
Association of Kinesiophobia with Catastrophism and Sensitization-Associated Symptoms in COVID-19 Survivors with Post-COVID Pain
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Kinesiophobia
2.4. Sensitization-Associated Symptoms
2.5. Psychological/Cognitive Variables
2.6. Health-Related Quality of Life
2.7. Sample Size Determination
2.8. Statistical Analysis
3. Results
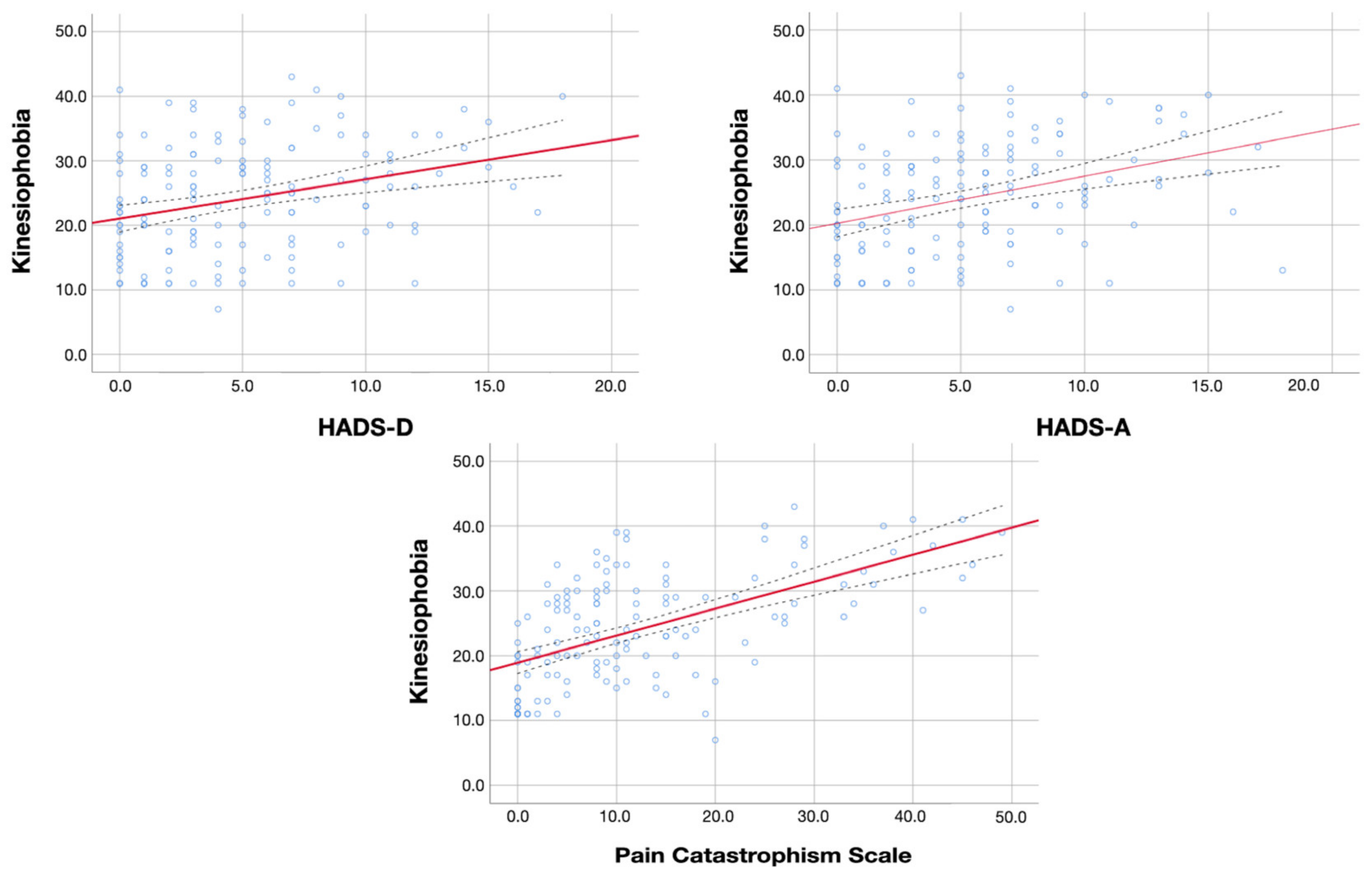
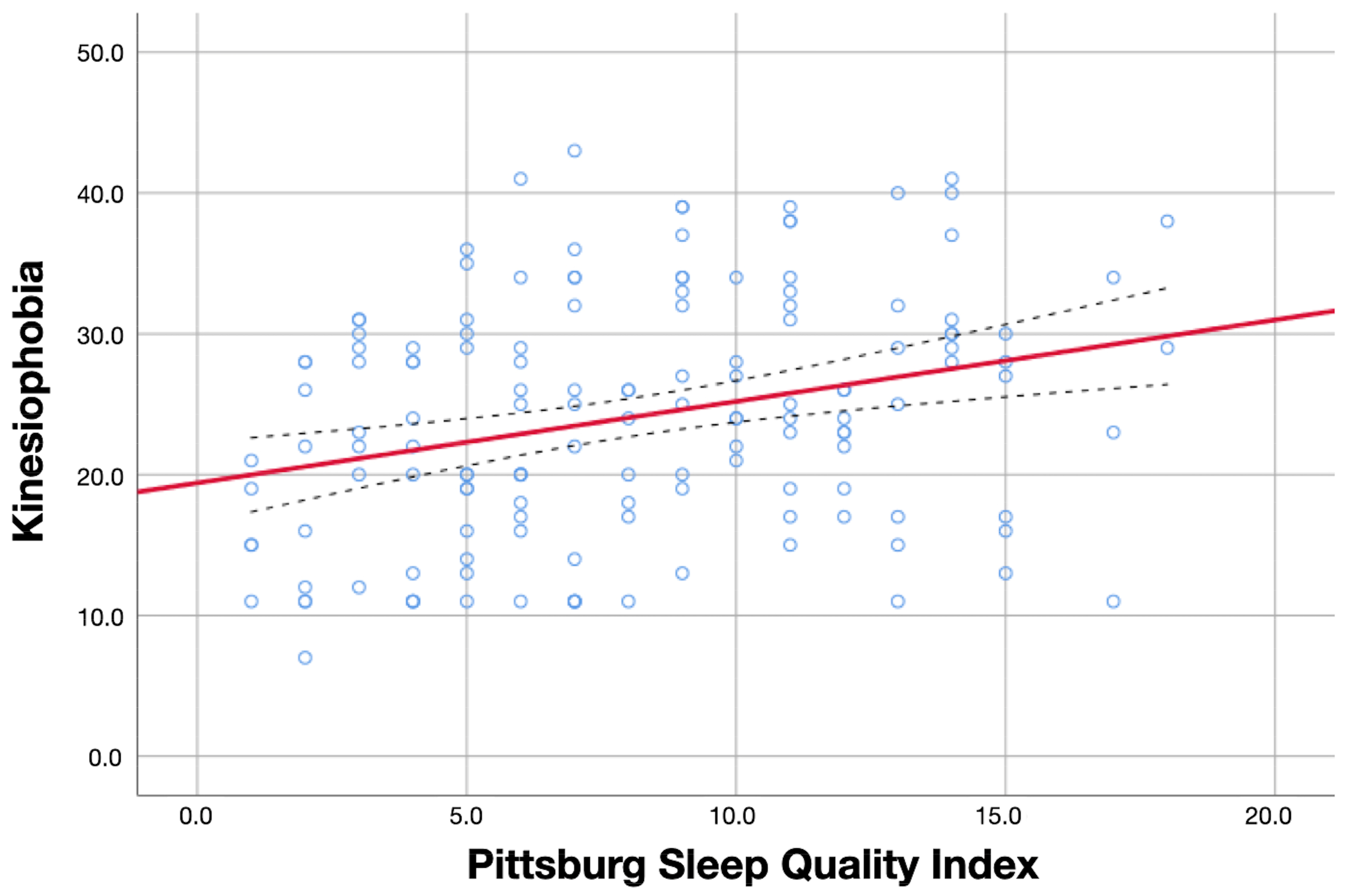
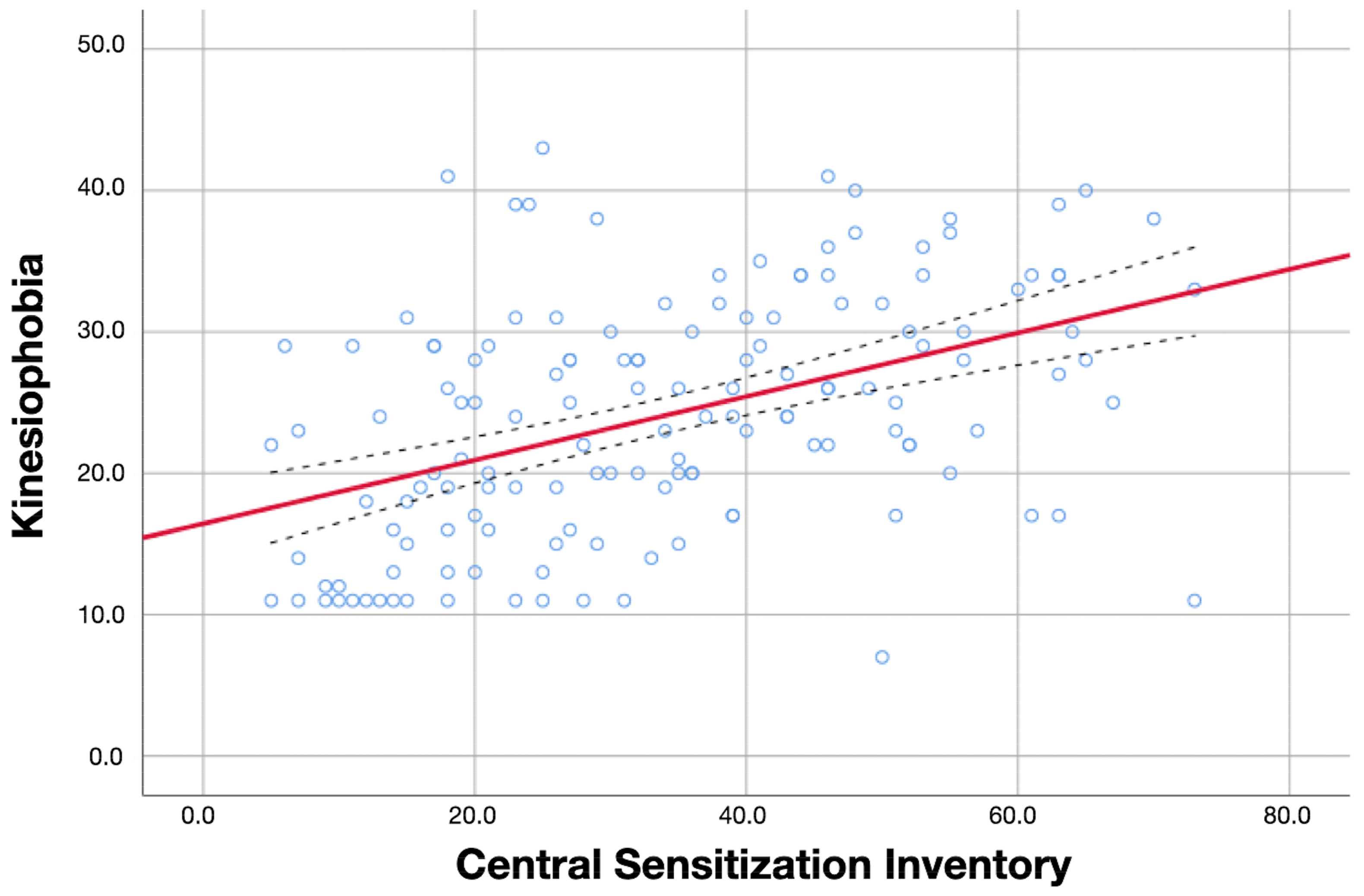
3.1. Bivariate Correlation Analyses
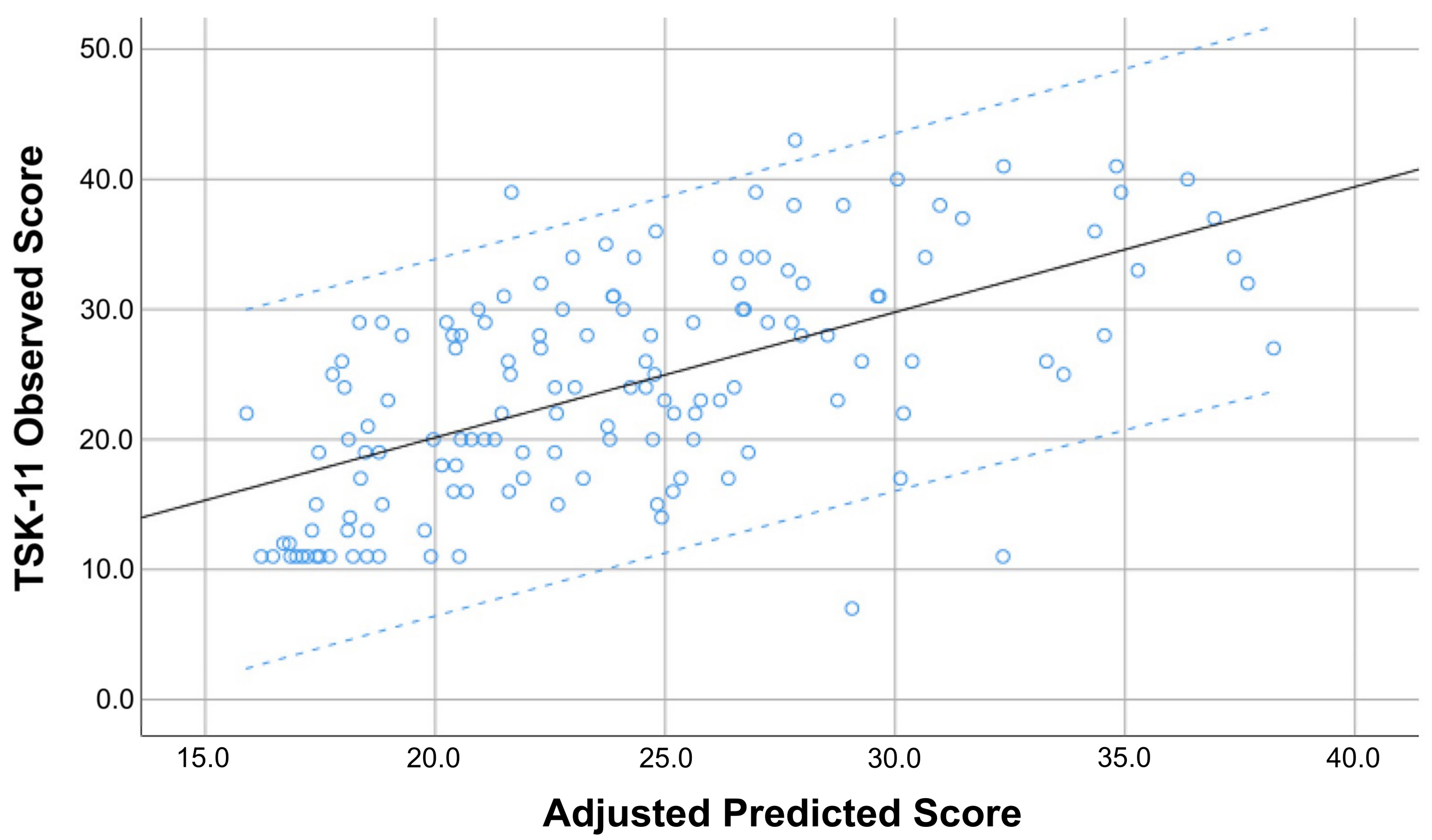
3.2. Multiple Regression Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 Long-term effects of COVID-19, a systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Inter. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global prevalence of post COVID-19 condition or long COVID: A meta-analysis and systematic review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef]
- Alkodaymi, M.S.; Omrani, O.A.; Fawzy, N.A.; Shaar, B.A.; Almamlouk, R.; Riaz, M.; Obeidat, M.; Obeidat, Y.; Gerberi, D.; Taha, R.M.; et al. Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 657–666. [Google Scholar] [CrossRef]
- Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-Term Sequelae of COVID-19, A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens 2022, 11, 269. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Yan, M.Z.; Li, X.; Lau, E.H.Y. Sequelae of COVID-19 among previously hospitalized patients up to 1 year after discharge: A systematic review and meta-analysis. Infection 2022, 50, 1067–1109. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Navarro-Santana, M.; Plaza-Manzano, G.; Palacios-Ceña Arendt-Nielsen, L. Time course prevalence of Post-COVID pain symptoms of musculoskeletal origin in patients who had survived to SARS-CoV-2 infection: A systematic review and meta-analysis. Pain 2022, 163, 1220–1231. [Google Scholar] [CrossRef] [PubMed]
- Bakılan, F.; Gökmen, İ.G.; Ortanca, B.; Uçan, A.; Eker Güvenç, Ş.; Şahin Mutlu, F.; Gökmen, H.M.; Ekim, A. Musculoskeletal symptoms and related factors in postacute COVID-19 patients. Int. J. Clin. Pract. 2021, 75, e14734. [Google Scholar] [CrossRef] [PubMed]
- Karaarslan, F.; Demircioğlu, G.F.; Kardeş, S. Postdischarge rheumatic and musculoskeletal symptoms following hospitalization for COVID-19, prospective follow-up by phone interviews. Rheumatol. Int. 2021, 41, 1263–1271. [Google Scholar] [CrossRef]
