
The Correlation between the Vascular Calcification Score of the Coronary Artery and the Abdominal Aorta in Patients with Psoriasis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
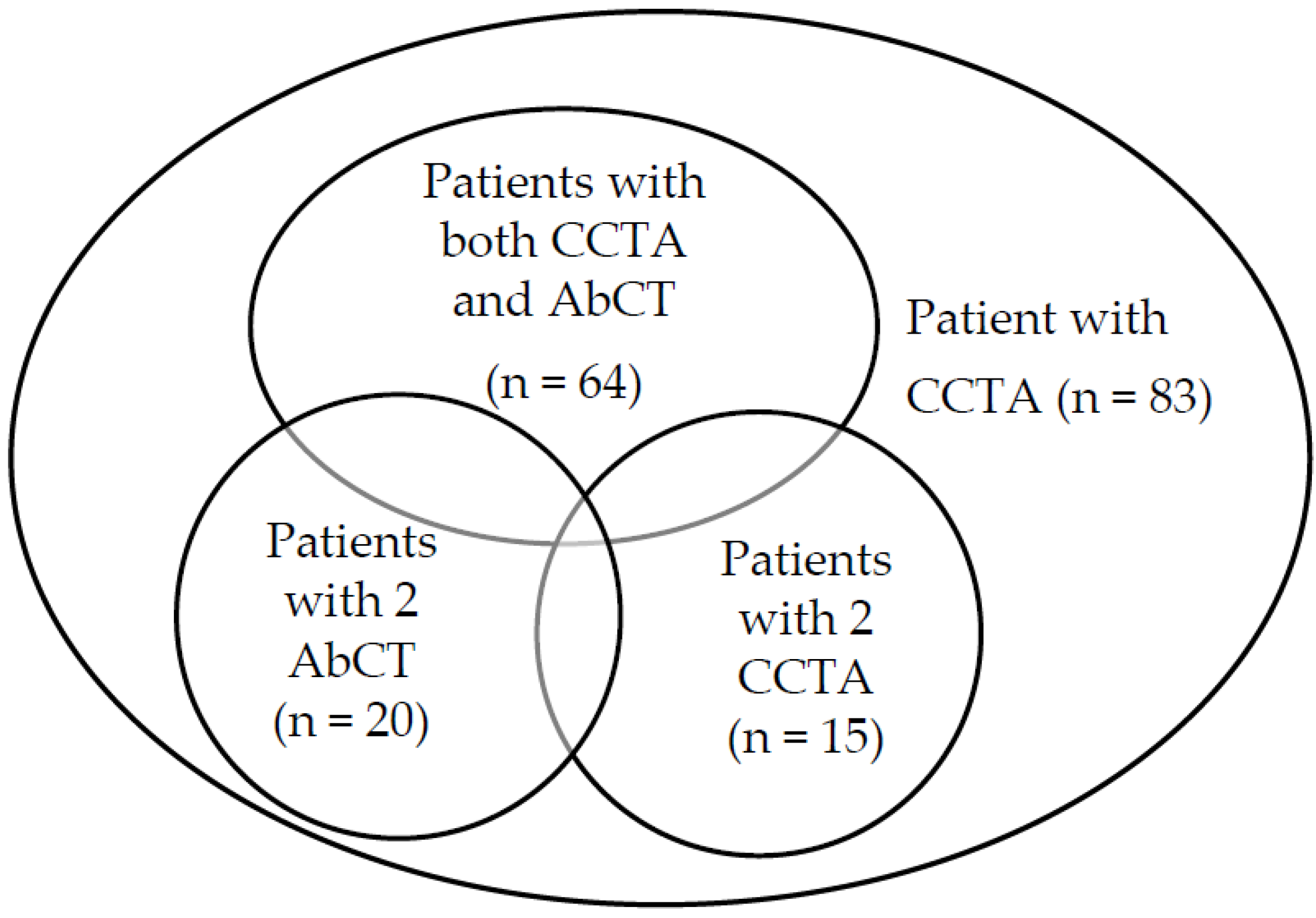
2.1. Study Design
2.2. Demographics, Clinical Measurements, and Laboratory Measurements
2.3. Measurement of CACS and AACS via CT Scan
2.4. Statistical Analysis
3. Results
3.1. Data Description of Participants in the Study
3.2. The Association between CCTA and CACS
3.3. The Association between CCTA and AACS
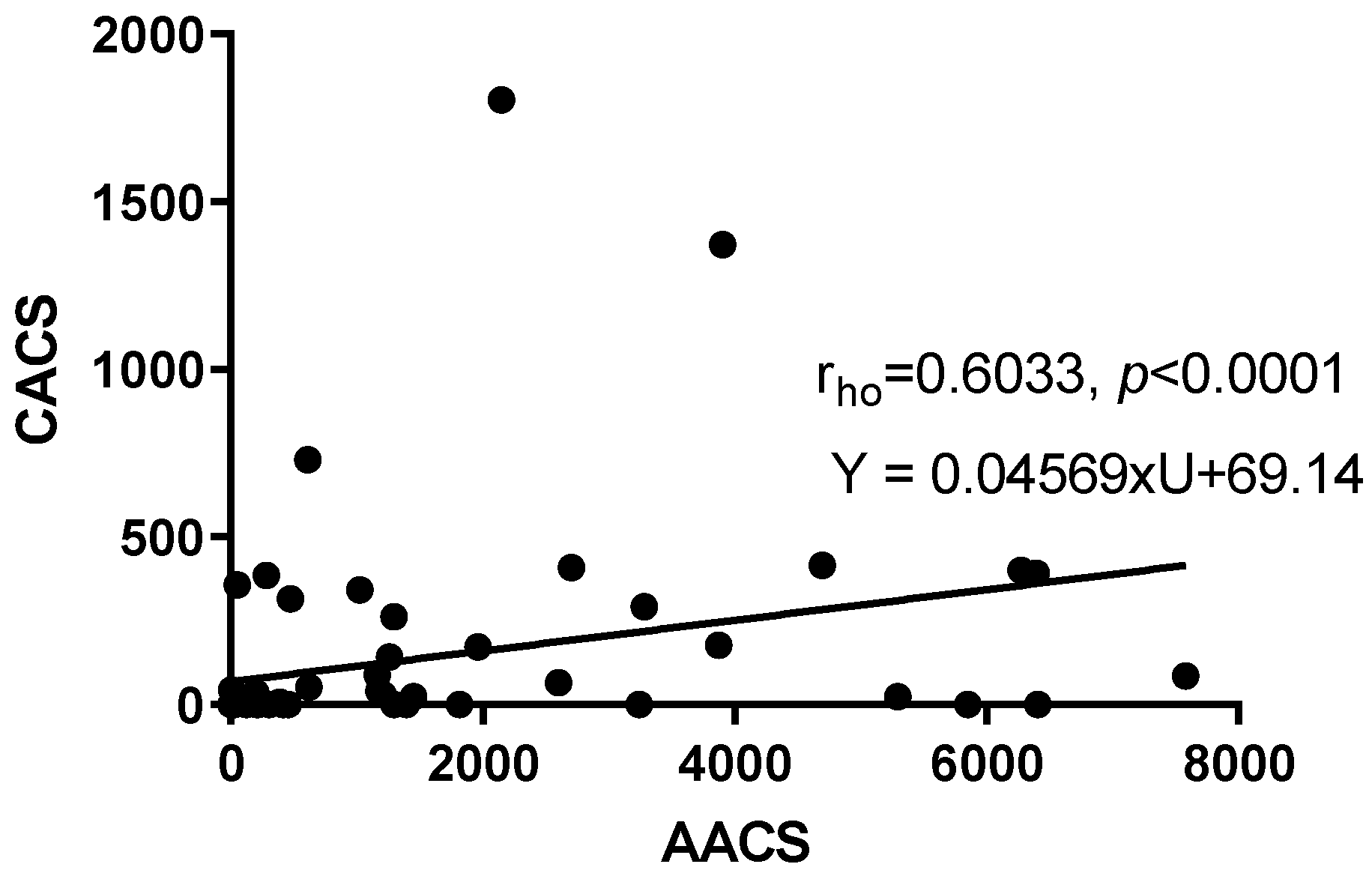
3.4. The Correlation between CACS and AACS
3.5. Discrepancy of CACS and AACS among Subgroups of Variables
3.6. The Role of CACS and AACS in Coronary Artery Involvement Diagnosis
3.7. The Progression of Artery Calcification and Its Correlation with Other Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lee, S.J.; Lee, I.K.; Jeon, J.H. Vascular Calcification-New Insights Into Its Mechanism. Int. J. Mol. Sci. 2020, 21, 2685. [Google Scholar] [CrossRef] [Green Version]
- Sandfort, V.; Lima, J.A.; Bluemke, D.A. Noninvasive Imaging of Atherosclerotic Plaque Progression: Status of Coronary Computed Tomography Angiography. Circ. Cardiovasc. Imaging 2015, 8, e003316. [Google Scholar] [CrossRef] [Green Version]
- Hajhosseiny, R.; Bahaei, T.S.; Prieto, C.; Botnar, R.M. Molecular and Nonmolecular Magnetic Resonance Coronary and Carotid Imaging. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 569–582. [Google Scholar] [CrossRef] [Green Version]
- Abdelrahman, K.M.; Chen, M.Y.; Dey, A.K.; Virmani, R.; Finn, A.V.; Khamis, R.Y.; Choi, A.D.; Min, J.K.; Williams, M.C.; Buckler, A.J.; et al. Coronary Computed Tomography Angiography from Clinical Uses to Emerging Technologies. J. Am. Coll. Cardiol. 2020, 76, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Leow, K.; Szulc, P.; Schousboe, J.T.; Kiel, D.P.; Teixeira-Pinto, A.; Shaikh, H.; Sawang, M.; Sim, M.; Bondonno, N.; Hodgson, J.M.; et al. Prognostic Value of Abdominal Aortic Calcification: A Systematic Review and Meta-Analysis of Observational Studies. J. Am. Heart Assoc. 2021, 10, e017205. [Google Scholar] [CrossRef] [PubMed]
- Bastos Gonçalves, F.; Voûte, M.T.; Hoeks, S.E.; Chonchol, M.B.; Boersma, E.E.; Stolker, R.J.; Verhagen, H.J.M. Calcification of the abdominal aorta as an independent predictor of cardiovascular events: A meta-analysis. Heart 2012, 98, 988. [Google Scholar] [CrossRef]
- Budoff, M.J.; Shaw, L.J.; Liu, S.T.; Weinstein, S.R.; Mosler, T.P.; Tseng, P.H.; Flores, F.R.; Callister, T.Q.; Raggi, P.; Berman, D.S. Long-term prognosis associated with coronary calcification: Observations from a registry of 25,253 patients. J. Am. Coll. Cardiol. 2007, 49, 1860–1870. [Google Scholar] [CrossRef] [Green Version]
- Yamazaki, F.; Takehana, K.; Tanaka, A. Relationship between Psoriasis and Prevalence of Cardiovascular Disease in 88 Japanese Patients. J. Clin. Med. 2021, 10, 3640. [Google Scholar] [CrossRef] [PubMed]
- Jurgens, P.T.; Carr, J.J.; Terry, J.G.; Rana, J.S.; Jacobs, D.R.; Duprez, D.A. Association of Abdominal Aorta Calcium and Coronary Artery Calcium with Incident Cardiovascular and Coronary Heart Disease Events in Black and White Middle-Aged People: The Coronary Artery Risk Development in Young Adults Study. J. Am. Heart Assoc. 2021, 10, e023037. [Google Scholar] [CrossRef]
