
Coronary Flow Velocity Reserve by Echocardiography: Beyond Atherosclerotic Disease
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
Abstract
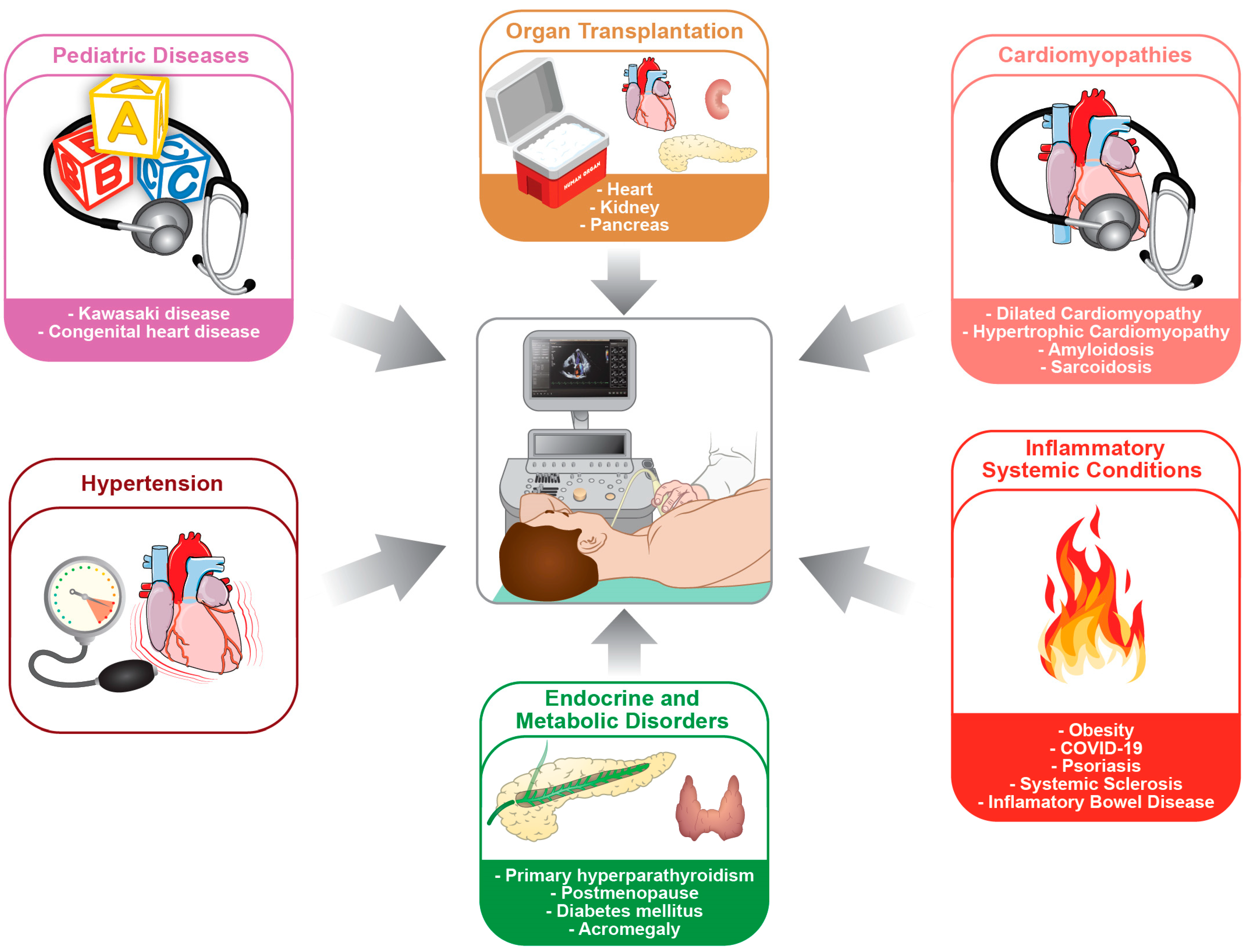
:1. Introduction
2. Organ Transplant
2.1. Heart Transplantation
2.2. Non-Heart Transplantation
3. Cardiomyopathies
3.1. Dilated Cardiomyopathy
3.2. Hypertrophic Cardiomyopathy
3.3. Acquired Cardiomyopathies
4. Inflammatory Systemic Conditions
4.1. Obesity
4.2. COVID-19
4.3. Chronic Inflammatory Disease
4.4. Psoriasis
4.5. Systemic Sclerosis
4.6. Other Inflammatory Conditions
5. Endocrine and Metabolic Disorders
Diabetes Mellitus
6. Hypertension
7. Aortic Stenosis
8. Pediatric Patients
9. Conclusions and Future Perspectives
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gould, K.L.; Lipscomb, K. Effects of coronary stenoses on coronary flow reserve and resistance. Am. J. Cardiol. 1974, 34, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Gould, K.L.; Lipscomb, K.; Hamilton, G.W. Physiologic basis for assessing critical coronary stenosis. Instantaneous flow response and regional distribution during coronary hyperemia as measures of coronary flow reserve. Am. J. Cardiol. 1974, 33, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Iliceto, S.; Marangelli, V.; Memmola, C.; Rizzon, P. Transesophageal Doppler echocardiography evaluation of coronary blood flow velocity in baseline conditions and during dipyridamole-induced coronary vasodilation. Circulation 1991, 83, 61–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caiati, C.; Montaldo, C.; Zedda, N.; Bina, A.; Iliceto, S. New Noninvasive Method for Coronary Flow Reserve Assessment: Contrast-Enhanced Transthoracic Second Harmonic Echo Doppler. Circulation 1999, 99, 771–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simova, I. Coronary Flow Velocity Reserve Assessment with Transthoracic Doppler Echocardiography. Eur. Cardiol. 2015, 10, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Hozumi, T.; Yoshida, K.; Ogata, Y.; Akasaka, T.; Asami, Y.; Takagi, T.; Morioka, S. Noninvasive assessment of significant left anterior descending coronary artery stenosis by coronary flow velocity reserve with transthoracic color Doppler echocardiography. Circulation 1998, 97, 1557–1562. [Google Scholar] [CrossRef] [Green Version]
- Caiati, C.; Montaldo, C.; Zedda, N.; Montisci, R.; Ruscazio, M.; Lai, G.; Cadeddu, M.; Meloni, L.; Iliceto, S. Validation of a new noninvasive method (contrast-enhanced transthoracic second harmonic echo Doppler) for the evaluation of coronary flow reserve: Comparison with intracoronary Doppler flow wire. J. Am. Coll. Cardiol. 1999, 34, 1193–1200. [Google Scholar] [CrossRef]
- Brainin, P.; Frestad, D.; Prescott, E. The prognostic value of coronary endothelial and microvascular dysfunction in subjects with normal or non-obstructive coronary artery disease: A systematic review and meta-analysis. Int. J. Cardiol. 2018, 254, 1–9. [Google Scholar] [CrossRef]
- Caforio, A.L.P.; Tona, F.; Fortina, A.B.; Angelini, A.; Piaserico, S.; Gambino, A.; Feltrin, G.; Ramondo, A.; Valente, M.; Iliceto, S.; et al. Immune and nonimmune predictors of cardiac allograft vasculopathy onset and severity: Multivariate risk factor analysis and role of immunosuppression. Am. J. Transplant. 2004, 4, 962–970. [Google Scholar] [CrossRef]
- Taylor, D.O.; Edwards, L.B.; Mohacsi, P.J.; Boucek, M.M.; Trulock, E.P.; Keck, B.M.; Hertz, M.I. The registry of the International Society for Heart and Lung Transplantation: Twentieth official adult heart transplant report--2003. J. Heart Lung Transplant. 2003, 22, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Fearon, W.F.; Kobayashi, Y. Invasive Assessment of the Coronary Microvasculature: The Index of Microcirculatory Resistance. Circ. Cardiovasc. Interv. 2017, 10, e005361. [Google Scholar] [CrossRef] [PubMed]
- Rickenbacher, P.R.; Pinto, F.J.; Lewis, N.P.; Hunt, S.A.; Alderman, E.L.; Schroeder, J.S.; Stinson, E.B.; Brown, B.W.; Valantine, H.A. Prognostic importance of intimal thickness as measured by intracoronary ultrasound after cardiac transplantation. Circulation 1995, 92, 3445–3452. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.A.; Tobis, J.M.; Starling, R.C.; Tuzcu, E.M.; Smith, A.L.; Valantine, H.A.; Yeung, A.C.; Mehra, M.R.; Anzai, H.; Oeser, B.T.; et al. Multicenter Intravascular Ultrasound Validation Study Among Heart Transplant Recipients. J. Am. Coll. Cardiol. 2005, 45, 1532–1537. [Google Scholar] [CrossRef] [Green Version]
