
A Sequalae of Lineage Divergence in Staphylococcus aureus from Community-Acquired Patterns in Youth to Hospital-Associated Profiles in Seniors Implied Age-Specific Host-Selection from a Common Ancestor
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Microbiological Diagnosis, Antimicrobial Susceptibility Testing, and Patients’ Demographics
2.2. Resistance Classifications of MRSA Lineages Based on Standard Definitions for Classification: As Multi-Drug Resistant Bacteria (MDR)
- MDR
- = non-susceptibility to at least one agent in three or more antimicrobial categories;
- XDR
- = non-susceptibility to at least one agent in all but two or fewer antimicrobial categories (i.e., bacterial isolates remain susceptible to only one or two categories);
- PDR
- = non-susceptibility to all agents in all antimicrobial categories as reported.
2.3. Molecular Detection and Characterization of S. aureus Lineages by Multi-Gene GeneXpert System
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gordon, R.J.; Lowy, F.D. Pathogenesis of Methicillin-Resistant Staphylococcus aureus Infection. Clin. Infect. Dis. 2008, 46 (Suppl. S5), S350–S359. [Google Scholar] [CrossRef] [Green Version]
- Klevens, R.M.; Morrison, M.A.; Nadle, J.; Petit, S.; Gershman, K.; Ray, S.; Harrison, L.H.; Lynfield, R.; Dumyati, G.; Townes, J.M.; et al. Invasive Methicillin-Resistant Staphylococcus aureus Infections in the United States. JAMA 2007, 298, 1763–1771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasigade, J.P.; Dumitrescu, O.; Lina, G. New Epidemiology of Staphylococcus aureus Infections. Clin. Microbiol. Infect. 2014, 20, 587–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, S.Y.C.; Davis, J.S.; Eichenberger, E.; Holland, T.L.; Fowler, V.G. Staphylococcus aureus Infections: Epidemiology, Pathophysiology, Clinical Manifestations, and Management. Clin. Microbiol. Rev. 2015, 28, 603. [Google Scholar] [CrossRef] [Green Version]
- Lowy, F.D. Staphylococcus aureus Infections. N. Engl. J. Med. 1998, 339, 520–532. [Google Scholar] [CrossRef]
- Udo, E.E. Community-Acquired Methicillin-Resistant Staphylococcus aureus: The New Face of an Old Foe? Med. Princ. Pract. 2013, 22 (Suppl. 1), 20–29. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.A.; Sharma-Kuinkel, B.K.; Maskarinec, S.A.; Eichenberger, E.M.; Shah, P.P.; Carugati, M.; Holland, T.L.; Fowler, V.G. Methicillin-Resistant Staphylococcus aureus: An Overview of Basic and Clinical Research. Nat. Rev. Microbiol. 2019, 17, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Balkhy, H.H.; Assiri, A.M.; Mousa, H.; Al-Abri, S.S.; Al-Katheeri, H.; Alansari, H.; Abdulrazzaq, N.M.; Aidara-Kane, A.; Pittet, D.; Erlacher-Vindel, E.; et al. The Strategic Plan for Combating Antimicrobial Resistance in Gulf Cooperation Council States. J. Infect. Public Health 2016, 9, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Balkhy, H.H.; Zowawi, H.M.; Alshamrani, M.M.; Allegranzi, B.; Srinivasan, A.; Al-Abdely, H.M.; Somily, A.M.; Al-Quwaizani, M.A.; Al-Maani, A.S.; Al-Abdely, H.M.; et al. Antimicrobial Resistance: A Round Table Discussion on the “One Health” Concept from the Gulf Cooperation Council Countries. Part Two: A Focus on Human Health. J. Infect. Public Health 2018, 11, 778–783. [Google Scholar] [CrossRef]
- Al-Saleh, A.; Shahid, M.; Farid, E.; Bindayna, K. Trends in Methicillin-Resistant Staphylococcus aureus in the Gulf Cooperation Council Countries: Antibiotic Resistance, Virulence Factors and Emerging Strains. East Mediterr. Health J. 2022, 28, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Vali, L.; Dashti, A.A.; Mathew, F.; Udo, E.E. Characterization of Heterogeneous MRSA and MSSA with Reduced Susceptibility to Chlorhexidine in Kuwaiti Hospitals. Front. Microbiol. 2017, 8, 1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfouzan, W.; Udo, E.E.; Modhaffer, A.; Alosaimi, A. Molecular Characterization of Methicillin- Resistant Staphylococcus aureus in a Tertiary Care Hospital in Kuwait. Sci. Rep. 2019, 9, 18527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senok, A.; Nassar, R.; Celiloglu, H.; Nabi, A.; Alfaresi, M.; Weber, S.; Rizvi, I.; Müller, E.; Reissig, A.; Gawlik, D.; et al. Genotyping of Methicillin Resistant Staphylococcus aureus from the United Arab Emirates. Sci. Rep. 2020, 10, 18551. [Google Scholar] [CrossRef]
- Al Jalaf, M.; Fadali, H.; Alanee, R.; Najjar, F.; al Deesi, Z.; Seliem, R.M.; Nilles, E.J. Methicillin Resistant Staphylococcus aureus in Emergency Department Patients in the United Arab Emirates. BMC Emerg. Med. 2018, 18, 12. [Google Scholar] [CrossRef] [PubMed]
