
Percutaneous Computed Tomography-Guided Oxygen-Ozone (O2O3) Injection Therapy in Patients with Lower Back Pain—An Interventional Two-Year Follow-Up Study of 321 Patients
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
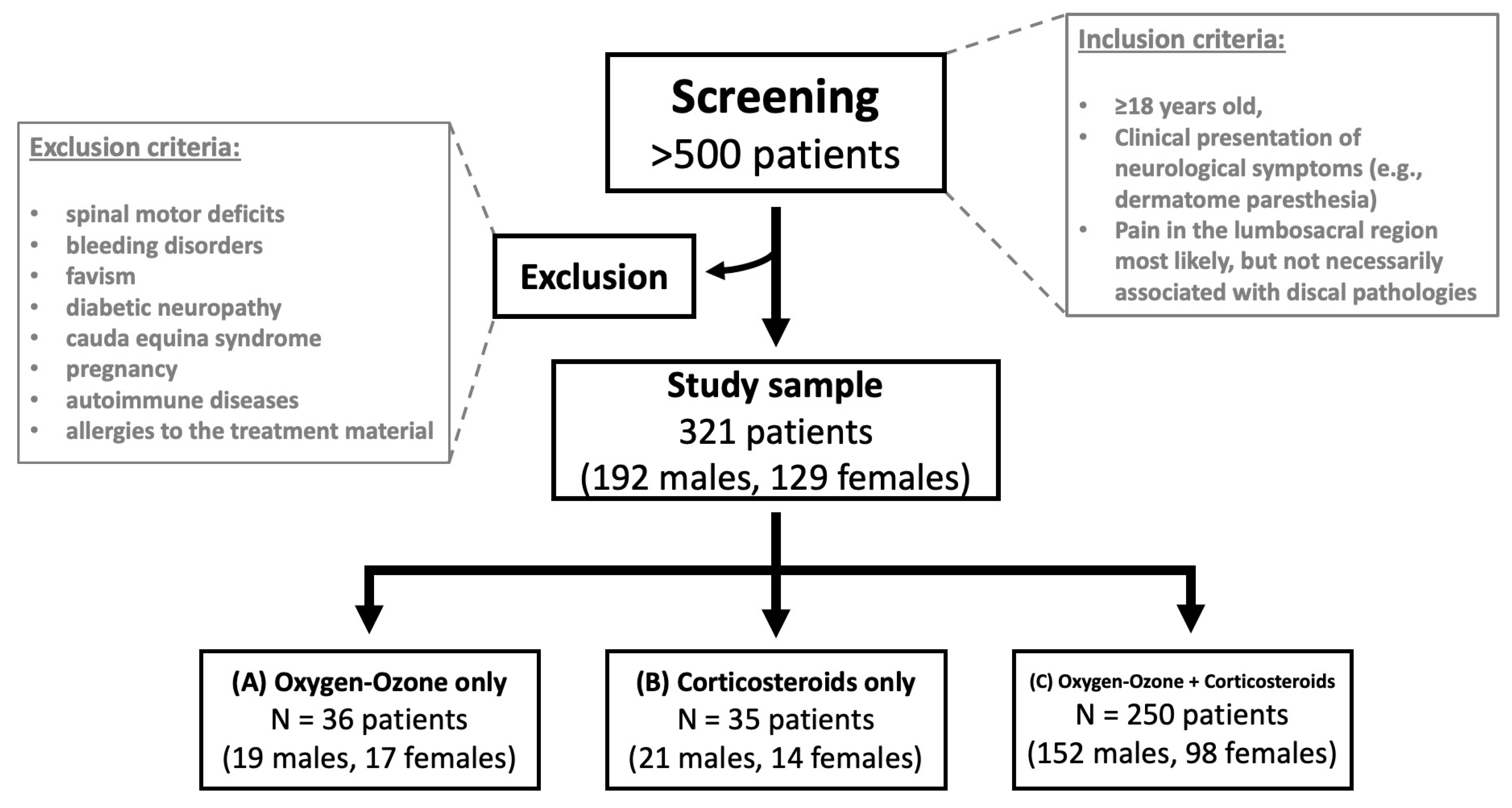
2.2. Study Sample and Inclusion/Exclusion Criteria
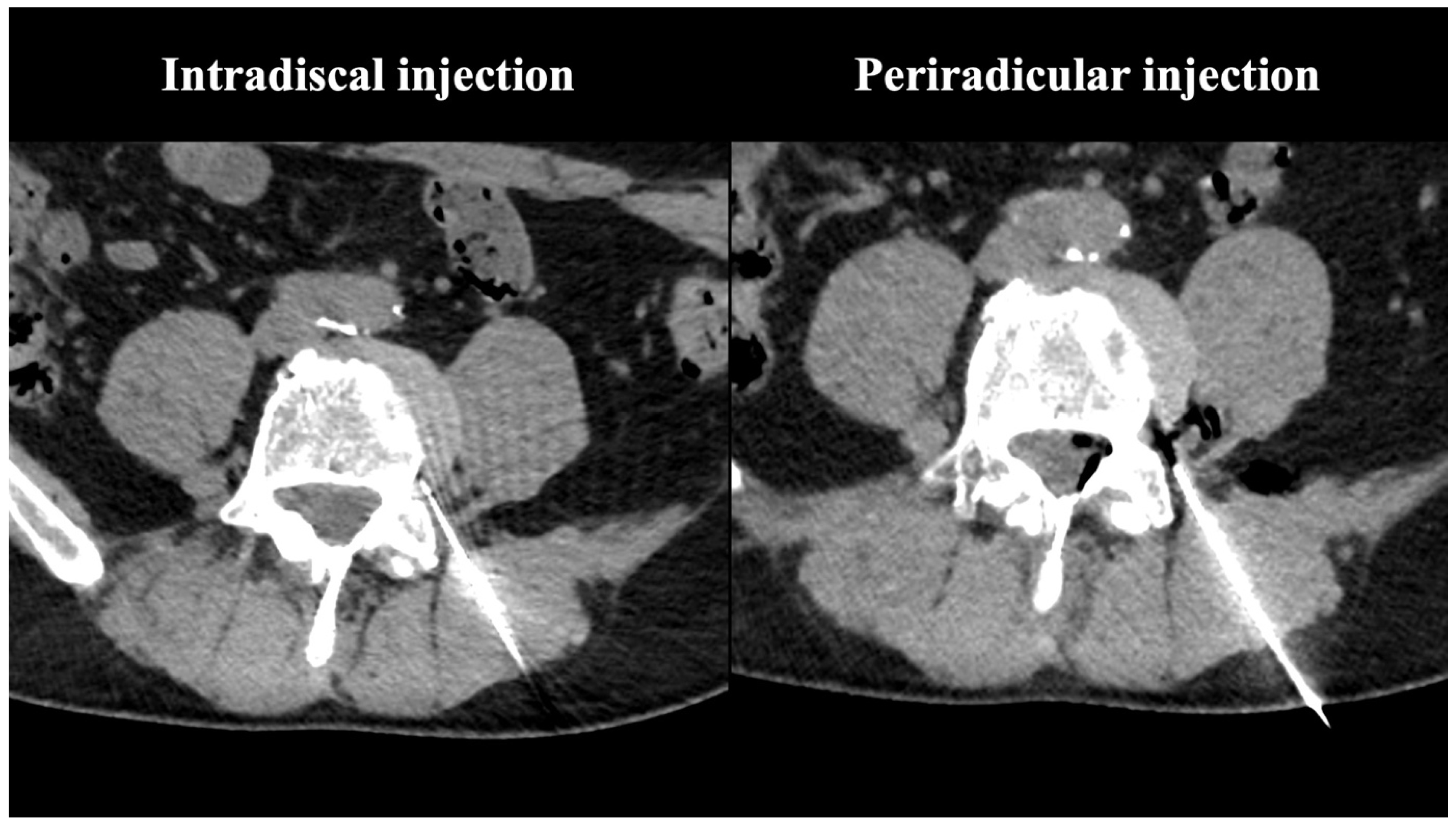
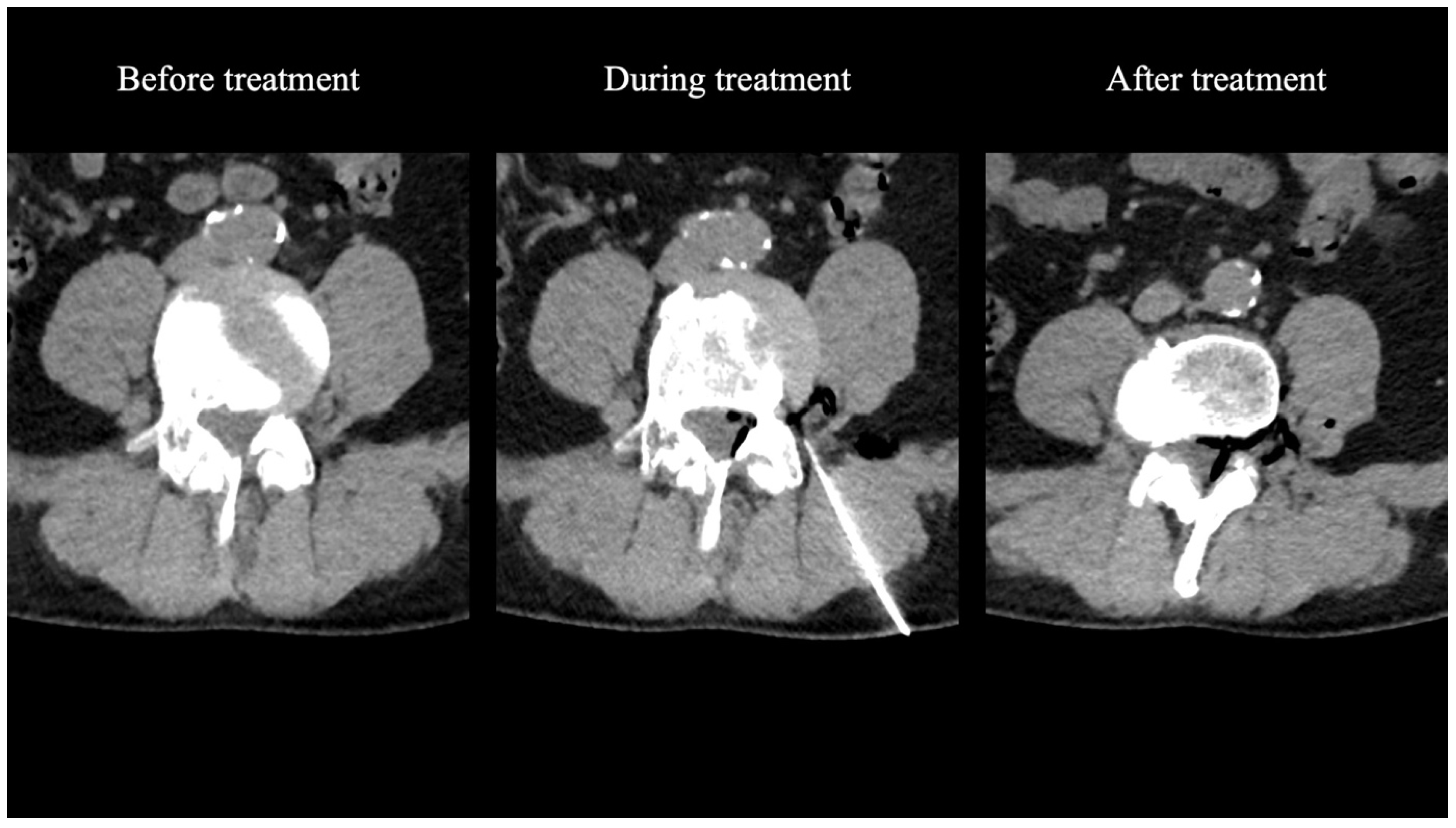
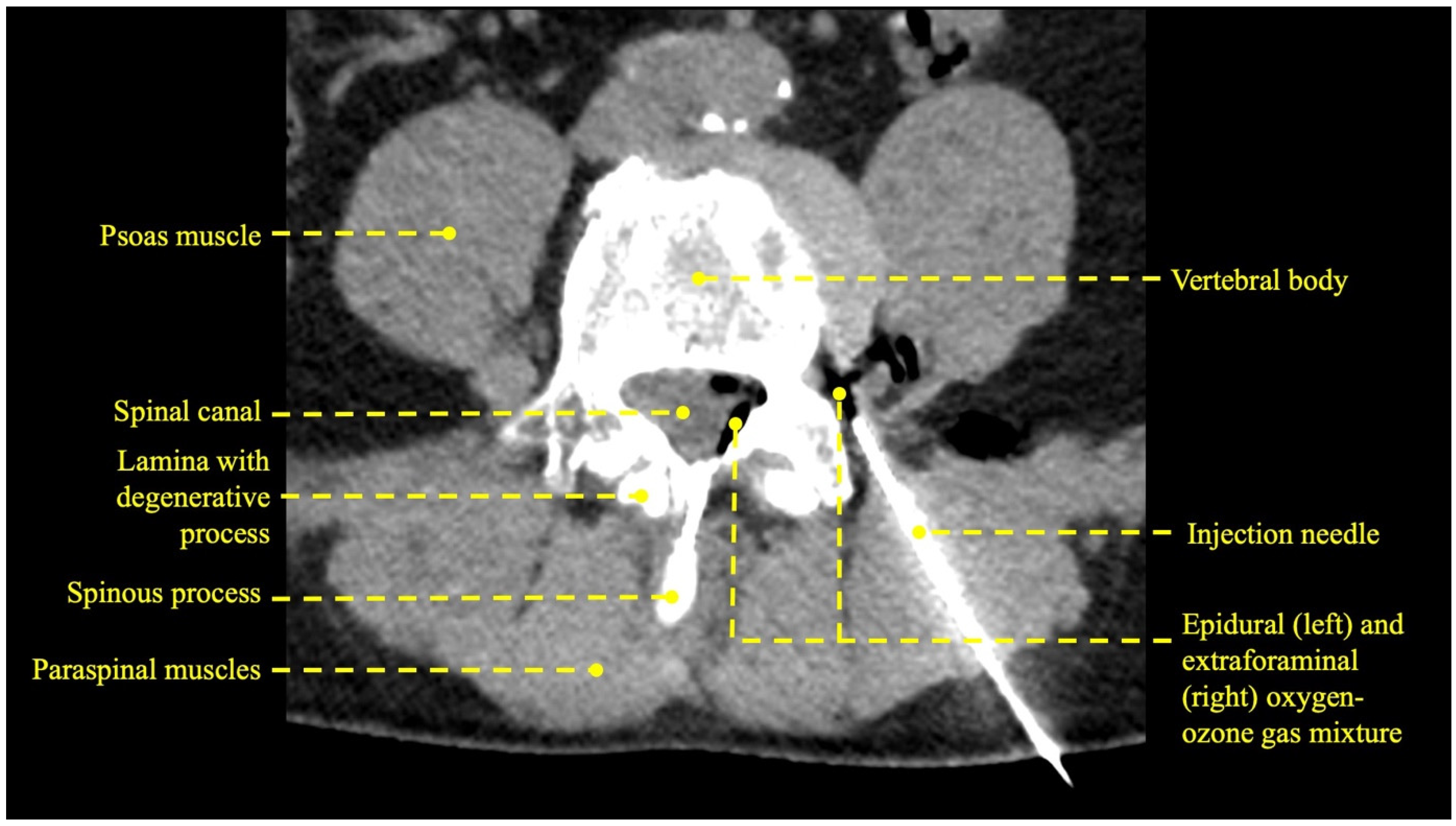
2.3. Treatment Protocol
- -
- Group A received percutaneous injections of 5–10 mL of an oxygen-ozone gas mixture (2% ozone in a concentration of 30–40 mg/mL and 98% oxygen);
- -
- Group B received percutaneous injections of corticosteroids (1 mL of long-acting corticosteroids and 1 mL of lidocaine chloride);
- -
- Group C received combined treatment with percutaneous injections of both oxygen-ozone gas mixture and corticosteroids (2% ozone in a concentration of 30–40 mg/mL and 98% oxygen + 1 mL of long-acting corticosteroids and 1 mL of lidocaine chloride).
2.4. Self-Reported Pain Scales
2.5. Statistical Analysis
3. Results
3.1. Procedural Technical Outcome
3.2. Patient Demographic Data
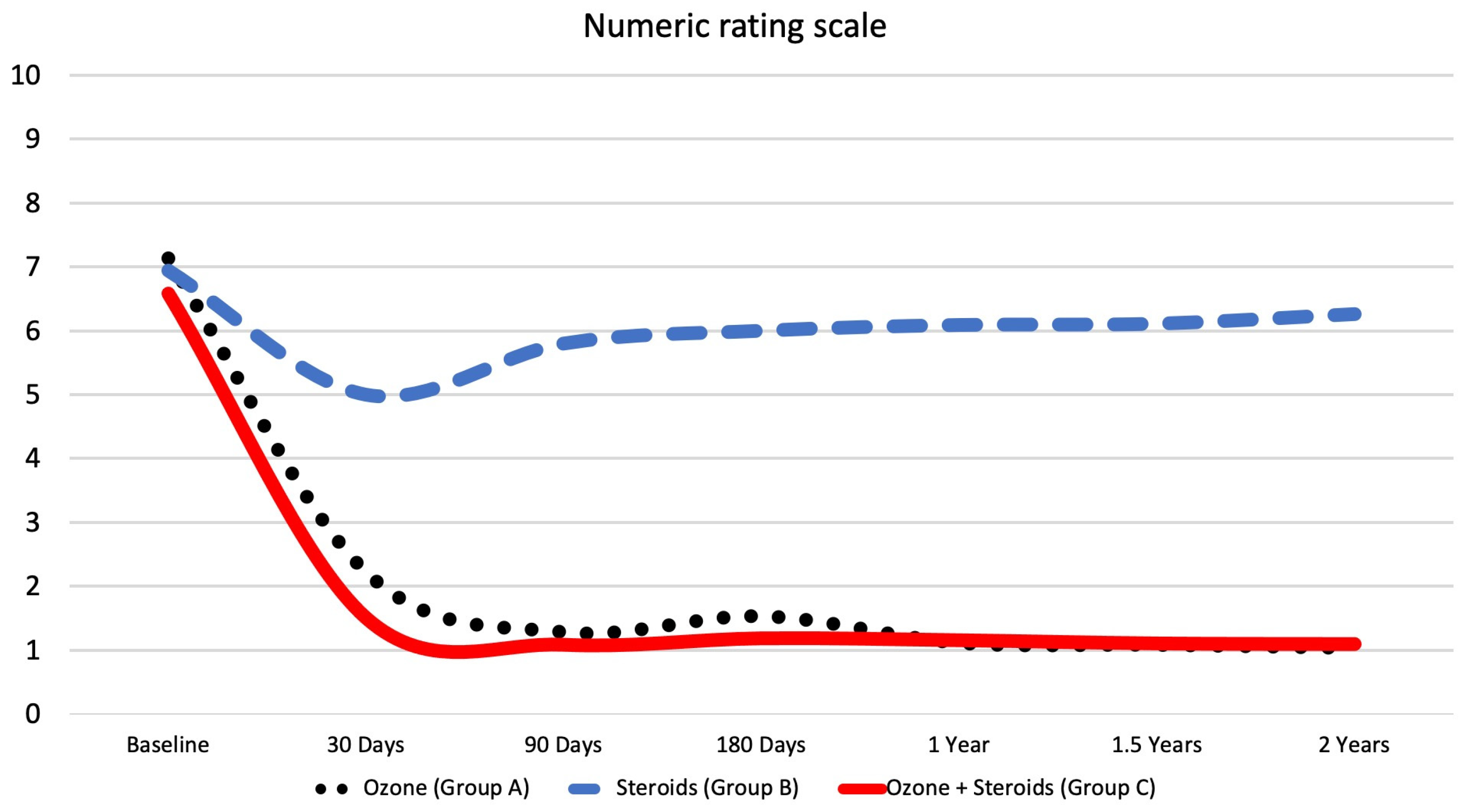
3.3. Numeric Rating Scale
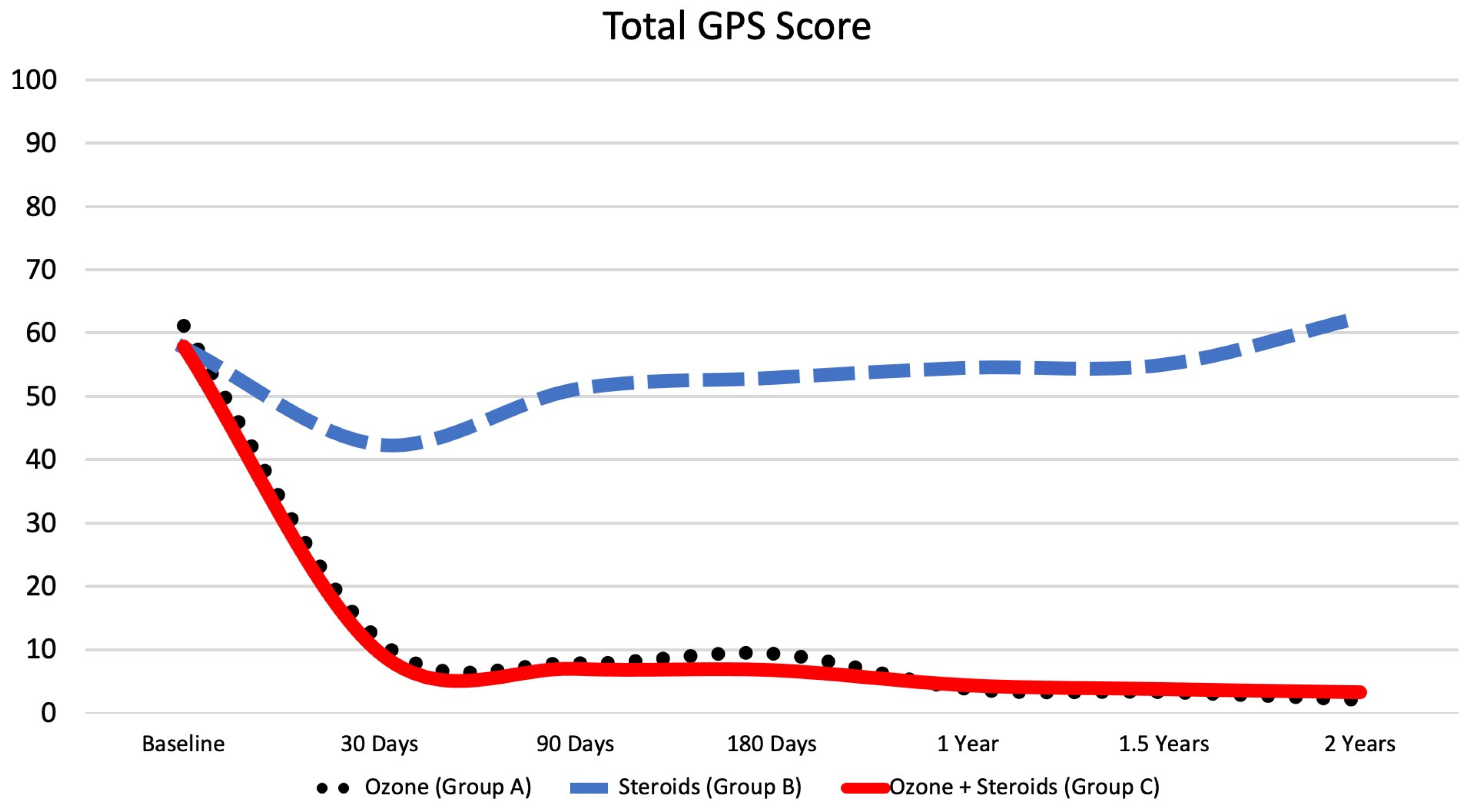
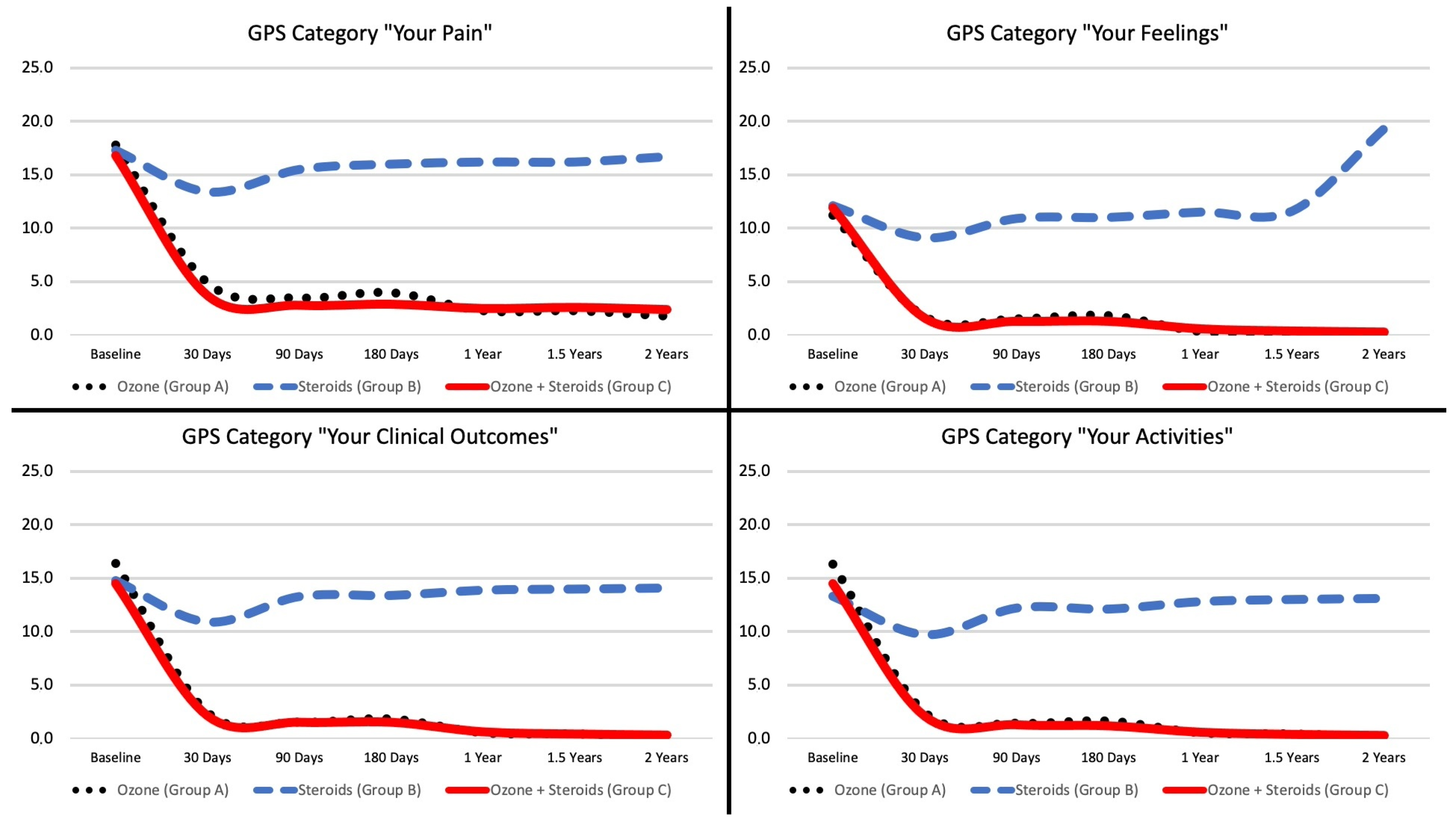
3.4. Global Pain Scale
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| LBP | Lower back pain |
| YLD | Years of life lost due to disability |
| MRI | Magnetic resonance imaging |
| CT | Computed tomography |
| NRS | Numeric rating scale |
| GPS | Global pain scale |
References
- Wu, A.; March, L.; Zheng, X.; Huang, J.; Wang, X.; Zhao, J.; Blyth, F.M.; Smith, E.; Buchbinder, R.; Hoy, D. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Ann. Transl. Med. 2020, 8, 299. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Chen, M.; Wu, X.; Lin, S.; Tao, C.; Cao, H.; Shao, Z.; Xiao, G. Global, regional and national burden of low back pain 1990–2019: A systematic analysis of the Global Burden of Disease study 2019. J. Orthop. Transl. 2022, 32, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Serranheira, F.; Sousa-Uva, M.; Heranz, F.; Kovacs, F.; Sousa-Uva, A. Low Back Pain (LBP), work and absenteeism. Work 2020, 65, 463–469. [Google Scholar] [CrossRef]