- Kimura, K.; Saika, Y.; Otani, H.; Fujii, R.; Mune, M.; Yukawa, S. Factors associated with calcification of the abdominal aorta in hemodialysis patients. Kidney Int. Suppl. 1999, 71, S238–S241. [Google Scholar] [CrossRef] [PubMed]
- Reaven, P.D.; Sacks, J. Reduced coronary artery and abdominal aortic calcification in Hispanics with type 2 diabetes. Diabetes Care 2004, 27, 1115–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M.J.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, C.; Bae, K.T.; Pilgram, T.K. Coronary artery calcium: Accuracy and reproducibility of measurements with multi-detector row CT—Assessment of effects of different thresholds and quantification methods. Radiology 2003, 227, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Fujiyoshi, A.; Miura, K.; Ohkubo, T.; Kadowaki, T.; Kadowaki, S.; Zaid, M.; Hisamatsu, T.; Sekikawa, A.; Budoff, M.J.; Liu, K.; et al. Cross-sectional comparison of coronary artery calcium scores between Caucasian men in the United States and Japanese men in Japan: The multi-ethnic study of atherosclerosis and the Shiga epidemiological study of subclinical atherosclerosis. Am. J. Epidemiol. 2014, 180, 590–598. [Google Scholar] [CrossRef] [Green Version]
- Yamazoe, M.; Hisamatsu, T.; Miura, K.; Kadowaki, S.; Zaid, M.; Kadota, A.; Torii, S.; Miyazawa, I.; Fujiyoshi, A.; Arima, H.; et al. Relationship of Insulin Resistance to Prevalence and Progression of Coronary Artery Calcification beyond Metabolic Syndrome Components: Shiga Epidemiological Study of Subclinical Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 1703–1708. [Google Scholar] [CrossRef] [Green Version]
- Rosen, B.D.; Fernandes, V.; McClelland, R.L.; Carr, J.J.; Detrano, R.; Bluemke, D.A.; Lima, J.A. Relationship between baseline coronary calcium score and demonstration of coronary artery stenoses during follow-up MESA (Multi-Ethnic Study of Atherosclerosis). JACC Cardiovasc. Imaging 2009, 2, 1175–1183. [Google Scholar] [CrossRef] [Green Version]
- Hokanson, J.E.; MacKenzie, T.; Kinney, G.; Snell-Bergeon, J.K.; Dabelea, D.; Ehrlich, J.; Eckel, R.H.; Rewers, M. Evaluating changes in coronary artery calcium: An analytic method that accounts for interscan variability. Am. J. Roentgenol. 2004, 182, 1327–1332. [Google Scholar] [CrossRef]
- Budoff, M.J.; Hokanson, J.E.; Nasir, K.; Shaw, L.J.; Kinney, G.L.; Chow, D.; Demoss, D.; Nuguri, V.; Nabavi, V.; Ratakonda, R.; et al. Progression of coronary artery calcium predicts all-cause mortality. JACC Cardiovasc. Imaging 2010, 3, 1229–1236. [Google Scholar] [CrossRef] [Green Version]
- Kronmal, R.A.; McClelland, R.L.; Detrano, R.; Shea, S.; Lima, J.A.; Cushman, M.; Bild, D.E.; Burke, G.L. Risk factors for the progression of coronary artery calcification in asymptomatic subjects: Results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 2007, 115, 2722–2730. [Google Scholar] [CrossRef] [Green Version]
- Lerman, J.B.; Joshi, A.A.; Chaturvedi, A.; Aberra, T.M.; Dey, A.K.; Rodante, J.A.; Salahuddin, T.; Chung, J.H.; Rana, A.; Teague, H.L.; et al. Coronary Plaque Characterization in Psoriasis Reveals High-Risk Features That Improve after Treatment in a Prospective Observational Study. Circulation 2017, 136, 263–276. [Google Scholar] [CrossRef]
