
Antibody Response to SARS-CoV-2 Vaccination in Heart Failure Patients: Retrospective Single-Center Cohort Study
 , , , ,
, , , ,
Abstract
:1. Introduction
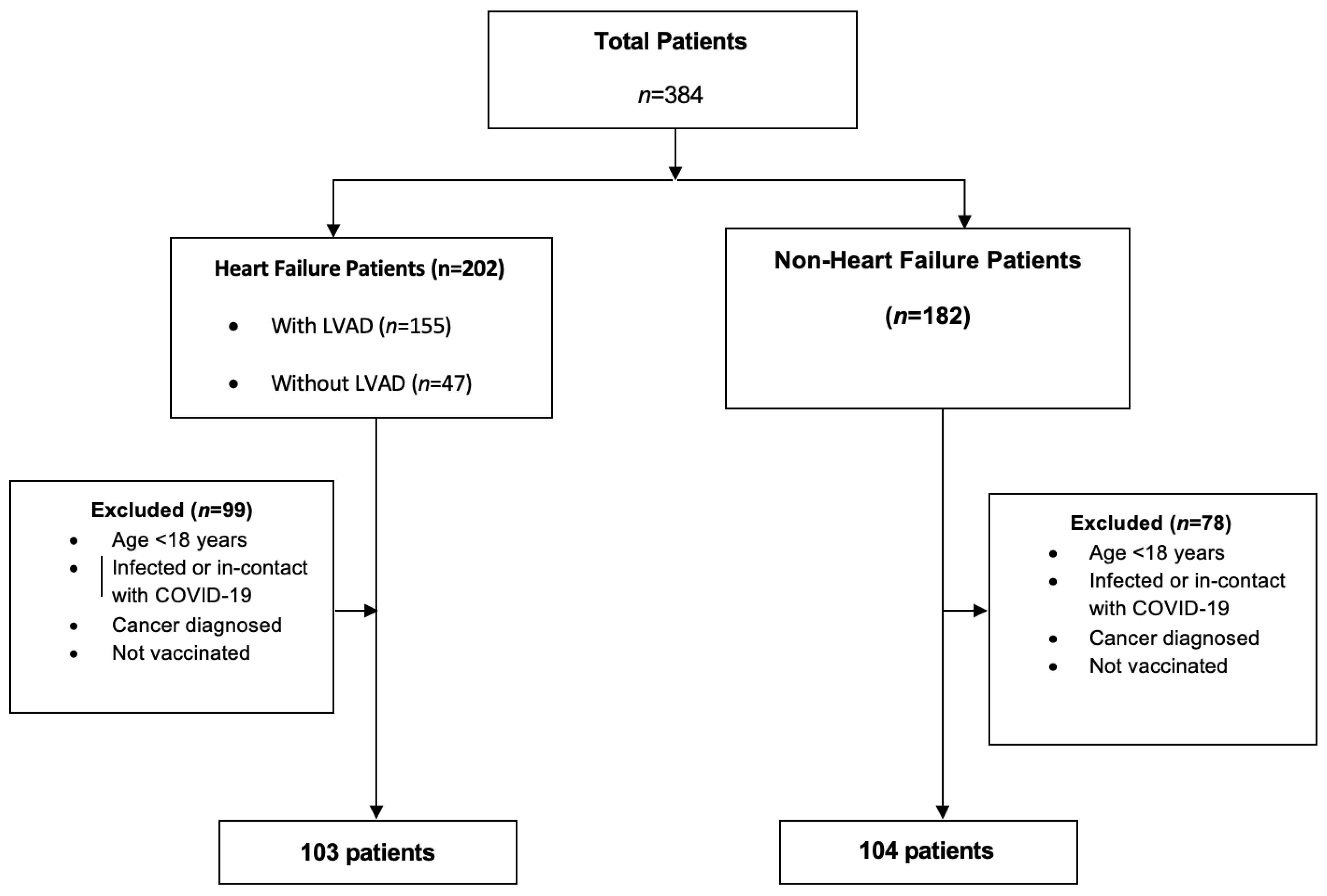
2. Materials and Methods
2.1. Data Collection and Measures
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Anti-Spike Antibody Positivity
3.3. Anti-Spike Antibody Levels with Different Vaccines
3.4. Anti-Spike Antibody Levels with Different Time Intervals from the Last Vaccine Dose
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mok, C.K.P.; Cohen, C.A.; Cheng, S.M.; Chen, C.; Kwok, K.O.; Yiu, K.; Chan, T.O.; Bull, M.; Ling, K.C.; Dai, Z.; et al. Comparison of the immunogenicity of BNT162b2 and CoronaVac COVID-19 vaccines in Hong Kong. Respirology 2022, 27, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Gao, Q.; Bao, L.; Mao, H.; Wang, L.; Xu, K.; Yang, M.; Li, Y.; Zhu, L.; Wang, N.; Lv, Z.; et al. Development of an inactivated vaccine candidate for SARS-CoV-2. Science 2020, 369, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Tanriover, M.D.; Doğanay, H.L.; Akova, M.; Güner, H.R.; Azap, A.; Akhan, S.; Erdinç, F.; Akalın, E.H.; Tabak, Ö.F.; Pullukçu, H.; et al. Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac): Interim results of a double-blind. randomized. placebo-controlled. phase 3 trial in Turkey. Lancet 2021, 398, 213–222. [Google Scholar] [CrossRef]
- Clark, D.J.; Cleman, M.W.; Pfau, S.E.; Rollins, S.A.; Ramahi, T.M.; Mayer, C.; Caulin-Glaser, T.; Daher, E.; Kosiborod, M.; Bell, L.; et al. Serum complement activation in congestive heart failure. Am. Heart J. 2001, 141, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Torre-Amione, G. Immune activation in chronic heart failure. Am. J. Cardiol. 2005, 95, 3C–8C. [Google Scholar] [CrossRef]
- Itescu, S.; Ankersmit, J.H.; Kocher, A.A.; Schuster, M.D. Immunobiology of left ventricular assist devices. Prog. Cardiovasc. Dis. 2000, 43, 67–80. [Google Scholar] [CrossRef]
- Fast, H.E.; Zell, E.; Murthy, B.P.; Murthy, N.; Meng, L.; Scharf, L.G.; Black, C.L.; Shaw, L.; Chorba, T.; Harris, L.T. Booster and Additional Primary Dose COVID-19 Vaccinations Among Adults Aged ≥ 65 Years—United States. August 13. 2021-November 19. 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1735–1739. [Google Scholar] [CrossRef]
- EUROIMMUN. Medizinische Labordiagnostika AG. “SARS-CoV-2 Infection/COVID-19 Diagnostics”. 2021. Available online: www.coronavirus-diagnostics.com/documents/Indications/Infections/Coronavirus/EI_2606_D_UK_E.pdf (accessed on 27 October 2023).
