossRef]
- Xie, Y.; Cao, L.; Qian, Y.; Zheng, H.; Liu, K.; Li, X. Effect of Deep Sedation on Mechanical Power in Moderate to Severe Acute Respiratory Distress Syndrome: A Prospective Self-Control Study. BioMed Res. Int. 2020, 2020, 2729354. [Google Scholar] [CrossRef] [Green Version]
- Kao, K.C.; Hu, H.C.; Hsieh, M.J.; Tsai, Y.H.; Huang, C.C. Comparison of community-acquired, hospital-acquired, and intensive care unit-acquired acute respiratory distress syndrome: A prospective observational cohort study. Crit. Care 2015, 19, 384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Villar, J.; Martin-Rodriguez, C.; Dominguez-Berrot, A.M.; Fernandez, L.; Ferrando, C.; Soler, J.A.; Diaz-Lamas, A.M.; Gonzalez-Higueras, E.; Nogales, L.; Ambros, A.; et al. A Quantile Analysis of Plateau and Driving Pressures: Effects on Mortality in Patients With Acute Respiratory Distress Syndrome Receiving Lung-Protective Ventilation. Crit. Care Med. 2017, 45, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Becher, T.; van der Staay, M.; Schadler, D.; Frerichs, I.; Weiler, N. Calculation of mechanical power for pressure-controlled ventilation. Intensive Care Med. 2019, 45, 1321–1323. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.P.; Chu, C.M.; Chuang, L.P.; Lin, S.W.; Leu, S.W.; Chang, K.W.; Chiu, L.C.; Liu, P.H.; Kao, K.C. The Association between Mechanical Power and Mortality in Patients with Pneumonia Using Pressure-Targeted Ventilation. Diagnostics 2021, 11, 1862. [Google Scholar] [CrossRef]
- Del Sorbo, L.; Goffi, A.; Tomlinson, G.; Pettenuzzo, T.; Facchin, F.; Vendramin, A.; Goligher, E.C.; Cypel, M.; Slutsky, A.S.; Keshavjee, S.; et al. Effect of Driving Pressure Change During Extracorporeal Membrane Oxygenation in Adults With Acute Respiratory Distress Syndrome: A Randomized Crossover Physiologic Study. Crit. Care Med. 2020, 48, 1771–1778. [Google Scholar] [CrossRef]
- Ferguson, N.D.; Fan, E.; Camporota, L.; Antonelli, M.; Anzueto, A.; Beale, R.; Brochard, L.; Brower, R.; Esteban, A.; Gattinoni, L.; et al. The Berlin definition of ARDS: An expanded rationale, justification, and supplementary material. Intensive Care Med. 2012, 38, 1573–1582. [Google Scholar] [CrossRef]
- Pelosi, P.; Ball, L.; Barbas, C.S.V.; Bellomo, R.; Burns, K.E.A.; Einav, S.; Gattinoni, L.; Laffey, J.G.; Marini, J.J.; Myatra, S.N.; et al. Personalized mechanical ventilation in acute respiratory distress syndrome. Crit. Care 2021, 25, 250. [Google Scholar] [CrossRef]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; Cadringher, P.; Herrmann, P.; Moerer, O.; Protti, A.; Gotti, M.; Chiurazzi, C.; Carlesso, E.; et al. Ventilator-related causes of lung injury: The mechanical power. Intensive Care Med. 2016, 42, 1567–1575. [Google Scholar] [CrossRef]
- Moraes, L.; Silva, P.L.; Thompson, A.; Santos, C.L.; Santos, R.S.; Fernandes, M.V.S.; Morales, M.M.; Martins, V.; Capelozzi, V.L.; de Abreu, M.G.; et al. Impact of Different Tidal Volume Levels at Low Mechanical Power on Ventilator-Induced Lung Injury in Rats. Front. Physiol. 2018, 9, 318. [Google Scholar] [CrossRef]
- Wu, H.P.; Hu, H.C.; Chu, C.M.; Kao, K.C. The association between higher driving pressure and higher mortality in patients with pneumonia without acute respiratory distress syndrome. J. Formos. Med. Assoc. 2021, 120, 204–211. [Google Scholar] [CrossRef]
- Miller, R.R., III; Dong, L.; Nelson, N.C.; Brown, S.M.; Kuttler, K.G.; Probst, D.R.; Allen, T.L.; Clemmer, T.P. Multicenter implementation of a severe sepsis and septic shock treatment bundle. Am. J. Respir. Crit. Care Med. 2013, 188, 77–82. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Patients (n = 942) | Survivors (n = 582) | Non-Survivors (n = 360) | p-Value |
|---|---|---|---|---|
| Age (years) * | 63.1 ± 16.2 | 62.3 ± 16.8 | 64.4 ± 15.0 | 0.040 |