- Hoffmann, U.; Massaro, J.M.; D’Agostino, R.B.S.; Kathiresan, S.; Fox, C.S.; O’Donnell, C.J. Cardiovascular Event Prediction and Risk Reclassification by Coronary, Aortic, and Valvular Calcification in the Framingham Heart Study. J. Am. Heart Assoc. 2016, 5, e003144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaikriangkrai, K.; Jhun, H.Y.; Shantha, G.P.S.; Abdulhak, A.B.; Sigurdsson, G.; Nabi, F.; Mahmarian, J.J.; Chang, S.M. Coronary artery calcium score as a predictor for incident stroke: Systematic review and meta-analysis. Int. J. Cardiol. 2017, 236, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Hisamatsu, T.; Liu, K.; Chan, C.; Krefman, A.E.; Fujiyoshi, A.; Budoff, M.J.; Miura, K.; Lloyd-Jones, D.M.; Ueshima, H. Coronary Artery Calcium Progression among the US and Japanese Men. Circ. Cardiovasc. Imaging 2019, 12, e008104. [Google Scholar] [CrossRef] [PubMed]
- Criqui, M.H.; Denenberg, J.O.; Ix, J.H.; McClelland, R.L.; Wassel, C.L.; Rifkin, D.E.; Carr, J.J.; Budoff, M.J.; Allison, M.A. Calcium density of coronary artery plaque and risk of incident cardiovascular events. JAMA 2014, 311, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, V.; Masaki, K.; Vishnu, A.; Ye, L.; Wilcox, B.; Wassel, C.; Fujiyoshi, A.; Barinas-Mitchell, E.J.M.; Miura, K.; Ueshima, H.; et al. Progression of coronary artery calcium in Japanese American men and white men in the ERA JUMP study. Int. J. Cardiol. 2017, 228, 672–676. [Google Scholar] [CrossRef]
- Hirata, A.; Kakino, A.; Okamura, T.; Usami, Y.; Fujita, Y.; Kadota, A.; Fujiyoshi, A.; Hisamatsu, T.; Kondo, K.; Segawa, H.; et al. The relationship between serum levels of LOX-1 ligand containing ApoAI as a novel marker of dysfunctional HDL and coronary artery calcification in middle-aged Japanese men. Atherosclerosis 2020, 313, 20–25. [Google Scholar] [CrossRef]
- Criqui, M.H.; Denenberg, J.O.; McClelland, R.L.; Allison, M.A.; Ix, J.H.; Guerci, A.; Cohoon, K.P.; Srikanthan, P.; Watson, K.E.; Wong, N.D. Abdominal aortic calcium, coronary artery calcium, and cardiovascular morbidity and mortality in the Multi-Ethnic Study of Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1574–1579. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.; Fujiyoshi, A.; Willcox, B.; Choo, J.; Vishnu, A.; Hisamatsu, T.; Ahuja, V.; Takashima, N.; Barinas-Mitchell, E.; Kadota, A. Increased aortic calcification is associated with arterial stiffness progression in multiethnic middle-aged men. Hypertension 2017, 69, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, L.; Saliba, W.; Hayeq, H.; Hasadia, R.; Zeina, A.-R. The impact of abdominal fat on abdominal aorta calcification measured on non-enhanced CT. Medicine 2018, 97, e13233. [Google Scholar] [CrossRef]
- Criqui, M.H.; Kamineni, A.; Allison, M.A.; Ix, J.H.; Carr, J.J.; Cushman, M.; Detrano, R.; Post, W.; Wong, N.D. Risk factor differences for aortic versus coronary calcified atherosclerosis: The multiethnic study of atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 2289–2296. [Google Scholar] [CrossRef]
- Elnabawi, Y.A.; Dey, A.K.; Goyal, A.; Groenendyk, J.W.; Chung, J.H.; Belur, A.D.; Rodante, J.; Harrington, C.L.; Teague, H.L.; Baumer, Y.; et al. Coronary artery plaque characteristics and treatment with biologic therapy in severe psoriasis: Results from a prospective observational study. Cardiovasc. Res. 2019, 115, 721–728. [Google Scholar] [CrossRef]