- Carregaro, R.L.; Tottoli, C.R.; Rodrigues, D.d.S.; Bosmans, J.E.; da Silva, E.N.; van Tulder, M. Low back pain should be considered a health and research priority in Brazil: Lost productivity and healthcare costs between 2012 to 2016. PLoS ONE 2020, 15, e0230902. [Google Scholar] [CrossRef] [PubMed]
- Dutmer, A.L.; Schiphorst Preuper, H.R.; Soer, R.; Brouwer, S.; Bültmann, U.; Dijkstra, P.U.; Coppes, M.H.; Stegeman, P.; Buskens, E.; van Asselt, A.D.I.; et al. Personal and Societal Impact of Low Back Pain: The Groningen Spine Cohort. Spine 2019, 44, E1443–E1451. [Google Scholar] [CrossRef]
- Martin, B.I.; Deyo, R.A.; Mirza, S.K.; Turner, J.A.; Comstock, B.A.; Hollingworth, W.; Sullivan, S.D. Expenditures and health status among adults with back and neck problems. JAMA 2008, 299, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, N.N.; Candido, K.D.; Vlaeyen, J.W.S.; Van Zundert, J.; Cohen, S.P. Low back pain. Lancet 2021, 398, 78–92. [Google Scholar] [CrossRef]
- Burr, J.; Shephard, R.; Cornish, S.; Vatanparast, H.; Chilibeck, P. Arthritis, osteoporosis, and low back pain: Evidence-based clinical risk assessment for physical activity and exercise clearance. Can. Fam. Physician 2012, 58, 59–62. [Google Scholar]
- Casiano, V.E.; Sarwan, G.; Dydyk, A.M.; Varacallo, M. Back Pain; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Balagué, F.; Pellisé, F. Adolescent idiopathic scoliosis and back pain. Scoliosis Spinal Disord. 2016, 11, 27. [Google Scholar] [CrossRef] [PubMed]
- Dydyk, A.M.; Ngnitewe Massa, R.; Mesfin, F.B. Disc Herniation; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Amin, R.M.; Andrade, N.S.; Neuman, B.J. Lumbar Disc Herniation. Curr. Rev. Musculoskelet. Med. 2017, 10, 507–516. [Google Scholar] [CrossRef]
- Lee, S.W.; Nguyen, D.; Mack, D.; Aguila, E.; Thomas, M.; Doddy, K. Conservative Management of Low Back Pain. HCA Healthc. J. Med. 2021, 2, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Baliga, S.; Treon, K.; Craig, N.J.A. Low Back Pain: Current Surgical Approaches. Asian Spine J. 2015, 9, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Hegmann, K.T.; Travis, R.; Andersson, G.B.J.; Belcourt, R.M.; Carragee, E.J.; Donelson, R.; Eskay-Auerbach, M.M.; Galper, J.P.; Goertz, M.; Haldeman, S.M.; et al. Non-Invasive and Minimally Invasive Management of Low Back Disorders. J. Occup. Environ. Med. 2020, 62, e111–e138. [Google Scholar] [CrossRef] [PubMed]
