
Robot-Aided Motion Analysis in Neurorehabilitation: Benefits and Challenges

Abstract
:1. Introduction
2. Methods
3. Motion Analysis and Its Biomechanical Contribution to Accuracy Prediction
4. Robotic Devices for Upper Limb Measurement
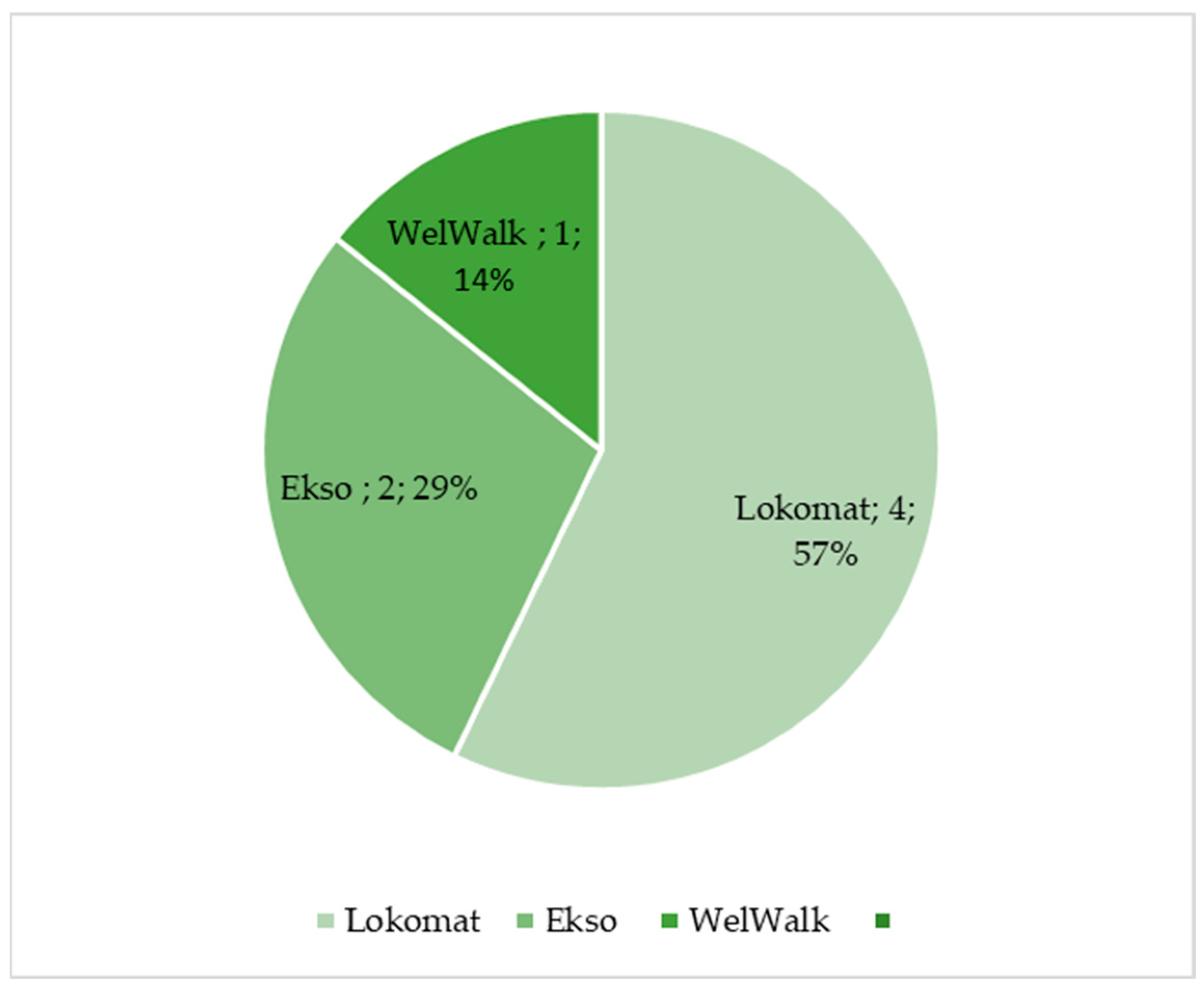
5. Robotic Device for Lower Limb Assessment
6. Discussion
6.1. Benefits of Robotic-Aided Motion Analysis
6.2. Challenges of Robotic-Aided Motion Analysis
6.3. Future Perspectives: Combined Approaches and Beyond
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iandolo, R.; Marini, F.; Semprini, M.; Laffranchi, M.; Mugnosso, M.; Cherif, A.; De Michieli, L.; Chiappalone, M.; Zenzeri, J. Perspectives and Challenges in Robotic Neurorehabilitation. Appl. Sci. 2019, 9, 3183. [Google Scholar] [CrossRef]
- Meng, W.; Liu, Q.; Zhou, Z.; Ai, Q.; Sheng, B.; Xie, S. Recent development of mechanisms and control strategies for robot-assisted lower limb rehabilitation. Mechatronics 2015, 31, 132–145. [Google Scholar] [CrossRef]
- Rehmat, N.; Zuo, J.; Meng, W.; Liu, Q.; Xie, S.Q.; Liang, H. Upper limb rehabilitation using robotic exoskeleton systems: A systematic review. Int. J. Intell. Robot. Appl. 2018, 2, 283–295. [Google Scholar] [CrossRef]
- Shishov, N.; Melzer, I.; Bar-Haim, S. Parameters and Measures in Assessment of Motor Learning in Neurorehabilitation; A Systematic Review of the Literature. Front. Hum. Neurosci. 2017, 11, 82. [Google Scholar] [CrossRef]
- Roggio, F.; Ravalli, S.; Maugeri, G.; Bianco, A.; Palma, A.; Di Rosa, M.; Musumeci, G. Technological advancements in the analysis of human motion and posture management through digital devices. World J. Orthop. 2021, 12, 467–484. [Google Scholar] [CrossRef]
- Crenna, F.; Rossi, G.B.; Berardengo, M. Filtering Biomechanical Signals in Movement Analysis. Sensors 2021, 21, 4580. [Google Scholar] [CrossRef] [PubMed]
- Muro-de-la-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef]
- Laut, J.; Porfiri, M.; Raghavan, P. The Present and Future of Robotic Technology in Rehabilitation. Curr. Phys. Med. Rehabil. Rep. 2016, 4, 312–319. [Google Scholar] [CrossRef]
- Maggioni, S.; Melendez-Calderon, A.; van Asseldonk, E.; Klamroth-Marganska, V.; Lünenburger, L.; Riener, R.; van der Kooij, H. Robot-aided assessment of lower extremity functions: A review. J. Neuroeng. Rehabil. 2016, 13, 72. [Google Scholar] [CrossRef]
- Green, B.N.; Johnson, C.D.; Adams, A. Writing narrative literature reviews for peer-reviewed journals: Secrets of the trade. J. Chiropr. Med. 2006, 5, 101–117. [Google Scholar] [CrossRef]
- Ma, C.Z.-H.; Li, Z.; He, C. Advances in Biomechanics-Based Motion Analysis. Bioengineering 2023, 10, 677. [Google Scholar] [CrossRef] [PubMed]
- Grimmer, M.; Zeiss, J.; Weigand, F.; Zhao, G.; Lamm, S.; Steil, M.; Heller, A. Lower limb joint biomechanics-based identification of gait transitions in between level walking and stair ambulation. PLoS ONE 2020, 15, e0239148. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, T.; Fujimoto, Y. Dynamics Analysis: Equations of Motion. In Humanoid Robotics: A Reference; Goswami, A., Vadakkepat, P., Eds.; Springer: Dordrecht, The Netherlands, 2017. [Google Scholar] [CrossRef]