- Choi, H.; Uceda, D.E.; Dey, A.K.; Abdelrahman, K.M.; Aksentijevich, M.; Rodante, J.A.; Elnabawi, Y.A.; Reddy, A.; Keel, A.; Erb-Alvarez, J.; et al. Treatment of Psoriasis with Biologic Therapy Is Associated with Improvement of Coronary Artery Plaque Lipid-Rich Necrotic Core: Results from a Prospective, Observational Study. Circ. Cardiovasc. Imaging 2020, 13, e011199. [Google Scholar] [CrossRef] [PubMed]
- Beigneux, Y.; Sablayrolles, J.L.; Varenne, O.; Mas, J.L.; Calvet, D. Coronary Artery Calcium Score Improves the Prediction of Occult Coronary Artery Stenosis in Ischemic Stroke Patients. J. Am. Heart Assoc. 2016, 5, e003770. [Google Scholar] [CrossRef]
- Nicoll, R.; Wiklund, U.; Zhao, Y.; Diederichsen, A.; Mickley, H.; Ovrehus, K.; Zamorano, P.; Gueret, P.; Schmermund, A.; Maffei, E.; et al. The coronary calcium score is a more accurate predictor of significant coronary stenosis than conventional risk factors in symptomatic patients: Euro-CCAD study. Int. J. Cardiol. 2016, 207, 13–19. [Google Scholar] [CrossRef]
- Kinoshita, R.; Matsunaga, E.; Nishizaki, Y.; Yokoyama, T.; Itou, S.; Miyauchi, K.; Daida, H. Coronary Artery Calcium Score as a Predictor of Coronary Stenosis in Patients with Diabetes Mellitus. J. Jpn. Soc. Coron. Dis. 2012, 18, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Lo-Kioeng-Shioe, M.S.; Rijlaarsdam-Hermsen, D.; van Domburg, R.T.; Hadamitzky, M.; Lima, J.A.C.; Hoeks, S.E.; Deckers, J.W. Prognostic value of coronary artery calcium score in symptomatic individuals: A meta-analysis of 34,000 subjects. Int. J. Cardiol. 2020, 299, 56–62. [Google Scholar] [CrossRef]
- Rahman, E.U.; Chobufo, M.D.; Farah, F.; Elhamdani, A.; Khan, A.; Thompson, E.A.; Aronow, W.S.; El-Hamdani, M. Prevalence and risk factors for the development of abdominal aortic calcification among the US population: NHANES study. Arch. Med. Sci. Atheroscler. Dis. 2021, 6, 95–101. [Google Scholar] [CrossRef]
- Howard, G.; Wagenknecht, L.E.; Burke, G.L.; Diez-Roux, A.; Evans, G.W.; McGovern, P.; Nieto, F.J.; Tell, G.S. Cigarette smoking and progression of atherosclerosis: The Atherosclerosis Risk in Communities (ARIC) Study. JAMA 1998, 279, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, N.; Sang, Y.; Chen, J.; Ballew, S.H.; Kalbaugh, C.A.; Salameh, M.J.; Blaha, M.J.; Allison, M.; Heiss, G.; Selvin, E.; et al. Cigarette Smoking, Smoking Cessation, and Long-Term Risk of 3 Major Atherosclerotic Diseases. J. Am. Coll. Cardiol. 2019, 74, 498–507. [Google Scholar] [CrossRef]
- Mallikethi-Reddy, S.; Rubenfire, M.; Jackson, L.A.; Brook, R.D. Coronary artery calcium in hypertension: A review. J. Am. Soc. Hypertens. JASH 2015, 9, 993–1000. [Google Scholar] [CrossRef]
- Jensky, N.E.; Criqui, M.H.; Wright, M.C.; Wassel, C.L.; Brody, S.A.; Allison, M.A. Blood Pressure and Vascular Calcification. Hypertension 2010, 55, 990–997. [Google Scholar] [CrossRef] [Green Version]
- Kanaya, A.M.; Vittinghoff, E.; Lin, F.; Kandula, N.R.; Herrington, D.; Liu, K.; Blaha, M.; Budoff, M.J. Incidence and Progression of Coronary Artery Calcium in South Asians Compared with 4 Race/Ethnic Groups. J. Am. Heart Assoc. 2019, 8, e011053. [Google Scholar] [CrossRef] [Green Version]
