
Red Blood Cell Alloimmunization and Its Associated Factors among Chronic Liver Disease Patients in a Teaching Hospital in Northeastern Malaysia
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
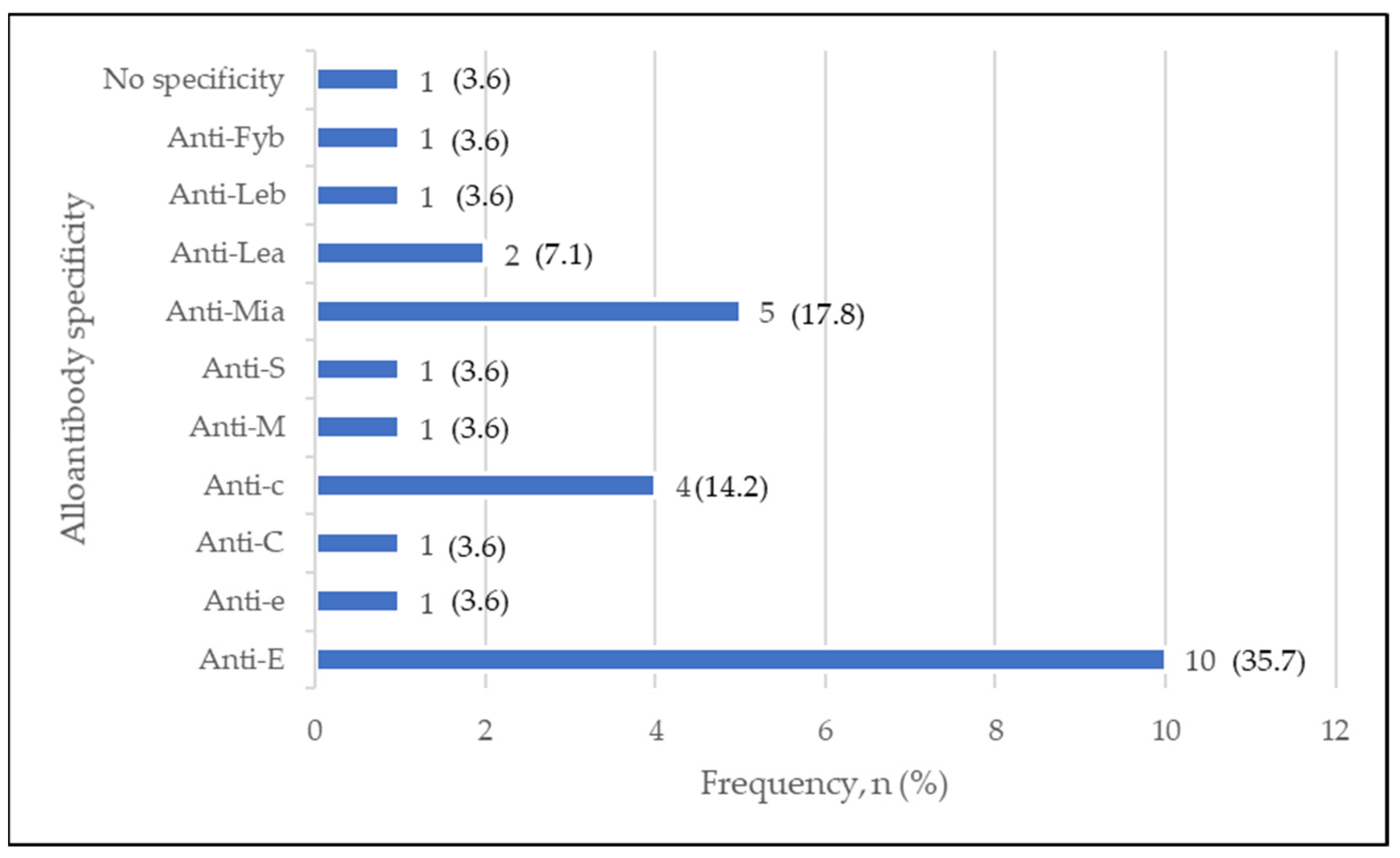
3.1. Prevalence and Specificity of RBC Alloantibody among CLD Patients
3.2. Factors Associated with RBC Alloimmunization among CLD Patients
4. Discussion
4.1. RBC Alloantibody Specificity among Alloimmunized CLD Patients
4.2. Factors Associated with RBC Alloimmunization in CLD Patients
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017. Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar]
- Gkamprela, E.; Deutsch, M.; Pectasides, D. Iron deficiency anemia in chronic liver disease: Etiopathogenesis, diagnosis and treatment. Ann. Gastroenterol. 2017, 30, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajpai, M.; Gupta, S.; Jain, P. Alloimmunization in multitransfused liver disease patients: Impact of underlying disease. Asian J. Transfus. Sci. 2016, 10, 136. [Google Scholar] [CrossRef] [PubMed]
- Jan, R.-H.; Yu, L.-C.; Wen, S.-H.; Tsai, S.-S.; Lin, T.-Y. Incidence of Alloantibodies in Transfused Patients in Eastern Taiwan. Tzu Chi Med. J. 2009, 21, 66–69. [Google Scholar] [CrossRef] [Green Version]
- Hendrickson, J.E.; Tormey, C.A. Understanding red blood cell alloimmunization triggers. Hematology 2016, 2016, 446–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tormey, C.A.; Hendrickson, J.E. Transfusion-related red blood cell alloantibodies: Induction and consequences. Blood 2019, 133, 1821–1830. [Google Scholar] [CrossRef] [Green Version]
- Philip, J.; Biswas, M.A.K.; Hiregoudar, S.; Kushwaha, N. Red Blood Cell Alloimmunization in Multitransfused Patients in a Tertiary Care Center in Western India. Lab. Med. 2014, 45, 324–330. [Google Scholar] [CrossRef] [Green Version]
- Yangdon, T. Prevalence of “unexpected antibodies” in patients requiring blood transfusion at National Referral Hospital, Thimphu from 2015 to 2017: Retrospective study. J. Med. Sci. Clin. Res. 2019, 7, 2015–2019. [Google Scholar] [CrossRef]
