
Differentiation of Spontaneous Bacterial Peritonitis from Secondary Peritonitis in Patients with Liver Cirrhosis: Retrospective Multicentre Study
 , ,
, ,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
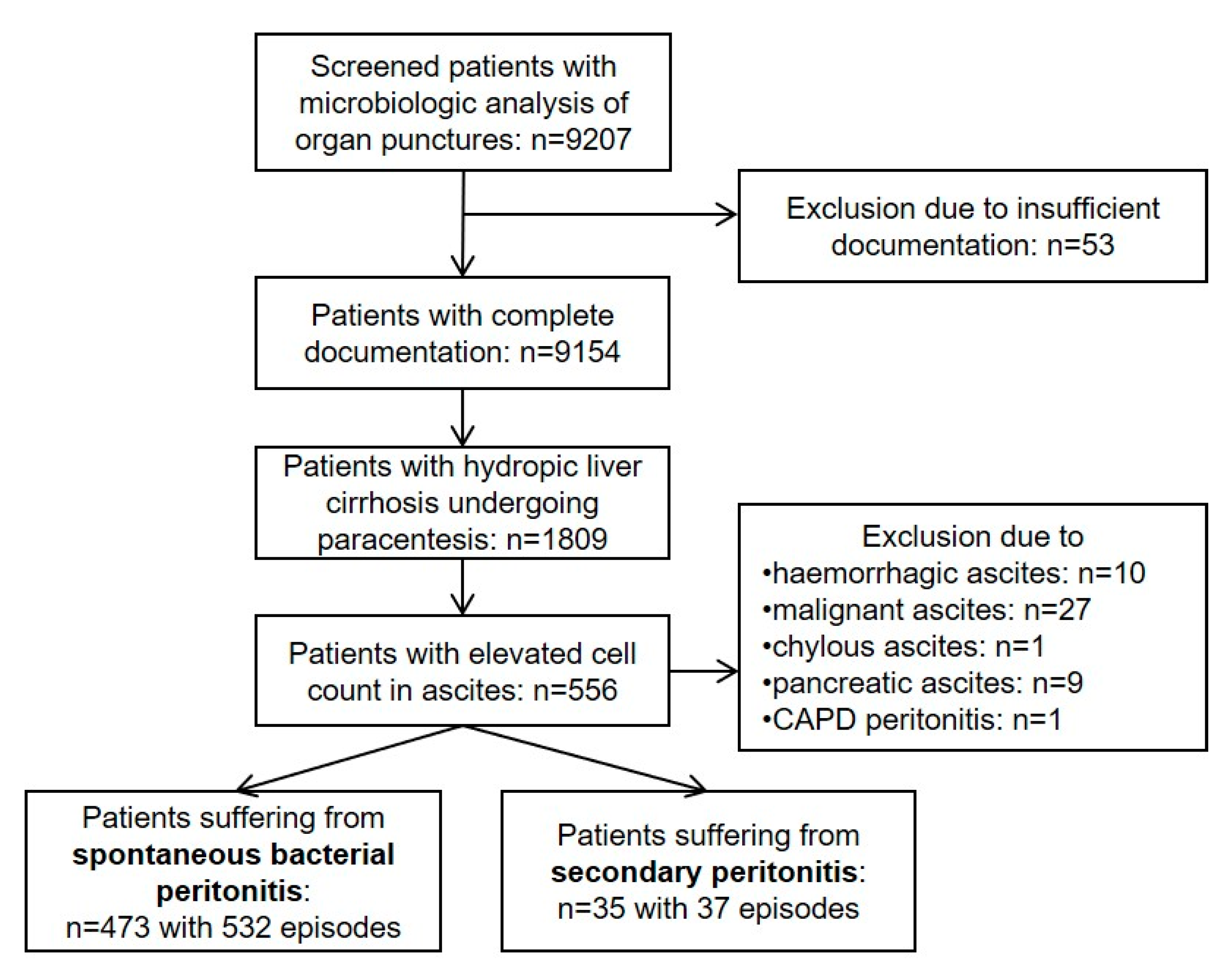
2.1. Study Population
2.2. Definition of SecP
2.3. Assessment of Predictors
2.4. Ethics
2.5. Sample Method and Microbiological Analysis
2.6. Statistical Methods
3. Results
3.1. Baseline Characteristics
3.2. Univariable Analyses
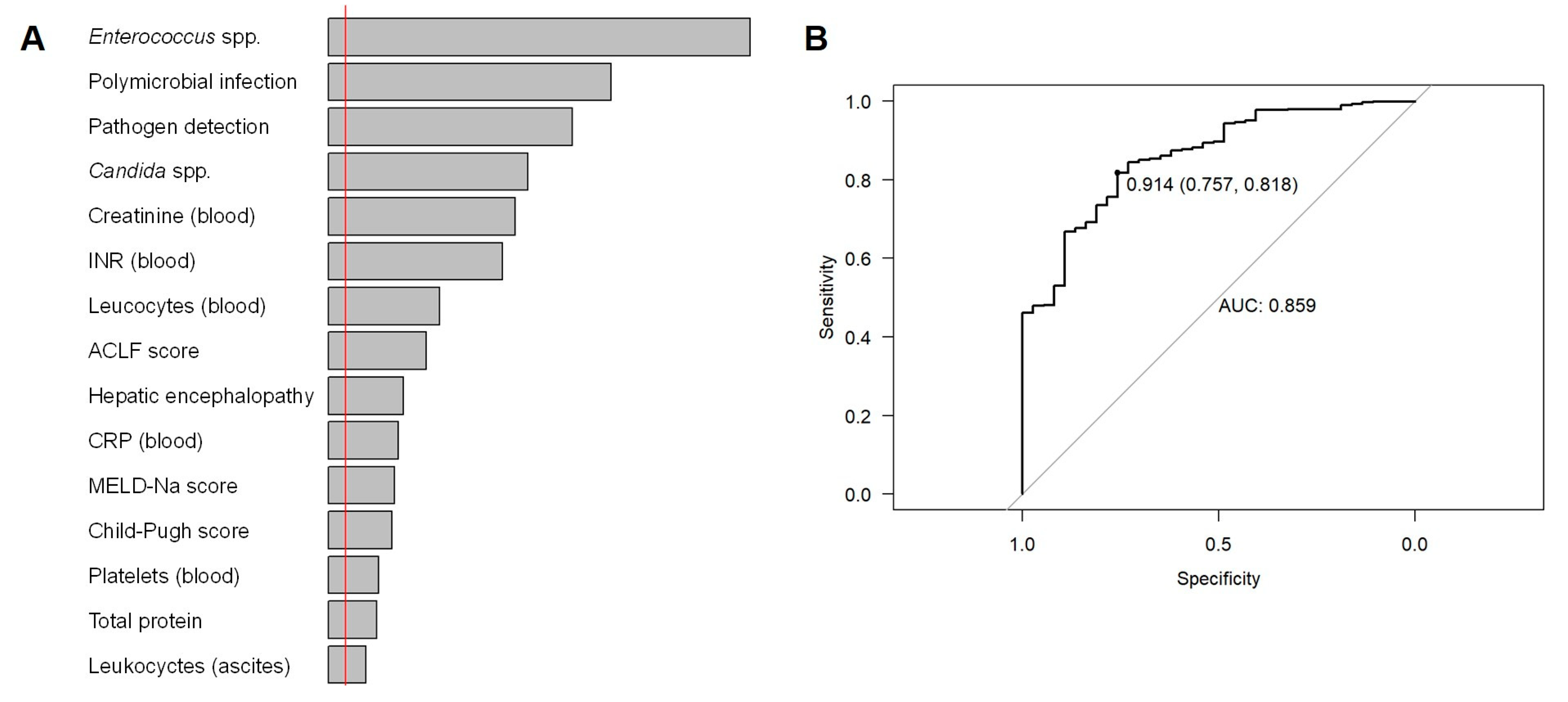
3.3. Random Forest Model: Important Features
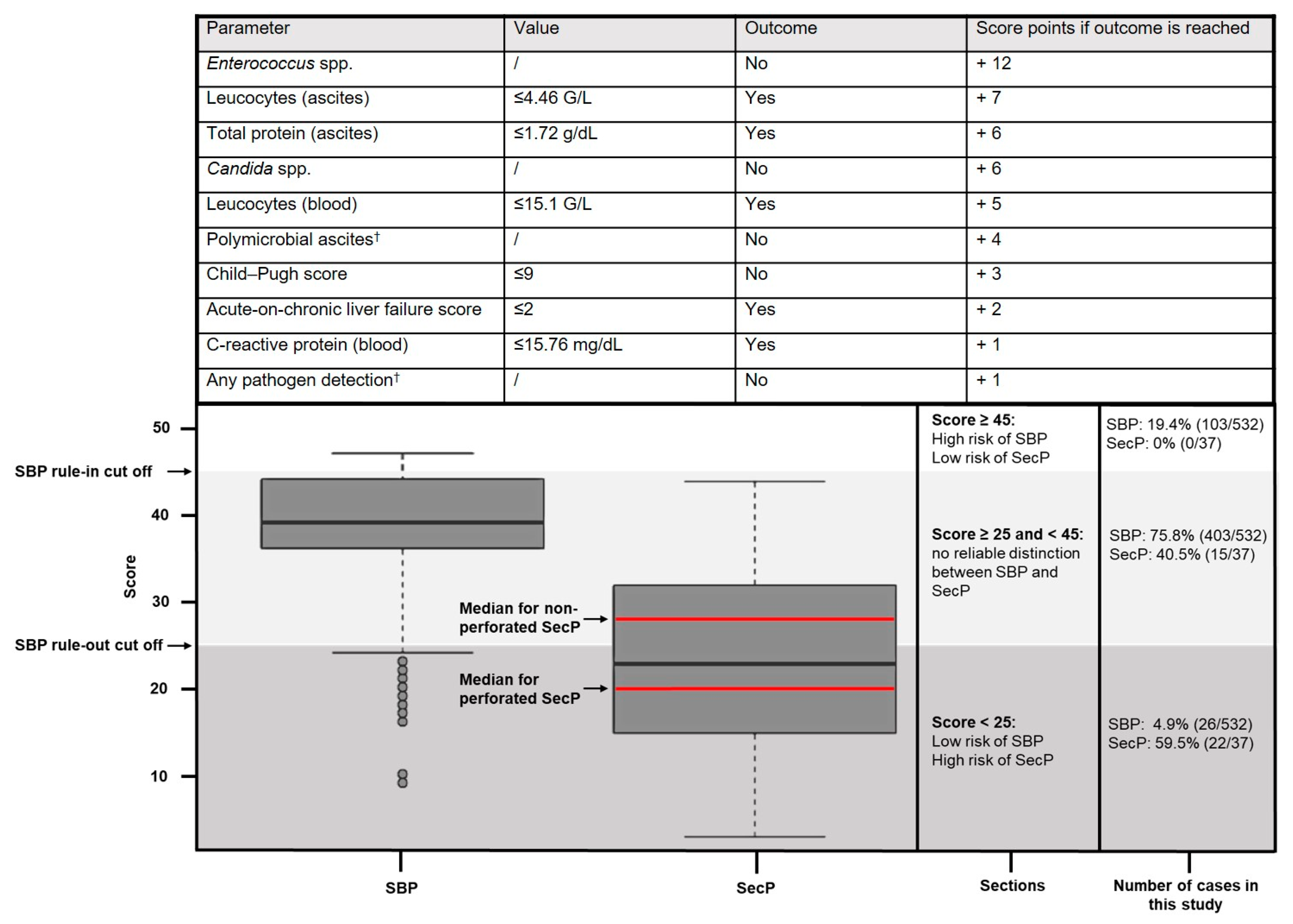
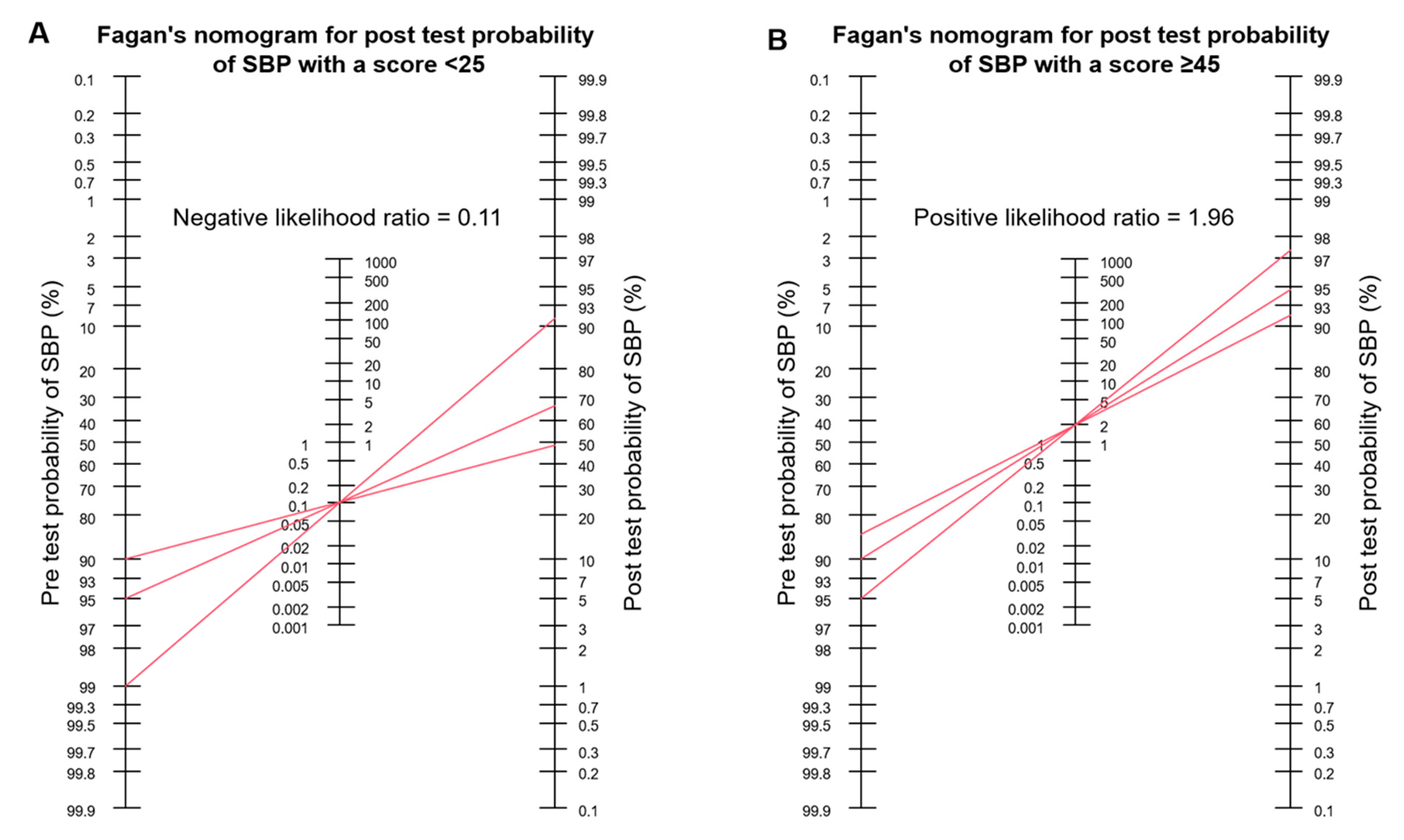
3.4. LASSO Regression Point-Score Model
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Aithal, G.P.; Palaniyappan, N.; China, L.; Harmala, S.; Macken, L.; Ryan, J.M.; Wilkes, E.A.; Moore, K.; Leithead, J.A.; Hayes, P.C.; et al. Guidelines on the management of ascites in cirrhosis. Gut 2021, 70, 9–29. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L: EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [Green Version]