- Tona, F.; Caforio, A.L.P.; Montisci, R.; Angelini, A.; Ruscazio, M.; Gambino, A.; Ramondo, A.; Thiene, G.; Gerosa, G.; Iliceto, S. Coronary Flow Reserve by Contrast-Enhanced Echocardiography: A New Noninvasive Diagnostic Tool for Cardiac Allograft Vasculopathy: Coronary Flow Reserve in Heart Transplantation. Am. J. Transplant. 2006, 6, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Pichel, I.Á.; Fernández Cimadevilla, O.C.; de la Hera Galarza, J.M.; Pasanisi, E.; Ruiz, J.M.G.; Molina, B.D.; Rodriguez, J.L.L.; Sicari, R.; Fernández, M.M. Usefulness of dual imaging stress echocardiography for the diagnosis of coronary allograft vasculopathy in heart transplant recipients. Int. J. Cardiol. 2019, 296, 109–112. [Google Scholar] [CrossRef]
- Bjerre, K.P.; Clemmensen, T.S.; Poulsen, S.H.; Hvas, A.-M.; Løgstrup, B.B.; Grove, E.L.; Flyvholm, F.; Kristensen, S.D.; Eiskjær, H. Coronary Flow Velocity Reserve and Myocardial Deformation Predict Long-Term Outcomes in Heart Transplant Recipients. J. Am. Soc. Echocardiogr. 2021, 34, 1294–1302. [Google Scholar] [CrossRef]
- Osto, E.; Tona, F.; Angelini, A.; Montisci, R.; Ruscazio, M.; Vinci, A.; Tarantini, G.; Ramondo, A.; Gambino, A.; Thiene, G.; et al. Determinants of Coronary Flow Reserve in Heart Transplantation: A Study Performed With Contrast-enhanced Echocardiography. J. Heart Lung Transplant. 2009, 28, 453–460. [Google Scholar] [CrossRef]
- Tona, F.; Fedrigo, M.; Famoso, G.; Previato, M.; Tellatin, S.; Vecchiati, A.; Bellu, R.; Marra, M.P.; Feltrin, G.; Gerosa, G.; et al. Everolimus Prevents Coronary Microvasculopathy in Heart Transplant Recipients With Normal Coronary Angiograms: An Anatomo-Functional Study. Transplant. Proc. 2014, 46, 2339–2344. [Google Scholar] [CrossRef]
- Tona, F.; Caforio, A.L.P.; Montisci, R.; Gambino, A.; Angelini, A.; Ruscazio, M.; Toscano, G.; Feltrin, G.; Ramondo, A.; Gerosa, G.; et al. Coronary flow velocity pattern and coronary flow reserve by contrast-enhanced transthoracic echocardiography predict long-term outcome in heart transplantation. Circulation 2006, 114, I49–I55. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, A.C.T.; de Frimm, C.C.; Bacal, F.; Andreolli, V.; Tsutsui, J.M.; Bocchi, E.A.; Mathias, W.; Lage, S.G. Coronary flow reserve impairment predicts cardiac events in heart transplant patients with preserved left ventricular function. Int. J. Cardiol. 2005, 103, 201–206. [Google Scholar] [CrossRef]
- Tona, F.; Osto, E.; Famoso, G.; Previato, M.; Fedrigo, M.; Vecchiati, A.; Perazzolo Marra, M.; Tellatin, S.; Bellu, R.; Tarantini, G.; et al. Coronary Microvascular Dysfunction Correlates With the New Onset of Cardiac Allograft Vasculopathy in Heart Transplant Patients With Normal Coronary Angiography: Microvascular Dysfunction Correlates With CAV. Am. J. Transplant. 2015, 15, 1400–1406. [Google Scholar] [CrossRef] [PubMed]
- Kerkhof, P.L.M.; Osto, E.; Tona, F.; Heyndrickx, G.R.; Handly, N. Sex-Specific Interpretation of Coronary Flow Reserve and Fractional Flow Reserve Metrics, Including Their Companions. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 7006–7009. [Google Scholar] [CrossRef]
- Kerkhof, P.L.M.; Peace, R.A.; Handly, N. Ratiology and a Complementary Class of Metrics for Cardiovascular Investigations. Physiology 2019, 34, 250–263. [Google Scholar] [CrossRef] [PubMed]
- Cecere, A.; Kerkhof, P.L.M.; Civieri, G.; Angelini, A.; Gambino, A.; Fraiese, A.; Bottio, T.; Osto, E.; Famoso, G.; Fedrigo, M.; et al. Coronary Flow Evaluation in Heart Transplant Patients Compared to Healthy Controls Documents the Superiority of Coronary Flow Velocity Reserve Companion as Diagnostic and Prognostic Tool. Front. Cardiovasc. Med. 2022, 9, 887370. [Google Scholar] [CrossRef] [PubMed]
- Bond, M.G.; Wilmoth, S.K.; Enevold, G.L.; Strickland, H.L. Detection and monitoring of asymptomatic atherosclerosis in clinical trials. Am. J. Med. 1989, 86, 33–36. [Google Scholar] [CrossRef]
- Jain, V.; Gupta, K.; Bhatia, K.; Rajapreyar, I.; Singh, A.; Zhou, W.; Klein, A.; Nanda, N.C.; Prabhu, S.D.; Bajaj, N.S. Coronary flow abnormalities in chronic kidney disease: A systematic review and meta-analysis. Echocardiography 2022, 39, 1382–1390. [Google Scholar] [CrossRef]
- Tok, D.; Gullu, H.; Erdogan, D.; Topcu, S.; Ciftci, O.; Yildirim, I.; Muderrisoglu, H. Impaired Coronary Flow Reserve in Hemodialysis Patients: A Transthoracic Doppler Echocardiographic Study. Nephron Clin. Pract. 2005, 101, c200–c206. [Google Scholar] [CrossRef]