- Kimani, C.; Kadota, A.; Miura, K.; Fujiyoshi, A.; Zaid, M.; Kadowaki, S.; Hisamatsu, T.; Arima, H.; Horie, M.; Ueshima, H.; et al. Differences between Coronary Artery Calcification and Aortic Artery Calcification in Relation to Cardiovascular Disease Risk Factors in Japanese Men. J. Atheroscler. Thromb. 2019, 26, 452–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsushita, M.; Nishikimi, N.; Sakurai, T.; Nimura, Y. Relationship between aortic calcification and atherosclerotic disease in patients with abdominal aortic aneurysm. Int. Angiol. 2000, 19, 276. [Google Scholar] [PubMed]
- Parr, A.; Buttner, P.; Shahzad, A.; Golledge, J. Relation of Infra-Renal Abdominal Aortic Calcific Deposits and Cardiovascular Events in Patients with Peripheral Artery Disease. Am. J. Cardiol. 2010, 105, 895–899. [Google Scholar] [CrossRef]
- Arai, Y.; Hirose, N.; Yamamura, K.; Kimura, M.; Murayama, A.; Fujii, I.; Tsushima, M. Long-Term Effect of Lipid-Lowering Therapy on Atherosclerosis of Abdominal Aorta in Patients with Hypercholesterolemia: Noninvasive Evaluation by a New Image Analysis Program. Angiology 2002, 53, 57–68. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, C.J.; Chazaro, I.; Wilson, P.W.F.; Fox, C.; Hannan, M.T.; Kiel, D.P.; Cupples, L.A. Evidence for Heritability of Abdominal Aortic Calcific Deposits in the Framingham Heart Study. Circulation 2002, 106, 337–341. [Google Scholar] [CrossRef] [Green Version]
- Onuma, O.K.; Pencina, K.; Qazi, S.; Massaro, J.M.; D’Agostino, R.B.S.; Chuang, M.L.; Fox, C.S.; Hoffmann, U.; O’Donnell, C.J. Relation of Risk Factors and Abdominal Aortic Calcium to Progression of Coronary Artery Calcium (from the Framingham Heart Study). Am. J. Cardiol. 2017, 119, 1584–1589. [Google Scholar] [CrossRef] [Green Version]
- Mansouri, B.; Kivelevitch, D.; Natarajan, B.; Joshi, A.A.; Ryan, C.; Benjegerdes, K.; Schussler, J.M.; Rader, D.J.; Reilly, M.P.; Menter, A.; et al. Comparison of Coronary Artery Calcium Scores between Patients with Psoriasis and Type 2 Diabetes. JAMA Dermatol. 2016, 152, 1244–1253. [Google Scholar] [CrossRef] [Green Version]
- Wagenknecht, L.E.; Langefeld, C.D.; Freedman, B.I.; Carr, J.J.; Bowden, D.W. A comparison of risk factors for calcified atherosclerotic plaque in the coronary, carotid, and abdominal aortic arteries: The diabetes heart study. Am. J. Epidemiol. 2007, 166, 340–347. [Google Scholar] [CrossRef]
- Yiu, K.H.; Yeung, C.K.; Zhao, C.T.; Chan, J.C.; Siu, C.W.; Tam, S.; Wong, C.S.; Yan, G.H.; Yue, W.S.; Khong, P.L.; et al. Prevalence and extent of subclinical atherosclerosis in patients with psoriasis. J. Intern. Med. 2013, 273, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Szentpetery, A.; Healy, G.M.; Brady, D.; Haroon, M.; Gallagher, P.; Redmond, C.E.; Fleming, H.; Duignan, J.; Dodd, J.D.; FitzGerald, O. Higher Coronary Plaque Burden in Psoriatic Arthritis Is Independent of Metabolic Syndrome and Associated with Underlying Disease Severity. Arthritis Rheumatol. 2018, 70, 396–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamil, M.; Aslam, R.; Patel, A.; Nadir, B.; Khan, S. Prevalence and Extent of Subclinical Atherosclerosis and Associated Cardiovascular Risk Factors in Adult Patients with Psoriatic Arthritis: A Systematic Review. Cureus 2021, 13, e16853. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnostic Criteria | Cut Points | |
