
Prognostic Role of CD200 in Acute Lymphoblastic Leukemia Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Immunophenotyping
2.2. Statistical Analysis
3. Results
3.1. Subsection
3.1.1. The Clinical and Laboratory Characteristics
3.1.2. Immunophenotyping
CD200 Expression in the B-ALL Group and the Control Group
Relation between CD200 Expression and Different Parameters
CD200 Expression and Other B-Cell Markers
CD200 Cutoff Value
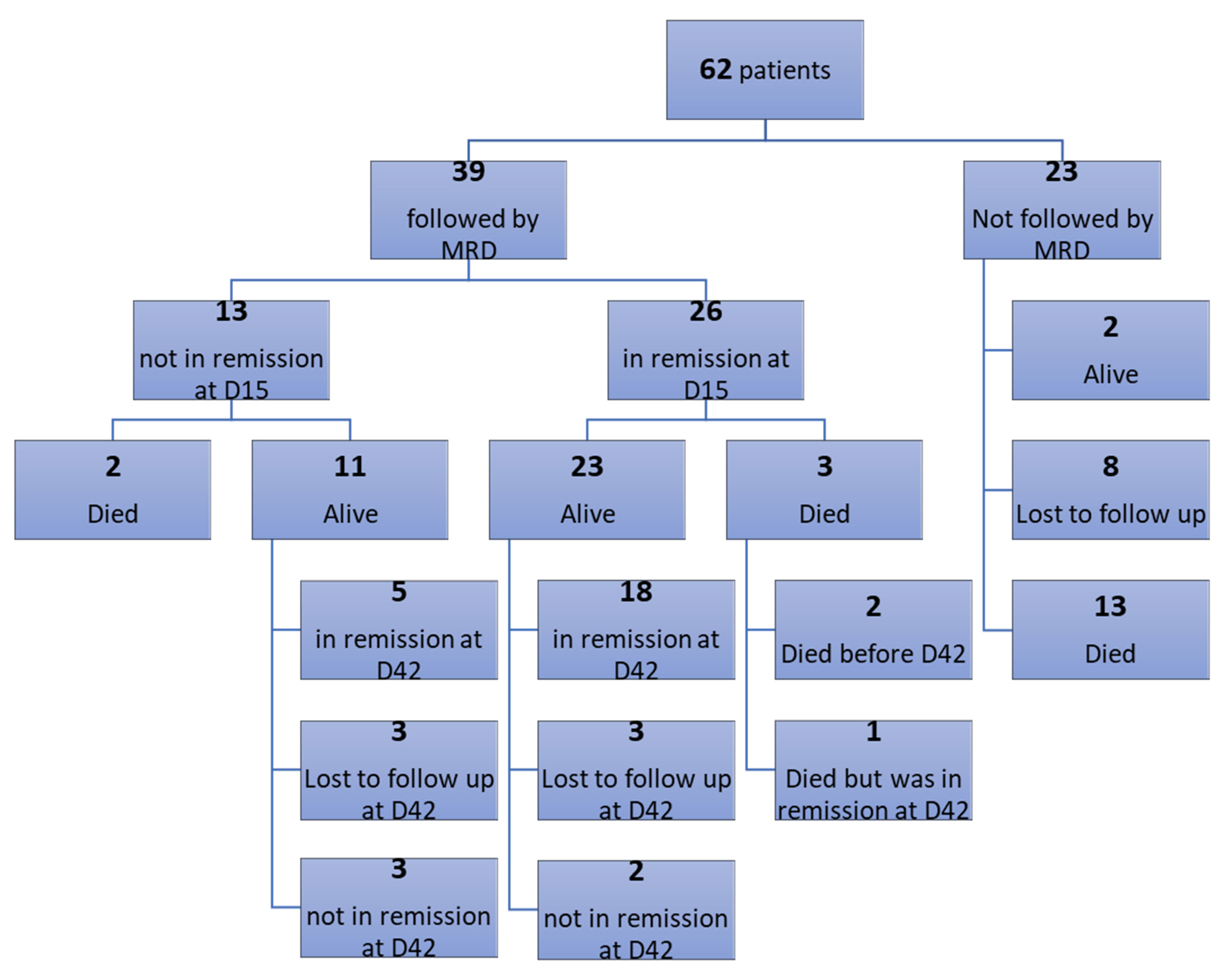
3.1.3. Clinical Outcome and Follow-Up
Overall Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Faderl, S.; O’Brien, S.; Pui, C.-H.; Stock, W.; Wetzler, M.; Hoelzer, D.; Kantarjian, H.M. Adult acute lymphoblastic leukemia: Concepts and strategies. Cancer 2010, 116, 1165–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biondi, A.; Cazzaniga, G. Novel clinical trials for pediatric leukemias: Lessons learned from genomic analyses. Hematology 2013, 2013, 612–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borowitz, M.J.; Devidas, M.; Hunger, S.P.; Bowman, W.P.; Carroll, A.J.; Carroll, W.L.; Linda, S.; Martin, P.L.; Pullen, D.J.; Viswanatha, D.; et al. Clinical significance of minimal residual disease in childhood acute lymphoblastic leukemia and its relationship to other prognostic factors: A Children’s Oncology Group study. Blood 2008, 111, 5477–5485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerst, G.; Kreyenberg, H.; Roth, C.; Well, C.; Dietz, K.; Coustan-Smith, E.; Campana, D.; Koscielniak, E.; Niemeyer, C.; Schlegel, P.G.; et al. Concurrent detection of minimal residual disease (MRD) in childhood acute lymphoblastic leukaemia by flow cytometry and real-time PCR. Br. J. Haematol. 2005, 128, 774–782. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, B.T.; Farrar, W.L. Cancer stem cells, CD200 and immunoevasion. Trends Immunol. 2008, 29, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Coustan-Smith, E.; Song, G.; Clark, C.; Key, L.; Liu, P.; Mehrpooya, M.; Stow, P.; Su, X.; Shurtleff, S.; Pui, C.-H.; et al. New markers for minimal residual disease detection in acute lymphoblastic leukemia. Blood 2011, 117, 6267–6276. [Google Scholar] [CrossRef] [PubMed]
- Alwan, M.J.; Al-Mudallel, S.S. Prognostic impact of CD200 expression in pediatric B-cell acute lymphoblastic leukemia. Med. J. Babylon 2021, 18, 358. [Google Scholar]
- Cox, C.V.; Diamanti, P.; Blair, A. Does Expression Of CD200 Provide a Target For LIC In Childhood ALL? Blood 2013, 122, 2894. [Google Scholar] [CrossRef]