- Turiel, M.; Sitia, S.; Tomasoni, L.; Cicala, S.; Viganò, S.M.; Menegotto, A.; Martina, V.; Bodini, B.D.; Bacchiani, G.; Ghio, L.; et al. Subclinical impairment of coronary flow velocity reserve assessed by transthoracic echocardiography in young renal transplant recipients. Atherosclerosis 2009, 204, 435–439. [Google Scholar] [CrossRef]
- Akagun, T.; Caliskan, Y.; Alpay, N.; Ozkok, A.; Yazici, H.; Polat, N.; Guz, G.; Oflaz, H.; Turkmen, A.; Sukru Sever, M. Long-Term Prognostic Value of Coronary Flow Velocity Reserve in Renal Transplant Recipients. Transplant. Proc. 2011, 43, 2612–2616. [Google Scholar] [CrossRef]
- Tona, F.; Silvestre, C.; Rigato, M.; Famoso, G.; Marchini, F.; Bonfante, L.; Neri, F.; Furian, L.; Crepaldi, C.; Iliceto, S.; et al. Coronary Microvascular Dysfunction Predicts Long-Term Outcome in Simultaneous Pancreas–Kidney Transplantation. Transplant. Proc. 2016, 48, 344–348. [Google Scholar] [CrossRef]
- Chen, J.W.; Ting, C.T.; Chen, Y.H.; Wu, T.C.; Hsu, N.W.; Lin, S.J.; Chang, M.S. Differential coronary microvascular function in patients with left ventricular dysfunction of unknown cause--implication for possible mechanism of myocardial ischemia in early stage of cardiomyopathy. Int. J. Cardiol. 1999, 69, 251–261. [Google Scholar] [CrossRef]
- Neglia, D.; Parodi, O.; Gallopin, M.; Sambuceti, G.; Giorgetti, A.; Pratali, L.; Salvadori, P.; Michelassi, C.; Lunardi, M.; Pelosi, G. Myocardial blood flow response to pacing tachycardia and to dipyridamole infusion in patients with dilated cardiomyopathy without overt heart failure. A quantitative assessment by positron emission tomography. Circulation 1995, 92, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Djordjevic Dikic, A.; Nikcevic, G.; Raspopovic, S.; Jovanovic, V.; Tesic, M.; Beleslin, B.; Stepanovic, J.; Giga, V.; Milasinovic, G. Prognostic role of coronary flow reserve for left ventricular functional improvement after cardiac resynchronization therapy in patients with dilated cardiomyopathy. Eur. Heart J.-Cardiovasc. Imaging 2014, 15, 1344–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santagata, P.; Rigo, F.; Gherardi, S.; Pratali, L.; Drozdz, J.; Varga, A.; Picano, E. Clinical and functional determinants of coronary flow reserve in non-ischemic dilated cardiomyopathy. Int. J. Cardiol. 2005, 105, 46–52. [Google Scholar] [CrossRef]
- Vanderheyden, M.; Bartunek, J.; Verstreken, S.; Mortier, L.; Goethals, M.; de Bruyne, B. Non-invasive assessment of coronary flow reserve in idiopathic dilated cardiomyopathy: Hemodynamic correlations. Eur. J. Echocardiogr. 2005, 6, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Rigo, F.; Gherardi, S.; Galderisi, M.; Pratali, L.; Cortigiani, L.; Sicari, R.; Picano, E. The prognostic impact of coronary flow-reserve assessed by Doppler echocardiography in non-ischaemic dilated cardiomyopathy. Eur. Heart J. 2006, 27, 1319–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opherk, D.; Schwarz, F.; Mall, G.; Manthey, J.; Baller, D.; Kübler, W. Coronary dilatory capacity in idiopathic dilated cardiomyopathy: Analysis of 16 patients. Am. J. Cardiol. 1983, 51, 1657–1662. [Google Scholar] [CrossRef] [PubMed]
- Tsagalou, E.P.; Anastasiou-Nana, M.; Agapitos, E.; Gika, A.; Drakos, S.G.; Terrovitis, J.V.; Ntalianis, A.; Nanas, J.N. Depressed Coronary Flow Reserve Is Associated with Decreased Myocardial Capillary Density in Patients with Heart Failure Due to Idiopathic Dilated Cardiomyopathy. J. Am. Coll. Cardiol. 2008, 52, 1391–1398. [Google Scholar] [CrossRef] [Green Version]
- Tona, F. Dilated cardiomyopathy and coronary flow reserve. Eur. Heart J. 2006, 27, 1884. [Google Scholar] [CrossRef] [Green Version]
- Cecchi, F.; Olivotto, I.; Gistri, R.; Lorenzoni, R.; Chiriatti, G.; Camici, P.G. Coronary Microvascular Dysfunction and Prognosis in Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2003, 349, 1027–1035. [Google Scholar] [CrossRef]
- McKenna, W.J. Hypertrophic cardiomyopathy: Management, risk stratification, and prevention of sudden death. Heart 2002, 87, 169–176. [Google Scholar] [CrossRef] [Green Version]
- Cortigiani, L.; Rigo, F.; Gherardi, S.; Galderisi, M.; Sicari, R.; Picano, E. Prognostic Implications of Coronary Flow Reserve on Left Anterior Descending Coronary Artery in Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2008, 102, 1718–1723. [Google Scholar] [CrossRef] [PubMed]
