
Evolution of Fetal Cardiac Imaging over the Last 20 Years

 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Three-Dimensional Ultrasound with Spatiotemporal Image Correlation
3. HDlive
4. Fetal Intelligent Navigation Echocardiography “5D Heart”
5. Realistic Vue, Crystal Vue, and LumiFlow
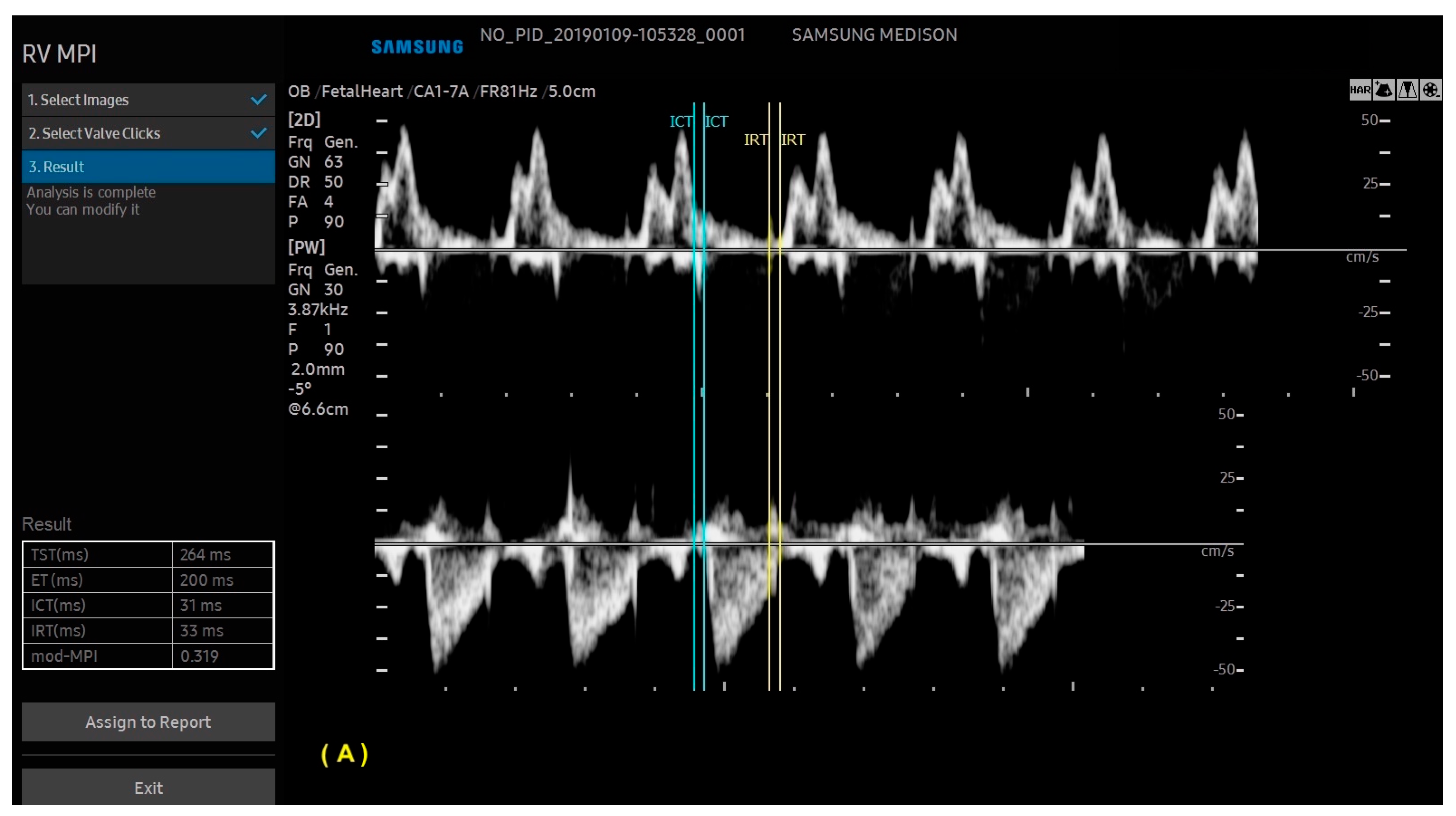
6. Artificial Intelligence
7. Isomerism
8. Atrioventricular Septal Defect
9. Tetralogy of Fallot
10. Transposition of the Great Arteries
11. Anomalous Venous Return
12. Right Aortic Arch
13. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meller, C.H.; Grinenco, S.; Aiello, H.; Córdoba, A.; Sáenz-Tejeira, M.M.; Marantz, P.; Otaño, L. Congenital heart disease, prenatal diagnosis and management. Arch. Argent. Pediatr. 2020, 118, e149–e161. [Google Scholar] [PubMed]
- Carvalho, J.S.; Axt-Fliedner, R.; Chaoui, R.; Copel, J.A.; Cuneo, B.F.; Goff, D.; Kopylov, L.G.; Hecher, K.; Lee, W.; Moon-Grady, A.J.; et al. ISUOG Practice Guidelines (updated): Fetal cardiac screening. Ultrasound Obstet. Gynecol. 2023, 61, 788–803. [Google Scholar] [CrossRef]
- DeVore, G.R.; Falkensammer, P.; Sklansky, M.S.; Platt, L.D. Spatio-temporal image correlation (STIC): New technology for evaluation of the fetal heart. Ultrasound Obstet. Gynecol. 2003, 22, 380–387. [Google Scholar] [CrossRef]
- Gonçalves, L.F.; Romero, R.; Espinoza, J.; Lee, W.; Treadwell, M.; Chintala, K.; Brandl, H.; Chaiworapongsa, T. Four-dimensional ultrasonography of the fetal heart using color Doppler spatiotemporal image correlation. J. Ultrasound Med. 2004, 23, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Viñals, F.; Ascenzo, R.; Naveas, R.; Huggon, I.; Giuliano, A. Fetal echocardiography at 11 + 0 to 13 + 6 weeks using four-dimensional spatiotemporal image correlation telemedicine via an Internet link: A pilot study. Ultrasound Obstet. Gynecol. 2008, 31, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Araujo Júnior, E.; Tonni, G.; Bravo-Valenzuela, N.J.; Da Silva Costa, F.; Meagher, S. Assessment of Fetal Congenital Heart Diseases by 4-Dimensional Ultrasound Using Spatiotemporal Image Correlation: Pictorial Review. Ultrasound Q. 2018, 34, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Hata, T.; Mashima, M.; Ito, M.; Uketa, E.; Mori, N.; Ishimura, M. Three dimensional HD live rendering images of the fetal heart. Ultrasound Med. Biol. 2013, 39, 1513–1517. [Google Scholar] [CrossRef]
- Hata, T.; AboEllail, M.A.M.; Sajapala, S.; Ishimura, M.; Masaoka, H. HDlive silhouette mode with spatiotemporal image correlation for assessment of the fetal heart. J. Ultrasound Med. 2016, 35, 1489–1495. [Google Scholar] [CrossRef]
- Hata, T.; Ito, M.; Nitta, E.; Pooh, R.; Sasahara, J.; Inamura, N. HDlive flow silhouette mode for diagnosis of ectopia cordis with a left ventricular diverticulum at 15 weeks’ gestation. J. Ultrasound Med. 2018, 37, 2465–2467. [Google Scholar] [CrossRef]
