
Acute Colonic Diverticulitis: CT Findings, Classifications, and a Proposal of a Structured Reporting Template
 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
CT Protocol
2. CT Findings: What to Look for
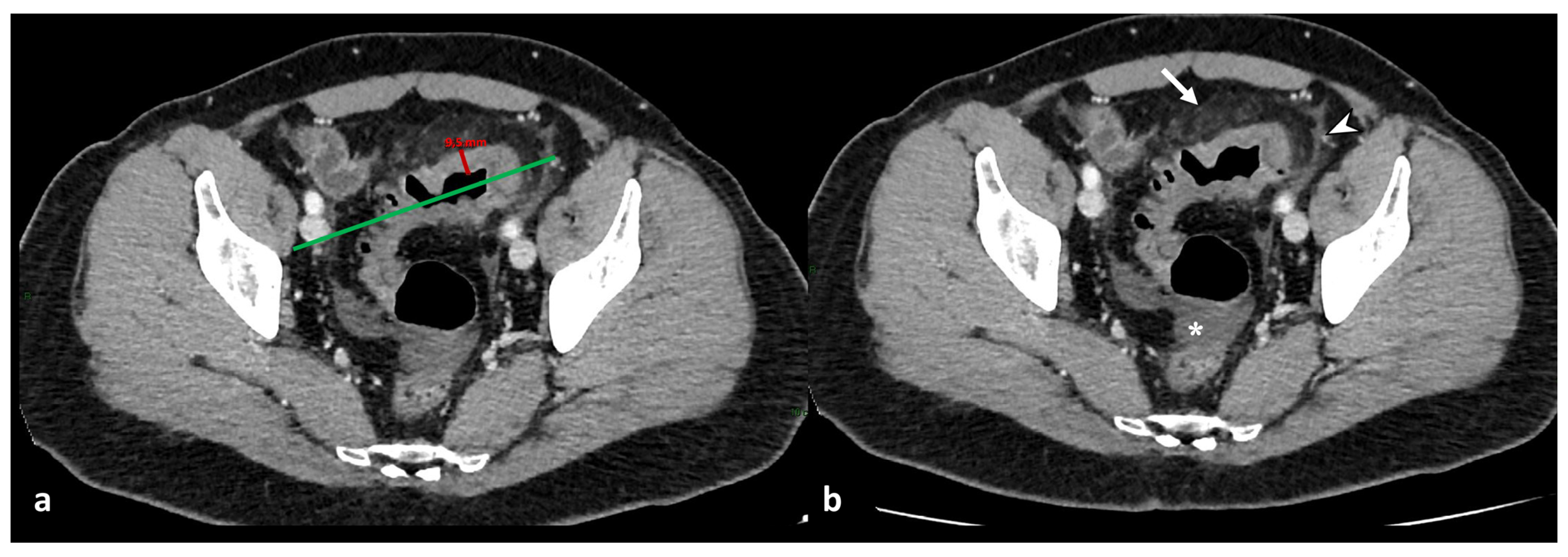
2.1. Bowel Wall Imaging Findings
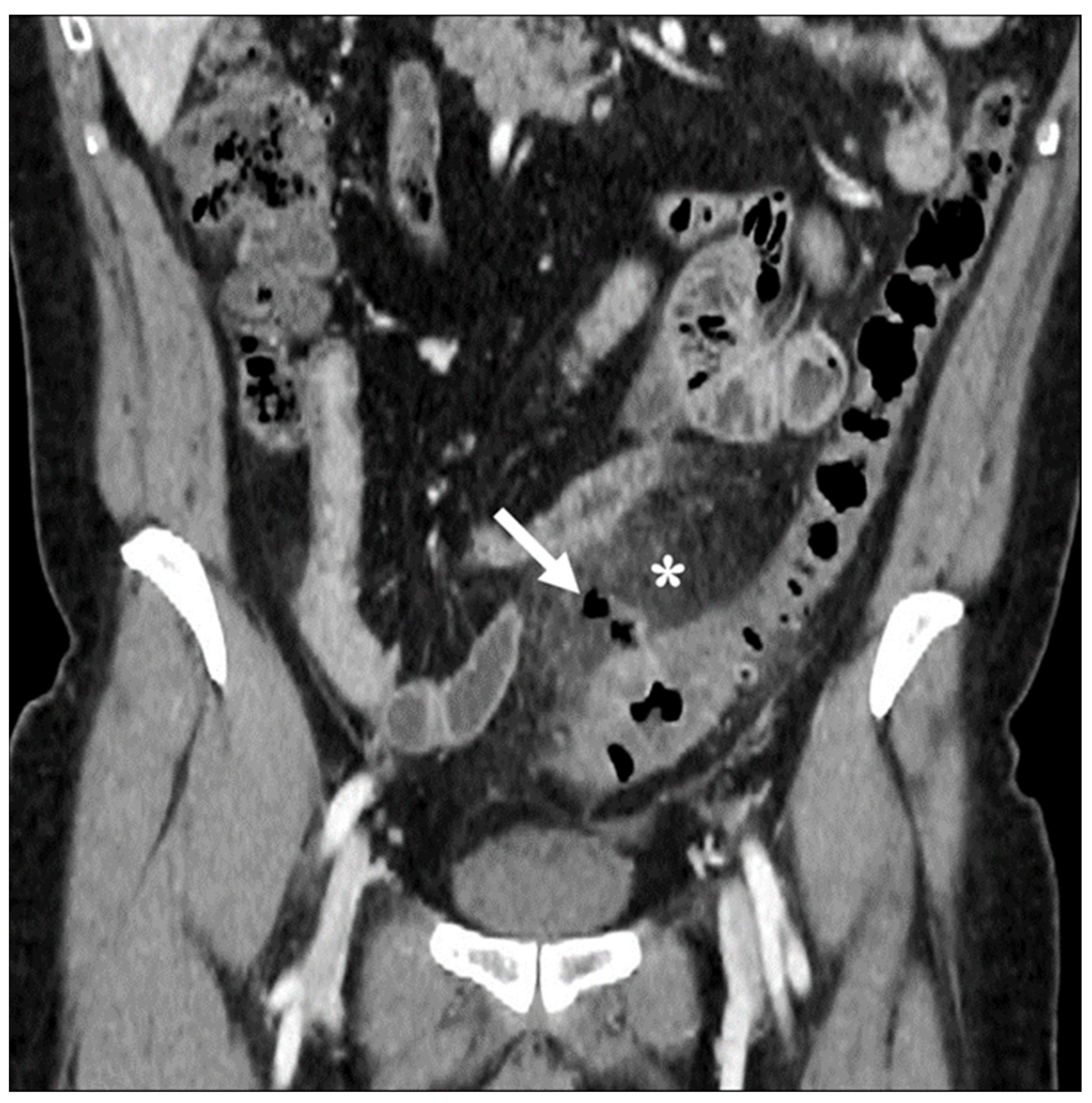
2.2. Extra-Intestinal Wall Imaging Findings
2.2.1. Mesenteric Findings
2.2.2. Vascular Findings
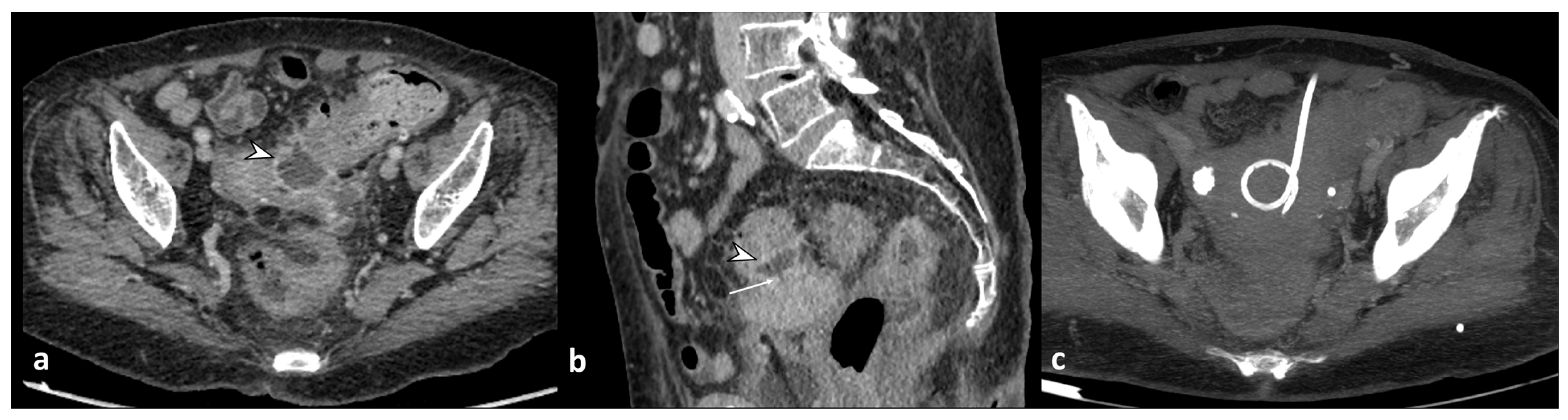
2.2.3. Findings of Complications
3. Staging and Management
4. Differential Diagnosis
5. Proposed Reporting Template
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hong, M.K.; Skandarajah, A.R.; Hayes, I.P. Diverticulosis, diverticular disease and diverticulitis—Definitions and differences. J. Stomal Ther. Aust. 2015, 35, 8–10. [Google Scholar]
- Naves, A.D.A.; D’Ippolito, G.; Souza, L.R.M.F.; Borges, S.P.; Fernandes, G.M. What radiologists should know about tomographic evaluation of acute diverticulitis of the colon. Radiol. Bras. 2017, 50, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Sugi, M.D.; Sun, D.C.; Menias, C.O.; Prabhu, V.; Choi, H.H. Acute diverticulitis: Key features for guiding clinical management. Eur. J. Radiol. 2020, 128, 109026. [Google Scholar] [CrossRef] [PubMed]
- Stollman, N.; Raskin, J.B. Diverticular disease of the colon. Lancet 2004, 363, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Onur, M.R.; Akpinar, E.; Karaosmanoglu, A.D.; Isayev, C.; Karcaaltincaba, M. Diverticulitis: A comprehensive review with usual and unusual complications. Insights Imaging 2017, 8, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Strate, L.L.; Morris, A.M. Epidemiology, Pathophysiology, and Treatment of Diverticulitis. Gastroenterology 2019, 156, 1282–1298.e1. [Google Scholar] [CrossRef]
- Galgano, S.J.; McNamara, M.M.; Peterson, C.M.; Kim, D.H.; Fowler, K.J.; Camacho, M.A.; Cash, B.D.; Chang, K.J.; Feig, B.W.; Gage, K.L.; et al. ACR Appropriateness Criteria® Left Lower Quadrant Pain-Suspected Diverticulitis. J. Am. Coll. Radiol. 2019, 16, S141–S149. [Google Scholar] [CrossRef]
- Sartelli, M.; Weber, D.G.; Kluger, Y.; Ansaloni, L.; Coccolini, F.; Abu-Zidan, F.; Augustin, G.; Ben-Ishay, O.; Biffl, W.L.; Bouliaris, K.; et al. 2020 update of the WSES guidelines for the management of acute colonic diverticulitis in the emergency setting. World J. Emerg. Surg. 2020, 15, 32. [Google Scholar] [CrossRef]
