
Assessment of UTI Diagnostic Techniques Using the Fuzzy–PROMETHEE Model
 ,
,
Abstract
:1. Introduction
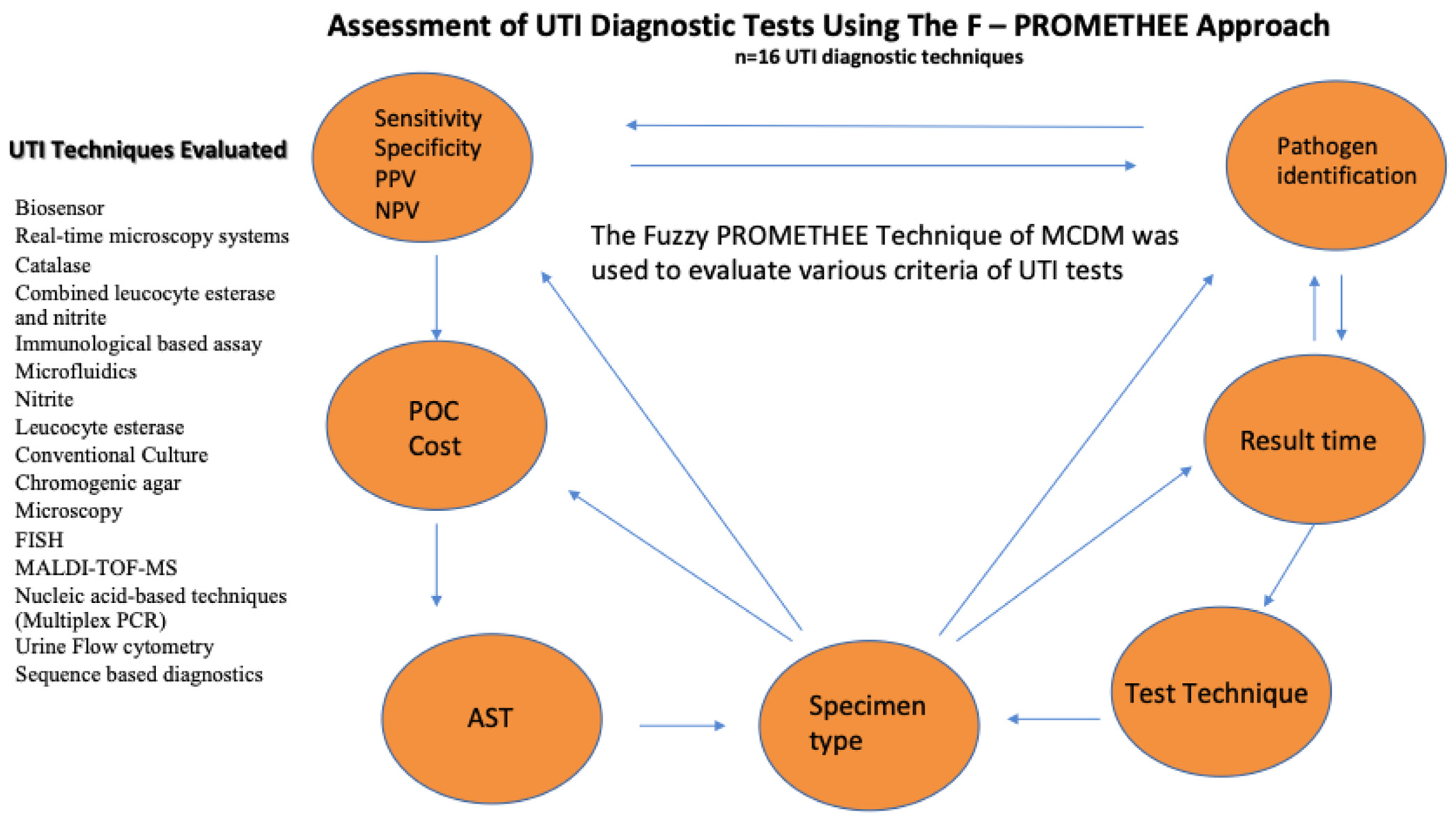
- Discussing detailed features of UTI tests, determining their advantages and disadvantages, and evaluating them analytically for potential enhancements of decision points;
- Guiding the decision makers in deciding the most appropriate and accurate UTI test;
- Applicability of current mathematical approaches in evaluating the test performances used in the diagnosis of infectious diseases.