- Soares, F.H.C.; Kubota, G.T.; Fernandes, A.M.; Hojo, B.; Couras, C.; Costa, B.V.; Lapa, J.D.D.S.; Braga, L.M.; Almeida, M.M.; Cunha, P.H.M.D.; et al. Prevalence and characteristics of new-onset pain in COVID-19 survivours, a controlled study. Eur. J. Pain 2021, 25, 1342–1354. [Google Scholar] [CrossRef]
- Bileviciute-Ljungar, I.; Norrefalk, J.R.; Borg, K. Pain burden in post-COVID-19 syndrome following mild COVID-19 infection. J. Clin. Med. 2022, 11, 771. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; de-la-Llave-Rincón, A.I.; Ortega-Santiago, R.; Ambite-Quesada, S.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Hernández-Barrera, V.; Martín-Guerrero, J.D.; Pellicer-Valero, O.J.; et al. Prevalence and risk factors of musculoskeletal pain symptoms as long-term post-COVID sequelae in hospitalized COVID-19 survivors: A multicenter study. Pain 2022, 163, e989–e996. [Google Scholar] [CrossRef] [PubMed]
- Oguz-Akarsu, E.; Gullu, G.; Kilic, E.; Dinç, Y.; Ursavas, A.; Yilmaz, E.; Zarifoglu, M.; Karli, N.; Pandemic Study Team. Insight into pain syndromes in acute phase of mild-to-moderate COVID-19, Frequency, clinical characteristics, and associated factors. Eur. J. Pain 2022, 26, 492–504. [Google Scholar] [CrossRef] [PubMed]
- Ursini, F.; Ciaffi, J.; Mancarella, L.; Lisi, L.; Brusi, V.; Cavallari, C.; D’Onghia, M.; Mari, A.; Borlandelli, E.; Faranda Cordella, J.; et al. Fibromyalgia: A new facet of the post-COVID-19 syndrome spectrum? Results from a web-based survey. RMD Open 2021, 7, e001735. [Google Scholar] [CrossRef]
- Goudman, L.; De Smedt, A.; Roggeman, S.; Fernández-de-las-Peñas, C.; Hatem, S.M.; Schiltz, M.; Billot, M.; Roulaud, M.; Rigoard, P.; Moens, M. Association between experimental pain measurements and the central sensitization inventory in patients at least 3 months after COVID-19 infection: A cross-sectional pilot study. J. Clin. Med. 2023, 12, 661. [Google Scholar] [CrossRef]
- Kroska, E.B. A meta-analysis of fear-avoidance and pain intensity: The paradox of chronic pain. Scand. J. Pain 2016, 13, 43–58. [Google Scholar] [CrossRef]
- Luque-Suarez, A.; Martinez-Calderon, J.; Falla, D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: A systematic review. Br. J. Sport. Med. 2019, 53, 554–559. [Google Scholar] [CrossRef] [Green Version]