- Aguiar Rosa, S.; Lopes, L.R.; Branco, L.; Galrinho, A.; Fiarresga, A.; Thomas, B.; Brás, P.; Gonçalves, A.; Cardoso, I.; Papoila, A.; et al. Blunted coronary flow velocity reserve is associated with impairment in systolic function and functional capacity in hypertrophic cardiomyopathy. Int. J. Cardiol. 2022, 359, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Tesic, M.; Seferovic, J.; Trifunovic, D.; Djordjevic-Dikic, A.; Giga, V.; Jovanovic, I.; Petrovic, O.; Marinkovic, J.; Stankovic, S.; Stepanovic, J.; et al. N-terminal pro-brain natriuretic peptide is related with coronary flow velocity reserve and diastolic dysfunction in patients with asymmetric hypertrophic cardiomyopathy. J. Cardiol. 2017, 70, 323–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tesic, M.; Beleslin, B.; Giga, V.; Jovanovic, I.; Marinkovic, J.; Trifunovic, D.; Petrovic, O.; Dobric, M.; Aleksandric, S.; Juricic, S.; et al. Prognostic Value of Transthoracic Doppler Echocardiography Coronary Flow Velocity Reserve in Patients with Asymmetric Hypertrophic Cardiomyopathy. J. Am. Heart Assoc. 2021, 10, e021936. [Google Scholar] [CrossRef] [PubMed]
- Tesic, M.; Djordjevic-Dikic, A.; Beleslin, B.; Trifunovic, D.; Giga, V.; Marinkovic, J.; Petrovic, O.; Petrovic, M.; Stepanovic, J.; Dobric, M.; et al. Regional Difference of Microcirculation in Patients with Asymmetric Hypertrophic Cardiomyopathy: Transthoracic Doppler Coronary Flow Velocity Reserve Analysis. J. Am. Soc. Echocardiogr. 2013, 26, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Dorbala, S.; Vangala, D.; Bruyere, J.; Quarta, C.; Kruger, J.; Padera, R.; Foster, C.; Hanley, M.; Di Carli, M.F.; Falk, R. Coronary microvascular dysfunction is related to abnormalities in myocardial structure and function in cardiac amyloidosis. JACC Heart Fail. 2014, 2, 358–367. [Google Scholar] [CrossRef]
- Kruse, M.J.; Kovell, L.; Kasper, E.K.; Pomper, M.G.; Moller, D.R.; Solnes, L.; Chen, E.S.; Schindler, T.H. Myocardial Blood Flow and Inflammatory Cardiac Sarcoidosis. JACC Cardiovasc. Imaging 2017, 10, 157–167. [Google Scholar] [CrossRef]
- Clemmensen, T.S.; Eiskjær, H.; Mølgaard, H.; Larsen, A.H.; Soerensen, J.; Andersen, N.F.; Tolbod, L.P.; Harms, H.J.; Poulsen, S.H. Abnormal Coronary Flow Velocity Reserve and Decreased Myocardial Contractile Reserve Are Main Factors in Relation to Physical Exercise Capacity in Cardiac Amyloidosis. J. Am. Soc. Echocardiogr. 2018, 31, 71–78. [Google Scholar] [CrossRef]
- Sagris, M.; Theofilis, P.; Antonopoulos, A.S.; Oikonomou, E.; Paschaliori, C.; Galiatsatos, N.; Tsioufis, K.; Tousoulis, D. Inflammation in Coronary Microvascular Dysfunction. Int. J. Mol. Sci. 2021, 22, 13471. [Google Scholar] [CrossRef]
- Hubert, H.B.; Feinleib, M.; McNamara, P.M.; Castelli, W.P. Obesity as an independent risk factor for cardiovascular disease: A 26-year follow-up of participants in the Framingham Heart Study. Circulation 1983, 67, 968–977. [Google Scholar] [CrossRef] [Green Version]
- Vaccarino, V.; Khan, D.; Votaw, J.; Faber, T.; Veledar, E.; Jones, D.P.; Goldberg, J.; Raggi, P.; Quyyumi, A.A.; Bremner, J.D. Inflammation is related to coronary flow reserve detected by positron emission tomography in asymptomatic male twins. J. Am. Coll. Cardiol. 2011, 57, 1271–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tedgui, A.; Mallat, Z. Cytokines in atherosclerosis: Pathogenic and regulatory pathways. Physiol. Rev. 2006, 86, 515–581. [Google Scholar] [CrossRef] [Green Version]
- Tona, F.; Serra, R.; Di Ascenzo, L.; Osto, E.; Scarda, A.; Fabris, R.; Montisci, R.; Famoso, G.; Tellatin, S.; Foletto, M.; et al. Systemic inflammation is related to coronary microvascular dysfunction in obese patients without obstructive coronary disease. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Hozumi, T.; Eisenberg, M.; Sugioka, K.; Kokkirala, A.R.; Watanabe, H.; Teragaki, M.; Yoshikawa, J.; Homma, S. Change in coronary flow reserve on transthoracic Doppler echocardiography after a single high-fat meal in young healthy men. Ann. Intern. Med. 2002, 136, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Herieka, M.; Erridge, C. High-fat meal induced postprandial inflammation. Mol. Nutr. Food Res. 2014, 58, 136–146. [Google Scholar] [CrossRef]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Lowenstein, C.J.; Solomon, S.D. Severe COVID-19 Is a Microvascular Disease. Circulation 2020, 142, 1609–1611. [Google Scholar] [CrossRef]
- Çalışkan, M.; Baycan, Ö.F.; Çelik, F.B.; Güvenç, T.S.; Atıcı, A.; Çağ, Y.; Konal, O.; İrgi, T.; Bilgili, Ü.Z.; Ağırbaşlı, M.A. Coronary microvascular dysfunction is common in patients hospitalized with COVID -19 infection. Microcirculation 2022, 29, e12757. [Google Scholar] [CrossRef]