- Hata, T.; Koyanagi, A.; Yamanishi, T.; Bouno, S.; Takayoshi, R.; Miyagi, Y.; Miyake, T. Success rate of five fetal cardiac views using HDlive Flow with spatiotemporal image correlation at 18–21 and 28–31 weeks of gestation. J. Perinat Med 2020, 48, 384–388. [Google Scholar] [CrossRef]
- Yeo, L.; Romero, R. Fetal Intelligent Navigation Echocardiography (FINE): A novel method for rapid, simple, and automatic examination of the fetal heart. Ultrasound Obstet. Gynecol. 2013, 42, 268–284. [Google Scholar] [CrossRef] [PubMed]
- Yeo, L.; Romero, R.; Jodicke, C.; Kim, S.K.; Gonzalez, J.M.; Oggè, G.; Lee, W.; Kusanovic, J.P.; Vaisbuch, E.; Hassan, S. Simple targeted arterial rendering (STAR) technique: A novel and simple method to visualize the fetal cardiac outflow tracts. Ultrasound Obstet. Gynecol. 2011, 37, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Rocha, L.A.; Rolo, L.C.; Barros, F.S.B.; Nardozza, L.M.M.; Moron, A.F.; Júnior, E.A. Assessment of Quality of Fetal Heart Views by 3D/4D Ultrasonography Using Spatio-Temporal Image Correlation in the Second and Third Trimesters of Pregnancy. Echocardiography 2015, 32, 1015–1021. [Google Scholar] [CrossRef]
- Espinoza, J.; Lee, W.; Romero, R.; Yeo, L.; Rizzo, G.; Paladini, D.; Viñals, F.; Achiron, R.; Gindes, L.; Abuhamad, A.; et al. Collaborative study on 4-dimensional echocardiography for the diagnosis of fetal heart defects: The COFEHD study. J. Ultrasound Med. 2010, 29, 1573–1580. [Google Scholar] [CrossRef] [PubMed]
- Bennasar, M.; Martínez, J.M.; Gómez, O.; Bartrons, J.; Olivella, A.; Puerto, B.; Gratacós, E. Accuracy of four-dimensional spatiotemporal image correlation echocardiography in the prenatal diagnosis of congenital heart defects. Ultrasound Obstet. Gynecol. 2010, 36, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Uittenbogaard, L.B.; Haak, M.C.; Spreeuwenberg, M.D.; Van Vugt, J.M.G. A systematic analysis of the feasibility of four-dimensional ultrasound imaging using spatiotemporal image correlation in routine fetal echocardiography. Ultrasound Obstet. Gynecol. 2008, 31, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, L.F.; Espinoza, J.; Lee, W.; Nien, J.K.; Hong, J.S.; Santolaya-Forgas, J.; Mazor, M.; Romero, R. A new approach to fetal echocardiography: Digital casts of the fetal cardiac chambers and great vessels for detection of congenital heart disease. J. Ultrasound Med. 2005, 24, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Rolo, L.C.; Santana, E.F.M.; da Silva, P.H.; Costa, F.D.S.; Nardozza, L.M.M.; Tonni, G.; Moron, A.F.; Júnior, E.A. Fetal cardiac interventricular septum: Volume assessment by 3D/4D ultrasound using spatio-temporal image correlation (STIC) and virtual organ computer-aided analysis (VOCAL). J. Matern. Fetal Neonatal Med. 2015, 28, 1388–1393. [Google Scholar] [CrossRef]
- Xiong, Y.; Liu, T.; Wu, Y.; Xu, J.F.; Ting, Y.H.; Yeung Leung, T.; Lau, T.K. Comparison of real-time three-dimensional echocardiography and spatiotemporal image correlation in assessment of fetal interventricular septum. J. Matern. Fetal Neonatal Med. 2012, 25, 2333–2338. [Google Scholar] [CrossRef]