|---|---|---|
| Elevated waist circumference | ≥90 cm (men) | |
| ≥80 cm (women) | ||
| Elevated TG | ≥150 mg/dL | |
| or drug treatment for elevated TG | ||
| Reduced HDL-C | <40 mg/dL (men) | |
| <50 mg/dL (women) | ||
| or drug treatment for reduced HDL-C | ||
| Elevated BP | Systolic BP | ≥130 mmHg |
| Diastolic BP | ≥85 mmHg | |
| or current anti-hypertension treatment | ||
| Elevated fasting glucose | ≥100 mg/dL | |
| or current anti-diabetic treatment | ||
| CT Scan Protocol | Tube Voltage (kVp) | Effective Tube Current (mAs) | Slice Thickness (mm) | Rotation Time (ms) | Threshold (Hounsfield Unit) | Field of View (Reconstruction) (mm) | Scan Collimation (mm) | Convolution Kernel | Reconstruction Matrix (mm) |
|---|---|---|---|---|---|---|---|---|---|
| Coronary | 120 | 380 | 0.75 | 0.28 | 130 | 120–150 | 0.6 | I36f ASA | 512 × 512 |
| Abdominal | 120 | 350 | 5 | 0.5 | 130 | 330 | 1.0 | Q40f | 512 × 512 |
| Coronary Stenosis Severity | Coronary Stenosis Distribution | ||
|---|---|---|---|
| >0–49% | Mild | 1-branch | Mild to severe stenosis of either the LAD, LCx, or RCA |
| 50–74% | Moderate | 2-branch | Mild to severe stenosis of two branches from the LAD, LCx, RCA |
| ≥75% | Severe | Diffused (3-branch) | At the time of evaluation, a stenosis level was present in all three major branches. |
| Variables | Total | Category | Number (Percentage) |
|---|---|---|---|
| Gender | 83 | Male | 59 (71.1) |
| Female | 24 (28.9) | ||
| Age | 83 | <55 years old | 32 (38.5) |
| 55–64 years old | 17 (20.5) | ||
| 65–74 years old | 22 (26.5) | ||
| ≥75 years old | 12 (14.5) | ||
| Psoriasis Type | 83 | Psoriasis vulgaris | 44 (53.0) |
| Psoriatic arthritis | 32 (38.6) | ||
| Pustular psoriasis | 6 (7.2) | ||
| Psoriasis erythroderma | 1 (1.2) | ||
| BMI Classification | 83 | Underweight | 2 (2.4) |
| Normal | 29 (34.9) | ||
| Overweight | 14 (16.9) | ||
| Obesity class 1 | 29 (34.9) | ||
| Obesity class 2 | 9 (10.9) | ||
| Comorbidity | 83 | Negative | 62 (74.7) |
| Coronary artery disease | 6 (7.2) | ||
| Stroke | 4 (4.8) | ||
| Arrhythmia | 4 (4.8) | ||
| Other | 7 (8.5) | ||
| CHD | 83 | Positive | 6 (7.2) |
| CVD | 83 | Positive | 14 (16.9) |
| Smoking | 83 | Positive | 31 (37.3) |
| Alcohol | 83 | Positive | 36 (43.4) |
| Coronary Family History | 83 | Positive | 12 (14.5) |
| Psoriasis Family History | 83 | Positive | 2 (2.4) |
| Metabolic Syndrome | 79 | Negative | 28 (35.4) |
| Undefined | 30 (38.0) | ||
| Positive | 21 (26.6) | ||
| Hyperlipidemia | 83 | Positive | 44 (53.0) |
| Hypertension | 83 | Positive | 47 (56.6) |
| Diabetes | 83 | Positive | 14 (16.9) |
| CACS Classification | 83 | 0 | 49 (59.0) |
| 1–10 | 4 (4.8) | ||
| 11–100 | 12 (14.5) | ||
| 101–400 | 11 (13.3) | ||
| ≥400 | 7 (8.4) | ||
| Coronary Morphology | 83 | Normal | 44 (53.0) |
| Noncalcified plaque | 6 (7.2) | ||
| Calcified plaque | 25 (30.1) | ||
| Mixed plaque | 4 (4.9) | ||
| Calcified plaque + coronary abnormality | 2 (2.4) | ||
| Coronary abnormalities only | 2 (2.4) | ||
| Plaque | 83 | Positive | 34 (41.0) |
| Noncalcified Plaque | 83 | Positive | 10 (12.0) |
| Calcified Plaque | 83 | Positive | 31 (37.3) |
| Stenosis | 83 | Positive | 31 (37.3) |