- Sandoval, Y.; Januzzi, J.L.; Jaffe, A.S. Cardiac Troponin for Assessment of Myocardial Injury in COVID-19. J. Am. Coll. Cardiol. 2020, 76, 1244–1258. [Google Scholar] [CrossRef]
- Rovas, A.; Osiaevi, I.; Buscher, K.; Sackarnd, J.; Tepasse, P.-R.; Fobker, M.; Kühn, J.; Braune, S.; Göbel, U.; Thölking, G.; et al. Microvascular dysfunction in COVID-19: The MYSTIC study. Angiogenesis 2021, 24, 145–157. [Google Scholar] [CrossRef]
- Landecho, M.F.; Yuste, J.R.; Gándara, E.; Sunsundegui, P.; Quiroga, J.; Alcaide, A.B.; García-Layana, A. COVID-19 retinal microangiopathy as an in vivo biomarker of systemic vascular disease? J. Intern. Med. 2021, 289, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Wang, S.; Liu, Y.; Chen, J.; Li, D.; Xu, T. Coronary microvascular dysfunction pathophysiology in COVID-19. Microcirculation 2021, 28, e12718. [Google Scholar] [CrossRef] [PubMed]
- Kakuta, K.; Dohi, K.; Sato, Y.; Yamanaka, T.; Kawamura, M.; Ogura, T.; Nakamori, S.; Fujimoto, N.; Fujii, E.; Yamada, N.; et al. Chronic Inflammatory Disease Is an Independent Risk Factor for Coronary Flow Velocity Reserve Impairment Unrelated to the Processes of Coronary Artery Calcium Deposition. J. Am. Soc. Echocardiogr. 2016, 29, 173–180. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. The Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef] [PubMed]
- Bulut, M.; Keles, N.; Caliskan, Z.; Kostek, O.; Aksu, F.; Ozdil, K.; Akcakoyun, M.; Demircioglu, K.; Yilmaz, Y.; Kanbay, M.; et al. Is the presence of AA amyloidosis associated with impaired coronary flow reserve? Atherosclerosis 2016, 251, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Caliskan, Z.; Tatlisu, M.A.; Kahraman, R.; Gokturk, S.; Sayar, S.; Kostek, O.; Kul, S.; Baycan, O.F.; Ozcan, F.G.; Caliskan, M. The impact of prognostic nutritional index on coronary flow reserve in patients with inflammatory bowel disease. Medeni. Med. J. 2019, 34, 271. [Google Scholar] [CrossRef] [Green Version]
- Kakuta, K.; Dohi, K.; Yamamoto, T.; Fujimoto, N.; Shimoyama, T.; Umegae, S.; Ito, M. Coronary Microvascular Dysfunction Restored After Surgery in Inflammatory Bowel Disease: A Prospective Observational Study. J. Am. Heart Assoc. 2021, 10, e019125. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, V.E.; Cather, J.C.; Gelfand, J.M.; Gordon, K.B.; Gibbons, G.H.; Grundy, S.M.; Jarratt, M.T.; Krueger, J.G.; Ridker, P.M.; Stone, N.; et al. AJC editor’s consensus: Psoriasis and coronary artery disease. Am. J. Cardiol. 2008, 102, 1631–1643. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Neimann, A.L.; Shin, D.B.; Wang, X.; Margolis, D.J.; Troxel, A.B. Risk of myocardial infarction in patients with psoriasis. JAMA 2006, 296, 1735–1741. [Google Scholar] [CrossRef] [PubMed]
- Osto, E.; Piaserico, S.; Maddalozzo, A.; Forchetti, G.; Montisci, R.; Famoso, G.; Giovagnoni, A.; Peserico, A.; Iliceto, S.; Tona, F. Impaired coronary flow reserve in young patients affected by severe psoriasis. Atherosclerosis 2012, 221, 113–117. [Google Scholar] [CrossRef]
- Gullu, H.; Caliskan, M.; Dursun, R.; Ciftci, O.; Guven, A.; Muderrisoglu, H. Impaired Coronary Microvascular Function and Its Association with Disease Duration and Inflammation in Patients with Psoriasis. Echocardiography 2013, 30, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Tona, F.; Osto, E.; Kerkhof, P.L.M.; Montisci, R.; Famoso, G.; Lorenzoni, G.; De Michieli, L.; Cecere, A.; Zanetti, I.; Civieri, G.; et al. Multiparametric analysis of coronary flow in psoriasis using a coronary flow reserve companion. Eur. J. Clin. Investig. 2021, 52, e13711. [Google Scholar] [CrossRef] [PubMed]
- Piaserico, S.; Osto, E.; Famoso, G.; Montisci, R.; De Michieli, L.; Zanetti, I.; Iliceto, S.; Tona, F. Long-term prognostic value of coronary flow reserve in psoriasis patients. Atherosclerosis 2019, 289, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Piaserico, S.; Osto, E.; Famoso, G.; Zanetti, I.; Gregori, D.; Poretto, A.; Iliceto, S.; Peserico, A.; Tona, F. Treatment with tumor necrosis factor inhibitors restores coronary microvascular function in young patients with severe psoriasis. Atherosclerosis 2016, 251, 25–30. [Google Scholar] [CrossRef]
- Follansbee, W.P. The cardiovascular manifestations of systemic sclerosis (scleroderma). Curr. Probl. Cardiol. 1986, 11, 241–298. [Google Scholar] [CrossRef]