| Gender, n (%) | 0.605 | |||
| Male | 653 (69.3) | 407 (69.9) | 246 (68.3) | |
| Female | 289 (30.7) | 175 (30.1) | 114 (31.7) | |
| Charlson Comorbidity Index * | 2.6 ± 2.2 | 2.4 ± 2.1 | 3.0 ± 2.4 | <0.001 |
| APACHE II score * | 23.2 ± 7.1 | 22.4 ± 7.1 | 24.5 ± 6.7 | <0.001 |
| SOFA score * | 9.8 ± 3.4 | 9.2 ± 3.1 | 10.7 ± 3.7 | <0.001 |
| Lung injury score * | 2.9 ± 0.5 | 2.9 ± 0.5 | 2.9 ± 0.5 | 0.066 |
| Severity of ARDS, n (%) | 0.155 | |||
| Mild | 214 (22.7) | 143 (24.6) | 71 (19.7) | |
| Moderate | 377 (40.0) | 233 (40.0) | 144 (40.0) | |
| Severe | 351 (37.3) | 206 (35.4) | 145 (40.3) | |
| Causes of ARDS, n (%) | 0.020 | |||
| Pneumonia | 670 (71.1) | 415 (71.3) | 255 (70.8) | |
| Sepsis | 127 (13.5) | 70 (12.0) | 57 (15.8) | |
| Aspiration | 50 (5.3) | 32 (5.5) | 18 (5.0) | |
| Post-surgery | 11 (1.2) | 9 (1.6) | 2 (0.6) | |
| Trauma | 23 (2.4) | 21 (3.6) | 2 (0.6) | |
| Others | 61 (6.5) | 35 (6.0) | 26 (7.2) | |
| PaO2/FiO2 (mm Hg) * | 141.1 ± 74.3 | 142.2 ± 72.2 | 136.8 ± 70.6 | 0.261 |
| ECMO support | 57 (6.1) | 41 (7.0) | 16 (4.4) | 0.122 |
| Ventilator parameters * | ||||
| Tidal volume (mL/kg PBW) | 8.4 ± 2.6 | 8.4 ± 2.6 | 8.4 ± 2.5 | 0.862 |
| PEEP (cm H2O) | 9.9 ± 2.1 | 9.9 ± 2.2 | 9.8 ± 2.0 | 0.728 |
| Driving pressure (cm H2O) | 19.4 ± 5.4 | 19.1 ± 5.3 | 19.9 ± 5.4 | 0.038 |
| Respiratory rate (/min) | 21.5 ± 5.9 | 21.6 ± 6.2 | 21.3 ± 5.3 | 0.411 |
| Mechanical power (J/min) | 28.3 ± 11.2 | 28.2 ± 11.2 | 28.4 ± 11.1 | 0.846 |
| Ventilator parameters after 2 days * | ||||
| Tidal volume (mL/kg PBW) | 8.3 ± 2.8 | 8.4 ± 3.0 | 8.3 ± 2.5 | 0.594 |
| PEEP (cm H2O) | 10.8 ± 2.6 | 10.5 ± 2.6 | 11.2 ± 2.6 | <0.001 |
| Driving pressure (cm H2O) | 17.6 ± 5.8 | 16.5 ± 5.6 | 19.5 ± 5.7 | <0.001 |
| Respiratory rate (/min) | 22.1 ± 5.6 | 21.4 ± 5.7 | 23.1 ± 5.3 | <0.001 |
| Mechanical power (J/min) | 28.0 ± 11.8 | 26.0 ± 11.2 | 31.3 ± 12.0 | <0.001 |
| Change in driving pressure (cm H2O) * | −1.8 ± 6.0 | −2.7 ± 5.9 | −0.4 ± 5.8 | <0.001 |
| Change in mechanical power (J/min) * | −0.2 ± 13.9 | −2.2 ± 13.5 | 2.9 ± 14.0 | <0.001 |
| Variables | Univariate OR (95% CI) | p-Value | Multivariate OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age | 1.008 (1.000–1.017) | 0.046 | 1.012 (1.003–1.022) | 0.014 |
| Charlson Comorbidity Index | 1.134 (1.070–1.203) | <0.001 | 1.056 (0.990–1.127) | 0.099 |
| APACHE II score | 1.042 (1.023–1.062) | <0.001 | 0.995 (0.970–1.020) | 0.668 |
| SOFA score | 1.142 (1.097–1.189) | <0.001 | 1.144 (1.086–1.206) | <0.001 |
| Trauma | 0.128 (0.028–0.596) | 0.009 | 0.172 (0.035–0.839) | 0.029 |
| Driving pressure | 1.027 (1.002–1.052) | 0.038 | 1.077 (1.044–1.111) | <0.001 |
| Change in driving pressure | 1.069 (1.044–1.094) | <0.001 | 1.087 (1.054–1.120) | <0.001 |
| Change in mechanical power | 1.028 (1.018–1.039) | <0.001 | 1.018 (1.006–1.029) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, H.-P.; Leu, S.-W.; Lin, S.-W.; Hung, C.-Y.; Chen, N.-H.; Hu, H.-C.; Huang, C.-C.; Kao, K.-C. Role of Changes in Driving Pressure and Mechanical Power in Predicting Mortality in Patients with Acute Respiratory Distress Syndrome. Diagnostics 2023, 13, 1226. https://doi.org/10.3390/diagnostics13071226
Wu H-P, Leu S-W, Lin S-W, Hung C-Y, Chen N-H, Hu H-C, Huang C-C, Kao K-C. Role of Changes in Driving Pressure and Mechanical Power in Predicting Mortality in Patients with Acute Respiratory Distress Syndrome. Diagnostics. 2023; 13(7):1226. https://doi.org/10.3390/diagnostics13071226
Chicago/Turabian StyleWu, Huang-Pin, Shaw-Woei Leu, Shih-Wei Lin, Chen-Yiu Hung, Ning-Hung Chen, Han-Chung Hu, Chung-Chi Huang, and Kuo-Chin Kao. 2023. "Role of Changes in Driving Pressure and Mechanical Power in Predicting Mortality in Patients with Acute Respiratory Distress Syndrome" Diagnostics 13, no. 7: 1226. https://doi.org/10.3390/diagnostics13071226