- Nickel, R.S.; Hendrickson, J.E.; Fasano, R.M.; Meyer, E.K.; Winkler, A.M.; Yee, M.M.; Lane, P.A.; Jones, Y.A.; Pashankar, F.D.; New, T.; et al. Impact of red blood cell alloimmunization on sickle cell disease mortality: A case series. Transfusion 2015, 56, 107–114. [Google Scholar] [CrossRef]
- Yousuf, R.; Aziz, S.A.; Yusof, N.; Leong, C.F. Incidence of Red Cell Alloantibody among the Transfusion Recipients of Universiti Kebangsaan Malaysia Medical Centre. Indian J. Hematol. Blood Transfus. 2012, 29, 65–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.-Y.; Cho, E.-J.; Chun, S.; Kim, K.-H.; Cho, D. Red Blood Cell Alloimmunization in Korean Patients with Myelodysplastic Syndrome and Liver Cirrhosis. Ann. Lab. Med. 2019, 39, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Harmening, D. Modern Blood Banking and Transfusion Practices; F.A. Davis: Philadelphia, PA, USA, 2019; pp. 233–253. [Google Scholar]
- Yazdanbakhsh, K.; Ware, R.E.; Noizat-Pirenne, F. Red blood cell alloimmunization in sickle cell disease: Pathophysiology, risk factors, and transfusion management. Blood 2012, 120, 528–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosse, W.F.; Gallagher, D.; Kinney, T.R.; Castro, O.; Dosik, H.; Moohr, J.; Wang, W.; Levy, P.S. Transfusion and Alloimmunization in Sickle Cell Disease. Blood 1990, 76, 1431–1437. [Google Scholar] [CrossRef] [Green Version]
- Ho, H.K.; Ha, S.Y.; Lam, C.K.; Chan, G.C.F.; Lee, T.L.; Alan, K.S.; Chiang, Y.-L.L. Alloimmunization in Hong Kong southern Chinese transfusion-dependent thalassemia patients. Blood 2001, 97, 3999–4000. Available online: http://ashpublications.org/blood/article-pdf/97/12/3999/1675482/h8120103998a.pdf (accessed on 30 January 2023). [CrossRef] [Green Version]
- Yusoff, S.M.; Bahar, R.; Hassan, M.N.; Noor, N.H.M.; Ramli, M.; Shafii, N.F. Prevalence of Red Blood Cell Alloimmunization among Transfused Chronic Kidney Disease Patients in Hospital Universiti Sains Malaysia. Oman Med. J. 2020, 35, e177. [Google Scholar] [CrossRef]
- Natukunda, B.; Schonewille, H.; Van De Watering, L.; Brand, A. Prevalence and specificities of red blood cell alloantibodies in transfused Ugandans with different diseases. Vox Sang. 2010, 98, 167–171. [Google Scholar] [CrossRef]