- Follansbee, W.P.; Miller, T.R.; Curtiss, E.I.; Orie, J.E.; Bernstein, R.L.; Kiernan, J.M.; Medsger, T.A. A controlled clinicopathologic study of myocardial fibrosis in systemic sclerosis (scleroderma). J. Rheumatol. 1990, 17, 656–662. [Google Scholar]
- Montisci, R.; Vacca, A.; Garau, P.; Colonna, P.; Ruscazio, M.; Passiu, G.; Iliceto, S.; Mathieu, A. Detection of early impairment of coronary flow reserve in patients with systemic sclerosis. Ann. Rheum. Dis. 2003, 62, 890–893. [Google Scholar] [CrossRef] [Green Version]
- Vacca, A. Absence of epicardial coronary stenosis in patients with systemic sclerosis with severe impairment of coronary flow reserve. Ann. Rheum. Dis. 2006, 65, 274–275. [Google Scholar] [CrossRef]
- Montisci, R.; Ruscazio, M.; Lai, S.; Vacca, A.; Cauli, A.; Passiu, G.; Montisci, M.; Meloni, L.; Mathieu, A.; Iliceto, S. Effect of a single IV administration of L-propionylcarnitine on myocardial microcirculation assessed by coronary flow velocity reserve measurement in patients with systemic sclerosis: A pilot study. Clin. Ther. 2007, 29, 163–171. [Google Scholar] [CrossRef]
- Zanatta, E.; Famoso, G.; Boscain, F.; Montisci, R.; Pigatto, E.; Polito, P.; Schiavon, F.; Iliceto, S.; Cozzi, F.; Doria, A.; et al. Nailfold avascular score and coronary microvascular dysfunction in systemic sclerosis: A newsworthy association. Autoimmun. Rev. 2019, 18, 177–183. [Google Scholar] [CrossRef]
- Sulli, A. Blunted coronary flow reserve in systemic sclerosis. Rheumatology 2004, 43, 505–509. [Google Scholar] [CrossRef] [Green Version]
- Faccini, A.; Agricola, E.; Oppizzi, M.; Margonato, A.; Galderisi, M.; Sabbadini, M.G.; Franchini, S.; Camici, P.G. Coronary Microvascular Dysfunction in Asymptomatic Patients Affected by Systemic Sclerosis –Limited vs. Diffuse Form–. Circ. J. 2015, 79, 825–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vacca, A.; Montisci, R.; Garau, P.; Siotto, P.; Piga, M.; Cauli, A.; Ruscazio, M.; Meloni, L.; Iliceto, S.; Mathieu, A. Prognostic impact of coronary microcirculation abnormalities in systemic sclerosis: A prospective study to evaluate the role of non-invasive tests. Arthritis Res. Ther. 2013, 15, R8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caliskan, M.; Turk, E.; Karagulle, E.; Ciftci, O.; Oguz, H.; Kostek, O.; Moray, G.; Haberal, M. Coronary Flow Velocity Reserve in Burn Injury: A Prospective Clinical Cohort Study. J. Burn Care Res. 2016, 37, e400–e408. [Google Scholar] [CrossRef]
- Kellermair, J.; Kiblboeck, D.; Blessberger, H.; Kammler, J.; Reiter, C.; Steinwender, C. Reversible impairment of coronary flow reserve in acute myocarditis. Microcirculation 2018, 25, e12491. [Google Scholar] [CrossRef] [PubMed]
- Oflaz, H.; Sen, F.; Bayrakli, S.K.; Elitok, A.; Cimen, A.O.; Golcuk, E.; Kasikcioglu, E.; Tukenmez, M.; Yazici, H.; Turkmen, A. Reduced Coronary Flow Reserve and Early Diastolic Filling Abnormalities in Patients with Nephrotic Syndrome. Ren. Fail. 2008, 30, 914–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverberg, S.J.; Shane, E.; Jacobs, T.P.; Siris, E.; Bilezikian, J.P. A 10-year prospective study of primary hyperparathyroidism with or without parathyroid surgery. N. Engl. J. Med. 1999, 341, 1249–1255. [Google Scholar] [CrossRef]
- Andersson, P.; Rydberg, E.; Willenheimer, R. Primary hyperparathyroidism and heart disease—A review. Eur. Heart J. 2004, 25, 1776–1787. [Google Scholar] [CrossRef]
- Rashid, G.; Bernheim, J.; Green, J.; Benchetrit, S. Parathyroid hormone stimulates the endothelial nitric oxide synthase through protein kinase A and C pathways. Nephrol. Dial. Transplant. 2007, 22, 2831–2837. [Google Scholar] [CrossRef] [Green Version]
- Nickols, G.A. Increased cyclic AMP in cultured vascular smooth muscle cells and relaxation of aortic strips by parathyroid hormone. Eur. J. Pharmacol. 1985, 116, 137–144. [Google Scholar] [CrossRef]
- Osto, E.; Fallo, F.; Pelizzo, M.R.; Maddalozzo, A.; Sorgato, N.; Corbetti, F.; Montisci, R.; Famoso, G.; Bellu, R.; Lüscher, T.F.; et al. Coronary microvascular dysfunction induced by primary hyperparathyroidism is restored after parathyroidectomy. Circulation 2012, 126, 1031–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nascimento, G.C.; de Oliveira, M.T.; Carvalho, V.C.; Lopes, M.H.C.; Sá, A.M.G.; Souza, M.T.; de Ferreira, A.S.P.; Ferreira, P.A.M.; dos Faria, M.S. Acromegalic cardiomyopathy in an extensively admixed population: Is there a role for GH/IGF-I axis? Clin. Endocrinol. 