
Galectin-8 Immunohistochemical Profile in Pancreatic Ductal Adenocarcinoma: Emerging Evidence for Its Prognostic Role
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Tissue Samples
2.2. Immunohistochemical Exam
2.3. Qualitative and Semi-Quantitative Evaluation of Gal8
2.4. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics
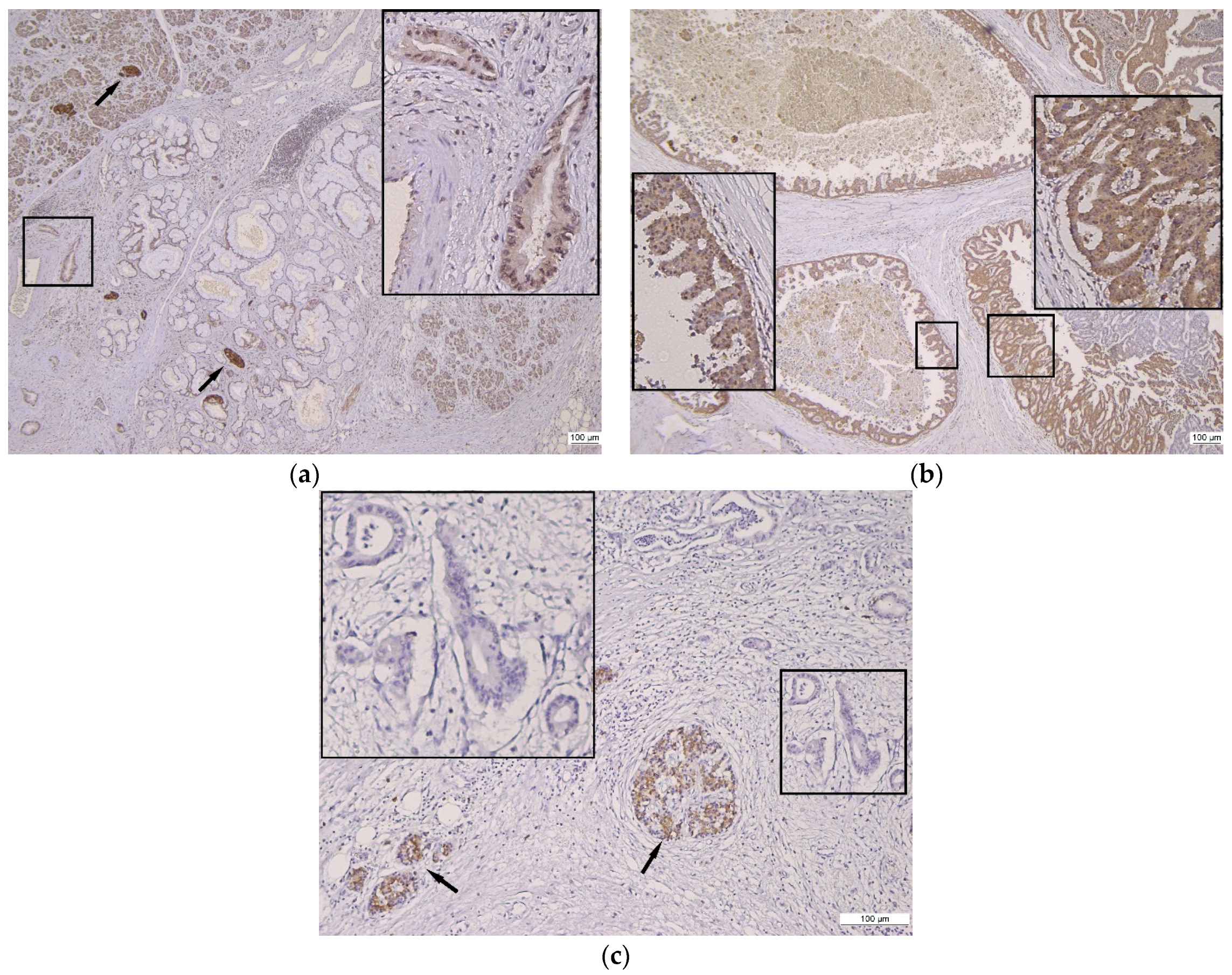
3.2. Qualitative Assessment of Gal8 Immunoexpression
3.3. Semi-Quantitative Assessment of Gal8 Immunoexpression
3.4. Correlation between Gal8 Immunoexpression and Clinicopathological Characteristics
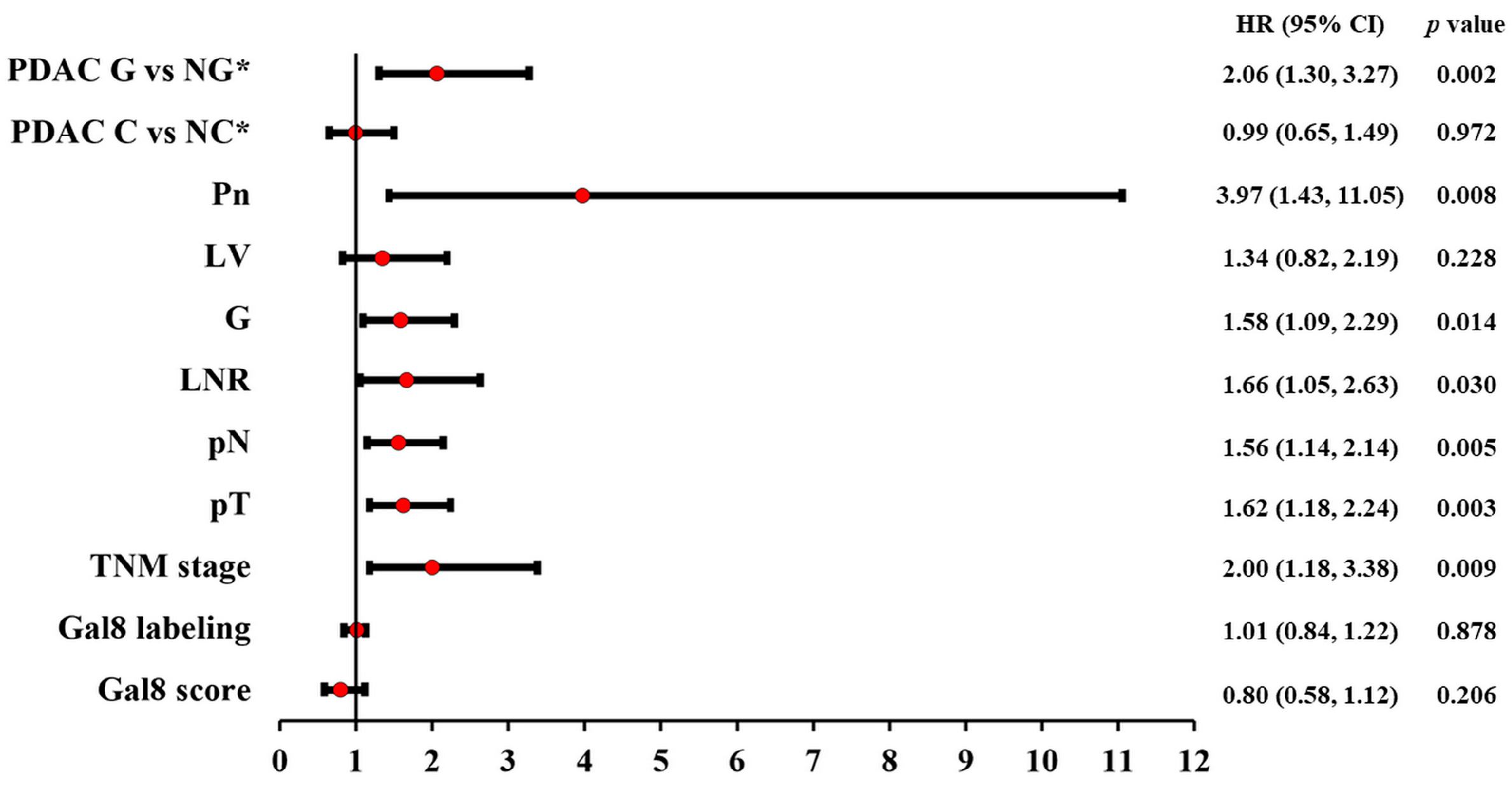
3.5. Correlation between Gal8 Immunoexpression and Survival
4. Discussion
- -
- The histopathological profile of PDAC is complex, and numerous morphological variants have been described, yet this variability cannot currently be directly associated with tumor behavior;
- -
- The molecular profile of PDAC is incompletely defined; we do not have, at this time, confirmed molecular prognostic factors;
- -
- Similarly to breast, colon, gastric, cervical, and prostatic cancer, the Gal8 heterogeneity in PDAC requires its investigation in correlation with the clinicopathological characteristics and survival parameters, aiming to confirm its potential prognostic value.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Verbeke, C. Morphological heterogeneity in ductal adenocarcinoma of the pancreas—Does it matter? Pancreatology 2016, 16, 295–301. [Google Scholar] [CrossRef]
- Schlitter, A.M.; Segler, A.; Steiger, K.; Michalski, C.W.; Jäger, C.; Konukiewitz, B.; Pfarr, N.; Endris, V.; Bettstetter, M.; Kong, B.; et al. Molecular, morphological and survival analysis of 177 resected pancreatic ductal adenocarcinomas (PDACs): Identification of prognostic subtypes. Sci. Rep. 2017, 7, srep41064. [Google Scholar] [CrossRef]
- Gill, A.J.; Klimstra, D.S.; Lam, A.K.; Washington, M.K. Tumors of the pancreas. In WHO Classification of Tumours of the Digestive System, 5th ed.; Lokuhetty, D., White, V., Watanabe, R., Cree, I., Eds.; IARC Press: Lyon, Frace, 2019; pp. 295–332. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Haeberle, L.; Esposito, I. Pathology of pancreatic cancer. Transl. Gastroenterol. Hepatol. 2019, 4, 50. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. (Eds.) TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Oxford, UK; Hoboken, NJ, USA, 2017. [Google Scholar]