- Ucero-Lozano, R.; López-Pina, J.A.; Ortiz-Pérez, A.; Cuesta-Barriuso, R. The relationship between chronic pain and psychosocial aspects in patients with haemophilic arthropathy. A cross-sectional study. Haemophilia 2022, 28, 176–182. [Google Scholar] [CrossRef]
- Priore, L.B.; Azevedo, F.M.; Pazzinatto, M.F.; Ferreira, A.S.; Hart, H.F.; Barton, C.; de Oliveira Silva, D. Influence of kinesiophobia and pain catastrophism on objective function in women with patellofemoral pain. Phys. Ther. Sport. 2019, 35, 116–121. [Google Scholar] [CrossRef]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 4, CD011279. [Google Scholar]
- Sluka, K.A.; O’Donnell, J.M.; Danielson, J.; Rasmussen, L.A. Regular physical activity prevents development of chronic pain and activation of central neurons. J. Appl. Physiol. 2013, 114, 725–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattadori, G.; Di Marco, S.; Baravelli, M.; Picozzi, A.; Ambrosio, G. Exercise training in post-COVID-19 patients: The Need for a multifactorial protocol for a multifactorial pathophysiology. J. Clin. Med. 2022, 11, 2228. [Google Scholar] [CrossRef] [PubMed]
- Taulaniemi, A.; Kankaanpää, M.; Rinne, M.; Tokola, K.; Parkkari, J.; Suni, J.H. Fear-avoidance beliefs are associated with exercise adherence: Secondary analysis of a randomised controlled trial (RCT) among female healthcare workers with recurrent low back pain. BMC Sport. Sci. Med. Rehabil. 2020, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Roelofs, J.; van Breukelen, G.; Sluiter, J.; Frings-Dresen, M.H.; Goossens, M.; Thibault, P.; Boersma, K.; Vlaeyen, J.W. Norming of the tampa scale for kinesiophobia across pain diagnoses and various countries. Pain 2011, 152, 1090–1095. [Google Scholar] [CrossRef] [PubMed]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: A study in 48440 adult patients. Br. J. Sport. Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef]
- Burtscher, J.; Burtscher, M.; Millet, G.P. (Indoor) isolation, stress, and physical inactivity: Vicious circles accelerated by COVID-19? Scand. J. Med. Sci. Sport. 2020, 30, 1544–1545. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [Green Version]
- Perrot, S.; Cohen, M.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.D.; IASP Taskforce for the Classification of Chronic Pain. The IASP classification of chronic pain for ICD-11, chronic secondary musculoskeletal pain. Pain 2019, 160, 77–82. [Google Scholar] [CrossRef]