- Sartelli, M.; Viale, P.; Catena, F.; Ansaloni, L.; Moore, E.; Malangoni, M.; Moore, F.A.; Velmahos, G.; Coimbra, R.; Ivatury, R.; et al. 2013 WSES guidelines for management of intra-abdominal infections. World J. Emerg. Surg. 2013, 8, 3. [Google Scholar] [CrossRef]
- Sartelli, M.; Moore, F.A.; Ansaloni, L.; Di Saverio, S.; Coccolini, F.; Griffiths, E.A.; Coimbra, R.; Agresta, F.; Sakakushev, B.; Ordoñez, C.A.; et al. A proposal for a CT driven classification of left colon acute diverticulitis. World J. Emerg. Surg. 2015, 10, 3. [Google Scholar] [CrossRef]
- Kircher, M.F.; Rhea, J.T.; Kihiczak, D.; Novelline, R.A. Frequency, Sensitivity, and Specificity of Individual Signs of Diverticulitis on Thin-Section Helical CT with Colonic Contrast Material: Experience with 312 Cases. Am. J. Roentgenol. 2002, 178, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- DeStigter, K.; Keating, D. Imaging Update: Acute Colonic Diverticulitis. Clin. Colon Rectal Surg. 2009, 22, 147–155. [Google Scholar] [CrossRef]
- Minordi, L.M.; Larosa, L.; Berte, G.; Pecere, S.; Manfredi, R. CT of the acute colonic diverticulitis: A pictorial essay. Diagn. Interv. Radiol. 2020, 26, 546–551. [Google Scholar] [CrossRef] [PubMed]
- You, H.; Sweeny, A.; Cooper, M.L.; Von Papen, M.; Innes, J. The management of diverticulitis: A review of the guidelines. Med. J. Aust. 2019, 211, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Hill, B.C.; Johnson, S.C.; Owens, E.K.; Gerber, J.L.; Senagore, A.J. CT Scan for Suspected Acute Abdominal Process: Impact of Combinations of IV, Oral, and Rectal Contrast. World J. Surg. 2010, 34, 699–703. [Google Scholar] [CrossRef] [PubMed]
- Horton, K.M.; Corl, F.M.; Fishman, E.K. CT Evaluation of the Colon: Inflammatory Disease. RadioGraphics 2000, 20, 399–418. [Google Scholar] [CrossRef] [PubMed]
- Broder, J.S.; Hamedani, A.G.; Liu, S.W.; Emerman, C.L. Emergency Department Contrast Practices for Abdominal/Pelvic Computed Tomography—A National Survey and Comparison with the American College of Radiology Appropriateness Criteria®. J. Emerg. Med. 2013, 44, 423–433. [Google Scholar] [CrossRef]