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moghadam, H.Z.; Maleki, F.; Ebrahimi, M.; Foroughian, M. Evaluating the diagnostic value of nitrite test in comparison with U/S results in patients with urinary tract infection symptoms: A cross-sectional study. J. Emerg. Pract. Trauma 2020, 6, 13–17. [Google Scholar] [CrossRef]
- Ejrnæs, K. Bacterial Characteristics of Importance for Recurrent Urinary Tract Infections Caused by Escherichia coli. J. Dan. Med. Bull. 2011, 58, 4187. [Google Scholar]
- Foxman, B.; Frerichs, R. Epidemiology of urinary tract infection: I. Diaphragm use and sexual intercourse. Am. J. Public Health 1985, 75, 1308–1313. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.; Mach, K.E.; Shortliffe, L.M.D.; Banaei, N.; Wang, T.H.; Liao, J.C. New and developing diagnostic technologies for urinary tract infections. Nat. Rev. Urol. 2017, 14, 296–310. [Google Scholar] [CrossRef]
- Services, H. Department of Health & Human Services. 2017. Available online: https://www.hhs.gov/sites/default/files/2017-hhs-computer-matching-report-final-omb-submitted.pdf (accessed on 8 May 2023).
- Waisman, Y.; Zerem, E.; Amir, L.; Mimouni, M. The validity of the uriscreen test for early detection of urinary tract infection in children. Pediatrics 1999, 104, e41. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.H.; Zhang, G.; Fan, Y.Y.; Yang, X.; Sui, W.J.; Lu, X.X. Direct identification of bacteria causing urinary tract infections by combining matrix-assisted laser desorption ionization-time of flight mass spectrometry with UF-1000i urine flow cytometry. J. Microbiol. Methods 2013, 92, 231–235. [Google Scholar] [CrossRef]
- Reyes, S.; Le, M.D.; Fuentes, N.; Upegui, J.; Dikici, E.; Broyles, D.; Deo, S.K. An intact cell bioluminescence-based assay for the simple and rapid diagnosis of urinary tract infection. Int. J. Mol. Sci. 2020, 21, 5015. [Google Scholar] [CrossRef]
- Foxman, B. The epidemiology of urinary tract infection. Nat. Rev. Urol. 2020, 7, 653–660. [Google Scholar] [CrossRef]
- Moshaver, B.; de Boer, F.; van Egmond-Kreileman, H.; Kramer, E.; Stegeman, C.; Groeneveld, P. Fast and accurate prediction of positive and negative urine cultures by flow cytometry. BMC Infect. Dis. 2016, 16, 211. [Google Scholar] [CrossRef]
- Broeren, M.A.; Bahçeci, S.; Vader, H.L.; Arents, N.L. Screening for urinary tract infection with the Sysmex UF-1000i urine flow cytometer. J. Clin. Microbiol. 2011, 49, 1025–1029. [Google Scholar] [CrossRef] [PubMed]
- Fredborg, M.; Rosenvinge, F.S.; Spillum, E.; Kroghsbo, S.; Wang, M.; Sondergaard, T.E. Rapid antimicrobial susceptibility testing of clinical isolates by digital time-lapse microscopy. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 2385–2394. [Google Scholar] [CrossRef] [PubMed]
- Mach, K.E.; Wong, P.K.; Liao, J.C. Biosensor diagnosis of urinary tract infections: A path to better treatment? Trends Pharmacol. Sci. 2011, 32, 330–336. [Google Scholar] [CrossRef]
- Anwer, R.; Darami, H.; Almarri, F.K.; Albogami, M.A.; Alahaydib, F. MALDI-TOF MS for rapid analysis of bacterial pathogens causing urinary tract infections in the Riyadh region. Diseases 2022, 10, 78. [Google Scholar] [CrossRef] [PubMed]
- Da, T.N.T.; Yoon, J.; Jin, C.E.; Koo, B.; Han, K.; Shin, Y.; Lee, T.Y. Rapid and sensitive detection of Salmonella based on microfluidic enrichment with a label-free nano biosensing platform. Sens. Actuators B Chem. 2018, 262, 588–594. [Google Scholar] [CrossRef]