- Fasoli, F.; Gandini, R.; Scaggiante, J.; Bartolo, M.; Capobianco, S.V.; Cerone, G. Minimally-invasive percutaneous treatments for low back pain and leg pain: A randomized controlled study of thermal disc decompression versus mechanical percutaneous disc decompression. Spine J. 2022, 22, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Masini, M.; Calaça, A. Minimally invasive treatment for refractory low back pain, targeted by epidural endoscopy with O2/O3 and steroid therapy. Acta Neurochir. Suppl. 2011, 108, 33–37. [Google Scholar]
- Epstein, N.E. Spine surgery in geriatric patients: Sometimes unnecessary, too much, or too little. Surg. Neurol. Int. 2011, 2, 188. [Google Scholar] [CrossRef]
- Hersey, A.E.; Durand, W.M.; Eltorai, A.E.M.; DePasse, J.M.; Daniels, A.H. Longer Operative Time in Elderly Patients Undergoing Posterior Lumbar Fusion Is Independently Associated With Increased Complication Rate. Glob. Spine J. 2019, 9, 179–184. [Google Scholar] [CrossRef]
- O’Lynnger, T.M.; Zuckerman, S.L.; Morone, P.J.; Dewan, M.C.; Vasquez-Castellanos, R.A.; Cheng, J.S. Trends for Spine Surgery for the Elderly: Implications for Access to Healthcare in North America. Neurosurgery 2015, 77 (Suppl. S4), S136–S141. [Google Scholar] [CrossRef]
- Chan, C.; Peng, P. Failed back surgery syndrome. Pain Med. 2011, 12, 577–606. [Google Scholar] [CrossRef]
- North, R.B.; Campbell, J.N.; James, C.S.; Conover-Walker, M.K.; Wang, H.; Piantadosi, S.; Rybock, J.D.; Long, D.M. Failed back surgery syndrome: 5-year follow-up in 102 patients undergoing repeated operation. Neurosurgery 1991, 28, 681–685. [Google Scholar] [CrossRef]
- Law, J.D.; Lehman, R.A.; Kirsch, W.M. Reoperation after lumbar intervertebral disc surgery. J. Neurosurg. 1978, 48, 259–263. [Google Scholar] [CrossRef]
- Lehmann, T.R.; LaRocca, H.S. Repeat lumbar surgery. A review of patients with failure from previous lumbar surgery treated by spinal canal exploration and lumbar spinal fusion. Spine 1981, 6, 615–619. [Google Scholar] [CrossRef]
- Magalhaes, F.N.D.O.; Dotta, L.; Sasse, A.; Teixera, M.J.; Fonoff, E.T. Ozone therapy as a treatment for low back pain secondary to herniated disc: A systematic review and meta-analysis of randomized controlled trials. Pain Physician 2012, 15, E115–E129. [Google Scholar] [PubMed]