- Soriano, G.; Castellote, J.; Alvarez, C.; Girbau, A.; Gordillo, J.; Baliellas, C.; Casas, M.; Pons, C.; Román, E.M.; Maisterra, S.; et al. Secondary bacterial peritonitis in cirrhosis: A retrospective study of clinical and analytical characteristics, diagnosis and management. J. Hepatol. 2010, 52, 39–44. [Google Scholar] [CrossRef]
- Wiest, R.; Schoelmerich, J. Secondary peritonitis in cirrhosis: “Oil in fire”. J. Hepatol. 2010, 52, 7–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Würstle, S.; Hapfelmeier, A.; Karapetyan, S.; Studen, F.; Isaakidou, A.; Schneider, T.; Schmid, R.M.; von Delius, S.; Gundling, F.; Triebelhorn, J.; et al. A Novel Machine Learning-Based Point-Score Model as a Non-Invasive Decision-Making Tool for Identifying Infected Ascites in Patients with Hydropic Decompensated Liver Cirrhosis: A Retrospective Multicentre Study. Antibiotics 2022, 11, 1610. [Google Scholar] [CrossRef]
- Mowat, C.; Stanley, A.J. Review article: Spontaneous bacterial peritonitis—Diagnosis, treatment and prevention. Aliment. Pharmacol. Ther. 2001, 15, 1851–1859. [Google Scholar] [CrossRef] [PubMed]
- Tay, P.W.L.; Xiao, J.; Tan, D.J.H.; Ng, C.; Lye, Y.N.; Lim, W.H.; Teo, V.X.Y.; Heng, R.R.Y.; Yeow, M.W.X.; Lum, L.H.W.; et al. An Epidemiological Meta-Analysis on the Worldwide Prevalence, Resistance, and Outcomes of Spontaneous Bacterial Peritonitis in Cirrhosis. Front. Med. 2021, 8, 693652. [Google Scholar] [CrossRef] [PubMed]
- Bonadio, W.; Molyneux, K.; Lavine, E.; Jackson, K.; Kagen, A.; Legome, E. Utility of measuring serum creatinine to detect renal compromise in ED patients receiving IV contrast-enhanced CT scan. Emerg. Radiol. 2021, 28, 899–902. [Google Scholar] [CrossRef]
- Caraiani, C.; Petresc, B.; Dong, Y.; Dietrich, C.F. Contraindications and adverse effects in abdominal imaging. Med. Ultrason. 2019, 21, 456–463. [Google Scholar] [CrossRef]
- Safi, W.; Rauscher, I.; Umgelter, A. Contrast-induced acute kidney injury in cirrhotic patients. A retrospective analysis. Ann. Hepatol. 2015, 14, 895–901. [Google Scholar] [CrossRef]