- Verbeke, C.; Webster, F.; Brosens, L.; Campbell, F.; Del Chiaro, M.; Esposito, I.; Feakins, R.M.; Fukushima, N.; Gill, A.J.; Kakar, S.; et al. Dataset for the reporting of carcinoma of the exocrine pancreas: Recommendations from the International Collaboration on Cancer Reporting (ICCR). Histopathology 2021, 79, 902–912. [Google Scholar] [CrossRef]
- O’Kane, G.M.; Grünwald, B.T.; Jang, G.-H.; Masoomian, M.; Picardo, S.; Grant, R.C.; Denroche, R.E.; Zhang, A.; Wang, Y.; Lam, B.; et al. GATA6 Expression Distinguishes Classical and Basal-like Subtypes in Advanced Pancreatic Cancer. Clin. Cancer Res. 2020, 26, 4901–4910. [Google Scholar] [CrossRef]
- Kalimuthu, S.N.; Wilson, G.W.; Grant, R.C.; Seto, M.; O’kane, G.; Vajpeyi, R.; Notta, F.; Gallinger, S.; Chetty, R. Morphological classification of pancreatic ductal adenocarcinoma that predicts molecular subtypes and correlates with clinical outcome. Gut 2020, 69, 317–328. [Google Scholar] [CrossRef]
- Girotti, M.R.; Salatino, M.; Dalotto-Moreno, T.; Rabinovich, G.A. Sweetening the hallmarks of cancer: Galectins as multifunctional mediators of tumor progression. J. Exp. Med. 2020, 217, e20182041. [Google Scholar] [CrossRef]
- Manero-Rupérez, N.; Martínez-Bosch, N.; Barranco, L.E.; Visa, L.; Navarro, P. The Galectin Family as Molecular Targets: Hopes for Defeating Pancreatic Cancer. Cells 2020, 9, 689. [Google Scholar] [CrossRef]
- Johannes, L.; Jacob, R.; Leffler, H. Galectins at a glance. J. Cell. Sci. 2018, 131, jcs208884. [Google Scholar] [CrossRef]
- Fernández, M.M.; Ferragut, F.; Delgado, V.M.C.; Bracalente, C.; Bravo, A.I.; Cagnoni, A.J.; Nuñez, M.; Morosi, L.G.; Quinta, H.R.; Espelt, M.V.; et al. Glycosylation-dependent binding of galectin-8 to activated leukocyte cell adhesion molecule (ALCAM/CD166) promotes its surface segregation on breast cancer cells. Biochim. Biophys. Acta 2016, 1860, 2255–2268. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Sancho, A.; Chung, W.-L.; Vinik, Y.; Groll, J.; Zick, Y.; Medalia, O.; Bershadsky, A.D.; Geiger, B. Differential cellular responses to adhesive interactions with galectin-8- and fibronectin-coated substrates. J. Cell Sci. 2021, 134, jcs252221. [Google Scholar] [CrossRef] [PubMed]