- Al Rahmany, D.; Albeloushi, A.; Alreesi, I.; Alzaabi, A.; Alreesi, M.; Pontiggia, L.; Ghazi, I.M. Exploring Bacterial Resistance in Northern Oman, a Foundation for Implementing Evidence-Based Antimicrobial Stewardship Program. Int. J. Infect Dis. 2019, 83, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Udo, E.E.; Boswihi, S.S. Antibiotic Resistance Trends in Methicillin-Resistant Staphylococcus aureus Isolated in Kuwait Hospitals: 2011-2015. Med. Princ. Pract. 2017, 26, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Eed, E.M.; Ghonaim, M.M.; Hussein, Y.M.; Saber, T.M.; Khalifa, A.S. Phenotypic and Molecular Characterization of HA-MRSA in Taif Hospitals, Saudi Arabia. J. Infect Dev. Ctries. 2015, 9, 298–303. [Google Scholar] [CrossRef] [Green Version]
- Monecke, S.; Skakni, L.; Hasan, R.; Ruppelt, A.; Ghazal, S.S.; Hakawi, A.; Slickers, P.; Ehricht, R. Characterisation of MRSA Strains Isolated from Patients in a Hospital in Riyadh, Kingdom of Saudi Arabia. BMC Microbiol. 2012, 12, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkharsah, K.R.; Rehman, S.; Alkhamis, F.; Alnimr, A.; Diab, A.; Al-Ali, A.K. Comparative and Molecular Analysis of MRSA Isolates from Infection Sites and Carrier Colonization Sites. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonnevend, Á.; Blair, I.; Alkaabi, M.; Jumaa, P.; Haj, M.; Ghazawi, A.; Akawi, N.; Jouhar, F.S.; Hamadeh, M.B.; Pál, T. Change in Meticillin-Resistant Staphylococcus aureus Clones at a Tertiary Care Hospital in the United Arab Emirates over a 5-Year Period. J. Clin. Pathol. 2012, 65, 178–182. [Google Scholar] [CrossRef]
- Senok, A.; Somily, A.M.; Nassar, R.; Garaween, G.; Sing, G.K.; Müller, E.; Reissig, A.; Gawlik, D.; Ehricht, R.; Monecke, S. Emergence of Novel Methicillin-Resistant Staphylococcus aureus Strains in a Tertiary Care Facility in Riyadh, Saudi Arabia. Infect. Drug Resist. 2019, 12, 2739–2746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, A.G.; Hwan, K.K.; Burts, M.L.; Krausz, T.; Schneewind, O.; Missiakas, D.M. Genetic Requirements for Staphylococcus aureus Abscess Formation and Persistence in Host Tissues. FASEB J. 2009, 23, 3393–3404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, A.G.; DeDent, A.C.; Schneewind, O.; Missiakas, D. A Play in Four Acts: Staphylococcus aureus Abscess Formation. Trends Microbiol. 2011, 19, 225–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boswihi, S.S.; Udo, E.E.; Monecke, S.; Mathew, B.; Noronha, B.; Verghese, T.; Tappa, S.B. Emerging Variants of Methicillin-Resistant Staphylococcus aureus Genotypes in Kuwait Hospitals. PLoS ONE 2018, 13, e0195933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollitt, E.J.G.; Szkuta, P.T.; Burns, N.; Foster, S.J. Staphylococcus aureus Infection Dynamics. PLoS Pathog. 2018, 14, e1007112. [Google Scholar] [CrossRef] [Green Version]
- Surewaard, B.G.J.; Deniset, J.F.; Zemp, F.J.; Amrein, M.; Otto, M.; Conly, J.; Omri, A.; Yates, R.M.; Kubes, P. Identification and Treatment of the Staphylococcus aureus Reservoir in Vivo. J. Exp. Med. 2016, 213, 1141–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jong, N.W.M.; van Kessel, K.P.M.; van Strijp, J.A.G. Immune Evasion by Staphylococcus aureus. Microbiol. Spectr. 2019, 7, 20. [Google Scholar] [CrossRef]
- Foster, T.J. The MSCRAMM Family of Cell-Wall-Anchored Surface Proteins of Gram-Positive Cocci. Trends Microbiol. 2019, 27, 927–941. [Google Scholar] [CrossRef]
- Rogers, D.E. Studies on bacteriemia i. mechanisms relating to the persistence of bacteriemia in rabbits following the intravenous injection of staphylococci. J. Exp. Med. 1956, 103, 713–742. [Google Scholar] [CrossRef] [Green Version]
- Gresham, H.D.; Lowrance, J.H.; Caver, T.E.; Wilson, B.S.; Cheung, A.L.; Lindberg, F.P. Survival of Staphylococcus aureus inside Neutrophils Contributes to Infection. J. Immunol. 2000, 164, 3713–3722. [Google Scholar] [CrossRef] [Green Version]
- Kubica, M.; Guzik, K.; Koziel, J.; Zarebski, M.; Richter, W.; Gajkowska, B.; Golda, A.; Maciag-Gudowska, A.; Brix, K.; Shaw, L.; et al. A Potential New Pathway for Staphylococcus aureus Dissemination: The Silent Survival of S. aureus Phagocytosed by Human Monocyte-Derived Macrophages. PLoS ONE 2008, 3, e1490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kale, P.; Dhawan, B. The Changing Face of Community-Acquired Methicillin-Resistant Staphylococcus aureus. Indian J. Med. Microbiol. 2016, 34, 275–285. [Google Scholar] [CrossRef]
- Boucher, H.W.; Corey, G.R. Epidemiology of Methicillin-Resistant Staphylococcus aureus. Clin. Infect. Dis. 2008, 46 (Suppl. 5), S344–S349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuehnert, M.J.; Hill, H.A.; Kupronis, B.A.; Tokars, J.I.; Solomon, S.L.; Jernigan, D.B. Methicillin-Resistant–Staphylococcus aureus Hospitalizations, United States. Emerg. Infect. Dis. 2005, 11, 868. [Google Scholar] [CrossRef]
- Gerberding, J.L.; Director, M.; Cohen, M.; Valdiserri, P.O.R.; Acting Director, M.; Janssen, R.S.; Centers for Disease Control and Prevention. FastStats—Viral Hepatitis. Available online: https://www.cdc.gov/nchs/fastats/hepatitis.htm (accessed on 19 March 2022).