- Caralis, P.V.; Sprung, C.L.; Schiff, E.R. Secondary bacterial peritonitis in cirrhotic patients with ascites. South. Med. J. 1984, 77, 579–583. [Google Scholar] [CrossRef]
- Akriviadis, E.A.; Runyon, B.A. Utility of an algorithm in differentiating spontaneous from secondary bacterial peritonitis. Gastroenterology 1990, 98, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.S.; Lin, O.S.; Chen, Y.Y.; Hwang, K.L.; Soon, M.S.; Keeffe, E.B. Ascitic fluid carcinoembryonic antigen and alkaline phosphatase levels for the differentiation of primary from secondary bacterial peritonitis with intestinal perforation. J. Hepatol. 2001, 34, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Ruault, C.; Zappella, N.; Labreuche, J.; Cronier, P.; Claude, B.; Garnier, M.; Vieillard-Baron, A.; Ortuno, S.; Mallet, M.; Cosic, O.; et al. Identifying early indicators of secondary peritonitis in critically ill patients with cirrhosis. Sci. Rep. 2021, 11, 21076. [Google Scholar] [CrossRef] [PubMed]
- Runyon, B.A.; Hoefs, J.C. Ascitic fluid analysis in the differentiation of spontaneous bacterial peritonitis from gastrointestinal tract perforation into ascitic fluid. Hepatology 1984, 4, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Ruf, A.; Dirchwolf, M.; Freeman, R.B. From Child-Pugh to MELD score and beyond: Taking a walk down memory lane. Ann. Hepatol. 2022, 27, 100535. [Google Scholar] [CrossRef] [PubMed]
- Biggins, S.W.; Kim, W.R.; Terrault, N.A.; Saab, S.; Balan, V.; Schiano, T.; Benson, J.; Therneau, T.; Kremers, W.; Wiesner, R.; et al. Evidence-based incorporation of serum sodium concentration into MELD. Gastroenterology 2006, 130, 1652–1660. [Google Scholar] [CrossRef] [PubMed]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013, 144, 1426–1437. [Google Scholar] [CrossRef]
- CLIF: CLIF-C-ACFL Calculator. European Foundation for the Study of Chronic Liver Failure. 2022. Available online: https://www.efclif.com/scientific-activity/score-calculators/clif-c-aclf (accessed on 14 January 2023).