- Rane, T.D.; Zec, H.C.; Wang, T.H. A Serial Sample Loading System: Interfacing Multiwell Plates with Microfluidic Devices. J. Lab. Autom. 2012, 17, 370–377. [Google Scholar] [CrossRef]
- Nishat, S.; Jafry, A.T.; Martinez, A.W.; Awan, F.R. based microfluidics: Simplified fabrication and assay methods. Sens. Actuators B Chem. 2021, 336, 129681. [Google Scholar] [CrossRef]
- Torab, L.H.; Mach, P.; Surrette, K.E.; England, C.; Craft, M.R.; Wong, P.K. Adaptable microfluidic system for single-cell pathogen classification and antimicrobial susceptibility testing. Proc. Natl. Acad. Sci. USA 2019, 11, 10270–10279. [Google Scholar] [CrossRef]
- Barbosa, V.B.; Rodrigues, C.F.; Cerqueira, L.; Miranda, J.M.; Azevedo, N.F. Microfluidics combined with fluorescence in situ hybridization (FISH) for Candida spp. Detection. Front. Bioeng. Biotechnol. 2022, 10, 987669. [Google Scholar] [CrossRef]
- Azevedo, A.S.; Sousa, I.M.; Fernandes, R.M.; Azevedo, N.F.; Almeida, C. Optimizing locked nucleic acid/2′-O-methyl-RNA fluorescence in situ hybridization (LNA/2′OMe-FISH) procedure for bacterial detection. PLoS ONE 2019, 14, 0217689. [Google Scholar] [CrossRef]
- Ganguly, A.; Ebrahimzadeh, T.; Zimmern, P.E.; De Nisco, N.J.; Prasad, S. Label Free, Lateral Flow Prostaglandin E2 Electrochemical Immunosensor for Urinary Tract Infection Diagnosis. Chemosensors 2021, 9, 271. [Google Scholar] [CrossRef]
- Ozsahin, D.U.; Gökcekus, H.; Uzun, B.; Lamoreaux, J.W. Application of Multi-Criteria Decision Analysis in Environmental and Civil Engineerin; Springer: Cham, Switzerland, 2021; pp. 37–41. [Google Scholar] [CrossRef]
- Abdullah, M.F.; Siraj, S.; Hodgett, R.E. An Overview of Multi-Criteria Decision Analysis (MCDA) Application in Managing Water-Related Disaster Events: Analyzing 20 Years of Literature for Flood and Drought Events. Water 2021, 13, 1358. [Google Scholar] [CrossRef]
- Wang, C.N.; Yang, F.C.; Vo, N.T.M.; Nguyen, V.T.T. Enhancing Lithium-Ion Battery Manufacturing Efficiency: A Comparative Analysis Using DEA Malmquist and Epsilon-Based Measures. Batteries 2023, 9, 317. [Google Scholar] [CrossRef]
- Wang, C.-N.; Yang, F.-C.; Vo, T.M.N.; Nguyen, V.T.T.; Singh, M. Enhancing Efficiency and Cost-Effectiveness: A Groundbreaking Bi-Algorithm MCDM Approach. Appl. Sci. 2023, 13, 9105. [Google Scholar] [CrossRef]
- Mustapha, M.T.; Ozsahin, D.U.; Ozsahin, I.; Uzun, B. Breast Cancer Screening Based on Supervised Learning and Multi-Criteria Decision-Making. Diagnostics 2022, 12, 1326. [Google Scholar] [CrossRef] [PubMed]
- Brans, J.P.; Vincke, P. Note—A Preference Ranking Organisation Method: (The PROMETHEE Method for Multiple Criteria Decision-Making). Manag. Sci. 1985, 31, 647–656. [Google Scholar] [CrossRef]
- Zadeh, L.A. Fuzzy sets. Inf. Control 1965, 8, 338–353. [Google Scholar] [CrossRef]
- Harris, M.; Fasolino, T. New and emerging technologies for the diagnosis of urinary tract infections. J. Lab. Med. 2022, 46, 3–15. [Google Scholar] [CrossRef]
- Panel, P.; Ahs, T. Corporate Medical Policy Pathogen Panel Testing AHS-G2149. 2022, pp. 1–27. Available online: https://www.bluecrossnc.com/content/dam/bcbsnc/pdf/providers/policies-guidelines-codes/policies/commercial/laboratory/pathogen_panel_testing.pdf (accessed on 8 May 2023).