- Woby, S.R.; Roach, N.K.; Urmston, M.; Watson, P.J. Psychometric properties of the TSK-11, a shortened version of the Tampa Scale for Kinesiophobia. Pain 2005, 117, 137–144. [Google Scholar] [CrossRef]
- Nicholas, M.K.; Asghari, A.; Blyth, F.M. What do the numbers mean? Normative data in chronic pain measures. Pain 2008, 134, 158–173. [Google Scholar] [CrossRef]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012, 12, 276–285. [Google Scholar] [CrossRef] [Green Version]
- Neblett, R.; Cohen, H.; Choi, Y.; Hartzell, M.M.; Williams, M.; Mayer, T.G.; Gatchel, R.J. The Central Sensitization Inventory (CSI): Establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J. Pain 2013, 14, 438–445. [Google Scholar] [CrossRef] [Green Version]
- Scerbo, T.; Colasurdo, J.; Dunn, S.; Unger, J.; Nijs, J.; Cook, C. Measurement properties of the central sensitization inventory: A systematic review. Pain Pract. 2018, 18, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.I.; Neblett, R.; Chiarotto, A.; Kregel, J.; Nijs, J.; van Wilgen, C.P.; Pitance, L.; Knezevic, A.; Gatchel, R.J.; Mayer, T.G.; et al. Dimensionality and reliability of the Central Sensitization Inventory in a pooled multi-country sample. J. Pain 2018, 19, 317–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goudman, L.; De Smedt, A.; Noppen, M.; Moens, M. Is central sensitisation the missing link of persisting symptoms after COVID-19 infection? J. Clin. Med. 2021, 10, 5594. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Parás-Bravo, P.; Ferrer-Pargada, D.; Cancela-Cilleruelo, I.; Rodríguez-Jiménez, J.; Nijs, J.; Arendt-Nielsen, L.; Herrero-Montes, M. Sensitization symptoms are associated with psychological and cognitive variables in COVID-19 survivors exhibiting post-COVID pain. Pain Pract. 2023, 23, 23–31. [Google Scholar] [CrossRef]
- Herrmann-Lingen, C.; Buss, U.; Snaith, R.P. Hospital Anxiety and Depression Scale—Deutsche Version (HADS-D); Verlag Hans Huber: Bern, Switzerland, 2011. [Google Scholar] [CrossRef]
- Grupo de Trabajo de la Guía de Práctica Clínica para el Manejo de Pacientes con Trastornos de Ansiedad en Atención Primaria. Guías de Práctica Clínica en el SNS—UETS Nº 2006/10. Madrid: Plan Nacional para el SNS del MSC; Unidad de Evaluación de Tecnologías Sanitarias, Agencia Laín Entralgo, Comunidad de Madrid: Madrid, Spain, 2008. [Google Scholar]