- Adriaanse, B.M.; Uittenbogaard, L.B.; Tromp, C.H.; Heymans, M.W.; van Vugt, J.M.; Haak, M.C. Prenatal Visualization of the Pulmonary and Aortic Valves and Leaflets Is Feasible Using 4-Dimensional Sonography. J. Ultrasound Med. 2016, 35, 497–504. [Google Scholar] [CrossRef]
- Rolo, L.C.; Rizzo, G.; Pietrolucci, M.E.; Barros, F.S.B.; Nardozza, L.M.M.; Martins, W.P.; Arduini, D.; Moron, A.F.; Júnior, E.A. Viewing rate and reference ranges for papillary muscle areas of the fetal heart using four-dimensional ultrasound in the rendering mode. Prenat. Diagn. 2014, 34, 1153–1160. [Google Scholar] [CrossRef]
- Rolo, L.C.; Pietrolucci, M.E.; Araujo Júnior, E.; Barros, F.S.B.; Nardozza, L.M.M.; Martins, W.P.; Moron, A.F.; Arduin, D.; Rizzo, G. Viewing rate and reproducibility of papillary muscle areas in foetal atrioventricular valves using spatio-temporal image correlation in the rendering mode in congenital heart disease. J. Matern. Neonatal Med. 2015, 28, 1375–1380. [Google Scholar] [CrossRef] [PubMed]
- Lima, A.I.F.; Júnior, E.A.; Martins, W.P.; Nardozza, L.M.M.; Moron, A.F.; Pares, D.B.S. Assessment of the fetal heart at 12–14 weeks of pregnancy using B-mode, color Doppler, and spatiotemporal image correlation via abdominal and vaginal ultrasonography. Pediatr. Cardiol. 2013, 34, 1577–1582. [Google Scholar] [CrossRef] [PubMed]
- Lei, W.; Ying, Z.; Ailu, C.; Xiaoguang, W. Evaluation of normal fetal ductus venosus using B-flow imaging with spatiotemporal image correlation and traditional color Doppler echocardiography. Echocardiography 2015, 32, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Zhang, Y.; Zhou, X.; Wang, Y.; Sun, W.; Chen, L.; Zhao, D.; Cai, A. Four-dimensional echocardiography with spatiotemporal image correlation and inversion mode for detection of congenital heart disease. Ultrasound Med. Biol. 2014, 40, 1434–1441. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.; Capponi, A.; Vendola, M.; Pietrolucci, M.E.; Arduini, D. Role of tomographic ultrasound imaging with spatiotemporal image correlation for identifying fetal ventricular septal defects. J. Ultrasound Med. 2008, 27, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Messing, B.; Cohen, S.M.; Valsky, D.V.; Rosenak, D.; Hochner-Celnikier, D.; Savchev, S.; Yagel, S. Fetal cardiac ventricle volumetry in the second half of gestation assessed by 4D ultrasound using STIC combined with inversion mode. Ultrasound Obstet. Gynecol. 2007, 30, 142–151. [Google Scholar] [CrossRef] [PubMed]
- DeKoninck, P.; Steenhaut, P.; Van Mieghem, T.; Mhallem, M.; Richter, J.; Bernard, P.; De Catte, L.; Deprest, J. Comparison of Doppler-based and three-dimensional methods for fetal cardiac output measurement. Fetal Diagn Ther. 2012, 32, 72–78. [Google Scholar] [CrossRef]