| Suffering Vessel Distribution | 83 | None | 49 (59.0) |
| 1 branch | 13 (15.7) | ||
| 2 branches | 13 (15.7) | ||
| 3 branches (diffused) | 8 (9.6) | ||
| Stenosis Severity | 83 | None | 52 (62.7) |
| Mild | 8 (9.6) | ||
| Moderate | 17 (20.5) | ||
| Severe | 6 (7.2) |
| Variables | Number | Mean | Standard Deviation | 95% Confidence Interval | Range | ||
| Lower | Upper | Minimum | Maximum | ||||
| Age | 83 | 59 | 13.5 | 56 | 62 | 32 | 83 |
| PASI before treatment | 83 | 12.57 | 9.83 | 10.43 | 14.72 | 1.20 | 53.40 |
| PASI before CT | 70 | 10.57 | 9.99 | 8.19 | 12.95 | 0.00 | 53.40 |
| Duration | 79 | 13 | 10.42 | 10.59 | 15.26 | 0.3 | 41.0 |
| Age of onset | 80 | 46 | 16.97 | 42.3 | 49.85 | 14 | 78 |
| BMI | 83 | 25.0 | 4.21 | 24.08 | 25.92 | 17.58 | 43.28 |
| Total cholesterol | 82 | 188.67 | 64.02 | 174.60 | 202.74 | 0 | 300 |
| Triglycerides | 82 | 158.30 | 101.53 | 136.00 | 180.61 | 0 | 596 |
| HDL cholesterol | 73 | 53.48 | 13.96 | 50.22 | 56.74 | 27 | 98 |
| LDL cholesterol | 77 | 119.26 | 33.27 | 111.71 | 126.81 | 56 | 203 |
| Systolic blood pressure | 83 | 135 | 18.0 | 131.12 | 138.98 | 103 | 179 |
| Diastolic blood pressure | 83 | 82 | 14.5 | 78.98 | 85.31 | 42 | 119 |
| Variables | Number | Median | 25–75 Percentile | Range | |||
| Lower | Upper | Minimum | Maximum | ||||
| CACS | 83 | 0.00 | 0.00 | 66.02 | 0.00 | 2178.14 | |
| AACS | 64 | 250.86 | 0.00 | 1423.21 | 0.00 | 7580.57 | |
| Plaque number | 83 | 0 | 0 | 2 | 0 | 7 | |
| Stenosis number | 83 | 0 | 0 | 1 | 0 | 4 | |
| Glucose | 77 | 98.50 | 89.00 | 109.00 | 73.00 | 351.00 | |
| HbA1c | 77 | 5.80 | 5.40 | 6.20 | 4.50 | 14.20 | |
| his-CRP | 83 | 0.090 | 0.043 | 0.2778 | 0.014 | 7.216 | |
| Variables | Category | CACS | AACS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean | Median | p-Value | N | Mean | Median | p-Value | ||
| Age | <55 yo | 32 | 5.08 | 0.00 | <0.0001 | 25 | 156.84 | 0.00 | <0.0001 |
| 55–64 yo | 17 | 148.90 | 24.03 | 16 | 1012.42 | 444.48 | |||
| 65–74 yo | 22 | 86.29 | 0.00 | 15 | 1248.75 | 1023.71 | |||
| ≥75 yo | 12 | 530.37 | 289.67 | 8 | 4803.17 | 4995.32 | |||
| Psoriasis Type | Psoriasis vulgaris | 44 | 39.79 | 0.00 | 0.015 | 32 | 982.24 | 163.61 | >0.05 |
| Psoriatic arthritis | 32 | 249.89 | 32.39 | 27 | 1554.72 | 390.96 | |||
| Pustular psoriasis | 6 | 201.56 | 53.86 | 4 | 963.43 | 1229.98 | |||
| Psoriasis erythroderma | 1 | 0.00 | 0.00 | 1 | 13.54 | 13.54 | |||
| CACS Classification | 0 | 49 | 0.00 | 0.00 | <0.0001 | 37 | 602.98 | 0.00 | <0.0001 |
| 1–10 | 4 | 5.63 | 5.38 | 3 | 143.59 | 37.33 | |||
| 11–100 | 12 | 45.73 | 39.41 | 10 | 2130.53 | 1194.05 | |||
| 101–400 | 11 | 269.58 | 293.17 | 9 | 1500.26 | 1258.29 | |||
| ≥400 | 7 | 1059.99 | 838.83 | 5 | 3945.53 | 3903.99 | |||
| BMI Classification | Underweight | 2 | 195.89 | 195.89 | >0.05 | 1 | 0.00 | 0.00 | 0.003 |
| Normal | 29 | 132.48 | 0.00 | 23 | 1079.40 | 37.33 | |||
| Overweight | 14 | 294.08 | 21.98 | 11 | 3377.40 | 2150.57 | |||
| Obesity1 | 29 | 88.56 | 0.00 | 23 | 644.78 | 217.53 | |||
| Obesity2 | 9 | 4.17 | 0.00 | 6 | 78.15 | 0.00 | |||
| Coronary Plaque | Negative | 49 | 12.93 | 0.00 | <0.0001 | 36 | 766.31 | 6.23 | <0.0001 |
| Positive | 34 | 303.62 | 87.23 | 28 | 1774.61 | 1194.05 | |||
| Coronary Morphology | Noncalcified plaque | 6 | 0.00 | 0.00 | 0.001 | 6 | 1367.47 | 265.31 | >0.05 |