- Al Kaabi, N.; Oulhaj, A.; Al Hosani, F.I.; Al Mazrouei, S.; Najim, O.; Hussen, S.E.; Abdalla, J.S.; Fasihuddin, M.S.; Hassan, A.A.; Elghazali, G.; et al. The incidence of COVID-19 infection following emergency use authorization of BBIBP-CORV inactivated vaccine in frontline workers in the United Arab Emirates. Sci. Rep. 2022, 12, 490. [Google Scholar] [CrossRef]
- Meo, S.A.; Al-Khlaiwi, T.; Usmani, A.M.; Meo, A.S.; Klonoff, D.C.; Hoang, T.D. Biological and Epidemiological Trends in the Prevalence and Mortality due to Outbreaks of Novel Coronavirus COVID-19. J. King Saud. Univ. Sci. 2020, 32, 2495–2499. [Google Scholar] [CrossRef]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective. multicentre. cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Rosano, G.; Jankowska, E.A.; Ray, R.; Metra, M.; Abdelhamid, M.; Adamopoulos, S.; Bayes-Genis, A.; Belenkov, Y.; Ben Gal, T.; Böhm, M.; et al. COVID-19 vaccination in patients with heart failure: A position paper of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2021, 23, 1806–1818. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Deng, Y.; Zhao, Z.; Mao, B.; Lu, M.; Lin, Y.; Huang, A. Characterization of SARS-CoV-2-specific humoral immunity and its potential applications and therapeutic prospects. Cell Mol. Immunol. 2022, 19, 150–157. [Google Scholar] [CrossRef]
- Goel, R.R.; Painter, M.M.; Apostolidis, S.A.; Mathew, D.; Meng, W.; Rosenfeld, A.M.; Lundgreen, K.A.; Reynaldi, A.; Khoury, D.S.; Pattekar, A.; et al. mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science 2021, 374, abm0829. [Google Scholar] [CrossRef]
- Sun, Z.; Wu, T.; Xie, H.; Li, Y.; Zhang, J.; Su, X.; Qi, H. The Role of Cellular Immunity in the Protective Efficacy of the SARS-CoV-2 Vaccines. Vaccines 2022, 10, 1103. [Google Scholar] [CrossRef]
- Notarangelo, L.; Casanova, J.L.; Fischer, A.; Puck, J.; Rosen, F.; Seger, R.; Geha, R. Primary Immunodeficiency Diseases: An Update. J. Allergy Clin. Immunol. 2004, 114, 677–687. [Google Scholar] [CrossRef]
- Seidel, M.G.; Kindle, G.; Gathmann, B.; Quinti, I.; Buckland, M.; van Montfrans, J.; Scheible, R.; Rusch, S.; Gasteiger Cm, L.M.; Grimbacher, B.; et al. The European Society for Immunodeficiencies (ESID) Registry Working Definitions for the Clinical Diagnosis of Inborn Errors of Immunity. J. Allergy Clin. Immunol. Pract. 2019, 7, 1763–1770. [Google Scholar] [CrossRef] [PubMed]
- Cunningham-Rundles, C. How I Treat Common Variable Immune Deficiency. Blood 2010, 116, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Maniar, S.; Kondareddy, S.; Topkara, V.K. Left ventricular assist device-related infections: Past. present and future. Expert. Rev. Med. Devices 2011, 8, 627–634. [Google Scholar] [CrossRef]