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Donato, V.; D’Oria, O.; Giannini, A.; Bogani, G.; Fischetti, M.; Santangelo, G.; Tomao, F.; Palaia, I.; Perniola, G.; Muzii, L.; et al. Age-Adjusted Charlson Comorbidity Index Predicts Survival in Endometrial Cancer Patients. Gynecol. Obs. Investig. 2022, 87, 191–199. [Google Scholar] [CrossRef]
- Stekhoven, D.J.; Buhlmann, P. MissForest—Non-parametric missing value imputation for mixed-type data. Bioinformatics 2012, 28, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Hothorn, T.; Hornik, K.; Zeileis, A. Unbiased recursive partitioning: A conditional inference framework. J. Comput. Graph Stat. 2006, 15, 651–674. [Google Scholar] [CrossRef] [Green Version]
- Hapfelmeier, A.; Hothorn, T.; Ulm, K.; Strobl, C. A new variable importance measure for random forests with missing data. Stat. Comput. 2014, 24, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Hothorn, T.; Lausen, B. On the exact distribution of maximally selected rank statistics. Comput. Stat. Data Anal. 2003, 43, 121–137. [Google Scholar] [CrossRef]
- Lu, M.L.R.; Agarwal, A.; Sloan, J.; Kosmin, A. Infected ascites: Distinguishing secondary peritonitis from spontaneous bacterial peritonitis in a cirrhotic patient with classic symptoms. IDCases 2017, 8, 29–31. [Google Scholar] [CrossRef]
- Dever, J.B.; Sheikh, M.Y. Review article: Spontaneous bacterial peritonitis—Bacteriology, diagnosis, treatment, risk factors and prevention. Aliment. Pharmacol. Ther. 2015, 41, 1116–1131. [Google Scholar] [CrossRef]
- Paul, K.; Kaur, J.; Kazal, H.L. To Study the Incidence, Predictive Factors and Clinical Outcome of Spontaneous Bacterial Peritonitis in Patients of Cirrhosis with Ascites. J. Clin. Diagn. Res. JCDR 2015, 9, OC09-12. [Google Scholar] [CrossRef]
- Targan, S.R.; Chow, A.W.; Guze, L.B. Role of anaerobic bacteria in spontaneous peritonitis of cirrhosis: Report of two cases and review of the literature. Am. J. Med. 1977, 62, 397–403. [Google Scholar] [CrossRef]
- Reuken, P.A.; Pletz, M.W.; Baier, M.; Pfister, W.; Stallmach, A.; Bruns, T. Emergence of spontaneous bacterial peritonitis due to enterococci—Risk factors and outcome in a 12-year retrospective study. Aliment. Pharmacol. Ther. 2012, 35, 1199–1208. [Google Scholar] [CrossRef]
- Karvellas, C.J.; Abraldes, J.G.; Arabi, Y.M.; Kumar, A. Cooperative Antimicrobial Therapy of Septic Shock Database Research G: Appropriate and timely antimicrobial therapy in cirrhotic patients with spontaneous bacterial peritonitis-associated septic shock: A retrospective cohort study. Aliment. Pharmacol. Ther. 2015, 41, 747–757. [Google Scholar] [CrossRef]
- Marciano, S.; Diaz, J.M.; Dirchwolf, M.; Gadano, A. Spontaneous bacterial peritonitis in patients with cirrhosis: Incidence, outcomes, and treatment strategies. Hepatic Med. Evid. Res. 2019, 11, 13–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.W.; Yoon, J.S.; Park, J.; Jung, Y.J.; Lee, J.S.; Song, J.; Lee, H.A.; Seo, Y.S.; Lee, M.; Park, J.M.; et al. Empirical Treatment With Carbapenem vs Third-generation Cephalosporin for Treatment of Spontaneous Bacterial Peritonitis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2021, 19, 976–986 e975. [Google Scholar] [CrossRef] [PubMed]