2013, 78, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Tellatin, S.; Maffei, P.; Osto, E.; Dassie, F.; Famoso, G.; Montisci, R.; Martini, C.; Fallo, F.; Marra, M.P.; Mioni, R.; et al. Coronary microvascular dysfunction may be related to IGF-1 in acromegalic patients and can be restored by therapy. Atherosclerosis 2018, 269, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Hirata, K.; Shimada, K.; Watanabe, H.; Muro, T.; Yoshiyama, M.; Takeuchi, K.; Hozumi, T.; Yoshikawa, J. Modulation of coronary flow velocity reserve by gender, menstrual cycle and hormone replacement therapy. J. Am. Coll. Cardiol. 2001, 38, 1879–1884. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, C.G.; Fisher, B.M.; Frier, B.M.; Dargie, H.J.; More, I.A.; Lindop, G.B. Endomyocardial biopsy pathology in insulin-dependent diabetic patients with abnormal ventricular function. Histopathology 1989, 14, 593–602. [Google Scholar] [CrossRef]
- Nahser, P.J.; Brown, R.E.; Oskarsson, H.; Winniford, M.D.; Rossen, J.D. Maximal coronary flow reserve and metabolic coronary vasodilation in patients with diabetes mellitus. Circulation 1995, 91, 635–640. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.E. Diabetic angiopathy--its lessons in vascular physiology. Am. Heart J. 1978, 96, 401–406. [Google Scholar] [CrossRef]
- Kranidis, A.; Zamanis, N.; Mitrakou, A.; Patsilinakos, S.; Bouki, T.; Tountas, N.; Anthopoulos, P.; Raptis, S.; Anthopoulos, L. Coronary microcirculation evaluation with transesophageal echocardiography Doppler in type II diabetics. Int. J. Cardiol. 1997, 59, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Atar, A.I.; Altuner, T.K.; Bozbas, H.; Korkmaz, M.E. Coronary Flow Reserve in Patients with Diabetes Mellitus and Prediabetes: Coronary Flow Reserve and Glucose Metabolism. Echocardiography 2012, 29, 634–640. [Google Scholar] [CrossRef]
- Caliskan, M.; Turan, Y.; Caliskan, Z.; Gullu, H.; Ciftci, F.C.; Avci, E.; Duran, C.; Kostek, O.; Telci Caklili, O.; Koca, H.; et al. Previous gestational diabetes history is associated with impaired coronary flow reserve. Ann. Med. 2015, 47, 615–623. [Google Scholar] [CrossRef]
- Kawata, T.; Daimon, M.; Hasegawa, R.; Teramoto, K.; Toyoda, T.; Sekine, T.; Yamamoto, K.; Uchida, D.; Himi, T.; Yoshida, K.; et al. Effect on coronary flow velocity reserve in patients with type 2 diabetes mellitus: Comparison between angiotensin-converting enzyme inhibitor and angiotensin II type 1 receptor antagonist. Am. Heart J. 2006, 151, e9–e798. [Google Scholar] [CrossRef] [PubMed]
- Kawata, T.; Daimon, M.; Hasegawa, R.; Toyoda, T.; Sekine, T.; Himi, T.; Uchida, D.; Miyazaki, S.; Hirose, K.; Ichikawa, R.; et al. Prognostic value of coronary flow reserve assessed by transthoracic Doppler echocardiography on long-term outcome in asymptomatic patients with type 2 diabetes without overt coronary artery disease. Cardiovasc. Diabetol. 2013, 12, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortigiani, L.; Rigo, F.; Gherardi, S.; Galderisi, M.; Bovenzi, F.; Sicari, R. Prognostic Meaning of Coronary Microvascular Disease in Type 2 Diabetes Mellitus: A Transthoracic Doppler Echocardiographic Study. J. Am. Soc. Echocardiogr. 2014, 27, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Antony, I.; Nitenberg, A.; Foult, J.M.; Aptecar, E. Coronary vasodilator reserve in untreated and treated hypertensive patients with and without left ventricular hypertrophy. J. Am. Coll. Cardiol. 1993, 22, 514–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozàkovà, M.; Palombo, C.; Pratali, L.; Pittella, G.; Galetta, F.; L’Abbate, A. Mechanisms of coronary flow reserve impairment in human hypertension. An integrated approach by transthoracic and transesophageal echocardiography. Hypertension 1997, 29, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Brush, J.E.; Cannon, R.O.; Schenke, W.H.; Bonow, R.O.; Leon, M.B.; Maron, B.J.; Epstein, S.E. Angina due to coronary microvascular disease in hypertensive patients without left ventricular hypertrophy. N. Engl. J. Med. 1988, 319, 1302–1307. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, D.; Yildirim, I.; Ciftci, O.; Ozer, I.; Caliskan, M.; Gullu, H.; Muderrisoglu, H. Effects of Normal Blood Pressure, Prehypertension, and Hypertension on Coronary Microvascular Function. Circulation 2007, 115, 593–599. [Google Scholar] [CrossRef] [Green Version]
- Pereira, V.; de Carvalho Frimm, C.; Rodrigues, A.; Tsutsui, J.M.; Cúri, M.; Mady, C.; Ramires, J. Coronary flow velocity reserve in hypertensive patients with left ventricular systolic dysfunction. Clin. Cardiol. 2002, 25, 95–102. [Google Scholar] [CrossRef]