- Qayyum, A.; Hameed, A.; Hamid, A.; Siddiqua, A.; Naveed, A. Determination of Red Cell Antigen Alloimmunization and Specific Type of Antibody in Multi-Transfused Liver Cirrhosis Patient. Ann. Punjab Med. Coll. 2018, 12, 186–190. [Google Scholar]
- Karafin, M.S.; Westlake, M.; Hauser, R.G.; Tormey, C.A.; Norris, P.J.; Roubinian, N.H.; Wu, Y.; Triulzi, D.J.; Kleinman, S.; Hendrickson, J.E.; et al. Risk factors for red blood cell alloimmunization in the Recipient Epidemiology and Donor Evaluation Study (REDS-III) database. Br. J. Haematol. 2018, 181, 672–681. [Google Scholar] [CrossRef] [Green Version]
- Mohsin, S.; Amjad, S.; Amin, H.; Saeed, T. Red Cell Alloimmunization in Repeatedly Transfused Cancer Patients. J. Rawalpindi Med. Coll. 2013, 17, 219–222. [Google Scholar]
- Schonewille, H.; Haak, H.; Van Zijl, A. Alloimmunization after blood transfusion in patients with hematologic and oncologic diseases. Transfusion 1999, 39, 763–771. [Google Scholar] [CrossRef]
- Dogra, A.; Sidhu, M.; Kapoor, R.; Kumar, D. Study of red blood cell alloimmunization in multitransfused thalassemic children of Jammu region. Asian J. Transfus. Sci. 2015, 9, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Luzo, C.M.; Pereira, F.B.; de Oliveira, R.C.; Azevedo, P.R.; Cunha, R.D.; Leonardi, M.; Leonardi, L.; Cardoso, A.; Caruy, C.; Ataíde, E.; et al. Red Blood Cell Antigen Alloimmunization in Liver Transplant Recipients. Transplant. Proc. 2010, 42, 494–495. [Google Scholar] [CrossRef] [PubMed]
- Noor, N.H.M.; Arifin, N.; Hassan, M.N.; Mustaffa, R. Red cell alloimmunization among haemato-oncologic patients in a teaching hospital in Malaysia. Sri Lanka J. Med. 2019, 28, 41. [Google Scholar] [CrossRef]
- Fluit, C.; Kunst, V.; Drenthe-Schonk, A. Incidence of red cell antibodies after multiple blood transfusion. Transfusion 1990, 30, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Musa, R.H.; Ahmed, S.A.; Hashim, H.; Ayob, Y.; Asidin, N.H.; Choo, P.Y.; Al-Joudi, F.S. Indian Society of Blood Transfusion and Immunohaematology Red cell phenotyping of blood from donors at the National blood center of Malaysia. Asian J. Transfus. Sci. 2012, 6, 3. [Google Scholar]