- Table 1|Reported TB in the US 2020| Data & Statistics |TB| CDC. Available online: https://www.cdc.gov/tb/statistics/reports/2020/table1.htm (accessed on 19 March 2022).
- Kourtis, A.P.; Hatfield, K.; Baggs, J.; Mu, Y.; See, I.; Epson, E.; Nadle, J.; Kainer, M.A.; Dumyati, G.; Petit, S.; et al. Vital Signs: Epidemiology and Recent Trends in Methicillin-Resistant and in Methicillin-Susceptible Staphylococcus aureus Bloodstream Infections—United States. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 214–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Yin, Y.; van Dorp, L.; Shaw, L.P.; Gao, H.; Acman, M.; Yuan, J.; Chen, F.; Sun, S.; Wang, X.; et al. Drivers of Methicillin-Resistant Staphylococcus aureus (MRSA) Lineage Replacement in China. Genome Med. 2021, 13, 171. [Google Scholar] [CrossRef]
- Mohamad Farook, N.A.; Argimón, S.; Abdul Samat, M.N.; Salleh, S.A.; Sulaiman, S.; Tan, T.L.; Periyasamy, P.; Lau, C.L.; Ismail, Z.; Muhammad Azami, N.A.; et al. Diversity and Dissemination of Methicillin-Resistant Staphylococcus aureus (MRSA) Genotypes in Southeast Asia. Trop. Med. Infect Dis. 2022, 7, 438. [Google Scholar] [CrossRef]
- Lawal, O.U.; Ayobami, O.; Abouelfetouh, A.; Mourabit, N.; Kaba, M.; Egyir, B.; Abdulgader, S.M.; Shittu, A.O. A 6-Year Update on the Diversity of Methicillin-Resistant Staphylococcus aureus Clones in Africa: A Systematic Review. Front. Microbiol. 2022, 13, 860436. [Google Scholar] [CrossRef]
- See, I.; Mu, Y.; Albrecht, V.; Karlsson, M.; Dumyati, G.; Hardy, D.J.; Koeck, M.; Lynfield, R.; Nadle, J.; Ray, S.M.; et al. Trends in Incidence of Methicillin-Resistant Staphylococcus aureus Bloodstream Infections Differ by Strain Type and Healthcare Exposure, United States, 2005-2013. Clin. Infect Dis. 2020, 70, 19–25. [Google Scholar] [CrossRef]
- Preeja, P.P.; Kumar, S.H.; Shetty, V. Prevalence and Characterization of Methicillin-Resistant Staphylococcus aureus from Community- and Hospital-Associated Infections: A Tertiary Care Center Study. Antibiotics 2021, 10, 197. [Google Scholar] [CrossRef]
- Guthrie, J.L.; Teatero, S.; Hirai, S.; Fortuna, A.; Rosen, D.; Mallo, G.V.; Campbell, J.; Pelude, L.; Golding, G.; Simor, A.E.; et al. Genomic Epidemiology of Invasive Methicillin-Resistant Staphylococcus aureus Infections Among Hospitalized Individuals in Ontario, Canada. J. Infect Dis. 2020, 222, 2071–2081. [Google Scholar] [CrossRef] [PubMed]