- Yeadon, M.; Pain, M. Fifty years of performance-related sports biomechanics research. J. Biomech. 2023, 155, 111666. [Google Scholar] [CrossRef] [PubMed]
- Lerchl, T.; Nispel, K.; Baum, T.; Bodden, J.; Senner, V.; Kirschke, J.S. Multibody Models of the Thoracolumbar Spine: A Review on Applications, Limitations, and Challenges. Bioengineering 2023, 10, 202. [Google Scholar] [CrossRef] [PubMed]
- Parashar, S.K.; Sharma, J.K. A review on application of finite element modelling in bone biomechanics. Perspect. Sci. 2016, 8, 696–698. [Google Scholar] [CrossRef]
- Colyer, S.L.; Evans, M.; Cosker, D.P.; Salo, A.I.T. A Review of the Evolution of Vision-Based Motion Analysis and the Integration of Advanced Computer Vision Methods towards Developing a Markerless System. Sports Med.-Open 2018, 4, 24. [Google Scholar] [CrossRef]
- Kwon, C.-W.; Yun, S.-H.; Koo, D.-K.; Kwon, J.-W. Kinetic and Kinematic Analysis of Gait Termination: A Comparison between Planned and Unplanned Conditions. Appl. Sci. 2023, 13, 7323. [Google Scholar] [CrossRef]
- Aprile, I.; Rabuffetti, M.; Padua, L.; Di Sipio, E.; Simbolotti, C.; Ferrarin, M. Kinematic Analysis of the Upper Limb Motor Strategies in Stroke Patients as a Tool towards Advanced Neurorehabilitation Strategies: A Preliminary Study. BioMed Res. Int. 2014, 2014, 636123. [Google Scholar] [CrossRef]
- Brihmat, N.; Loubinoux, I.; Castel-Lacanal, E.; Marque, P.; Gasq, D. Kinematic parameters obtained with the ArmeoSpring for upper-limb assessment after stroke: A reliability and learning effect study for guiding parameter use. J. Neuroeng. Rehabil. 2020, 17, 130. [Google Scholar] [CrossRef]
- Branco, M.P.; de Boer, L.M.; Ramsey, N.F.; Vansteensel, M.J. Encoding of kinetic and kinematic movement parameters in the sensorimotor cortex: A Brain-Computer Interface perspective. Eur. J. Neurosci. 2019, 50, 2755–2772. [Google Scholar] [CrossRef]
- Al-Mulla, M.R.; Sepulveda, F.; Colley, M. A Review of Non-Invasive Techniques to Detect and Predict Localised Muscle Fatigue. Sensors 2011, 11, 3545–3594. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, L.V.; Bittmann, F.N. Are there two forms of isometric muscle action? Results of the experimental study support a distinction between a holding and a pushing isometric muscle function. BMC Sports Sci. Med. Rehabil. 2017, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Halilaj, E.; Rajagopal, A.; Fiterau, M.; Hicks, J.L.; Hastie, T.J.; Delp, S.L. Machine learning in human movement biomechanics: Best practices, common pitfalls, and new opportunities. J. Biomech. 2018, 81, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Giarmatzis, G.; Zacharaki, E.I.; Moustakas, K. Real-Time Prediction of Joint Forces by Motion Capture and Machine Learning. Sensors 2020, 20, 6933. [Google Scholar] [CrossRef] [PubMed]
- Mundt, M.; Koeppe, A.; Bamer, F.; David, S.; Markert, B. Artificial Neural Networks in Motion Analysis—Applications of Unsupervised and Heuristic Feature Selection Techniques. Sensors 2020, 20, 4581. [Google Scholar] [CrossRef] [PubMed]