- Fernandes, T.; Oliveira, M.I.; Castro, R.; Araújo, B.; Viamonte, B.; Cunha, R. Bowel wall thickening at CT: Simplifying the diagnosis. Insights Imaging 2014, 5, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Wiesner, W.; Mortelé, K.J.; Ji, H.; Ros, P.R. Normal Colonic Wall Thickness at CT and Its Relation to Colonic Distension. J. Comput. Assist. Tomogr. 2002, 26, 102–106. [Google Scholar] [CrossRef]
- Dickerson, E.C.; Chong, S.T.; Ellis, J.H.; Watcharotone, K.; Nan, B.; Davenport, M.S.; Al-Hawary, M.; Mazza, M.B.; Rizk, R.; Morris, A.M.; et al. Recurrence of Colonic Diverticulitis: Identifying Predictive CT Findings—Retrospective Cohort Study. Radiology 2017, 285, 850–858. [Google Scholar] [CrossRef]
- Pereira, J.M.; Sirlin, C.B.; Pinto, P.S.; Jeffrey, R.B.; Stella, D.L.; Casola, G. Disproportionate Fat Stranding: A Helpful CT Sign in Patients with Acute Abdominal Pain. RadioGraphics 2004, 24, 703–715. [Google Scholar] [CrossRef]
- Ben Yaacoub, I.; Boulay-Coletta, I.; Jullès, M.C.; Zins, M. CT findings of misleading features of colonic diverticulitis. Insights Imaging 2011, 2, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Perez-Cruet, M.J.; Grable, E.; Drapkin, M.S.; Jablons, D.M.; Cano, G. Pylephiebitis Associated With Diverticulitis. South. Med. J. 1993, 86, 578–580. [Google Scholar] [CrossRef]
- Schreyer, A.; Layer, G. S2k Guidlines for Diverticular Disease and Diverticulitis: Diagnosis, Classification, and Therapy for the Radiologist. Fortschr. Röntgenstr. 2015, 187, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Puylaert, J.B.C.M. Ultrasound of Colon Diverticulitis. Dig. Dis. 2012, 30, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Sessa, B.; Galluzzo, M.; Ianniello, S.; Pinto, A.; Trinci, M.; Miele, V. Acute Perforated Diverticulitis: Assessment With Multidetector Computed Tomography. Semin. Ultrasound CT MRI 2016, 37, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.W.; Jang, J.Y.; Lee, T.H.; Kim, H.G.; Hong, S.W.; Park, S.H.; Kim, S.G.; Cheon, Y.K.; Kim, Y.S.; Cho, Y.D.; et al. Cryptogenic pyogenic liver abscess as the herald of colon cancer: Colon cancer in cryptogenic liver abscess. J. Gastroenterol. Hepatol. 2012, 27, 248–255. [Google Scholar] [CrossRef]
- Woods, R.J.; Lavery, I.C.; Fazio, V.W.; Jagelman, D.G.; Weakley, F.L. Internal fistulas in diverticular disease. Dis. Colon Rectum 1988, 31, 591–596. [Google Scholar] [CrossRef]