- Fernández-de-Las-Peñas, C.; Rodríguez-Jiménez, J.; Palacios-Ceña, M.; de-la-Llave-Rincón, A.I.; Fuensalida-Novo, S.; Florencio, L.L.; Ambite-Quesada, S.; Ortega-Santiago, R.; Arias-Buría, J.L.; Liew, B.X.W.; et al. Psychometric Properties of the Hospital Anxiety and Depression Scale (HADS) in Previously Hospitalized COVID-19 Patients. Int. J. Environ. Res. Public Health 2022, 19, 9273. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Van Hout, B.; Janssen, M.F.; Feng, Y.J.; Kohlmann, T.; Busschbach, J.; Golicki, D.; Lloyd, A.; Scalone, L.; Kind, P.; Pickard, A.S. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health 2012, 15, 708–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-de-las-Peñas, C.; Rodríguez-Jiménez, J.; Moro-López-Menchero, P.; Cancela-Cilleruelo, I.; Pardo-Hernández, A.; Hernández-Barrera, V.; Gil-de-Miguel, Á. Psychometric properties of the Spanish version of the EuroQol-5D-5L in previously hospitalized COVID-19 survivors with long COVID. Sci. Rep. 2022, 12, 12605. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Steyerberg, E.W. The number of subjects per variable required in linear regression analyses. J. Clin. Epidemiol. 2015, 68, 627–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, D.G.; Quintana-Ascencio, P.F. A solution to minimum sample size for regressions. PLoS ONE 2020, 15, e0229345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundberg, M.; Larsson, M.; Östlund, H.; Styf, J. Kinesiophobia among patients with musculoskeletal pain in primary healthcare. J. Rehabil. Med. 2006, 38, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Vlaeyen, J.W.; Linton, S.J. Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain 2012, 153, 1144–1147. [Google Scholar] [CrossRef]
- Quartana, P.J.; Campbell, C.M.; Edwards, R.R. Pain catastrophizing: A critical review. Expert Rev. Neurother. 2009, 9, 745–758. [Google Scholar] [CrossRef]
- Rogers, A.H.; Farris, S.G. A Meta-analysis of the associations of elements of the Fear-Avoidance Model of chronic pain with negative affect, depression, anxiety, pain-related disability and pain intensity. Eur. J. Pain 2022, 26, 1611–1635. [Google Scholar] [CrossRef]
- Sullivan, M.; Tanzer, M.; Stanish, W.; Fallaha, M.; Keefe, F.J.; Simmonds, M.; Dunbar, M. Psychological determinants of problematic outcomes following total knee arthroplasty. Pain 2009, 143, 123–129. [Google Scholar] [CrossRef]