- Beyer, S.; Wehrmann, M.; Meister, S.; Kolben, T.M.; Trillsch, F.; Burges, A.; Czogalla, B.; Schmoeckel, E.; Mahner, S.; Jeschke, U.; et al. Galectin-8 and -9 as prognostic factors for cervical cancer. Arch. Gynecol. Obstet. 2022, 306, 1211–1220. [Google Scholar] [CrossRef] [PubMed]
- Nagy, N.; Bronckart, Y.; Camby, I.; Legendre, H.; Lahm, H.; Kaltner, H.; Hadari, Y.; Van Ham, P.; Yeaton, P.; Pector, J.-C.; et al. Galectin-8 expression decreases in cancer compared with normal and dysplastic human colon tissue and acts significantly on human colon cancer cell migration as a suppressor. Gut 2002, 50, 392–401. [Google Scholar] [CrossRef]
- Gentilini, L.D.; Jaworski, F.M.; Tiraboschi, C.; Pérez, I.G.; Kotler, M.L.; Chauchereau, A.; Laderach, D.J.; Compagno, D. Stable and high expression of Galectin-8 tightly controls metastatic progression of prostate cancer. Oncotarget 2017, 8, 44654–44668. [Google Scholar] [CrossRef]
- Wu, S.; Liu, H.; Zhang, H.; Lin, C.; Li, R.; Cao, Y.; He, H.; Li, H.; Shen, Z.; Qin, J.; et al. Galectin-8 is associated with recurrence and survival of patients with non-metastatic gastric cancer after surgery. Tumor Biol. 2016, 37, 12635–12642. [Google Scholar] [CrossRef]
- Grosset, A.-A.; Labrie, M.; Vladoiu, M.C.; Yousef, E.M.; Gaboury, L.; St-Pierre, Y. Galectin signatures contribute to the heterogeneity of breast cancer and provide new prognostic information and therapeutic targets. Oncotarget 2016, 7, 18183–18203. [Google Scholar] [CrossRef]
- Danguy, A.; Rorive, S.; Decaestecker, C.; Bronckart, Y.; Kaltner, H.; Hadari, Y.R.; Goren, R.; Zich, Y.; Petein, M.; Salmon, I.; et al. Immunohistochemical profile of galectin-8 expression in benign and malignant tumors of epithelial, mesenchymatous and adipous origins, and of the nervous system. Histol. Histopathol. 2001, 16, 861–868. [Google Scholar] [CrossRef]
- Baldwin, S.; Kukar, M.; Gabriel, E.; Attwood, K.; Wilkinson, N.; Hochwald, S.N.; Kuvshinoff, B. Pancreatic cancer metastatic to a limited number of lymph nodes has no impact on outcome. HPB 2016, 18, 523–528. [Google Scholar] [CrossRef]