- Dworzak, M.N.; Gaipa, G.; Schumich, A.; Maglia, O.; Ratei, R.; Veltroni, M.; Husak, Z.; Basso, G.; Karawajew, L.; Gadner, H.; et al. Modulation of antigen expression in B-cell precursor acute lymphoblastic leukemia during induction therapy is partly transient: Evidence for a drug-induced regulatory phenomenon. Results of the AIEOP-BFM-ALL-FLOW-MRD-Study Group. Cytom. Part B Clin. Cytom. 2010, 78, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Wongprajun, S.; Auewarakul, C.U. A method comparison study of flow cytometry and cytomorphology to determine the percentages of blasts in patients with acute leukemia after induction and consolidation chemotherapy. J. Med. Assoc. Thai 2010, 93, S157–S164. [Google Scholar] [PubMed]
- Mallick, D.; Karmakar, R.; Barui, G.; Gon, S.; Chakrabarti, S. The Prognostic Significance of HbF in Childhood Haematological Malignancies. Indian J. Hematol. Blood Transfus. 2015, 31, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.manualslib.com/manual/1336895/Beckman-Coulter-Navios.html?page=300&term=prism&selected=3#manual (accessed on 31 December 2022).
- Howlader, N.; Noone, A.-M.; Krapcho, M.; Garshell, J.; Neyman, N.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z. SEER Cancer Statistics Review, 1975–2010. National Cancer Institute; 2014. Available online: https://seer.cancer.gov/archive/csr/1975_2010/ (accessed on 7 November 2022).
- Lustosa de Sousa, D.W.; de Almeida Ferreira, F.V.; Cavalcante Félix, F.H.; de Oliveira Lopes, M.V. Acute lymphoblastic leukemia in children and adolescents: Prognostic factors and analysis of survival. Rev. Bras. Hematol. Hemoter. 2015, 37, 223–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverman, L.B. Improved outcome for children with acute lymphoblastic leukemia: Results of Dana-Farber Consortium Protocol 91-01. Blood 2001, 97, 1211–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aricò, M.; Valsecchi, M.G.; Rizzari, C.; Barisone, E.; Biondi, A.; Casale, F.; Locatelli, F.; Lo Nigro, L.; Luciani, M.; Messina, C.; et al. Long-Term Results of the AIEOP-ALL-95 Trial for Childhood Acute Lymphoblastic Leukemia: Insight on the Prognostic Value of DNA Index in the Framework of Berlin-Frankfurt-Muenster–Based Chemotherapy. J. Clin. Oncol. 2008, 26, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Alapat, D.; Coviello-Malle, J.; Owens, R.; Qu, P.; Barlogie, B.; Shaughnessy, J.D.; Lorsbach, R.B. Diagnostic usefulness and prognostic impact of CD200 expression in lymphoid malignancies and plasma cell myeloma. Am. J. Clin. Pathol. 2012, 137, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorfman, D.M.; Shahsafaei, A. CD200 (OX-2 Membrane Glycoprotein) Expression in B Cell–Derived Neoplasms. Am. J. Clin. Pathol. 2010, 134, 726–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aref, S.; Azmy, E.; El-bakry, K.; Ibrahim, L.; Abdel Aziz, S. Prognostic impact of CD200 and CD56 expression in pediatric B-cell acute lymphoblastic leukemia patients. Pediatr. Hematol. Oncol. 2017, 34, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Diamanti, P.; Cox, C.V.; Ede, B.C.; Uger, R.A.; Moppett, J.P.; Blair, A. Targeting pediatric leukemia-propagating cells with anti-CD200 antibody therapy. Blood Adv. 2021, 5, 3694–3708. [Google Scholar] [CrossRef] [PubMed]