- Neale, J. Surgical Management of Diverticular Disease in the Elective Setting. Clin. Colon Rectal Surg. 2018, 31, 236–242. [Google Scholar] [CrossRef]
- Maddu, K.K.; Mittal, P.; Shuaib, W.; Tewari, A.; Ibraheem, O.; Khosa, F. Colorectal Emergencies and Related Complications: A Comprehensive Imaging Review—Imaging of Colitis and Complications. Am. J. Roentgenol. 2014, 203, 1205–1216. [Google Scholar] [CrossRef]
- Hinchey, E.J.; Schaal, P.G.; Richards, G.K. Treatment of perforated diverticular disease of the colon. Adv. Surg. 1978, 12, 85–109. [Google Scholar] [PubMed]
- Kaiser, A.M.; Jiang, J.K.; Lake, J.P.; Ault, G.; Artinyan, A.; Gonzalez-Ruiz, C.; Essani, R.; Beart, R.W. The Management of Complicated Diverticulitis and the Role of Computed Tomography. Am. J. Gastroenterol. 2005, 100, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Shafi, S.; Aboutanos, M.; Brown, C.V.R.; Ciesla, D.; Cohen, M.J.; Crandall, M.L.; Inaba, K.; Miller, P.R.; Mowery, N.T. Measuring anatomic severity of disease in emergency general surgery. J. Trauma Acute Care Surg. 2014, 76, 884–887. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Bessoff, K.; Bromley-Dulfano, R.; Li, Z.; Gupta, A.; Taylor, K.; Wadhwa, H.; Seltzer, R.; Spain, D.A.; Knowlton, L.M. Prospectively Assigned AAST Grade versus Modified Hinchey Class and Acute Diverticulitis Outcomes. J. Surg. Res. 2021, 259, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.; Medvecz, A.J.; Connolly, C.; Sborov, K.; Matevish, L.; Wile, G.; Gondek, S.; Gunter, O.; Guillamondegui, O.; Dennis, B. Comparison of American Association for the Surgery of Trauma grading scale with modified Hinchey classification in acute colonic diverticulitis: A pilot study. J. Trauma Acute Care Surg. 2020, 88, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Cremonini, C.; Biloslavo, A.; Robustelli, V.; Giannessi, S.; Rossi Del Monte, S.; Mastronardi, M.; Musetti, S.; Strambi, S.; Coccolini, F.; Chiarugi, M.M.; et al. What are the differences between the three most used classifications for acute colonic diverticulitis? A comparative multicenter study: Acute diverticulitis classifications comparison. J. Trauma Acute Care Surg. 2023, 10–97. [Google Scholar] [CrossRef] [PubMed]