- Itzhaki Ben Zadok, O.; Shaul, A.A.; Ben-Avraham, B.; Yaari, V.; Ben Zvi, H.; Eliakim-Raz, N.; Abed, G.; Abuhazira, M.; Barac, Y.D.; Mats, I.; et al. Six-months immunogenicity of BNT162b2 mRNA vaccine in heart transplanted and ventricle assist device-supported patients. ESC Heart Fail. 2022, 9, 905–911. [Google Scholar] [CrossRef]
- Laing, E.D.; Weiss, C.D.; Samuels, E.C.; Si’Ana, A.C.; Wang, W.; Wang, R.; Vassel, R.; Sterling, S.L.; Tso, M.S.; Conner, T.; et al. Durability of Antibody Response and Frequency of SARS-CoV-2 Infection 6 Months after COVID-19 Vaccination in Healthcare Workers. Emerg. Infect. Dis. 2022, 28, 828–832. [Google Scholar] [CrossRef] [PubMed]
- Steensels, D.; Pierlet, N.; Penders, J.; Mesotten, D.; Heylen, L. Comparison of SARS-CoV-2 Antibody Response Following Vaccination With BNT162b2 and mRNA-1273. JAMA 2021, 326, 1533–1535. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.; Guan, W.; Staggs, R.; Hamel, A.; Hozayen, S.; Adhikari, N.; Grindle, S.; Desir, S.; John, R.; Hall, J.L.; et al. Identification of differentially expressed transcripts and pathways in blood one week and six months following implant of left ventricular assist devices. PLoS ONE 2013, 8, e77951. [Google Scholar] [CrossRef] [PubMed]
- Globerson, A.E.; Effros, R.B. Ageing of lymphocytes and lymphocytes in the aged. Immunol. Today 2000, 21, 515–521. [Google Scholar] [CrossRef]
- Graves, D.T.; Kayal, R.A. Diabetic complications and dysregulated innate immunity. Front. Biosci. 2008, 13, 1227–1239. [Google Scholar] [CrossRef] [PubMed]
- Tall, A.R.; Yvan-Charvet, L. Cholesterol, inflammation and innate immunity. Nat. Rev. Immunol. 2015, 15, 104–116. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions, and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim(s) responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |




{kind=link}
{kind=link}
{kind=link}
| Variable | Heart Failure (n = 103) | Non-Heart Failure (n = 104) | p Value |
|---|---|---|---|
| Age, years, median (Q1–Q3) | 56.0 (48.0–62.5) | 63.0 (56.0–70.2) | <0.001 1 |
| Hypertension | 40 (38.8%) | 64 (61.5%) | 0.001 2 |
| Diabetes | 22 (21.3%) | 43 (41.3%) | 0.002 2 |
| Hyperlipidemia | 15 (14.5%) | 47 (45.1%) | <0.001 2 |
| Gender | 0.840 2 | ||
| Female | 25 (24.3%) | 24 (23.1%) | |
| Male | 78 (75.7%) | 80 (76.9%) | |
| Vaccine | 0.002 2 | ||
| BNT162b2 | 21 (20.8%) | 35 (33.6%) | |
| CoronaVac | 39 (37.8%) | 17 (16.3%) | |
| Heterologous (CoronaVac and BNT162b2) | 43 (41.7%) | 52 (50.3%) | |