- Bravo-Valenzuela, N.J.; Peixoto, A.B.; Mattar, R.; Júnior, J.F.M.; Pares, D.B.d.S.; Júnior, E.A. Fetal Cardiac Function and Ventricular Volumes Determined by Three-Dimensional Ultrasound Using STIC and VOCAL Methods in Fetuses from Pre-gestational Diabetic Women. Pediatr. Cardiol. 2020, 41, 1125–1134. [Google Scholar] [CrossRef]
- Júnior, J.F.M.; Bravo-Valenzuela, N.J.; Nardozza, L.M.M.; Peixoto, A.B.; Mattar, R.; Martins, W.P.; Pares, D.B.d.S.; Júnior, E.A. References Values of Fetal Heart Myocardial Volume by Three-Dimensional Ultrasound using Spatiotemporal Image Correlation and Virtual Organ Computer-Aided Analysis Methods and Their Applicability in Pregestational Diabetic Women. Am. J. Perinatol. 2021, 38, 721–727. [Google Scholar] [CrossRef]
- Ito, M.; AboEllail, M.A.M.; Yamamoto, K.; Kanenishi, K.; Tanaka, H.; Masaoka, H.; Hata, T. HDlive Flow silhouette mode and spatiotemporal image correlation for diagnosing congenital heart disease. Ultrasound Obstet. Gynecol. 2017, 50, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Malho, A.S.; Bravo-Valenzuela, N.J.; Ximenes, R.; Peixoto, A.B.; Araujo Júnior, E. Antenatal diagnosis of congenital heart disease by 3D ultrasonography using spatiotemporal image correlation with HDlive Flow and HDlive Flow silhouette rendering modes. Ultrasonography 2022, 41, 578–596. [Google Scholar] [CrossRef] [PubMed]
- Hata, T.; AboEllail, M.A.M.; Sajapala, S.; Ito, M. HDliveFlow in the assessment of fetal circulation. Donald School J. Ultrasound Obstet. Gynecol. 2015, 9, 462–470. [Google Scholar]
- Li, T.G.; Su, X.R.; Wu, W.R.; Zhang, W.D.; Ma, B. Prenatal diagnosis of fetal conotruncal defects by using 2D ultrasound and HD live flow combined with spatiotemporal image correlation. J. Clin. Ultrasound 2023, 51, 1166–1171. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Shao, Q.; Sun, L.; Ge, S.; He, Y. Prenatal diagnosis of total anomalous pulmonary venous connection by 2D and 3D fetal echocardiography. Echocardiography 2017, 34, 1852–1857. [Google Scholar] [CrossRef] [PubMed]
- Carrilho, M.C.; Rolo, L.C.; Tonni, G.; Araujo Júnior, E. Assessment of the quality of fetal heart standard views using the FAST, STAR, and FINE four-dimensional ultrasound techniques in the screening of congenital heart diseases. Echocardiography 2020, 37, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Yeo, L.; Romero, R. Color and power Doppler combined with Fetal Intelligent Navigation Echocardiography (FINE) to evaluate the fetal heart. Ultrasound Obstet. Gynecol. 2017, 50, 476–491. [Google Scholar] [CrossRef]
- Pappalardo, E.; Gulino, F.A.; Ettore, C.; Cannone, F.; Ettore, G. Body Stalk Anomaly Complicated by Ectopia Cordis: First-Trimester Diagnosis of Two Cases Using 2- and 3-Dimensional Sonography. J. Clin. Med. 2023, 12, 1896. [Google Scholar] [CrossRef]
- Dall’Asta, A.; Grisolia, G.; Volpe, N.; Schera, G.; Sorrentino, F.; Frusca, T.; Ghi, T. Prenatal visualization of the torcular herophili by means of a Doppler technology highly sensitive for low-velocity flow in the expert assessment of the posterior fossa: A prospective study. BJOG 2021, 128, 347–352. [Google Scholar] [CrossRef]