- Ozsahin, I.; Onakpojeruo, E.P.; Uzun, B.; Uzun Ozsahin, D.; Butler, T.A. A Multi-Criteria Decision Aid Tool for Radiopharmaceutical Selection in Tau PET Imaging. Pharmaceutics 2023, 15, 1304. [Google Scholar] [CrossRef]
- Arikan, A.; Sanlidag, T.; Sayan, M.; Uzun, B.; Uzun Ozsahin, D. Fuzzy-Based PROMETHEE Method for Performance Ranking of SARS-CoV-2 IgM Antibody Tests. Diagnostics 2022, 12, 2830. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Nour, Z.; Wu, G. Comparison of multi-criteria group decision-making methods for urban sewer network plan selection. Civil. Eng. 2020, 1, 26–48. [Google Scholar] [CrossRef]
- Yager, R.R. A procedure for ordering fuzzy subsets of the unit interval. Inf. Sci. 1981, 24, 143–161. [Google Scholar] [CrossRef]
- Al-Hasan, M.N.; Eckel-Passow, J.E.; Baddour, L.M. Bacteremia complicating gram negative urinary tract infections: A population-based study. J. Infect. 2010, 60, 278–285. [Google Scholar] [CrossRef]
- Wu, T.F.; Chen, Y.C.; Wang, W.C.; Fang, Y.C.; Fukuoka, S.; Pride, D.T.; Pak, O.S. A rapid and low-cost pathogen detection platform by using a molecular agglutination assay. ACS Cent. Sci. 2018, 4, 1485–1494. [Google Scholar] [CrossRef]
- Whiting, P.; Westwood, M.; Bojke, L.; Palmer, S.; Richardson, G.; Cooper, J.; Kleijnen, J. Clinical effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: A systematic review and economic model. Health Technol. Assess. 2006, 10, iii–iv. [Google Scholar] [CrossRef]
- Olanrewaju, A.O.; Ng, A.; De Corwin-Martin, P.; Robillard, A.; Juncker, D. Microfluidic capillaric circuit for rapid and facile bacteria detection. Anal. Chem. 2017, 89, 6846–6853. [Google Scholar] [CrossRef] [PubMed]
- Tseng, W.T.; Tseng, H.Y.; Chou, Y.Y.; Wang, Y.C.; Tseng, T.N.; Ho, L.I.; Ho, M.L. Quantitative urinary tract infection diagnosis of leukocyte esterase with a microfluidic paper-based device. Dalton Trans. 2021, 50, 9417–9425. [Google Scholar] [CrossRef]
- Mach, K.E.; Du, C.D.; Phull, H.; Haake, D.A.; Shih, M.C.; Baron, E.J.; Liao, J.C. Multiplex pathogen identification for polymicrobial urinary tract infections using biosensor technology: A prospective clinical study. J. Urol. 2009, 182, 2735–2741. [Google Scholar] [CrossRef] [PubMed]
- MI, A.D. Evaluation of the efficiency of URO-QUICKTM System in the Detection of Urinary Tract Infections and use of Fluorescence In-Situ Hybridization (FISH) In Detection of Escherichia coli in Urine. Egypt. J. Med. Microbiol. 2019, 28, 155–161. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Linguistic Scale for Evaluation | Triangular Fuzzy Scale | Criteria |
|---|---|---|
| Very High | (0.75, 1, 1) | Result time (C5), point of care testing (C6) |
| High | (0.50, 0.75, 1) | Cost (C3), efficiency (C4), limitation/pathogen identification (C10), sensitivity (C11), specificity (C12), PPV (C13), NPV (C14), antimicrobial susceptibility testing (C15) |