- Ai, Q.; Liu, Z.; Meng, W.; Liu, Q.; Xie, S.Q. Machine Learning in Robot Assisted Upper Limb Rehabilitation: A Focused Review. IEEE Trans. Cogn. Dev. Syst. 2021. [Google Scholar] [CrossRef]
- Maura, R.M.; Parra, S.R.; Stevens, R.E.; Weeks, D.L.; Wolbrecht, E.T.; Perry, J.C. Literature review of stroke assessment for upper-extremity physical function via EEG, EMG, kinematic, and kinetic measurements and their reliability. J. Neuroeng. Rehabil. 2023, 20, 21. [Google Scholar] [CrossRef] [PubMed]
- Galeoto, G.; Berardi, A.; Mangone, M.; Tufo, L.; Silvani, M.; González-Bernal, J.; Seco-Calvo, J. Assessment Capacity of the Armeo® Power: Cross-Sectional Study. Technologies 2023, 11, 125. [Google Scholar] [CrossRef]
- Merlo, A.; Longhi, M.; Giannotti, E.; Prati, P.; Giacobbi, M.; Ruscelli, E.; Mancini, A.; Ottaviani, M.; Montanari, L.; Mazzoli, D. Upper limb evaluation with robotic exoskeleton. Normative values for indices of accuracy, speed and smoothness. NeuroRehabilitation 2013, 33, 523–530. [Google Scholar] [CrossRef]
- Longhi, M.; Merlo, A.; Prati, P.; Giacobbi, M.; Mazzoli, D. Instrumental indices for upper limb function assessment in stroke patients: A validation study. J. Neuroeng. Rehabil. 2016, 13, 52. [Google Scholar] [CrossRef]
- Goffredo, M.; Pournajaf, S.; Proietti, S.; Gison, A.; Posteraro, F.; Franceschini, M. Retrospective Robot-Measured Upper Limb Kinematic Data From Stroke Patients Are Novel Biomarkers. Front. Neurol. 2021, 12, 803901. [Google Scholar] [CrossRef] [PubMed]
- Cordella, F.; Scotto, D.; Luzio, F.; Bravi, M.; Santacaterina, F.; Bressi, F.; Zollo, L. Hand motion analysis during robot-aided rehabilitation in chronic stroke. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. S3), 45–52. [Google Scholar] [PubMed]
- Calabrò, R.S.; Russo, M.; Naro, A.; Milardi, D.; Balletta, T.; Leo, A.; Filoni, S.; Bramanti, P. Who May Benefit From Armeo Power Treatment? A Neurophysiological Approach to Predict Neurorehabilitation Outcomes. PM&R 2016, 8, 971–978. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Russo, M.; Milardi, D.; Leo, A.; Filoni, S.; Trinchera, A.; Bramanti, P. Is two better than one? Muscle vibration plus robotic rehabilitation to improve upper limb spasticity and function: A pilot randomized controlled trial. PLoS ONE 2017, 12, e0185936. [Google Scholar] [CrossRef] [PubMed]
- Palermo, E.; Hayes, D.R.; Russo, E.F.; Calabrò, R.S.; Pacilli, A.; Filoni, S. Translational effects of robot-mediated therapy in subacute stroke patients: An experimental evaluation of upper limb motor recovery. PeerJ 2018, 6, e5544. [Google Scholar] [CrossRef]
- Santisteban, L.; Térémetz, M.; Bleton, J.-P.; Baron, J.-C.; Maier, M.A.; Lindberg, P.G. Upper Limb Outcome Measures Used in Stroke Rehabilitation Studies: A Systematic Literature Review. PLoS ONE 2016, 11, e0154792. [Google Scholar] [CrossRef]
- De-La-Torre, R.; Oña, E.D.; Balaguer, C.; Jardón, A. Robot-Aided Systems for Improving the Assessment of Upper Limb Spasticity: A Systematic Review. Sensors 2020, 20, 5251. [Google Scholar] [CrossRef]