- Cotchett, M.; Lennecke, A.; Medica, V.G.; Whittaker, G.A.; Bonanno, D.R. The association between pain catastrophising and kinesiophobia with pain and function in people with plantar heel pain. Foot 2017, 32, 8–14. [Google Scholar] [CrossRef]
- Giusti, E.M.; Lacerenza, M.; Manzoni, G.M.; Castelnuovo, G. Psychological and psychosocial predictors of chronic postsurgical pain: A systematic review and meta-analysis. Pain 2021, 162, 10–30. [Google Scholar] [CrossRef]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central sensitisation in chronic pain conditions: Latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- van Wilgen, C.P.; Vuijk, P.J.; Kregel, J.; Voogt, L.; Meeus, M.; Descheemaeker, F.; Keizer, D.; Nijs, J. Psychological distress and widespread pain contribute to the variance of the Central Sensitization Inventory: A cross-sectional study in patients with chronic pain. Pain Pract. 2018, 18, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Adams, G.R.; Gandhi, W.; Harrison, R.; van Reekum, C.M.; Gilron, I.; Salomons, T.V. Do “central sensitization” questionnaires reflect measures of nociceptive sensitization or psychological constructs? Protocol for a systematic review. Pain Rep. 2021, 6, e962. [Google Scholar] [PubMed]
- Fernández-de-las-Peñas, C.; Nijs, J.; Neblett, R.; Polli, A.; Moens, M.; Goudman, L.; Shekhar Patil, M.; Knaggs, R.D.; Pickering, G.; Arendt-Nielsen, L. Phenotyping Post-COVID Pain as a Nociceptive, Neuropathic, or Nociplastic Pain Condition. Biomedicines 2022, 10, 2562. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Xu, Y.; Xuan, R.; Baker, J.S.; Gu, Y.A. Mixed comparison of interventions for kinesiophobia in individuals with musculoskeletal pain: Systematic review and network meta-analysis. Front. Psychol. 2022, 13, 886015. [Google Scholar] [CrossRef]
- Kamonseki, D.H.; Christenson, P.; Rezvanifar, S.C.; Calixtre, L.B. Effects of manual therapy on fear avoidance, kinesiophobia and pain catastrophizing in individuals with chronic musculoskeletal pain: Systematic review and meta-analysis. Musculoskelet. Sci. Pract. 2021, 51, 102311. [Google Scholar] [CrossRef]
- Ram, A.; Booth, J.; Thom, J.M.; Gibbs, M.T.; Jones, M.D. Are improvements in pain neurophysiology knowledge following pain science education associated with improved outcomes in people with chronic pain? A systematic review and meta-analysis. Clin. J. Pain 2023, 39, 41–52. [Google Scholar] [CrossRef]