- Earls, M.R.; Steinig, E.J.; Monecke, S.; Samaniego Castruita, J.A.; Simbeck, A.; Schneider-Brachert, W.; Vremerǎ, T.; Dorneanu, O.S.; Loncaric, I.; Bes, M.; et al. Exploring the Evolution and Epidemiology of European CC1-MRSA-IV: Tracking a Multidrug-Resistant Community-Associated Meticillin-Resistant Staphylococcus aureus Clone. Microb Genom 2021, 7, 000601. [Google Scholar] [CrossRef] [PubMed]
- Belhout, C.; Elgroud, R.; Butaye, P. Methicillin-Resistant Staphylococcus aureus (MRSA) and Other Methicillin-Resistant Staphylococci and Mammaliicoccus (MRNaS) Associated with Animals and Food Products in Arab Countries: A Review. Vet. Sci. 2022, 9, 317. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing An Informational Supplement for Global: Application Developed through the Clinical and Laboratory Standards Institute Consensus Process, 26th ed.; Clinical and Laboratory Standards Institute (CLSI): Wayne, PV, USA, 2016. [Google Scholar]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Malachowa, N.; Deleo, F.R. Mobile Genetic Elements of Staphylococcus aureus. Cell. Mol. Life Sci. 2010, 67, 3057–3071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patil, S.S.; Suresh, K.P.; Shinduja, R.; Amachawadi, R.G.; Chandrashekar, S.; Pradeep, S.; Kollur, S.P.; Syed, A.; Sood, R.; Roy, P.; et al. Prevalence of Methicillin-Resistant Staphylococcus aureus in India: A Systematic Review and Meta-Analysis. Oman Med. J. 2022, 37, e440. [Google Scholar] [CrossRef] [PubMed]
- Tabaja, H.; Hindy, J.R.; Kanj, S.S. Epidemiology of Methicillin-Resistant Staphylococcus aureus in Arab Countries of the Middle East and North African (MENA) Region. Mediterr. J. Hematol. Infect Dis. 2021, 13, e2021050. [Google Scholar] [CrossRef]
- Al-Hamad, A.M.; Alfaraj, A.A.; Altowaileb, J.A.; Al-Shamlan, S.M.; Leskafi, H.H.; Alsubeikhy, F.A.; Abbas, H.R. Incidence and Antibiotic Susceptibility of MRSA Infections in a Saudi Arabian Hospital: A 10-Year Surveillance Study. J. Infect. Dev. Ctries 2018, 12, 454–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Zahrani, I.A.; Azhar, E.I.; Jiman-Fatani, A.A.; Siddig, L.A.; Yasir, M.; Al-Ghamdi, A.K.; Harwood, C.R. Impact of Mass Migrations on the Clonal Variation of Clinical Staphylococcus aureus Strains Isolated from the Western Region of Saudi Arabia. J. Infect Public Health 2019, 12, 317–322. [Google Scholar] [CrossRef]