- Yousuf, R.; Thalith, N.F.A.; Loong, T.Y.; Leong, C.F. Naturally Occurring ‘enzyme only’ Anti-E antibody: A Rare Occurrence. Bangladesh J. Med. Sci. 2019, 18, 818–819. [Google Scholar] [CrossRef]
- Harrison, J. The ‘Naturally Occurring’ Anti-E. Vox Sang. 1970, 19, 123–131. [Google Scholar] [CrossRef]
- Prathiba, R.; Frcpa, L.; Mary, F.; Dipmlt, U. The prevalence of GP Mur and anti-”Mi a “ in a tertiary hospital in Peninsula Malaysia. Malays. J. Pathol. 2002, 24, 95–98. [Google Scholar]
- Promwong, C.; Siammai, S.; Hassarin, S.; Yeela, T.; Soisangwan, P.; Roxby, D.; Buakaew, J. Frequencies and specificities of red cell alloantibodies in the Southern Thai population. Asian J. Transfus. Sci. 2013, 7, 16–20. [Google Scholar] [CrossRef]
- Che Wanik, C.F.; Nazri, M.; Noor, M.; Haslina, N.; Zulkafli, Z.; Mohamed Yusoff, S.; Bahar, R.; Ramli, M.; Iberahim, S.; Ab Rahman, W.; et al. Prevalence and specificity of red blood cell alloantibodies among patients with solid tumors in a teaching hospital in malaysia. Iran. J. Blood Cancer 2021, 13, 6–10. [Google Scholar]
- Broadberry, R.E.; Lin, M. The incidence and significance of anti-“Mia” in Taiwan. Transfusion 1994, 34, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Mak, K.; Szeto, S.; Poon, K.; Yuen, C.; Chan, N.; Liu, H.; Ng, C. First case of haemolytic disease of the newborn due to anti-Mur in Hong Kong. Clin. Lab. Haematol. 1996, 18, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Tormey, C.A.; Stack, G. Immunogenicity of blood group antigens: A mathematical model corrected for antibody evanescence with exclusion of naturally occurring and pregnancy-related antibodies. Blood 2009, 114, 4279–4282. [Google Scholar] [CrossRef]
- Guastafierro, S.; Sessa, F.; Cuomo, C.; Tirelli, A. Delayed hemolytic transfusion reaction due to anti-S antibody in patient with anti-Jk a autoantibody and multiple alloantibodies. Ann. Hematol. 2004, 83, 307–308. [Google Scholar] [CrossRef]
- Singer, S.T.; Wu, V.; Mignacca, R.; Kuypers, F.A.; Morel, P.; Vichinsky, E.P. Alloimmunization and erythrocyte autoimmunization in transfusion-dependent thalassemia patients of predominantly Asian descent. Blood 2000, 96, 3369–3373. [Google Scholar] [CrossRef]