- Jimeno-Almazán, A.; Pallarés, J.G.; Buendía-Romero, Á.; Martínez-Cava, A.; Franco-López, F.; Sánchez-Alcaraz Martínez, B.J.; Bernal-Morel, E.; Courel-Ibáñez, J. Post-COVID-19 syndrome and the potential benefits of exercise. Int. J. Environ. Res. Public Health 2021, 18, 5329. [Google Scholar] [CrossRef]
- Ojeda, A.; Calvo, A.; Cuñat, T.; Mellado-Artigas, R.; Comino-Trinidad, O.; Aliaga, J.; Arias, M.; Ferrando, C.; Martinez-Pallí, G.; Dürsteler, C. Characteristics and influence on quality of life of new-onset pain in critical COVID-19 survivors. Eur. J. Pain 2022, 26, 680–694. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | Sample (n = 146) | Males (n = 67) | Females (n = 78) | Between-Gender Differences |
|---|---|---|---|---|
| Demographic Characteristics | ||||
| Age (years) | 57.5 ± 11.8 | 60.0 ± 10.3 | 55.2 ± 12.5 | 4.8 (1.03; 8.65) p = 0.013 |
| Height (m) | 1.67 ± 0.09 | 1.73 ± 0.08 | 1.61 ± 0.06 | 0.11 (0.08; 0.13) p < 0.001 |
| Weight (kg) | 81.8 ± 17.1 | 86.5 ± 15.6 | 77.8 ± 17.4 | 8.7 (3.3; 14.2) p = 0.002 |
| Clinical Characteristics | ||||
| Post-COVID symptoms (months) | 18.8 ± 1.8 | 18.7 ± 2.0 | 18.9 ± 1.7 | 0.2 (−0.4; 0.8) p = 0.489 |
| Pain-Related Features | ||||
| Pain intensity (0 to 10) | 5.59 ± 1.72 | 5.23 ± 1.85 | 5.92 ± 1.54 | 0.69 (0.13; 1.25) p = 0.016 |
| CSI (0 to 100) | 33.91 ± 17.25 | 25.92 ± 14.33 | 41.06 ± 16.46 | 15.13 (10.02; 20.24) p < 0.001 |
| Quality of Life | ||||
| EuroQol-5D-5L Questionnaire (0 to 100) | 0.77 ± 0.20 | 0.79 ± 0.22 | 0.76 ± 0.17 | 0.02 (−0.03; 0.09) p = 0.427 |
| Pittsburgh Sleeping Quality Index (0 to 21) | 8.07 ± 4.28 | 6.86 ± 4.42 | 9.11 ± 3.91 | 2.24 (0.88; 3.61) p = 0.001 |
| Psychological Characteristics | ||||
| HADS-A (0 to 21) | 5.28 ± 4.21 | 4.44 ± 4.04 | 6.07 ± 4.22 | 1.62 (−0.26; 2.99) p = 0.020 |
| HADS-D (0 to 21) | 5.07 ± 4.29 | 4.38 ± 4.28 | 5.60 ± 4.27 | 1.21 (−0.19; 2.62) p = 0.091 |
| Pain Catastrophizing Scale (0 to 52) | 12.14 ± 11.95 | 10.27 ± 11.30 | 13.80 ± 12.40 | 3.52 (−0.43; 7.48) p = 0.080 |
| Tampa Scale for Kinesiophobia (0 to 44) | 24.11 ± 8.56 | 22.59 ± 8.74 | 25.47 ± 8.25 | 2.88 (0.07; 5.68) p = 0.044 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | ||||||||||||
| 2. Gender | −0.206 * | |||||||||||
| 3. Height | 0.003 | −0.595 ** | ||||||||||
| 4. Weight | −0.090 | −0.256 ** | 0.509 ** | |||||||||