- Molina, K.C.; Morrisette, T.; Miller, M.A.; Huang, V.; Fish, D.N. The Emerging Role of β-Lactams in the Treatment of Methicillin-Resistant Staphylococcus aureus Bloodstream Infections. Antimicrob. Agents Chemother. 2020, 64, e00468-20. [Google Scholar] [CrossRef]
- Shang, W.; Rao, Y.; Zheng, Y.; Yang, Y.; Hu, Q.; Hu, Z.; Yuan, J.; Peng, H.; Xiong, K.; Tan, L.; et al. β-Lactam Antibiotics Enhance the Pathogenicity of Methicillin-Resistant Staphylococcus aureus via SarA-Controlled Lipoprotein-Like Cluster Expression. mBio 2019, 10, e00880-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- el Amin, N.M.; Faidah, H.S. Methicillin-Resistant Staphylococcus aureus in the Western Region of Saudi Arabia: Prevalence and Antibiotic Susceptibility Pattern. Ann. Saudi Med. 2012, 32, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Qodrati, M.; SeyedAlinaghi, S.A.; Dehghan Manshadi, S.A.; Abdollahi, A.; Dadras, O. Antimicrobial Susceptibility Testing of Staphylococcus aureus Isolates from Patients at a Tertiary Hospital in Tehran, Iran, 2018–2019. Eur. J. Med. Res. 2022, 27, 152. [Google Scholar] [CrossRef]
- Draghi, D.C.; Sheehan, D.F.; Hogan, P.; Sahm, D.F. Current Antimicrobial Resistance Profiles among Methicillin-Resistant Staphylococcus aureus Encountered in the Outpatient Setting. Diagn. Microbiol. Infect Dis. 2006, 55, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Neela, V.; Sasikumar, M.; Ghaznavi, G.R.; Zamberi, S.; Mariana, S. In vitro activities of 28 antimicrobial agents against methicillin-resistant Staphylococcus aureus (mrsa) from a clinical setting in malaysia. Vitr. Antimicrob. Act. Against Mrsa 2008, 39, 885–892. [Google Scholar]
- Kaibni, M.H.; Farraj, M.A.; Adwan, K.; Essawi, T.A. Community-Acquired Meticillin-Resistant Staphylococcus aureus in Palestine. J. Med. Microbiol. 2009, 58, 644–647. [Google Scholar] [CrossRef] [Green Version]
- Sabri, I.; Adwan, K.; Essawi, T.A.; Farraj, M.A. Molecular Characterization of Methicillin-Resistant Staphylococcus aureus Isolates in Three Different Arab World Countries. Eur. J. Microbiol. Immunol. 2013, 3, 183–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adwan, K.; Jarrar, N.; Abu-Hijleh, A.; Adwan, G.; Awwad, E.; Salameh, Y. Molecular Analysis and Susceptibility Patterns of Methicillin-Resistant Staphylococcus aureus Strains Causing Community- and Health Care-Associated Infections in the Northern Region of Palestine. Am. J. Infect. Control. 