- Ramsey, G.; Smietana, S.J. Multiple or uncommon red cell alloantibodies in women: Association with autoimmune disease. Transfusion 1995, 35, 582–586. [Google Scholar] [CrossRef]
- Bonnel, A.R.; Bunchorntavakul, C.; Reddy, K.R. Immune Dysfunction and Infections in Patients with Cirrhosis. Clin. Gastroenterol. Hepatol. 2011, 9, 727–738. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | All Patients, n (%) | Alloimmunized Patients, n (%) | |
|---|---|---|---|
| Yes (n = 24) | No (n = 417) | ||
| Age (years) * | 57.9 (±12.1) | 56.2 (12.4) | 58.01 (12.1) |
| Gender | |||
| Male | 287 (65.1) | 13 (54.2) | 274 (65.7) |
| Female | 154 (34.9) | 11 (45.8) | 143 (34.3) |
| Race | |||
| Malay | 406 (92.1) | 23 (95.8) | 383 (91.8) |
| Non-Malay | 35 (7.9) | 1 (4.2) | 34 (8.2) |
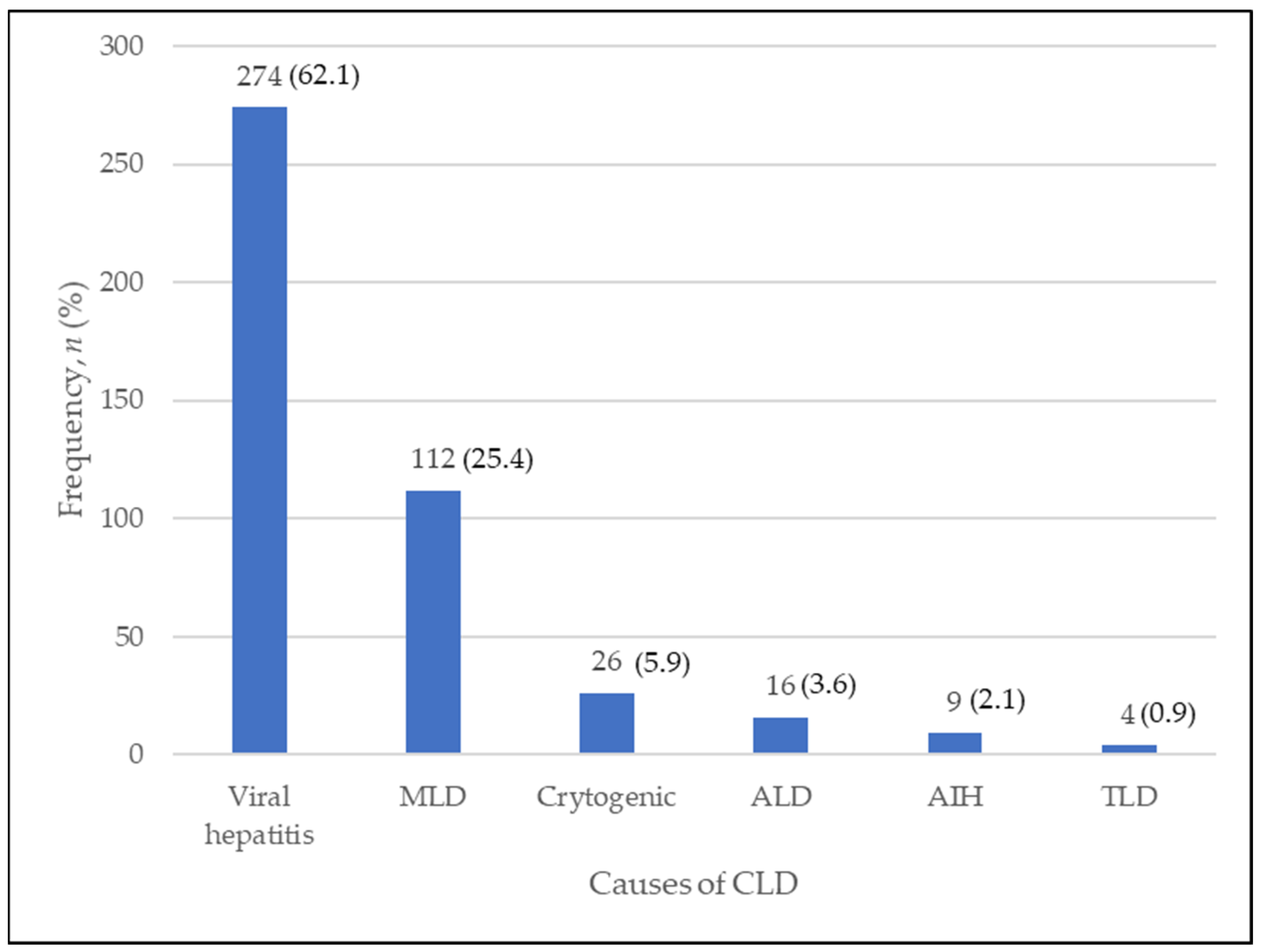
| Causes of CLD | |||
| Viral hepatitis | 274 (62.1) | 14 (58.3) | 260 (62.4) |
| MLD | 112 (25.4) | 8 (33.3) | 104 (24.9) |
| Cryptogenic | 26 (5.9) | 1 (4.2) | 25 (6.0) |
| ALD | 16 (3.6) | 0 (0) | 16 (3.8) |
| AIH | 9 (2.0) | 1 (4.2) | 8 (1.9) |
| TLD | 4 (0.9) | 0 (0) | 4 (1.0) |
| ABO group | |||
| O | 139 (31.5) | 6 (25.0) | 133 (31.9) |
| A | 124 (28.1) | 9 (37.5) | 115 (27.6) |
| B | 138 (31.3) | 8 (33.3) | 130 (31.2) |
| AB | 40 (9.1) | 1 (4.2) | 39 (9.3) |
| RhD group | |||
| +ve | 438 (99.3) | 25 (100) | 414 (99.3) |
| −ve | 3 (0.7) | 0 (0) | 3 (0.7) |
| WBC (109/L) * | 9.3 (13.8) | 6.9 (3.4) | 9.5 (14.1) |
| Hb (g/dL) * | 8.9 (2.3) | 8.5 (2.1) | 8.9 (2.3) |
| Plt (109/L) * | 130.2 (93.2) | 102.2 (89.4) | 131.8 (93.3) |
| History of tx | |||
| Yes | 242 (54.9) | 14 (58.3) | 228 (54.7) |
| No | 199 (45.1) | 10 (41.7) | 189 (45.3) |
| PRBC tx (U) *† | 2.3 (3.7) | 2.8 (4.5) | 2.3 (3.6) |
| Plt tx (U) *† | 1.5 (4.03) | 2.9 (5.9) | 1.4 (3.9) |
| Smoking (Yes/No) | |||
| Yes | 176 (39.9) | 7 (29.2) | 169 (40.5) |
| No | 265 (60.1) | 17 (70.8) | 248 (59.5) |
| Alcohol (Yes/No) | |||
| Yes | 35 (7.9) | 0 (0) | 35 (8.4) |
| No | 406 (92.1) | 24 (100) | 382 (91.6) |
| RBC Alloantibody | Frequency, n (%) | Clinical Significance |
|---|---|---|
| Number of alloantibodies | ||
| Single | 20 (83.3) | |
| Multiple (≥2) | 4 (16.7) | |