- Steppan, J.; Meaders, T.; Muto, M.; Murphy, K.J. A metaanalysis of the effectiveness and safety of ozone treatments for herniated lumbar discs. J. Vasc. Interv. Radiol. 2010, 21, 534–548. [Google Scholar] [CrossRef]
- Filippiadis, D.K.; Kelekis, A. A review of percutaneous techniques for low back pain and neuralgia: Current trends in epidural infiltrations, intervertebral disk and facet joint therapies. Br. J. Radiol. 2016, 89, 20150357. [Google Scholar] [CrossRef] [PubMed]
- Sconza, C.; Kon, E.; Marcacci, M.; Massazza, G.; Matteo, B.; Respizzi, S.; Leonardi, G. Oxygen-ozone therapy for the treatment of low back pain: A systematic review of randomized controlled trials. Eur. Rev. Med. Pharmacol. Sci. 2021, 2021, 6034–6046. [Google Scholar]
- Gallucci, M.; Limbucci, N.; Zugaro, L.; Barile, A.; Stavroulis, E.; Ricci, A.; Galzio, R.; Masciocchi, C. Sciatica: Treatment with intradiscal and intraforaminal injections of steroid and oxygen-ozone versus steroid only. Radiology 2007, 242, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Muto, M.; Andreula, C.; Leonardi, M. Treatment of herniated lumbar disc by intradiscal and intraforaminal oxygen-ozone (O2-O3) injection. J. Neuroradiol. 2004, 31, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.L. CT fluoroscopy-guided epidural injections: Technique and results. AJNR Am. J. Neuroradiol. 2004, 25, 1821–1823. [Google Scholar]
- Paoloni, M.; Di Sante, L.; Cacchio, A.; Apuzzo, D.; Marotta, S.; Razzano, M.; Franzini, M.; Santilli, V. Intramuscular oxygen-ozone therapy in the treatment of acute back pain with lumbar disc herniation: A multicenter, randomized, double-blind, clinical trial of active and simulated lumbar paravertebral injection. Spine 2009, 34, 1337–1344. [Google Scholar] [CrossRef]
- Verga, C. Nuovo approccio terapeutico alle ernie e protrusioni discali lombari. Riv. Neuroradiol. 1989, 2 (Suppl. S1), 148. [Google Scholar] [CrossRef]
- Muto, M.; Avella, F. Percutaneous Treatment of Herniated Lumbar Disc by Intradiscal Oxygen-Ozone Injection. Interv. Neuroradiol. 1998, 4, 279–286. [Google Scholar] [CrossRef]
- Das, G.; Ray, S.; Ishwarari, S.; Roy, M.; Ghosh, P. Ozone nucleolysis for management of pain and disability in prolapsed lumber intervertebral disc. A prospective cohort study. Interv. Neuroradiol. J. Peritherapeutic Neuroradiol. Surg. Proced. Relat. Neurosci. 2009, 15, 330–334. [Google Scholar]