| Mixed plaque | 4 | 207.79 | 175.50 | 3 | 2333.15 | 1961.13 | |||
| Calcified plaque | 27 | 371.78 | 142.22 | 22 | 1911.51 | 1235.30 | |||
| Calcified Plaque | Negative | 52 | 1.68 | 0.00 | <0.0001 | 39 | 723.68 | 6.91 | <0.0001 |
| Positive | 31 | 350.62 | 173.08 | 25 | 1962.11 | 1258.29 | |||
| Stenosis | Negative | 52 | 13.96 | 0.00 | <0.0001 | 39 | lesions | 12.46 | 0.001 |
| Positive | 31 | 330.03 | 122.16 | 25 | 1825.24 | 1175.81 | |||
| Stenosis Severity | Mild | 8 | 84.31 | 4.03 | 0.021 | 8 | 695.35 | 444.48 | >0.05 |
| Moderate | 17 | 364.01 | 86.06 | 12 | 2474.04 | 1586.72 | |||
| Severe | 6 | 561.36 | 350.64 | 5 | 2075.93 | 2150.57 | |||
| Suffering Vessel Distribution | 1 branch | 13 | 64.36 | 24.03 | 0.009 | 12 | 968.18 | 403.52 | >0.05 |
| 2 branches | 13 | 351.68 | 262.80 | 10 | 2452.79 | 1983.31 | |||
| 3 branches (diffused) | 8 | 614.31 | 318.07 | 6 | 2257.18 | 2228.02 | |||
| Comorbidity | Negative | 62 | 77.77 | 0.00 | 0.013 | 49 | 951.21 | 120.88 | >0.05 |
| CHD | 6 | 113.62 | 30.32 | 4 | 744.47 | 815.57 | |||
| Stroke | 4 | 265.10 | 110.79 | 3 | 1303.81 | 30.49 | |||
| Arrhythmia | 4 | 796.26 | 690.51 | 3 | 2148.51 | 2150.57 | |||
| Other | 7 | 172.52 | 86.06 | 5 | 3466.48 | 3280.24 | |||
| Comorbidity | Negative | 62 | 77.77 | 0.00 | <0.0001 | 49 | 951.21 | 120.88 | 0.028 |
| Positive | 21 | 292.13 | 43.67 | 15 | 2044.49 | 1175.81 | |||
| CVD | Negative | 69 | 87.38 | 0.00 | 0.008 | 54 | 1184.10 | 202.55 | >0.05 |
| Positive | 14 | 351.94 | 42.49 | 10 | 1333.49 | 815.57 | |||
| Hypertension | Negative | 36 | 51.77 | 0.00 | 0.049 | 28 | 646.90 | 13.00 | 0.004 |
| Positive | 47 | 193.46 | 0.00 | 36 | 1643.42 | 890.83 | |||
| Diabetes | Negative | 69 | 137.14 | 0.00 | >0.05 | 51 | 1077.69 | 114.53 | 0.032 |
| Positive | 14 | 106.71 | 19.61 | 13 | 1716.50 | 1212.30 | |||
| Coronary Family History | Negative | 71 | 151.78 | 0.00 | 0.050 | 53 | 1348.92 | 390.96 | >0.05 |
| Positive | 12 | 15.00 | 0.00 | 11 | 525.79 | 0.00 | |||
| Biologic Treatment | Without | 62 | 169.01 | 0.00 | 0.013 | 51 | 1243.78 | 284.18 | <0.0001 |
| With | 16 | 6.05 | 0.00 | 9 | 241.08 | 5.80 | |||
| Anti-IL12/23 Treatment | Without | 72 | 146.88 | 0.00 | 0.049 | 57 | 1147.11 | 206.33 | >0.05 |
| With | 6 | 0.00 | 0.00 | 3 | 72.51 | 0.00 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huynh, T.N.-M.; Yamazaki, F.; Kishimoto, I.; Tanaka, A.; Son, Y.; Ozaki, Y.; Takehana, K.; Tanizaki, H. The Correlation between the Vascular Calcification Score of the Coronary Artery and the Abdominal Aorta in Patients with Psoriasis. Diagnostics 2023, 13, 274. https://doi.org/10.3390/diagnostics13020274
Huynh TN-M, Yamazaki F, Kishimoto I, Tanaka A, Son Y, Ozaki Y, Takehana K, Tanizaki H. The Correlation between the Vascular Calcification Score of the Coronary Artery and the Abdominal Aorta in Patients with Psoriasis. Diagnostics. 2023; 13(2):274. https://doi.org/10.3390/diagnostics13020274
Chicago/Turabian StyleHuynh, Trang Nguyen-Mai, Fumikazu Yamazaki, Izumi Kishimoto, Akihiro Tanaka, Yonsu Son, Yoshio Ozaki, Kazuya Takehana, and Hideaki Tanizaki. 2023. "The Correlation between the Vascular Calcification Score of the Coronary Artery and the Abdominal Aorta in Patients with Psoriasis" Diagnostics 13, no. 2: 274. https://doi.org/10.3390/diagnostics13020274