2013, 41, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.H.; Monk, I.R.; Gonçalves da Silva, A.; Seemann, T.; Chua, K.Y.L.; Kearns, A.; Hill, R.; Woodford, N.; Bartels, M.D.; Strommenger, B.; et al. Global Spread of Three Multidrug-Resistant Lineages of Staphylococcus Epidermidis. Nat. Microbiol. 2018, 3, 1175–1185. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Nakamura, I.; Sato, T.; Ono, D.; Sato, A.; Sonoda, S.; Aoki, K.; Miura, Y.; Koyama, S.; Tamai, K.; et al. Changes in the Genotypic Characteristics of Community-Acquired Methicillin-Resistant Staphylococcus aureus Collected in 244 Medical Facilities in Japan between 2010 and 2018: A Nationwide Surveillance. Microbiol. Spectr. 2022, 10, e02272-21. [Google Scholar] [CrossRef] [PubMed]
- Guillemot, D.; Bonacorsi, S.; Blanchard, J.S.; Weber, P.; Simon, S.; Guesnon, B.; Bingen, E.; Carbon, C. Amoxicillin-Clavulanate Therapy Increases Childhood Nasal Colonization by Methicillin-Susceptible Staphylococcus aureus Strains Producing High Levels of Penicillinase. Antimicrob. Agents Chemother. 2004, 48, 4618–4623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinelli, M.; Monaco, M.; Vimercati, M.; Ceraminiello, A.; Pantosti, A. Methicillin-Susceptible Staphylococcus aureus in Skin and Soft Tissue Infections, Northern Italy. Emerg. Infect. Dis. 2009, 15, 250. [Google Scholar] [CrossRef] [PubMed]
- Tein Ngoi, S.; Kiong Niek, W.; Lee, Y.W.; Abubakar, S.; Shuan, C.; Teh, J. Genomic Analysis Revealed a Novel Genotype of Methicillin-Susceptible Staphylococcus aureus Isolated from a Fatal Sepsis Case in Dengue Patient. Sci. Rep. 2021, 11, 4228. [Google Scholar] [CrossRef] [PubMed]
- Kanjilal, S.; Abdul Sater, M.R.; Thayer, M.; Lagoudas, G.K.; Kim, S.; Blainey, P.C.; Gradc, Y.H. Trends in Antibiotic Susceptibility in Staphylococcus aureus in Boston, Massachusetts, from 2000 to 2014. J. Clin. Microbiol. 2018, 56, e01160-17. [Google Scholar] [CrossRef] [Green Version]