- Lips, L.M.J.; Cremers, P.T.J.; Pickhardt, P.J.; Cremers, S.E.H.; Janssen-Heijnen, M.L.G.; De Witte, M.T.; Simons, P.C.G. Sigmoid Cancer versus Chronic Diverticular Disease: Differentiating Features at CT Colonography. Radiology 2015, 275, 127–135. [Google Scholar] [CrossRef]
- Singh, A.K.; Gervais, D.A.; Hahn, P.F.; Rhea, J.; Mueller, P.R. CT Appearance of Acute Appendagitis. Am. J. Roentgenol. 2004, 183, 1303–1307. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Gervais, D.A.; Hahn, P.F.; Sagar, P.; Mueller, P.R.; Novelline, R.A. Acute Epiploic Appendagitis and Its Mimics. RadioGraphics 2005, 25, 1521–1534. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Panicek, D.M.; Berk, A.R.; Li, Y.; Hricak, H. Improving Communication of Diagnostic Radiology Findings through Structured Reporting. Radiology 2011, 260, 174–181. [Google Scholar] [CrossRef]
- Kruskal, J.B.; Reedy, A.; Pascal, L.; Rosen, M.P.; Boiselle, P.M. Quality Initiatives: Lean Approach to Improving Performance and Efficiency in a Radiology Department. RadioGraphics 2012, 32, 573–587. [Google Scholar] [CrossRef] [PubMed]
- Khurana, A.; Nelson, L.W.; Myers, C.B.; Akisik, F.; Jeffrey, B.R.; Miller, F.H.; Mittal, P.; Morgan, D.; Mortele, K.; Poullos, P.; et al. Reporting of acute pancreatitis by radiologists-time for a systematic change with structured reporting template. Abdom. Radiol. 2020, 45, 1277–1289. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Caruso, D.; Grassi, R.; Cappabianca, S.; Reginelli, A.; Rizzati, R.; Masselli, G.; Golfieri, R.; Rengo, M.; Regge, D.; et al. Structured Reporting of Rectal Cancer Staging and Restaging: A Consensus Proposal. Cancers 2021, 13, 2135. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hinchey Classification [31] | Modified Hinchey Classification by Kaiser et al. [32] | CDD * by Schreyer et al. [24] | AAST ** Grade [33] | WSES Classification by Sartelli et al. [10] | |
|---|---|---|---|---|---|
| 0 | Mild clinical diverticulitis | Asymptomatic diverticulosis | Uncomplicated diverticulitis | ||
| 1 | Pericolic abscess or phlegmon | Acute uncomplicated diverticular disease/diverticulitis | Colonic inflammation | ||
| 1a | Confined pericolic inflammation/phlegmon | Diverticulitis/diverticular disease without reaction of surrounding tissue | Pericolic air bubbles or little pericolic fluid without abscess | ||
| 1b | Pericolonic/mesocolic abscess | diverticulitis with phlegmonous reaction of surrounding tissue | Abscess ≤ 4 cm | ||