- Day, T.G.; Kainz, B.; Hajnal, J.; Razavi, R.; Simpson, J.M. Artificial intelligence, fetal echocardiography, and congenital heart disease. Prenat. Diagn. 2021, 41, 733–742. [Google Scholar] [CrossRef]
- Rizzo, G.; Pietrolucci, M.E.; Capponi, A.; Mappa, I. Exploring the role of artificial intelligence in the study of fetal heart. Int. J. Cardiovasc. Imaging 2022, 38, 1017–1019. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Wu, B.; Lai, F.; Liu, P.; Lyu, G.; He, S.; Dai, J. Application of Artificial Intelligence in Anatomical Structure Recognition of Standard Section of Fetal Heart. Comput. Math. Methods Med. 2023, 2023, 5650378. [Google Scholar] [CrossRef] [PubMed]
- Truong, V.T.; Nguyen, B.P.; Nguyen-Vo, T.-H.; Mazur, W.; Chung, E.S.; Palmer, C.; Tretter, J.T.; Alsaied, T.; Pham, V.T.; Do, H.Q.; et al. Application of machine learning in screening for congenital heart diseases using fetal echocardiography. Int. J. Cardiovasc. Imaging 2022, 38, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Scharf, J.L.; Dracopoulos, C.; Gembicki, M.; Welp, A.; Weichert, J. How Automated Techniques Ease Functional Assessment of the Fetal Heart: Applicability of MPI+™ for Direct Quantification of the Modified Myocardial Performance Index. Diagnostics 2023, 13, 1705. [Google Scholar] [CrossRef] [PubMed]
- Sheley, R.C.; A Nyberg, D.; Kapur, R. Azygous continuation of the interrupted inferior vena cava: A clue to prenatal diagnosis of the cardiosplenic syndromes. J. Ultrasound Med. 1995, 14, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Bronshtein, M.; Gover, A.; Zimmer, E.Z. Sonographic definition of the fetal situs. Obstet. Gynecol. 2002, 99, 1129–1130. [Google Scholar] [PubMed]
- Anderson, R.H.; Shirali, G. Sequential segmental analysis. Ann. Pediatr. Cardiol. 2009, 2, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Veronese, P.; Guariento, A.; Cattapan, C.; Fedrigo, M.; Gervasi, M.T.; Angelini, A.; Riva, A.; Vida, V. Prenatal Diagnosis and Fetopsy Validation of Complete Atrioventricular Septal Defects Using the Fetal Intelligent Navigation Echocardiography Method. Diagnostics 2023, 13, 456. [Google Scholar] [CrossRef]
- Anderson, R.H.; Spicer, D.E.; Giroud, J.M.; Mohun, T.J. Tetralogy of Fallot: Nosological, morphological, and morphogenetic considerations. Cardiol. Young 2013, 23, 858–866. [Google Scholar] [CrossRef]
- Sharma, R.; Niederhoffer, K.Y.; Caluseriu, O.; Cooke, C.; Hornberger, L.K.; He, R.; Eckersley, L.; Lin, L.; Rushfeldt, M.; McBrien, A. Extra-cardiac diagnoses and postnatal outcomes of fetal tetralogy of fallot. Prenat. Diagn. 2022, 42, 260–266. [Google Scholar] [CrossRef]