- Völz, S.; Svedlund, S.; Andersson, B.; Li-Ming, G.; Rundqvist, B. Coronary flow reserve in patients with resistant hypertension. Clin. Res. Cardiol. 2017, 106, 151–157. [Google Scholar] [CrossRef]
- Marcus, M.L.; Doty, D.B.; Hiratzka, L.F.; Wright, C.B.; Eastham, C.L. Decreased coronary reserve: A mechanism for angina pectoris in patients with aortic stenosis and normal coronary arteries. N. Engl. J. Med. 1982, 307, 1362–1366. [Google Scholar] [CrossRef]
- O’Keefe, D.D.; Hoffman, J.I.; Cheitlin, R.; O’Neill, M.J.; Allard, J.R.; Shapkin, E. Coronary blood flow in experimental canine left ventricular hypertrophy. Circ. Res. 1978, 43, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Hildick-Smith, D.J.; Shapiro, L.M. Coronary flow reserve improves after aortic valve replacement for aortic stenosis: An adenosine transthoracic echocardiography study. J. Am. Coll. Cardiol. 2000, 36, 1889–1896. [Google Scholar] [CrossRef] [Green Version]
- Banovic, M.; Bosiljka, V.-T.; Voin, B.; Milan, P.; Ivana, N.; Dejana, P.; Danijela, T.; Serjan, N. Prognostic value of coronary flow reserve in asymptomatic moderate or severe aortic stenosis with preserved ejection fraction and nonobstructed coronary arteries. Echocardiography 2014, 31, 428–433. [Google Scholar] [CrossRef]
- Noto, N.; Karasawa, K.; Ayusawa, M.; Misawa, M.; Sumitomo, N.; Okada, T.; Harada, K. Measurement of coronary flow reserve in children by transthoracic Doppler echocardiography. Am. J. Cardiol. 1997, 80, 1638–1639. [Google Scholar] [CrossRef]
- Noto, N.; Karasawa, K.; Kanamaru, H.; Ayusawa, M.; Sumitomo, N.; Okada, T.; Harada, K. Non-invasive measurement of coronary flow reserve in children with Kawasaki disease. Heart 2002, 87, 559–565. [Google Scholar] [CrossRef]
- Hiraishi, S.; Hirota, H.; Horiguchi, Y.; Takeda, N.; Fujino, N.; Ogawa, N.; Nakahata, Y. Transthoracic Doppler assessment of coronary flow velocity reserve in children with Kawasaki disease: Comparison with coronary angiography and thallium-201 imaging. J. Am. Coll. Cardiol. 2002, 40, 1816–1824. [Google Scholar] [CrossRef] [Green Version]
- Tsuda, E.; Hashimoto, S. Characteristics of coronary flow velocity reserve on transthoracic Doppler echocardiography in patients with a history of Kawasaki disease. Cardiol. Young 2022, 32, 1451–1455. [Google Scholar] [CrossRef]
- Harada, K.; Yasuoka, K.; Tamura, M.; Toyono, M. Coronary flow reserve assessment by Doppler echocardiography in children with and without congenital heart defect: Comparison with invasive technique. J. Am. Soc. Echocardiogr. 2002, 15, 1121–1126. [Google Scholar] [CrossRef]
- Harada, K.; Tamura, M.; Toyono, M.; Takada, G. Transthoracic Doppler echocardiographic measurement of flow velocity and flow velocity reserve in the great cardiac vein and in the left anterior descending coronary artery in children with left ventricular volume overload secondary to ventricular septal defect. Am. J. Cardiol. 2002, 89, 1129–1133. [Google Scholar] [CrossRef]
- Nohtomi, Y.; Takeuchi, M.; Nagasawa, K.; Arimura, K.; Miyata, K.; Kuwata, K.; Yamawaki, T.; Kondo, S.; Yamada, A.; Okamatsu, S. Simultaneous assessment of wall motion and coronary flow velocity in the left anterior descending coronary artery during dipyridamole stress echocardiography. J. Am. Soc. Echocardiogr. 2003, 16, 457–463. [Google Scholar] [CrossRef]
- Takeuchi, M.; Miyazaki, C.; Yoshitani, H.; Otani, S.; Sakamoto, K.; Yoshikawa, J. Which is the better method in detecting significant left anterior descending coronary artery stenosis during contrast-enhanced dobutamine stress echocardiography: Coronary flow velocity reserve or wall-motion assessment? J. Am. Soc. Echocardiogr. 2003, 16, 614–621. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Civieri, G.; Montisci, R.; Kerkhof, P.L.M.; Iliceto, S.; Tona, F. Coronary Flow Velocity Reserve by Echocardiography: Beyond Atherosclerotic Disease. Diagnostics 2023, 13, 193. https://doi.org/10.3390/diagnostics13020193
Civieri G, Montisci R, Kerkhof PLM, Iliceto S, Tona F. Coronary Flow Velocity Reserve by Echocardiography: Beyond Atherosclerotic Disease. Diagnostics. 2023; 13(2):193. https://doi.org/10.3390/diagnostics13020193
Chicago/Turabian StyleCivieri, Giovanni, Roberta Montisci, Peter L. M. Kerkhof, Sabino Iliceto, and Francesco Tona. 2023. "Coronary Flow Velocity Reserve by Echocardiography: Beyond Atherosclerotic Disease" Diagnostics 13, no. 2: 193. https://doi.org/10.3390/diagnostics13020193