- Bonanno, M.; De Luca, R.; Torregrossa, W.; Tonin, P.; Calabrò, R.S. Moving toward Appropriate Motor Assessment Tools in People Affected by Severe Acquired Brain Injury: A Scoping Review with Clinical Advices. Healthcare 2022, 10, 1115. [Google Scholar] [CrossRef]
- Kung, P.-C.; Lin, C.-C.K.; Ju, M.-S. Neuro-rehabilitation robot-assisted assessments of synergy patterns of forearm, elbow and shoulder joints in chronic stroke patients. Clin. Biomech. 2010, 25, 647–654. [Google Scholar] [CrossRef]
- Zhao, K.; Zhang, Z.; Wen, H.; Liu, B.; Li, J.; D’avella, A.; Scano, A. Muscle synergies for evaluating upper limb in clinical applications: A systematic review. Heliyon 2023, 9, e16202. [Google Scholar] [CrossRef]
- Safavynia, S.A.; Torres-Oviedo, G.; Ting, L.H. Muscle Synergies: Implications for Clinical Evaluation and Rehabilitation of Movement. Top. Spinal Cord Inj. Rehabil. 2011, 17, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Toigo, M.; Flück, M.; Riener, R.; Klamroth-Marganska, V. Robot-assisted assessment of muscle strength. J. Neuroeng. Rehabil. 2017, 14, 103. [Google Scholar] [CrossRef] [PubMed]
- Tiboni, M.; Borboni, A.; Vérité, F.; Bregoli, C.; Amici, C. Sensors and Actuation Technologies in Exoskeletons: A Review. Sensors 2022, 22, 884. [Google Scholar] [CrossRef]
- Bonanno, M.; De Nunzio, A.M.; Quartarone, A.; Militi, A.; Petralito, F.; Calabrò, R.S. Gait Analysis in Neurorehabilitation: From Research to Clinical Practice. Bioengineering 2023, 10, 785. [Google Scholar] [CrossRef] [PubMed]
- Imoto, D.; Hirano, S.; Mukaino, M.; Saitoh, E.; Otaka, Y. A novel gait analysis system for detecting abnormal hemiparetic gait patterns during robot-assisted gait training: A criterion validity study among healthy adults. Front. Neurorobot. 2022, 16, 1047376. [Google Scholar] [CrossRef] [PubMed]
- Boudarham, J.; Hameau, S.; Zory, R.; Hardy, A.; Bensmail, D.; Roche, N. Coactivation of Lower Limb Muscles during Gait in Patients with Multiple Sclerosis. PLoS ONE 2016, 11, e0158267. [Google Scholar] [CrossRef]
- Romanato, M.; Spolaor, F.; Beretta, C.; Fichera, F.; Bertoldo, A.; Volpe, D.; Sawacha, Z. Quantitative assessment of training effects using EksoGT® exoskeleton in Parkinson’s disease patients: A randomized single blind clinical trial. Contemp. Clin. Trials Commun. 2022, 28, 100926. [Google Scholar] [CrossRef]
- Afzal, T.; Zhu, F.; Tseng, S.-C.; Lincoln, J.A.; Francisco, G.E.; Su, H.; Chang, S.-H. Evaluation of Muscle Synergy During Exoskeleton-Assisted Walking in Persons With Multiple Sclerosis. IEEE Trans. Biomed. Eng. 2022, 69, 3265–3274. [Google Scholar] [CrossRef]
- Domingo, A.; Marriott, E.; de Grave, R.B.; Lam, T. Quantifying lower limb joint position sense using a robotic exoskeleton: A pilot study. In Proceedings of the 2011 IEEE 12th International Conference on Rehabilitation Robotics: Reaching Users & the Community (ICORR 2011), Zurich, Switzerland, 29 June–1 July 2011; pp. 1–6. [Google Scholar]