- Hadari, Y.R.; Paz, K.; Dekel, R.; Mestrovic, T.; Accili, D.; Zick, Y. Galectin-8. A new rat lectin, related to galectin-4. J. Biol. Chem. 1995, 270, 3447–3453. [Google Scholar] [CrossRef]
- Nio-Kobayashi, J. Tissue- and cell-specific localization of galectins, β-galactose-binding animal lectins, and their potential functions in health and disease. Anat. Sci. Int. 2016, 92, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Satelli, A.; Rao, P.S.; Gupta, P.K.; Lockman, P.R.; Srivenugopal, K.S.; Rao, U.S. Varied expression and localization of multiple galectins in different cancer cell lines. Oncol. Rep. 2008, 19, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Schulz, H.; Kuhn, C.; Hofmann, S.; Mayr, D.; Mahner, S.; Jeschke, U.; Schmoeckel, E. Overall Survival of Ovarian Cancer Patients Is Determined by Expression of Galectins-8 and -and-9. Int. J. Mol. Sci. 2018, 19, 323. [Google Scholar] [CrossRef]
- Chen, W.-S.; Cao, Z.; Sugaya, S.; Lopez, M.J.; Sendra, V.G.; Laver, N.; Leffler, H.; Nilsson, U.J.; Fu, J.; Song, J.; et al. Pathological lymphangiogenesis is modulated by galectin-8-dependent crosstalk between podoplanin and integrin-associated VEGFR-3. Nat. Commun. 2016, 7, 11302. [Google Scholar] [CrossRef] [PubMed]
- Duray, A.; DE Maesschalck, T.; Decaestecker, C.; Remmelink, M.; Chantrain, G.; Neiveyans, J.; Horoi, M.; Leroy, X.; Gabius, H.-J.; Saussez, S. Galectin fingerprinting in naso-sinusal diseases. Oncol. Rep. 2014, 32, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.M.C.; Nugnes, L.G.; Colombo, L.L.; Troncoso, M.F.; Fernández, M.M.; Malchiodi, E.L.; Frahm, I.; Croci, D.O.; Compagno, D.; Rabinovich, G.A.; et al. Modulation of endothelial cell migration and angiogenesis: A novel function for the “tandem-repeat” lectin galectin-8. FASEB J. 2010, 25, 242–254. [Google Scholar] [CrossRef]
- Kahlert, C.; Weber, H.; Mogler, C.; Bergmann, F.; Schirmacher, P.; Kenngott, H.G.; Matterne, U.; Mollberg, N.; Rahbari, N.N.; Hinz, U.; et al. Increased expression of ALCAM/CD166 in pancreatic cancer is an independent prognostic marker for poor survival and early tumour relapse. Br. J. Cancer 2009, 101, 457–464. [Google Scholar] [CrossRef]