- Muto, M.; Ambrosanio, G.; Guarnieri, G.; Capobianco, E.; Piccolo, G.; Annunziata, G.; Rotondo, A. Low back pain and sciatica: Treatment with intradiscal-intraforaminal O(2)-O (3) injection. Our experience. Radiol. Med. 2008, 113, 695–706. [Google Scholar] [CrossRef]
- Simon, C.; Le Corroller, T.; Pauly, V.; Creze, M.; Champsaur, P.; Guenoun, D. Intradiscal oxygen-ozone therapy for the treatment of symptomatic lumbar disc herniation: A preliminary study. J. Neuroradiol. 2022, 49, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Oder, B.; Loewe, M.; Reisegger, M.; Lang, W.; Ilias, W.; Thurnher, S.A. CT-guided ozone/steroid therapy for the treatment of degenerative spinal disease--effect of age, gender, disc pathology and multi-segmental changes. Neuroradiology 2008, 50, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Buric, J.; Molino Lova, R. Ozone chemonucleolysis in non-contained lumbar disc herniations: A pilot study with 12 months follow-up. Acta Neurochir. Suppl. 2005, 92, 93–97. [Google Scholar] [PubMed]
- Biazzo, A.; Corriero, A.S.; Confalonieri, N. Intramuscular oxygen-ozone therapy in the treatment of low back pain. Acta Biomed. 2018, 89, 41–46. [Google Scholar]
- Hashemi, M.; Poorfarokh, M.; Mohajerani, S.A.; Jalili, P.; Akhyani, V.; Barikani, A.; Farivar, F. Injection of intradiscal O2-O3 to reduce pain and disability of patients with low back pain due to prolapsed lumbar disk. Anesthesiol. Pain Med. 2014, 4, e19206. [Google Scholar] [CrossRef]
- Andreula, C.F.; Simonetti, L.; De Santis, F.; Agati, R.; Ricci, R.; Leonardi, M. Minimally invasive oxygen-ozone therapy for lumbar disk herniation. AJNR Am. J. Neuroradiol. 2003, 24, 996–1000. [Google Scholar]
- Simonetti, L.; Raffi, L.; Cenni, P.; Agati, R.; Leonardi, M. Pharmacological Mechanisms Underlying Oxygen-Ozone Therapy for Herniated Disc. Riv. Neuroradiol. 2003, 16 (Suppl. S2), 201–204. [Google Scholar] [CrossRef]
- Bocci, V.A. Scientific and medical aspects of ozone therapy. State of the art. Arch. Med. Res. 2006, 37, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Bocci, V. Basic Biological and Therapeutic Effects of Ozone Therapy in Human Medicine. In Ozone Science and Technology; Eolss Publishers: Oxford, UK, 2011. [Google Scholar]