| 2 | Pelvic, distant intraabdominal, or retroperitoneal abscess | Pelvic, distant intraabdominal, or retroperitoneal abscess | Acute complicated diverticulitis as in 1b, additionally | Colon microperforation or pericolic phlegmon without abscess | |
| 2a | Microabscess | Abscess > 4 cm | |||
| 2b | Macroabscess | Distant air (>5 cm from inflamed bowel segment) | |||
| 2c | Free perforation (2c1 purulent peritonitis; 2c2 fecal peritonitis) | ||||
| 3 | Generalized purulent peritonitis | Generalized purulent peritonitis | Chronic diverticular disease recurrent or chronic symptomatic diverticular disease | Localized pericolic abscess | Diffuse fluid without distant free air (no hole in colon) |
| 3a | Symptomatic uncomplicated diverticular disease (SUDD) | ||||
| 3b | Recurrent diverticulitis without complications | ||||
| 3c | Recurrent diverticulitis with complications | ||||
| 4 | Generalized fecal peritonitis | Generalized fecal peritonitis | Diverticular bleeding | Distant and/or multiple abscesses | Diffuse fluid with distant free air (persistent hole in the colon) |
| 5 | Free colonic perforation with generalized peritonitis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiralongo, F.; Di Pietro, S.; Milazzo, D.; Galioto, S.; Castiglione, D.G.; Ini’, C.; Foti, P.V.; Mosconi, C.; Giurazza, F.; Venturini, M.; et al. Acute Colonic Diverticulitis: CT Findings, Classifications, and a Proposal of a Structured Reporting Template. Diagnostics 2023, 13, 3628. https://doi.org/10.3390/diagnostics13243628
Tiralongo F, Di Pietro S, Milazzo D, Galioto S, Castiglione DG, Ini’ C, Foti PV, Mosconi C, Giurazza F, Venturini M, et al. Acute Colonic Diverticulitis: CT Findings, Classifications, and a Proposal of a Structured Reporting Template. Diagnostics. 2023; 13(24):3628. https://doi.org/10.3390/diagnostics13243628
Chicago/Turabian StyleTiralongo, Francesco, Stefano Di Pietro, Dario Milazzo, Sebastiano Galioto, Davide Giuseppe Castiglione, Corrado Ini’, Pietro Valerio Foti, Cristina Mosconi, Francesco Giurazza, Massimo Venturini, and et al. 2023. "Acute Colonic Diverticulitis: CT Findings, Classifications, and a Proposal of a Structured Reporting Template" Diagnostics 13, no. 24: 3628. https://doi.org/10.3390/diagnostics13243628