- Sheckman, P.; Onderdonk, A.B.; Bartlett, J.G. Anaerobes in spontaneous peritonitis. Lancet 1977, 2, 1223. [Google Scholar] [CrossRef]
- Jang, J.Y.; Lee, S.H.; Shim, H.; Choi, J.Y.; Yong, D.; Lee, J.G. Epidemiology and Microbiology of Secondary Peritonitis Caused by Viscus Perforation: A Single-Center Retrospective Study. Surg. Infect. 2015, 16, 436–442. [Google Scholar] [CrossRef]
- Würstle, S.; Hapfelmeier, A.; Ka-rapetyan, S.; Studen, F.; Isaakidou, A.; Schneider, T.; Schmid, R.M.; von Delius, S.; Gundling, F.; Burgkart, R.; et al. Differentiation of Spontaneous Bacterial Peritonitis from Secondary Peritonitis in Patients with Liver Cirrhosis: Retrospective Multicentre Study. 2023. Available online: https://bookerar.shinyapps.io/Score_SecP/ (accessed on 14 January 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | SecP Episodes (n = 37; 35 Patients) | SBP Episodes (n = 532; 473 Patients) | p-Value |
|---|---|---|---|
| Clinical parameters | |||
| Age (years) † | 63 (45–92) | 63 (23–88) | 0.573 |
| Female patients † | 20.0% (7/35) | 25.2% (119/473) | 0.911 |
| Length of stay (days) † | 32 (2–124) | 17 (1–287) | 0.005 |
| ICU admission † | 73.0% (27/37) | 44.5% (237/532) | 0.001 |
| Mortality † | 45.7% (16/35) | 39.7% (188/473) | 0.428 |
| Laboratory parameters | |||
| Creatinine in serum (mg/dL) | 2.9 (1.0–4.0; 1 NA) | 1.7 (0.9–4.0; 9 NA) | 0.01 |
| C-reactive protein in serum (mg/dL) | 10.4 (1.1–34.3; 5 NA) | 6.1 (0.1–32.7; 84 NA) | 0.004 |
| Leucocytes in blood (G/L) | 12.7 (3.2–27.8) | 9.1 (1.2–41.0; 6 NA) | 0.007 |
| Leucocytes in ascites (G/L) | 4.0 (0.5–70.3) | 1.5 (0.1–146.0) | 0.027 |
| Microbiologic parameters | |||
| Pathogen detection | 78.4% (29/37) | 42.1% (224/532) | <0.001 |
| Polymicrobial infection | 62.1% (18/29) | 16.5% (37/224) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Würstle, S.; Hapfelmeier, A.; Karapetyan, S.; Studen, F.; Isaakidou, A.; Schneider, T.; Schmid, R.M.; von Delius, S.; Gundling, F.; Burgkart, R.; et al. Differentiation of Spontaneous Bacterial Peritonitis from Secondary Peritonitis in Patients with Liver Cirrhosis: Retrospective Multicentre Study. Diagnostics 2023, 13, 994. https://doi.org/10.3390/diagnostics13050994
Würstle S, Hapfelmeier A, Karapetyan S, Studen F, Isaakidou A, Schneider T, Schmid RM, von Delius S, Gundling F, Burgkart R, et al. Differentiation of Spontaneous Bacterial Peritonitis from Secondary Peritonitis in Patients with Liver Cirrhosis: Retrospective Multicentre Study. Diagnostics. 2023; 13(5):994. https://doi.org/10.3390/diagnostics13050994
Chicago/Turabian StyleWürstle, Silvia, Alexander Hapfelmeier, Siranush Karapetyan, Fabian Studen, Andriana Isaakidou, Tillman Schneider, Roland M. Schmid, Stefan von Delius, Felix Gundling, Rainer Burgkart, and et al. 2023. "Differentiation of Spontaneous Bacterial Peritonitis from Secondary Peritonitis in Patients with Liver Cirrhosis: Retrospective Multicentre Study" Diagnostics 13, no. 5: 994. https://doi.org/10.3390/diagnostics13050994