- Giurazza, F.; Guarnieri, G.; Murphy, K.J.; Muto, M. Intradiscal O2O3: Rationale, Injection Technique, Short- and Long-term Outcomes for the Treatment of Low Back Pain Due to Disc Herniation. Can. Assoc. Radiol. J. 2017, 68, 171–177. [Google Scholar] [CrossRef]
- Rahimi-Movaghar, V.; Eslami, V. The major efficient mechanisms of ozone therapy are obtained in intradiscal procedures. Pain Physician 2012, 15, E1007–E1008. [Google Scholar] [CrossRef]
- Yang, C.-S.; Zhang, L.-J.; Sun, Z.-H.; Yang, L.; Shi, F.-D. Acute prevertebral abscess secondary to intradiscal oxygen-ozone chemonucleolysis for treatment of a cervical disc herniation. J. Int. Med. Res. 2018, 46, 2461–2465. [Google Scholar] [CrossRef] [PubMed]
- Beyaz, S.G.; Altaş, C.; Sayhan, H. Cardiopulmonary Arrest and Pneumoencephaly Developing after Epidural Oxygen-ozone Mixture Therapy. Anesth. Essays Res. 2018, 12, 285–287. [Google Scholar] [CrossRef]
- Ovidiu, B.; Dumitru, M.; Vrinceanu, D.; Cergan, R.; Jeican, I.I.; Giurcaneanu, C.; Miron, A. Current Approach to Medico-Legal Aspects of Allergic Reactions. Rom. J. Leg. Med. 2021, 29, 328–331. [Google Scholar]
- Rimeika, G.; Saba, L.; Arthimulam, G.; Della Gatta, L.; Davidovic, K.; Bonetti, M.; Franco, D.; Russo, C.; Muto, M. Metanalysis on the effectiveness of low back pain treatment with oxygen-ozone mixture: Comparison between image-guided and non-image-guided injection techniques. Eur. J. Radiol. Open 2021, 8, 100389. Available online: https://www.sciencedirect.com/science/article/pii/S2352047721000691 (accessed on 12 July 2023). [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (A) Oxygen-Ozone Group A N = 36 | (B) Steroids Group B N = 35 | (C) Oxygen-Ozone + Steroids Group C N = 250 | |
|---|---|---|---|
| Gender | |||
| Male (N =192) | 19 (52.8%) | 21 (60.0%) | 152 (60.8%) |
| Female (N = 129) | 17 (47.2%) | 14 (38.9%) | 98 (39.2%) |
| Age | |||
| Age Mean ± SD (years) | 52.9 ± 13.3 | 51.7 ± 18.5 | 51.3 ± 14.9 |
| Duration of lower back pain | |||
| Less than 6 months | 3 (8.3%) | 4 (11.4%) | 48 (19.2%) |
| 6–12 months | 2 (5.6%) | 4 (11.4%) | 41 (16.4%) |
| 12–24 months | 4 (11.1%) | 5 (14.3%) | 44 (17.6%) |
| More than 24 months | 27 (75.0%) | 22 (62.9%) | 117 (46.8%) |
| Patient history | |||
| Previous therapy (Yes) | 17 (47.2%) | 21 (60.0%) | 119 (47.6%) |