- Yoo, S.J.; Lee, Y.-H.; Kim, E.S.; Ryu, H.M.; Kim, M.Y.; Choi, H.-K.; Cho, K.S.; Kim, A. Three-vessel view of the fetal upper mediastinum: An easy means of detecting abnormalities of the ventricular outflow tracts and great arteries during obstetric screening. Ultrasound Obstet. Gynecol. 1997, 9, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Martínez, J.M.; Gómez, O.; Bennasar, M.; Olivella, A.; Crispi, F.; Puerto, B.; Gratacós, E. The ‘question mark’ sign as a new ultrasound marker of tetralogy of Fallot in the fetus. Ultrasound Obstet. Gynecol. 2010, 36, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, I.; Jehle, C.; Herberg, U.; Breuer, J.; Brockmeier, K.; Bennink, G.; Hellmund, A.; Strizek, B.; Gembruch, U.; Geipel, A.; et al. Prenatal diagnosis of absent pulmonary valve syndrome from first trimester onwards: Novel insights into pathophysiology, associated conditions and outcome. Ultrasound Obstet. Gynecol. 2017, 49, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Manzano, P.; Mendoza, A.; Herraiz, I.; Escribano, D.; Román, V.; Aguilar, J.M.; Galindo, A. Transposition of the Great Arteries in Fetal Life: Accuracy of Diagnosis and Short-Term Outcome. Fetal Diagn Ther. 2016, 40, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.; Capponi, A.; Cavicchioni, O.; Vendola, M.; Pietrolucci, M.E.; Arduini, D. Application of automated sonography on 4-dimensional volumes of fetuses with transposition of the great arteries. J. Ultrasound Med. 2008, 27, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Shih, J.C.; Shyu, M.K.; Su, Y.N.; Chiang, Y.C.; Lin, C.H.; Lee, C.N. ‘Big-eyed frog’ sign on spatiotemporal image correlation (STIC) in the antenatal diagnosis of transposition of the great arteries. Ultrasound Obstet. Gynecol. 2008, 32, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Valenzuela, N.J.M.; Peixoto, A.B.; Júnior, E.A. Prenatal diagnosis of total anomalous pulmonary venous connection: 2D and 3D echocardiographic findings. J. Clin. Ultrasound 2021, 49, 240–247. [Google Scholar] [CrossRef]
- Galindo, A.; Nieto, O.; Nieto, M.T.; Rodríguez-Martín, M.O.; Herraiz, I.; Escribano, D.; Granados, M.A. Prenatal diagnosis of right aortic arch: Associated findings, pregnancy outcome, and clinical significance of vascular rings. Prenat. Diagn. 2009, 29, 975–981. [Google Scholar] [CrossRef]





























Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magioli Bravo-Valenzuela, N.J.; Malho, A.S.; Nieblas, C.d.O.; Castro, P.T.; Werner, H.; Araujo Júnior, E. Evolution of Fetal Cardiac Imaging over the Last 20 Years. Diagnostics 2023, 13, 3509. https://doi.org/10.3390/diagnostics13233509
Magioli Bravo-Valenzuela NJ, Malho AS, Nieblas CdO, Castro PT, Werner H, Araujo Júnior E. Evolution of Fetal Cardiac Imaging over the Last 20 Years. Diagnostics. 2023; 13(23):3509. https://doi.org/10.3390/diagnostics13233509
Chicago/Turabian StyleMagioli Bravo-Valenzuela, Nathalie Jeanne, André Souza Malho, Caroline de Oliveira Nieblas, Pedro Teixeira Castro, Heron Werner, and Edward Araujo Júnior. 2023. "Evolution of Fetal Cardiac Imaging over the Last 20 Years" Diagnostics 13, no. 23: 3509. https://doi.org/10.3390/diagnostics13233509