- Domingo, A.; Lam, T. Reliability and validity of using the Lokomat to assess lower limb joint position sense in people with incomplete spinal cord injury. J. Neuroeng. Rehabil. 2014, 11, 167. [Google Scholar] [CrossRef]
- Chisholm, A.E.; Domingo, A.; Jeyasurya, J.; Lam, T. Quantification of Lower Extremity Kinesthesia Deficits Using a Robotic Exoskeleton in People With a Spinal Cord Injury. Neurorehabilit. Neural Repair 2016, 30, 199–208. [Google Scholar] [CrossRef]
- Moeller, T.; Moehler, F.; Krell-Roesch, J.; Dežman, M.; Marquardt, C.; Asfour, T.; Stein, T.; Woll, A. Use of Lower Limb Exoskeletons as an Assessment Tool for Human Motor Performance: A Systematic Review. Sensors 2023, 23, 3032. [Google Scholar] [CrossRef] [PubMed]
- Maggioni, S.; Lunenburger, L.; Riener, R.; Melendez-Calderon, A. Robot-aided assessment of walking function based on an adaptive algorithm. In Proceedings of the 2015 IEEE International Conference on Rehabilitation Robotics (ICORR 2015), Singapore, 11–14 August 2015; Yu, H., Ed.; IEEE: Piscataway, NJ, USA, 2015; pp. 804–809, ISBN 978-1-4799-1808-9. [Google Scholar]
- Mercado, L.; Alvarado, L.; Quiroz-Compean, G.; Romo-Vazquez, R.; Vélez-Pérez, H.; Platas-Garza, M.; González-Garrido, A.A.; Gómez-Correa, J.; Morales, J.A.; Rodriguez-Liñan, A.; et al. Decoding the torque of lower limb joints from EEG recordings of pre-gait movements using a machine learning scheme. Neurocomputing 2021, 446, 118–129. [Google Scholar] [CrossRef]
- El Yaakoubi, N.A.; McDonald, C.; Lennon, O. Prediction of Gait Kinematics and Kinetics: A Systematic Review of EMG and EEG Signal Use and Their Contribution to Prediction Accuracy. Bioengineering 2023, 10, 1162. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, P. Upper Limb Motor Impairment After Stroke. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Spaulding, W.; Deogun, J. A Pathway to Personalization of Integrated Treatment: Informatics and Decision Science in Psychiatric Rehabilitation. Schizophr. Bull. 2011, 37, S129–S137. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Zhang, X.; Qiu, H. Rehabilomics: A state-of-the-art review of framework, application, and future considerations. Front. Neurol. 2023, 14, 1103349. [Google Scholar] [CrossRef] [PubMed]
- Garro, F.; Chiappalone, M.; Buccelli, S.; De Michieli, L.; Semprini, M. Neuromechanical Biomarkers for Robotic Neurorehabilitation. Front. Neurorobot. 2021, 15, 742163. [Google Scholar] [CrossRef]
- Úbeda, A.; Costa-Garcia, A.; Torricelli, D.; Vujaklija, I.; Del Vecchio, A. Editorial: Neuromechanical Biomarkers in Robot-Assisted Motor Rehabilitation. Front. Neurorobot. 2022, 15, 831113. [Google Scholar] [CrossRef]
- Mallat, R.; Khalil, M.; Venture, G.; Bonnet, V.; Mohammed, S. Human-Exoskeleton Joint Misalignment: A Systematic Review. In Proceedings of the 2019 Fifth International Conference on Advances in Biomedical Engineering (ICABME), Tripoli, Lebanon, 17–19 October 2019; pp. 1–4. [Google Scholar]