- Awad, S.; Kamel, M.M.; Ayoub, M.A.; Kamel, A.M.; Elnoshokaty, E.; El Hifnawi, N. Immunophenotypic Characterization of Cytogenetic subgroups in Egyptian Pediatric B-Acute Lymphoblastic Leukemia Patients. Clin. Lymphoma Myeloma Leuk. 2015, 15, S1. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Mean | Standard Deviation | p-Value * | ||
|---|---|---|---|---|---|
| Age | adults | 14 | 43.571 | 17.99 | |
| children | 48 | 6.279 | 5.188 | ||
| Sex (male to female ratio) | 40/22 | - | - | ||
| TLC | <50,000 | 49 | 62.4776 | 23.88601 | 0.001 |
| ≥50,000 | 13 | 80.0000 | 12.81926 | ||
| HB | <10 | 48 | 70.2792 | 20.52762 | 0.03 |
| ≥10 | 14 | 52.0000 | 26.43715 | ||
| PLT | <50 | 30 | 61.2333 | 23.45161 | 0.11 |
| ≥50 | 32 | 70.7625 | 22.11200 |
| Cytogenetics | N | Mean ± SD | p-Value * |
|---|---|---|---|
| Normal | 12 | 28.53 ± 5 | 0.005 |
| Abnormal | 23 | 12.26 ± 3.5 |
| Karyotyping | N | Mean ± SD | p-Value * |
|---|---|---|---|
| Hyper-diploid | 13 | 56.7 ± 33 | 0.389 |
| Other abnormal karyotype | 10 | 66.8 ± 21.8 |
| MRD D15 | MRD D42 | |||
|---|---|---|---|---|
| Blasts (%) | negative (N = 26) | positive (N = 13) | negative (N = 23) | positive (N = 5) |
| <5 | 26 (100%) | 7 (53.8%) | 23 (100%) | 5 (100%) |
| ≥5 | 0 (0%) | 6 (46.2%) | 0 (0%) | 0 (0%) |
| CD200 % | p-Value * | ||||
|---|---|---|---|---|---|
| ≤60% | >60% | ||||
| Count | % | Count | % | ||
| MRD D15 | |||||
| −ve | 8 | 72.7 | 18 | 64.3 | 0.72 |
| +ve | 3 | 27.3 | 10 | 35.7 | |
| MRD D42 | |||||
| −ve | 6 | 100 | 17 | 77.3 | 0.55 |
| +ve | 0 | 0 | 5 | 22.7 | |
| MRD 15 | p-Value * | ||||
|---|---|---|---|---|---|
| −VE | +VE | ||||
| PRISM | −VE | Count | 11 | 0 | <0.001 |
| % within PRISM | 100.0% | 0.0% | |||
| % within MRD 15 | 84.6% | 0.0% | |||
| +VE | Count | 2 | 7 | ||
| % within PRISM | 22.2% | 77.8% | |||
| % within MRD 15 | 15.4% | 100.0% | |||
| Death | MRD D15 | p-Value * | |
|---|---|---|---|
| −ve (N = 26) | +ve (N = 13) | ||
| Yes | 3 (11.5%) | 2 (15.4%) | 1.0 |
| No | 23 (88.5%) | 11 (84.6%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khalil, M.; Elsharkawy, N.; Elmawardy, M.M.; Ayoub, M.A. Prognostic Role of CD200 in Acute Lymphoblastic Leukemia Patients. Diagnostics 2023, 13, 325. https://doi.org/10.3390/diagnostics13020325
Khalil M, Elsharkawy N, Elmawardy MM, Ayoub MA. Prognostic Role of CD200 in Acute Lymphoblastic Leukemia Patients. Diagnostics. 2023; 13(2):325. https://doi.org/10.3390/diagnostics13020325
Chicago/Turabian StyleKhalil, Mohamed, Nahla Elsharkawy, Mona Mohsen Elmawardy, and Mahmoud Aly Ayoub. 2023. "Prognostic Role of CD200 in Acute Lymphoblastic Leukemia Patients" Diagnostics 13, no. 2: 325. https://doi.org/10.3390/diagnostics13020325