| Moderate | (0.25, 0.50, 0.75) | Applicability/direct from samples (C7), practicality for patients (C8), practicality for personnel (C9) |
| Low | (0, 0.25, 0.50) | Specimen type (C2) |
| Very Low | (0, 0, 0.25) | Specimen volume (C1) |
| Rank | UTI Tests | |||
|---|---|---|---|---|
| 1 | Biosensor | 0.0063 | 0.0064 | 0.0001 |
| 2 | Real-time microscopy systems | 0.003 | 0.0041 | 0.0011 |
| 3 | Catalase | 0.0026 | 0.004 | 0.0014 |
| 4 | Combined leucocyte esterase and nitrite | 0.0025 | 0.0039 | 0.0014 |
| 5 | Immunologically based assay | 0.002 | 0.0031 | 0.0011 |
| 6 | Microfluidics | 0.0019 | 0.0031 | 0.0012 |
| 7 | Nitrite | 0.0018 | 0.0039 | 0.0021 |
| 8 | Leucocyte esterase | 0.0018 | 0.0039 | 0.0021 |
| 9 | Conventional Culture | 0.0004 | 0.0038 | 0.0034 |
| 10 | Chromogenic agar | −0.0021 | 0.0025 | 0.0045 |
| 11 | Microscopy | −0.0022 | 0.0013 | 0.0035 |
| 12 | FISH | −0.0029 | 0.0012 | 0.0041 |
| 13 | MALDI–TOF–MS | −0.003 | 0.0011 | 0.0042 |
| 14 | Nucleic acid-based techniques (Multiplex PCR) | −0.0036 | 0.0013 | 0.0049 |
| 15 | Urine Flow cytometry | −0.0037 | 0.0008 | 0.0045 |
| 16 | Sequence-based diagnostics | −0.0048 | 0.0029 | 0.0077 |
| Rank | UTI Tests | |||
|---|---|---|---|---|
| 1 | Microfluidics | 0.2182 | 0.2194 | 0.0012 |
| 2 | Biosensor | 0.1925 | 0.1998 | 0.0073 |
| 3 | FISH (Flourescent in situ hybridisation) | 0.1337 | 0.1658 | 0.0321 |
| 4 | Real-time microscopy systems | 0.0808 | 0.1595 | 0.0787 |
| 5 | Urine Flow cytometry | 0.0651 | 0.1419 | 0.0768 |
| 6 | Chromogenic agar | 0.0569 | 0.1565 | 0.0997 |
| 7 | MALDI–TOF–MS | 0.0364 | 0.1269 | 0.0905 |
| 8 | Nucleic acid-based techniques (Multiplex PCR) | −0.0087 | 0.1091 | 0.1178 |
| 9 | Conventional Culture | −0.0241 | 0.0992 | 0.1233 |
| 10 | Catalase | −0.0282 | 0.1032 | 0.1314 |
| 11 | Sequence-based diagnostics | −0.0311 | 0.1067 | 0.1378 |
| 12 | Immunologically based assay | −0.1112 | 0.0733 | 0.1845 |
| 13 | Nitrite | −0.1212 | 0.0702 | 0.1914 |
| 14 | Combined leucocyte esterase and nitrite | −0.1335 | 0.0563 | 0.1899 |
| 15 | Microscopy | −0.1513 | 0.058 | 0.2093 |
| 16 | Leucocyte esterase | −0.1743 | 0.0439 | 0.2182 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abobakr, M.; Uzun, B.; Uzun Ozsahin, D.; Sanlidag, T.; Arikan, A. Assessment of UTI Diagnostic Techniques Using the Fuzzy–PROMETHEE Model. Diagnostics 2023, 13, 3421. https://doi.org/10.3390/diagnostics13223421
Abobakr M, Uzun B, Uzun Ozsahin D, Sanlidag T, Arikan A. Assessment of UTI Diagnostic Techniques Using the Fuzzy–PROMETHEE Model. Diagnostics. 2023; 13(22):3421. https://doi.org/10.3390/diagnostics13223421
Chicago/Turabian StyleAbobakr, Mariam, Berna Uzun, Dilber Uzun Ozsahin, Tamer Sanlidag, and Ayse Arikan. 2023. "Assessment of UTI Diagnostic Techniques Using the Fuzzy–PROMETHEE Model" Diagnostics 13, no. 22: 3421. https://doi.org/10.3390/diagnostics13223421