- Ramos, O.; Múnera, M.; Moazen, M.; Wurdemann, H.; Cifuentes, C.A. Assessment of Soft Actuators for Hand Exoskeletons: Pleated Textile Actuators and Fiber-Reinforced Silicone Actuators. Front. Bioeng. Biotechnol. 2022, 10, 924888. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Müller-Eising, C.; Diliberti, M.L.; Manuli, A.; Parrinello, F.; Rao, G.; Barone, V.; Civello, T. Who Will Pay for Robotic Rehabilitation? The Growing Need for a Cost-effectiveness Analysis. Innov. Clin. Neurosci. 2020, 17, 14–16. [Google Scholar]
- McManus, L.; De Vito, G.; Lowery, M.M. Analysis and Biophysics of Surface EMG for Physiotherapists and Kinesiologists: Toward a Common Language With Rehabilitation Engineers. Front. Neurol. 2020, 11, 576729. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Park, S.-J. Prediction of Myoelectric Biomarkers in Post-Stroke Gait. Sensors 2021, 21, 5334. [Google Scholar] [CrossRef] [PubMed]
- Rohrer, B.; Fasoli, S.; Krebs, H.I.; Hughes, R.; Volpe, B.; Frontera, W.R.; Stein, J.; Hogan, N. Movement Smoothness Changes during Stroke Recovery. J. Neurosci. 2002, 22, 8297–8304. [Google Scholar] [CrossRef] [PubMed]
- Schiefelbein, M.L.; Salazar, A.P.; Marchese, R.R.; Rech, K.D.; Schifino, G.P.; Figueiredo, C.S.; Cimolin, V.; Pagnussat, A.S. Upper-limb movement smoothness after stroke and its relationship with measures of body function/structure and activity—A cross-sectional study. J. Neurol. Sci. 2019, 401, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Korovesis, N.; Kandris, D.; Koulouras, G.; Alexandridis, A. Robot Motion Control via an EEG-Based Brain–Computer Interface by Using Neural Networks and Alpha Brainwaves. Electronics 2019, 8, 1387. [Google Scholar] [CrossRef]
- Hekmatmanesh, A.; Nardelli, P.H.J.; Handroos, H. Review of the State-of-the-Art of Brain-Controlled Vehicles. IEEE Access 2021, 9, 110173–110193. [Google Scholar] [CrossRef]
- Moioli, R.C.; Nardelli, P.H.J.; Barros, M.T.; Saad, W.; Hekmatmanesh, A.; Silva, P.E.G.; de Sena, A.S.; Dzaferagic, M.; Siljak, H.; Van Leekwijck, W.; et al. Neurosciences and Wireless Networks: The Potential of Brain-Type Communications and Their Applications. IEEE Commun. Surv. Tutor. 2021, 23, 1599–1621. [Google Scholar] [CrossRef]
- Scano, A.; Guanziroli, E.; Mira, R.M.; Brambilla, C.; Tosatti, L.M.; Molteni, F. Biomechanical assessment of the ipsilesional upper limb in post-stroke patients during multi-joint reaching tasks: A quantitative study. Front. Rehabil. Sci. 2022, 3, 943397. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference No. | Robotic Device | Description | Usefulness of Robot-Aided Motion Analysis |
|---|---|---|---|
| [29] | Armeo®Power (Hocoma AG, Switzerland) | The Armeo®Power is a 6-degrees-of-freedom exoskeleton for upper limb rehabilitation. | Useful tool for the objective evaluation of upper limbs in post-stroke patients. The kinetic parameters of the motion analysis included kinetic parameters of the shoulder (flexion–extension, abduction and adduction, internal and external rotation), of the elbow (flexion–extension, prone–supination), of the wrist (flexion–extension), and of the hand (opening and closing). The values deriving from the valuation of the articular range were expressed in degrees; the values deriving from the evaluation of the force were expressed in Newton meters (Nm). |