- Taha, A.E.; Al-Ruwaili, N.M.; El-Masry, E.A.; Saad, A.E.; Taher, I.A. MRSA as an Indicator of Infection Control Measures in Turaif General Hospital, Northern Area-Saudi Arabia. J. Infect. Dev. Ctries. 2022, 16, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Bordon, J.; Master, R.N.; Clark, R.B.; Duvvuri, P.; Karlowsky, J.A.; Ayesu, K.; Klotchko, A.; Kapoor, R.; Ramirez, J. Methicillin-Resistant Staphylococcus aureus Resistance to Non-Beta-Lactam Antimicrobials in the United States from 1996 to 2008. Diagn. Microbiol. Infect Dis. 2010, 67, 395–398. [Google Scholar] [CrossRef]
- Alhunaif, S.A.; Almansour, S.; Almutairi, R.; Alshammari, S.; Alkhonain, L.; Alalwan, B.; Aljohani, S.; Alsaedy, A.; Bosaeed, M.; Alothman, A. Methicillin-Resistant Staphylococcus aureus Bacteremia: Epidemiology, Clinical Characteristics, Risk Factors, and Outcomes in a Tertiary Care Center in Riyadh, Saudi Arabia. Cureus 2021, 13, e14934. [Google Scholar] [CrossRef]
- Loke, H.Y.; Kyaw, W.M.; Chen, M.I.C.; Lim, J.W.; Ang, B.; Chow, A. Length of Stay and Odds of MRSA Acquisition: A Dose-Response Relationship? Epidemiol. Infect 2019, 147, e223. [Google Scholar] [CrossRef] [Green Version]
- Pomorska-Wesołowska, M.; Rózańska, A.; Natkaniec, J.; Gryglewska, B.; Szczypta, A.; Dzikowska, M.; Chmielarczyk, A.; Wójkowska-Mach, J. Longevity and Gender as the Risk Factors of Methicillin-Resistant Staphylococcus aureus Infections in Southern Poland. BMC Geriatr. 2017, 17, 51. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
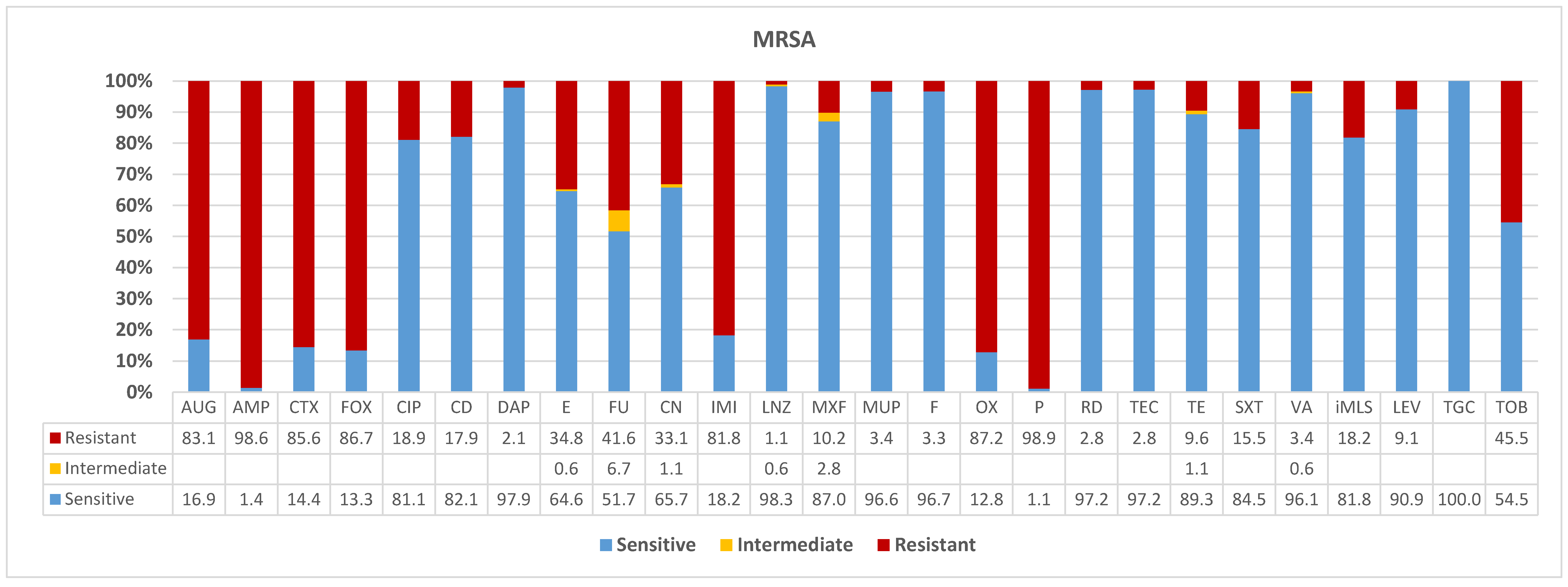
| AUG | AMP | CTX | FOX | CIP | CD | DAP | E | FU | CN | IMI | LNZ | MXF | MUP | F | OX | P | RD | TEC | TE | SXT | VA | iMLS | LEV | TGC | TOB | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sensitive | 16.9 | 1.4 | 14.4 | 13.3 | 81.1 | 82.1 | 97.9 | 64.6 | 51.7 | 65.7 | 18.2 | 98.3 | 87.0 | 96.6 | 96.7 | 12.8 | 1.1 | 97.2 | 97.2 | 89.3 | 84.5 | 96.1 | 81.8 | 90.9 | 100.0 | 54.5 |
| Intermediate | 0.6 | 6.7 | 1.1 | 0.6 | 2.8 | 1.1 | 0.6 | |||||||||||||||||||
| Resistant | 83.1 | 98.6 | 85.6 | 86.7 | 18.9 | 17.9 | 2.1 | 34.8 | 41.6 | 33.1 | 81.8 | 1.1 | 10.2 | 3.4 | 3.3 | 87.2 | 98.9 | 2.8 | 2.8 | 9.6 | 15.5 | 3.4 | 18.2 | 9.1 | 45.5 | |
| n | 148 | 142 | 146 | 180 | 148 | 179 | 146 | 178 | 178 | 181 | 148 | 179 | 177 | 145 | 180 | 179 | 179 | 178 | 179 | 178 | 181 | 179 | 33 | 33 | 33 | 33 |
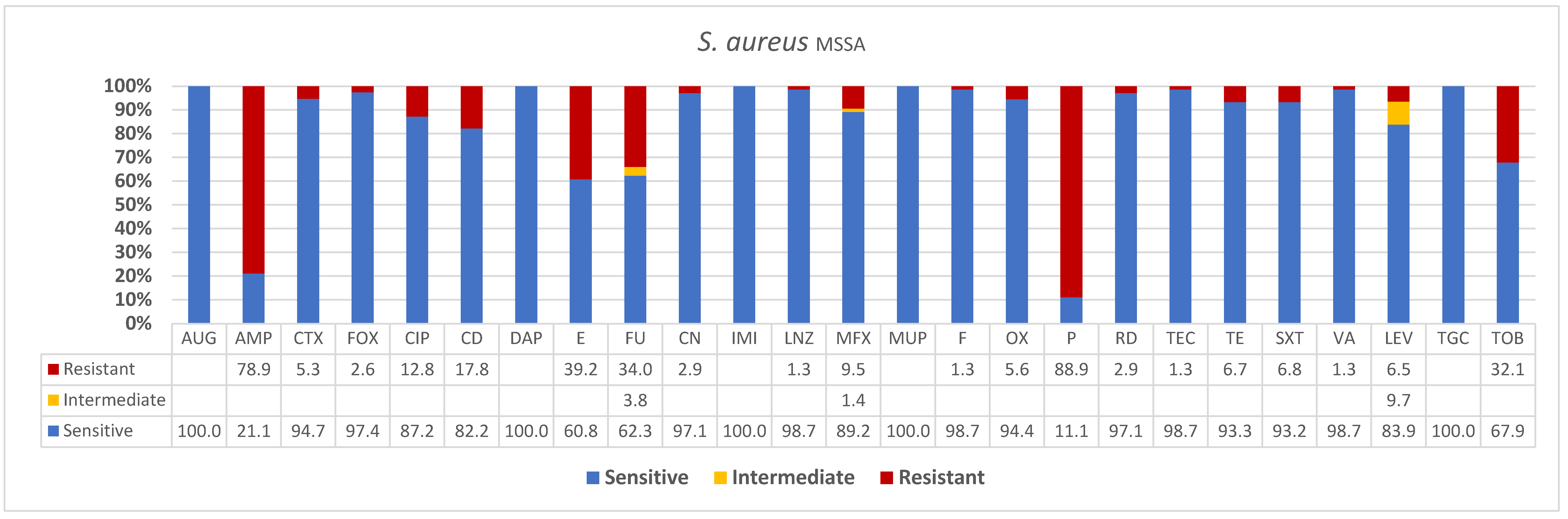
| AUG | AMP | CTX | FOX | CIP | CD | DAP | E | FU | CN | IMI | LNZ | MFX | MUP | F | OX | P | RD | TEC | TE | SXT | VA | LEV | TGC | TOB | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sensitive | 100.0 | 21.1 | 94.7 | 97.4 | 87.2 | 82.2 | 100.0 | 60.8 | 62.3 | 97.1 | 100.0 | 98.7 | 89.2 | 100.0 | 98.7 | 94.4 | 11.1 | 97.1 | 98.7 | 93.3 | 93.2 | 98.7 | 83.9 | 100.0 | 67.9 |