| 5. Post-COVID symptoms | −0.122 | 0.058 | 0.010 | 0.127 | ||||||||
| 6. Pain intensity | −0.047 | 0.200 * | −0.191 * | −0.109 | 0.016 | |||||||
| 7. HADS-A | 0.028 | 0.194 * | −0.158 | −0.090 | −0.271 ** | 0.175 * | ||||||
| 8. HADS-D | 0.078 | 0.141 | −0.104 | −0.091 | −0.136 | 0.225 ** | 0.750 ** | |||||
| 9. PSQI | 0.121 | 0.262 ** | −0.213 ** | −0.102 | −0.189 * | 0.137 | 0.316 ** | 0.354 ** | ||||
| 10. CSI | −0.076 | 0.440 ** | −0.285 ** | −0.121 | −0.158 | 0.190 * | 0.551 ** | 0.446 ** | 0.390 ** | |||
| 11. PCS | 0.132 | 0.147 | −0.128 | −0.083 | −0.343 ** | 0.045 | 0.492 ** | 0.483 ** | 0.282 ** | 0.402 ** | ||
| 12. TSK-11 | 0.000 | 0.168 * | −0.065 | 0.034 | −0.092 | 0.150 | 0.356 ** | 0.306 ** | 0.288 ** | 0.450 ** | 0.578 ** | |
| 13. EuroQol-5D-5L | −0.039 | −0.066 | 0.004 | 0.051 | 0.081 | −0.006 | −0.143 | −0.174 * | −0.301 ** | −0.199 * | −0.210 * | −0.132 |
| Predictor Outcome | Β | SE B | 95% CI | B | t | p Value | |
|---|---|---|---|---|---|---|---|
| TSK-11 | Step 1 | ||||||
| Catastrophism | 0.416 | 0.050 | 0.318; 00.515 | 0.578 | 80.377 | <0.001 | |
| Step 2 | |||||||
| Catastrophism | 0.343 | 0.052 | 0.240; 00.445 | 0.475 | 60.593 | <0.001 | |
| Central Sensitization Inventory | 0.130 | 0.036 | 0.058; 00.201 | 0.259 | 30.585 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrero-Montes, M.; Fernández-de-las-Peñas, C.; Ferrer-Pargada, D.; Izquierdo-Cuervo, S.; Abascal-Bolado, B.; Valera-Calero, J.A.; Paras-Bravo, P. Association of Kinesiophobia with Catastrophism and Sensitization-Associated Symptoms in COVID-19 Survivors with Post-COVID Pain. Diagnostics 2023, 13, 847. https://doi.org/10.3390/diagnostics13050847
Herrero-Montes M, Fernández-de-las-Peñas C, Ferrer-Pargada D, Izquierdo-Cuervo S, Abascal-Bolado B, Valera-Calero JA, Paras-Bravo P. Association of Kinesiophobia with Catastrophism and Sensitization-Associated Symptoms in COVID-19 Survivors with Post-COVID Pain. Diagnostics. 2023; 13(5):847. https://doi.org/10.3390/diagnostics13050847
Chicago/Turabian StyleHerrero-Montes, Manuel, César Fernández-de-las-Peñas, Diego Ferrer-Pargada, Sheila Izquierdo-Cuervo, Beatriz Abascal-Bolado, Juan Antonio Valera-Calero, and Paula Paras-Bravo. 2023. "Association of Kinesiophobia with Catastrophism and Sensitization-Associated Symptoms in COVID-19 Survivors with Post-COVID Pain" Diagnostics 13, no. 5: 847. https://doi.org/10.3390/diagnostics13050847