| [30] | Armeo®Spring (Hocoma AG, Switzerland) | The Armeo®Spring device is an exoskeleton for upper limb rehabilitation. It is equipped with 7 goniometers and 1 pressure sensor, which permits free 3D arm movement. At the end of the robotic arm, there is a handle, which contains a pressure sensor, measuring the grip force. | The authors used the Armeo®Spring device to conduct a quantitative assessment of the precision, speed, and smoothness of upper limb motion. Among the several measures, the hand path ratio is the ratio between the actual path in the horizontal plane and the shortest-possible path, which reflects movement efficiency. The mean velocity and the number of peaks in the velocity profile were also assessed. Additionally, the normalized jerk (Norm Jerk), a measure of trajectory smoothness, was analyzed. |
| [31] | Armeo®Spring (Hocoma AG, Switzerland) | As described before | The Armeo®Spring was used to assess movement accuracy by measuring the hand path ratio, the mean velocity, and the number of peaks in the velocity profile. The authors concluded that the device should be integrated into the clinical evaluation of upper limb functions in post-stroke patients. |
| [32] | InMotion 2.0 (Bionik Laboratories, Watertown, MA, USA) | The InMotion 2.0 device is an end effector in which the subject moves their arm from a central target to 8 peripheral targets. | The authors assessed kinematic parameters of the upper limb, including elbow extension and shoulder flexion, abduction and external rotation of the shoulder, elbow flexion and shoulder extension, and adduction and internal rotation of the shoulder. These parameters, calculated at baseline, can assist clinicians in defining a rehabilitation program for post-stroke patients. |
| [33] | Gloreha Sinfonia (Idrogenet, Lumezzane BS, Italy –) | Gloreha Sinfonia is a robotic glove for hand rehabilitation to maintain range of motion (i.e., the flexion angle excursion of the finger metacarpophalangeal joints) of the patient’s hand. | The authors objectively evaluated hand movements using the Gloreha Sinfonia glove in order to customize rehabilitation sessions according to patients’ motor abilities. The angular values of the joints were assessed using bending sensors embedded in the glove. |
| Reference No. | Robotic Device | Description | Usefulness of Robot-Aided Motion Analysis |
|---|---|---|---|
| [46] | WelWalk (WW-2000, Toyota Motor Corporation, Aichi, Japan) | Knee-ankle-foot robot, low floor treadmill, safety suspension device for body weight support, monitor for patient use, 3D sensor, and control panel | Three-dimensional joint positions, lower limb tilt, and knee joint angle were recorded during a task using a 3D sensor, an inertial sensor, and a knee angle sensor. Two-dimensional joint positions collected using skeletal tracking software (VisionPose®, NEXT-SYSTEM Co., Ltd., Fukuoka, Japan) and depth data from the 3D sensor were used to estimate the three-dimensional coordinates of the joint positions. Bilateral hip, knee, ankle, and shoulder joints, as well as the midpoints of the shoulder and hip joints, were the predicted locations of the 3D joints. This objective gait analysis can be useful for individuals with hemiparetic stroke, as it provides individually tailored gait training based on these assessments. |