| Previous surgery (Yes) | 4 (11.1%) | 5 (14.3%) | 15 (6.0%) |
| Previous physical therapy (Yes) | 13 (36.1%) | 19 (54.3%) | 133 (53.2%) |
| Baseline | 30 Days | p Value | 90 Days | p Value | 180 Days | p Value | 1 Year | p Value | 1.5 Years | p Value | 2 Years | p Value | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Oxygen-ozone | Numeric rating scale | 7.1 ± 2.3 | 2.2 ± 2.3 | <0.001 | 1.3 ± 2.1 | <0.001 | 1.5 ± 2.3 | <0.001 | 1.1 ± 2.3 | <0.001 | 1.1 ± 2.2 | <0.001 | 1.0 ± 2.2 | <0.001 |
| Group A | Total GPS Score | 61.1 ± 22.7 | 11.3 ± 11.3 | <0.001 | 7.8 ± 10.4 | <0.001 | 9.3 ± 12.3 | <0.001 | 3.7 ± 6.9 | <0.001 | 3.2 ± 6.8 | <0.001 | 2.0 ± 4.4 | <0.001 |
| “Your Pain” | 17.8 ± 5.0 | 4.9 ± 5.1 | <0.001 | 3.5 ± 5.2 | <0.001 | 4.0 ± 5.6 | <0.001 | 2.3 ± 4.7 | <0.001 | 2.3 ± 4.7 | <0.001 | 1.8 ± 3.9 | <0.001 | |
| “Your Feelings” | 11.2 ± 6.1 | 1.7 ± 2.6 | <0.001 | 1.5 ± 1.9 | <0.001 | 1.8 ± 2.5 | <0.001 | 0.3 ± 0.9 | <0.001 | 0.1 ± 0.5 | <0.001 | 0.0 ± 0.0 | <0.001 | |
| “Your Clinical Outcomes” | 16.4 ± 6.9 | 2.4 ± 2.9 | <0.001 | 1.5 ± 2.4 | <0.001 | 1.8 ± 2.9 | <0.001 | 0.5 ± 1.0 | <0.001 | 0.4 ± 1.1 | <0.001 | 0.1 ± 0.3 | <0.001 | |
| “Your Activities” | 16.3 ± 7.8 | 2.4 ± 2.9 | <0.001 | 1.4 ± 2.4 | <0.001 | 1.6 ± 2.7 | <0.001 | 0.5 ± 1.1 | <0.001 | 0.4 ± 1.2 | <0.001 | 0.1 ± 0.4 | <0.001 | |
| Corticosteroids | Numeric rating scale | 6.9 ± 2.4 | 5.0 ± 2.2 | <0.001 | 5.8 ± 1.9 | <0.001 | 6.0 ± 2.0 | <0.001 | 6.1 ± 2.0 | <0.001 | 6.1 ± 1.9 | <0.001 | 6.3 ± 1.8 | <0.001 |
| Group B | Total GPS Score | 57.7 ± 21.2 | 42.3 ± 22.4 | <0.001 | 51.1 ± 16.6 | <0.001 | 52.9 ± 19.1 | <0.001 | 54.5 ± 19.3 | <0.001 | 55.0 ± 18.9 | 0.002 | 62.5 ± 17.0 | <0.001 |
| Total GPS Score | 17.3 ± 5.0 | 13.4 ± 5.4 | <0.001 | 15.5 ± 3.9 | <0.001 | 16.0 ± 4.3 | 0.002 | 16.2 ± 4.2 | 0.004 | 16.2 ± 4.1 | 0.007 | 16.7 ± 4.9 | 0.328 | |
| “Your Pain” | 12.1 ± 7.3 | 9.1 ± 6.7 | <0.001 | 10.9 ± 6.0 | 0.013 | 11.0 ± 6.3 | 0.008 | 11.5± 6.5 | 0.214 | 11.6 ± 6.5 | 0.313 | 19.3 ± 4.2 | <0.001 | |
| “Your Feelings” | 14.8 ± 6.5 | 10.9 ± 6.6 | <0.001 | 13.3 ± 5.7 | <0.001 | 13.4 ± 6.2 | <0.001 | 13.9 ± 6.2 | <0.001 | 14.0 ± 6.1 | <0.001 | 14.1 ± 6.3 | <0.001 | |
| “Your Clinical Outcomes” | 13.3 ± 7.0 | 9.7 ± 6.7 | <0.001 | 12.2 ± 6.1 | 0.005 | 12.1 ± 6.4 | 0.018 | 12.8 ± 6.6 | 0.080 | 13.0 ± 6.4 | 0.207 | 13.1 ± 6.5 | 0.413 | |