| Intermediate | 3.8 | 1.4 | 9.7 | ||||||||||||||||||||||
| Resistant | 78.9 | 5.3 | 2.6 | 12.8 | 17.8 | 39.2 | 34.0 | 2.9 | 1.3 | 9.5 | 1.3 | 5.6 | 88.9 | 2.9 | 1.3 | 6.7 | 6.8 | 1.3 | 6.5 | 32.1 | |||||
| n | 39 | 38 | 38 | 39 | 39 | 73 | 39 | 74 | 53 | 69 | 39 | 75 | 74 | 39 | 75 | 54 | 54 | 68 | 75 | 75 | 74 | 75 | 31 | 36 | 28 |
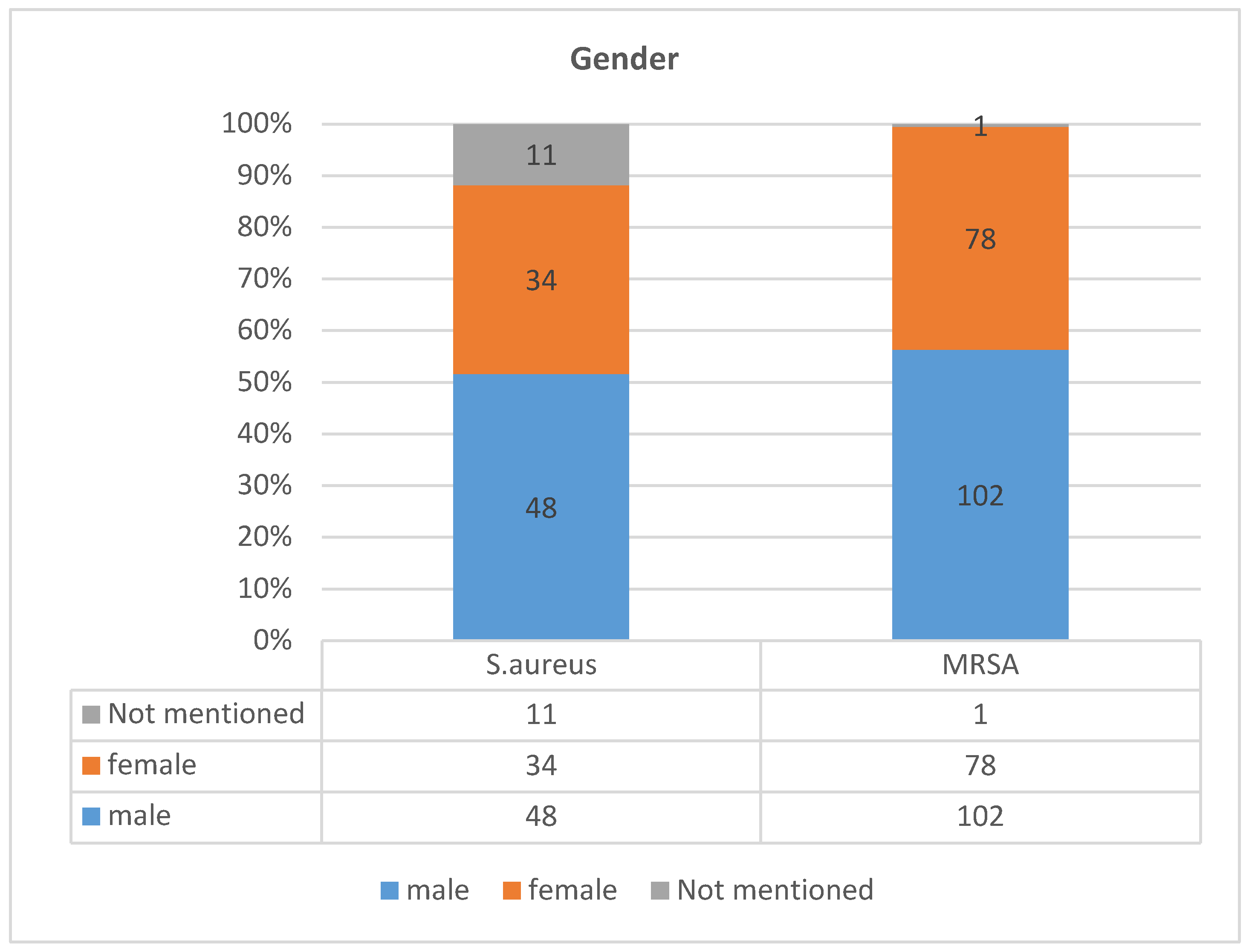
| Gender | MSSA | MRSA |
|---|---|---|
| male | 48 (17.5) | 102 (37) |
| female | 34 (12.4) | 78 (28.4) |
| Not mentioned | 11 | 1 |
| total | 93 (34%) | 181 (66%) |
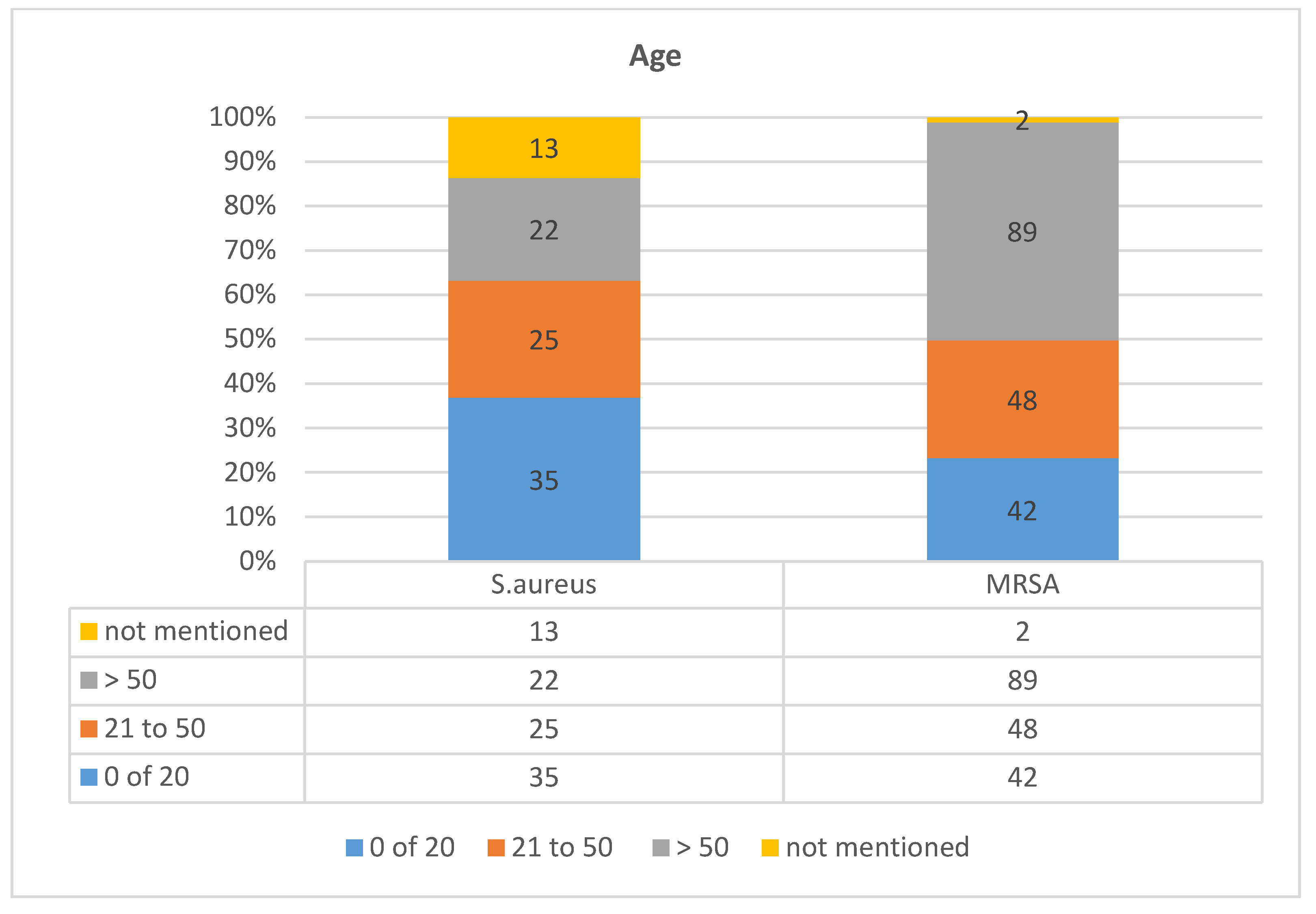
| Age | 0 of 20 | 21 to 50 | >50 | Not Mentioned | Total |
|---|---|---|---|---|---|
| MSSA | 35 (13%) | 25 (9%) | 22 (8%) | 13 (5%) | 95 (34.4) |
| MRSA | 42 (15%) | 48 (17%) | 89 (32%) | 2 | 181 (65.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said, K.B.; AlGhasab, N.S.; Alharbi, M.S.M.; Alsolami, A.; Bashir, A.I.; Saleem, M.; Syed Khaja, A.S.; Aldakheel, D.F.; Rakha, E.; Alshamri, J.A.; et al. A Sequalae of Lineage Divergence in Staphylococcus aureus from Community-Acquired Patterns in Youth to Hospital-Associated Profiles in Seniors Implied Age-Specific Host-Selection from a Common Ancestor. Diagnostics 2023, 13, 819. https://doi.org/10.3390/diagnostics13050819
Said KB, AlGhasab NS, Alharbi MSM, Alsolami A, Bashir AI, Saleem M, Syed Khaja AS, Aldakheel DF, Rakha E, Alshamri JA, et al. A Sequalae of Lineage Divergence in Staphylococcus aureus from Community-Acquired Patterns in Youth to Hospital-Associated Profiles in Seniors Implied Age-Specific Host-Selection from a Common Ancestor. Diagnostics. 2023; 13(5):819. https://doi.org/10.3390/diagnostics13050819
Chicago/Turabian StyleSaid, Kamaleldin B., Naif Saad AlGhasab, Mohammed S. M. Alharbi, Ahmed Alsolami, Abdelhafiz I. Bashir, Mohd Saleem, Azharuddin Sajid Syed Khaja, Dakheel F. Aldakheel, Ehab Rakha, Jabar A. Alshamri, and et al. 2023. "A Sequalae of Lineage Divergence in Staphylococcus aureus from Community-Acquired Patterns in Youth to Hospital-Associated Profiles in Seniors Implied Age-Specific Host-Selection from a Common Ancestor" Diagnostics 13, no. 5: 819. https://doi.org/10.3390/diagnostics13050819