- Fujiwara, K.; Ohuchida, K.; Sada, M.; Horioka, K.; Ulrich, C.D., 3rd; Shindo, K.; Ohtsuka, T.; Takahata, S.; Mizumoto, K.; Oda, Y.; et al. CD166/ALCAM Expression Is Characteristic of Tumorigenicity and Invasive and Migratory Activities of Pancreatic Cancer Cells. PLoS ONE 2014, 9, e107247. [Google Scholar] [CrossRef]
- Amantini, C.; Morelli, M.B.; Nabissi, M.; Piva, F.; Marinelli, O.; Maggi, F.; Bianchi, F.; Bittoni, A.; Berardi, R.; Giampieri, R.; et al. Expression Profiling of Circulating Tumor Cells in Pancreatic Ductal Adenocarcinoma Patients: Biomarkers Predicting Overall Survival. Front. Oncol. 2019, 9, 874. [Google Scholar] [CrossRef]
- Yang, Y.; Sanders, A.J.; Ruge, F.; Dong, X.; Cui, Y.; Dou, Q.P.; Jia, S.; Hao, C.; Ji, J.; Jiang, W.G. Activated leukocyte cell adhesion molecule (ALCAM)/CD166 in pancreatic cancer, a pivotal link to clinical outcome and vascular embolism. Am. J. Cancer Res. 2021, 11, 5917–5932. [Google Scholar]
- Ferragut, F.; Cagnoni, A.J.; Colombo, L.L.; Terrero, C.S.; Wolfenstein-Todel, C.; Troncoso, M.F.; Vanzulli, S.I.; Rabinovich, G.A.; Mariño, K.V.; Elola, M.T. Dual knockdown of Galectin-8 and its glycosylated ligand, the activated leukocyte cell adhesion molecule (ALCAM/CD166), synergistically delays in vivo breast cancer growth. Biochim. Biophys. Acta Mol. Cell. Res. 2019, 1866, 1338–1352. [Google Scholar] [CrossRef] [PubMed]
- Renard, H.-F.; Tyckaert, F.; Giudice, C.L.; Hirsch, T.; Valades-Cruz, C.A.; Lemaigre, C.; Shafaq-Zadah, M.; Wunder, C.; Wattiez, R.; Johannes, L.; et al. Endophilin-A3 and Galectin-8 control the clathrin-independent endocytosis of CD166. Nat. Commun. 2020, 11, 1457. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Michalski, C.W.; Kong, B.; Zhang, W.; Raggi, M.C.; Sauliunaite, D.; De Oliveira, T.; Friess, H.; Kleeff, J. ALCAM is associated with chemoresistance and tumor cell adhesion in pancreatic cancer. J. Surg. Oncol. 2010, 101, 564–569. [Google Scholar] [CrossRef]
- Zhang, W.-W.; Zhan, S.-H.; Geng, C.-X.; Sun, X.; Erkan, M.; Kleeff, J.; Xie, X.-J. Activated leukocyte cell adhesion molecule regulates the interaction between pancreatic cancer cells and stellate cells. Mol. Med. Rep. 2016, 14, 3627–3633. [Google Scholar] [CrossRef] [PubMed]