| Oxygen-ozone + Corticosteroids | Numeric rating scale | 6.6 ± 2.2 | 1.5 ± 2.0 | <0.001 | 1.1 ± 1.7 | <0.001 | 1.2 ± 2.0 | <0.001 | 1.2 ± 2.0 | <0.001 | 1.1 ± 2.0 | <0.001 | 1.1 ± 2.0 | <0.001 |
| Group C | Total GPS Score | 57.9 ± 22.2 | 9.5 ± 14.5 | <0.001 | 7.0 ± 12.1 | <0.001 | 6.8 ± 13.6 | <0.001 | 4.4 ± 8.8 | <0.001 | 3.8 ± 7.6 | <0.001 | 3.3 ± 6.5 | <0.001 |
| Total GPS Score | 16.8 ± 4.8 | 3.7 ± 5.1 | <0.001 | 2.8 ± 4.3 | <0.001 | 2.9 ± 4.9 | <0.001 | 2.5 ± 4.7 | <0.001 | 2.6 ± 4.6 | <0.001 | 2.4 ± 4.4 | <0.001 | |
| “Your Pain” | 11.9 ± 6.9 | 1.6 ± 3.4 | <0.001 | 1.3 ± 3.0 | <0.001 | 1.3 ± 3.4 | <0.001 | 0.6 ± 1.7 | <0.001 | 0.4 ± 1.5 | <0.001 | 0.3 ± 1.3 | <0.001 | |
| “Your Feelings” | 14.5 ± 6.8 | 2.1 ± 3.4 | <0.001 | 1.5 ± 2.8 | <0.001 | 1.5 ± 3.2 | <0.001 | 0.6 ± 1.7 | <0.001 | 0.4 ± 1.4 | <0.001 | 0.3 ± 1.0 | <0.001 | |
| “Your Clinical Outcomes” | 14.5 ± 7.0 | 2.1 ± 3.8 | <0.001 | 1.3 ± 2.8 | <0.001 | 1.2 ± 3.1 | <0.001 | 0.6 ± 1.5 | <0.001 | 0.4 ± 1.1 | <0.001 | 0.3 ± 1.0 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davidovic, K.; Cotofana, S.; Heisinger, S.; Savic, S.; Alfertshofer, M.; Antonić, T.; Jovanović, S.; Ercegovac, M.; Muto, M.; Jeremić, D.; et al. Percutaneous Computed Tomography-Guided Oxygen-Ozone (O2O3) Injection Therapy in Patients with Lower Back Pain—An Interventional Two-Year Follow-Up Study of 321 Patients. Diagnostics 2023, 13, 3370. https://doi.org/10.3390/diagnostics13213370
Davidovic K, Cotofana S, Heisinger S, Savic S, Alfertshofer M, Antonić T, Jovanović S, Ercegovac M, Muto M, Jeremić D, et al. Percutaneous Computed Tomography-Guided Oxygen-Ozone (O2O3) Injection Therapy in Patients with Lower Back Pain—An Interventional Two-Year Follow-Up Study of 321 Patients. Diagnostics. 2023; 13(21):3370. https://doi.org/10.3390/diagnostics13213370
Chicago/Turabian StyleDavidovic, Kristina, Sebastian Cotofana, Stephan Heisinger, Slavica Savic, Michael Alfertshofer, Tatjana Antonić, Sanja Jovanović, Marko Ercegovac, Mario Muto, Danilo Jeremić, and et al. 2023. "Percutaneous Computed Tomography-Guided Oxygen-Ozone (O2O3) Injection Therapy in Patients with Lower Back Pain—An Interventional Two-Year Follow-Up Study of 321 Patients" Diagnostics 13, no. 21: 3370. https://doi.org/10.3390/diagnostics13213370