| Antibody specificity | ||
| Single alloantibody | ||
| Rhesus | 9 (37.6) | |
| Anti-E | 6 (25.0) | Yes |
| Anti-e | 1 (4.2) | Yes |
| Anti-C | 1 (4.2) | Yes |
| Anti-c | 1 (4.2) | Yes |
| MNS | 7 (29.2) | |
| Anti-M | 1 (4.2) | Rarely |
| Anti-S | 1 (4.2) | Yes |
| Anti-Mia | 5 (20.8) | Rarely |
| Lewis | 3 (12.5) | |
| Anti-Lea | 2 (8.3) | Rarely |
| Anti-Leb | 1 (4.2) | Rarely |
| No specificity | 1 (4.2) | No |
| Multiple alloantibodies | ||
| Anti-E and Anti-c | 3 (12.5) | Yes |
| Anti-E and Anti-Fyb | 1 (4.2) | Yes |
| No. | Age (Years) | Gender | Causes of CLD | ABO Group | Antibody Specificity | Transfusion | No. of PRBC/Plt Transfused (Unit) |
|---|---|---|---|---|---|---|---|
| 1 | 47 | M | NAFLD | A | Anti-E | No | 0 |
| 2 | 61 | F | Hepatitis C | A | Anti-E | No | 0 |
| 3 | 27 | M | Hepatitis C | B | Anti-E | Yes | 2 Plt |
| 4 | 73 | F | Cryptogenic | O | Anti-E | Yes | 2 PRBC |
| 5 | 66 | F | NASH | A | Anti-E | Yes | 9 PRBC, 21 Plt |
| 6 | 70 | F | NASH | B | Anti-E | Yes | 18 PRBC |
| 7 | 43 | F | NAFLD | A | Anti-c | Yes | 4 PRBC |
| 8 | 66 | M | Hepatitis B | O | Anti-C | Yes | 3 PRBC |
| 9 | 32 | M | AIH | A | Anti-e | Yes | 3 PRBC |
| 10 | 56 | F | Hepatitis B | A | Anti-E, Anti-c | Yes | 11 Plt |
| 11 | 47 | F | NAFLD | AB | Anti-E, Anti-c | Yes | 6 PRBC, 2 Plt |
| 12 | 58 | M | NAFLD | O | Anti-E, Anti-c | Yes | 12 PRBC, 16 Plt |
| 13 | 59 | M | NASH | O | Anti-E, Anti-Fyb | Yes | 2 PRBC |
| 14 | 65 | F | Hepatitis C | B | Anti-S | Yes | 12 Plt |
| 15 | 52 | M | Hepatitis C | B | Anti-M | No | 0 |
| 16 | 68 | M | Hepatitis C | A | Anti-Mia | No | 0 |
| 17 | 52 | F | Hepatitis B | A | Anti-Mia | No | 0 |
| 18 | 70 | F | Hepatitis B | O | Anti-Mia | No | 0 |
| 19 | 69 | M | NAFLD | B | Anti-Mia | No | 0 |
| 20 | 41 | M | Hepatitis C | O | Anti-Mia | Yes | 3 PRBC, 2 Plt |
| 21 | 66 | F | Hepatitis B | B | Anti-Lea | No | 0 |
| 22 | 61 | M | Hepatitis B | A | Anti-Lea | No | 0 |
| 23 | 51 | M | Hepatitis C | B | Anti-Leb | No | 0 |
| 24 | 49 | M | Hepatitis C | B | No specificity | Yes | 4 PRBC, 4 Plt |
| Independent Variables | Crude OR (95% CI) | p Value | Adjusted OR | p Value |
|---|---|---|---|---|
| Age | 0.99 (0.96, 1.02) | 0.478 | - | - |