| [48] | Ekso (Ekso Bionics, San Rafael, CA 94901, USA) | Ekso a wearable unthethered exoskeleton. Motors power the hip and knee joints and all motion are started either through specific patient actions or the use of an external controller. | The authors conducted a comprehensive assessment by utilizing both kinematic and kinetic parameters, as well as EEG registrations, in patients with Parkinson’s disease. In this way, clinicians can personalize the rehabilitation treatment with a device that could increase the treatment intensity and dose without burdening therapists. |
| [49] | Ekso (Ekso Bionics, San Rafael, CA 94901, USA) | As described before | Muscle synergies and activation profiles were extracted using non-negative matrix factorization. The authors’ findings provided insights into the potential underlying mechanism for improving gait functions through exoskeleton-assisted locomotor training. |
| [50] | Lokomat (Hocoma AG, Switzerland) | The Lokomat is a robotic tethered exoskeleton with active hip–knee actuation and passive ankle control during the swing phase, in addition to a variable level of assistance. | The Lokomat was used to assess proprioception, which provides information about static position and movement sense, using custom software to measure joint position sense in the hip and knee. The authors demonstrated the usefulness of the Lokomat in measuring proprioception in SCI patients. |
| [51] | Lokomat (Hocoma AG, Switzerland) | As described before | The authors proved the Lokomat’s usefulness in objectively assessing proprioception at the hip and knee in people with SCI. |
| [52] | Lokomat (Hocoma AG, Switzerland) | As described before | Since lower limb kinesthesia deficits are common in SCI patients, the authors demonstrated that the Lokomat can serve as a valid and reliable robotic device for monitoring sensory function. Kinesthesia was evaluated using angular encoders of the hip and knee. During the analysis, a score was generated based on the difference between the initial angle and the final angle. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonanno, M.; Calabrò, R.S. Robot-Aided Motion Analysis in Neurorehabilitation: Benefits and Challenges. Diagnostics 2023, 13, 3561. https://doi.org/10.3390/diagnostics13233561
Bonanno M, Calabrò RS. Robot-Aided Motion Analysis in Neurorehabilitation: Benefits and Challenges. Diagnostics. 2023; 13(23):3561. https://doi.org/10.3390/diagnostics13233561
Chicago/Turabian StyleBonanno, Mirjam, and Rocco Salvatore Calabrò. 2023. "Robot-Aided Motion Analysis in Neurorehabilitation: Benefits and Challenges" Diagnostics 13, no. 23: 3561. https://doi.org/10.3390/diagnostics13233561