- Ferragut, F.; Vachetta, V.S.; Troncoso, M.F.; Rabinovich, G.A.; Elola, M.T. ALCAM/CD166: A pleiotropic mediator of cell adhesion, stemness and cancer progression. Cytokine Growth Factor Rev. 2021, 61, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Trebo, A.; Ditsch, N.; Kuhn, C.; Heidegger, H.H.; Zeder-Goess, C.; Kolben, T.; Czogalla, B.; Schmoeckel, E.; Mahner, S.; Jeschke, U.; et al. High Galectin-7 and Low Galectin-8 Expression and the Combination of both are Negative Prognosticators for Breast Cancer Patients. Cancers 2020, 12, 953. [Google Scholar] [CrossRef]
- Levy, Y.; Arbel-Goren, R.; Hadari, Y.R.; Eshhar, S.; Ronen, D.; Elhanany, E.; Geiger, B.; Zick, Y. Galectin-8 Functions as a Matricellular Modulator of Cell Adhesion. J. Biol. Chem. 2001, 276, 31285–31295. [Google Scholar] [CrossRef]
- Zick, Y.; Eisenstein, M.; Goren, R.A.; Hadari, Y.R.; Levy, Y.; Ronen, D. Role of galectin-8 as a modulator of cell adhesion and cell growth. Glycoconj. J. 2002, 19, 517–526. [Google Scholar] [CrossRef]
- Cueni, L.N.; Detmar, M. Galectin-8 interacts with podoplanin and modulates lymphatic endothelial cell functions. Exp. Cell Res. 2009, 315, 1715–1723. [Google Scholar] [CrossRef]
- Cattaneo, V.; Tribulatti, M.V.; Carabelli, J.; Carestia, A.; Schattner, M.; Campetella, O. Galectin-8 elicits pro-inflammatory activities in the endothelium. Glycobiology 2014, 24, 966–973. [Google Scholar] [CrossRef]
- Tribulatti, M.V.; Carabelli, J.; Prato, C.A.; Campetella, O. Galectin-8 in the onset of the immune response and inflammation. Glycobiology 2020, 30, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Laderach, D.J.; Compagno, D. Unraveling How Tumor-Derived Galectins Contribute to Anti-Cancer Immunity Failure. Cancers 2021, 13, 4529. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | Gal8 Negative Score | Gal8 Low Score | Gal8 High Score | p Value |
|---|---|---|---|---|
| Gender | ||||
| Female | 12 (60%) | 26 (55.32%) | 8 (40%) | 0.39 |
| Male | 8 (40%) | 21 (44.68%) | 12 (60%) | |
| Age | ||||
| ≤50 years | 3 (15%) | 6 (12.77%) | 3 (15%) | |
| 51–70 years | 14 (70%) | 30 (63.83%) | 12 (60%) | 0.94 |
| >70 years | 3 (15%) | 11 (23.40%) | 5 (25%) | |
| Tumor size | ||||
| ≤4 cm | 8 (40%) | 30 (63.82%) | 17 (85%) | 0.01 |
| >4 cm | 12 (60%) | 17 (36.17%) | 3 (15%) | |