| Gender | ||||
| F/M | 1/1.62 (0.71, 3.71) | 0.253 | - | - |
| Ethnicity | ||||
| Non-Malay/Malay | 1/2.04 (0.27, 15.59) | 0.491 | - | - |
| Causes of CLD: | ||||
| Viral Hepatitis | 1 | |||
| MLD | 0.70 (0.29, 1.72) | 0.436 | - | - |
| Cryptogenic | 1.35 (0.17, 10.67) | 0.778 | - | - |
| ALD | 0.00 (0.00, 0.00) | >0.950 | - | - |
| AIH | 0.43 (0.05, 3.69) | 0.442 | - | - |
| TLD | 0.00 (0.00, 0.00) | >0.950 | - | - |
| ABO blood group: | ||||
| O | 1 | |||
| A | 0.58 (0.20, 1.67) | 0.310 | - | - |
| B | 0.73 (0.25, 2.17) | 0.575 | - | - |
| AB | 1.76 (0.21, 15.06) | 0.606 | - | - |
| RhD Blood group: | ||||
| +ve/−ve | 1/0.00 (0.00, 0.00) | >0.950 | - | - |
| WBC (109/L) | 0.92 (0.83, 1.02) | 0.122 | 0.56 (0.21, 1.58) | 0.284 |
| Hb (g/dL) | 0.91 (0.75, 1.11) | 0.353 | - | - |
| Platelet (109/L) | 1.00 (0.99, 1.00) | 0.134 | 1.08 (0.99, 1.15) | 0.130 |
| History of tx | ||||
| No/Yes | 1/1.16 (0.50, 2.67) | 0.726 | - | - |
| No. of PRBC tx (U) * | 1.03 (0.93, 1.14) | 0.572 | - | - |
| No. of Plt tx (U) * | 1.06 (0.99, 1.13) | 0.100 | 1.07 (0.67, 1.18) | 0.103 |
| Smoking (Yes/No) | 1/1.66 (0.67, 4.08) | 0.273 | - | - |
| Alcohol consumption (No/Yes) | 1/0.00 (0.00, 0.00) | >0.950 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
S. Abdullah, S.Z.; Hassan, M.N.; Ramli, M.; Abdullah, M.; Mohd Noor, N.H. Red Blood Cell Alloimmunization and Its Associated Factors among Chronic Liver Disease Patients in a Teaching Hospital in Northeastern Malaysia. Diagnostics 2023, 13, 886. https://doi.org/10.3390/diagnostics13050886
S. Abdullah SZ, Hassan MN, Ramli M, Abdullah M, Mohd Noor NH. Red Blood Cell Alloimmunization and Its Associated Factors among Chronic Liver Disease Patients in a Teaching Hospital in Northeastern Malaysia. Diagnostics. 2023; 13(5):886. https://doi.org/10.3390/diagnostics13050886
Chicago/Turabian StyleS. Abdullah, Siti Zaleha, Mohd Nazri Hassan, Marini Ramli, Marne Abdullah, and Noor Haslina Mohd Noor. 2023. "Red Blood Cell Alloimmunization and Its Associated Factors among Chronic Liver Disease Patients in a Teaching Hospital in Northeastern Malaysia" Diagnostics 13, no. 5: 886. https://doi.org/10.3390/diagnostics13050886