| Period *, Days, Median (Q1–Q3) | 118.0 (83.5–140.0) | 130.5 (97.8–162.0) | 0.040 1 |
| Procedure | |||
| Isolated CABG | 65 (62.5%) | ||
| Single MVR | 4 (3.8%) | ||
| Single AVR | 10 (9.6%) | ||
| Single TVR | 1 (0.9%) | ||
| ASD Repair | 1 (0.9%) | ||
| Septal Myectomy | 1 (0.9%) | ||
| Bentall Procedure | 3 (2.8%) | ||
| CABG with AVR | 4 (3.8%) | ||
| CABG with MVR | 1 (0.9%) | ||
| CABG with CEA | 2 (1.9%) | ||
| Double-Valve Operation | 8 (7.6%) | ||
| Triple-Valve Operation | 1 (0.9%) | ||
| CABG with Ascending Aorta Replacement | 2 (1.9%) | ||
| Etiology of Heart Failure | |||
| ICMP | 48 (46.6%) | ||
| DCMP | 50 (48.5%) | ||
| RCMP | 2 (1.9%) | ||
| HCMP | 4 (3.8%) | ||
| Ventricular Assist Device | |||
| Abbott HeartMate 2 | 5 (5.8%) | ||
| Abbott HeartMate 3 | 19 (22%) | ||
| Medtronic HeartWare HVAD | 62 (72%) |
| B | S.E. | p Value | OR | 95% C.I. | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Model 1 | ||||||
| Hyperlipidemia (Reference Category: No) | 1.550 | 0.540 | 0.004 | 4.711 | 1.635 | 13.575 |
| Period * | −0.021 | 0.006 | 0.001 | 0.979 | 0.967 | 0.991 |
| Vaccine Group (Reference Category: CoronaVac) | ||||||
| BNT162b2 | 2.403 | 0.535 | <0.001 | 11.059 | 3.877 | 31.549 |
| Heterologous (CoronaVac and BNT162b2) | 3.274 | 0.560 | <0.001 | 26.412 | 8.810 | 79.189 |
| Model 2 ** | ||||||
| Heart Failure (Reference Category: Non-Heart Failure) | 0.437 | 1.240 | 0.725 | 1.548 | 0.136 | 17.602 |
| Heart Failure * Period (Reference Category: Non-Heart Failure) | 0.003 | 0.008 | 0.727 | 1.003 | 0.987 | 1.019 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ergi, D.G.; Kahraman, Ü.; Akkuş, G.; Durmaz, S.; Balcıoğlu, Ö.; Engin, Ç.; Yağmur, B.; Nalbantgil, S.; Çiçek, C.; Özbaran, M.; et al. Antibody Response to SARS-CoV-2 Vaccination in Heart Failure Patients: Retrospective Single-Center Cohort Study. Diagnostics 2023, 13, 3460. https://doi.org/10.3390/diagnostics13223460
Ergi DG, Kahraman Ü, Akkuş G, Durmaz S, Balcıoğlu Ö, Engin Ç, Yağmur B, Nalbantgil S, Çiçek C, Özbaran M, et al. Antibody Response to SARS-CoV-2 Vaccination in Heart Failure Patients: Retrospective Single-Center Cohort Study. Diagnostics. 2023; 13(22):3460. https://doi.org/10.3390/diagnostics13223460
Chicago/Turabian StyleErgi, Defne Güneş, Ümit Kahraman, Gözde Akkuş, Seyfi Durmaz, Özlem Balcıoğlu, Çağatay Engin, Burcu Yağmur, Sanem Nalbantgil, Candan Çiçek, Mustafa Özbaran, and et al. 2023. "Antibody Response to SARS-CoV-2 Vaccination in Heart Failure Patients: Retrospective Single-Center Cohort Study" Diagnostics 13, no. 22: 3460. https://doi.org/10.3390/diagnostics13223460