| T stage | ||||
| T1 | 1 (5%) | 5 (10.63%) | 3 (15%) | |
| T2 | 7 (35%) | 25 (53.19%) | 14 (70%) | 0.07 |
| T3 | 11 (55%) | 17 (36.17%) | 2 (10%) | |
| T4 | 1 (5%) | 0 (0%) | 1 (5%) | |
| N stage | ||||
| N0 | 5 (25%) | 16 (34.04%) | 3 (15%) | |
| N1 | 8 (40%) | 26 (55.31%) | 9 (45%) | 0.04 |
| N2 | 7 (35%) | 5 (10.63%) | 8 (40%) | |
| Lymph node ratio | ||||
| LNR ≤ 0.08 | 15 (75%) | 25 (53.20%) | 15 (75%) | 0.44 |
| LNR > 0.08 | 5 (25%) | 22 (46.80%) | 5 (25%) | |
| TNM stage | ||||
| Low (Ia, Ib, IIa) | 4 (25%) | 16 (34.04%) | 3 (15%) | 0.20 |
| High (IIb, III, IV) | 16 (75%) | 31 (65.96%) | 17 (85%) | |
| Tumor grade | ||||
| G1 | 6 (30%) | 12 (25.53%) | 2 (10%) | |
| G2 | 10 (50%) | 32 (68.09%) | 17 (85%) | 0.13 |
| G3 | 4 (20%) | 3 (6.38%) | 1 (5%) | |
| Lympho-vascular invasion | ||||
| LV0 | 4 (20%) | 20 (42.55%) | 3 (15%) | 0.03 |
| LV1 | 16 (80%) | 27 (57.44%) | 17 (85%) | |
| Perineural invasion | ||||
| Pn0 | 0 (0%) | 4 (8.5%) | 2 (10%) | 0.53 |
| Pn1 | 20 (100%) | 43 (91.5%) | 18 (90%) | |
| Pattern-based classification | ||||
| Conventional PDAC | 12 (60%) | 31 (65.95%) | 14 (70%) | 0.79 |
| Non-conventional PDAC | 8 (40%) | 16 (34.05%) | 6 (30%) | |
| Glandular PDAC | 10 (50%) | 26 (55.32%) | 13 (65%) | 0.61 |
| Non-glandular PDAC | 10 (50%) | 21 (44.68%) | 7 (35%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusu, A.; Caruntu, I.-D.; Lozneanu, L.; Ciobanu, D.G.; Amalinei, C.; Giusca, S.-E. Galectin-8 Immunohistochemical Profile in Pancreatic Ductal Adenocarcinoma: Emerging Evidence for Its Prognostic Role. Diagnostics 2023, 13, 3215. https://doi.org/10.3390/diagnostics13203215
Rusu A, Caruntu I-D, Lozneanu L, Ciobanu DG, Amalinei C, Giusca S-E. Galectin-8 Immunohistochemical Profile in Pancreatic Ductal Adenocarcinoma: Emerging Evidence for Its Prognostic Role. Diagnostics. 2023; 13(20):3215. https://doi.org/10.3390/diagnostics13203215
Chicago/Turabian StyleRusu, Andreea, Irina-Draga Caruntu, Ludmila Lozneanu, Delia Gabriela Ciobanu, Cornelia Amalinei, and Simona-Eliza Giusca. 2023. "Galectin-8 Immunohistochemical Profile in Pancreatic Ductal Adenocarcinoma: Emerging Evidence for Its Prognostic Role" Diagnostics 13, no. 20: 3215. https://doi.org/10.3390/diagnostics13203215