

Relationship between Serum 25-Hydroxyvitamin D Levels and Hormonal Status in Infertile Women: A Retrospective Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Anthropometric Assessments and Blood Assays
2.3. Statistical Analysis
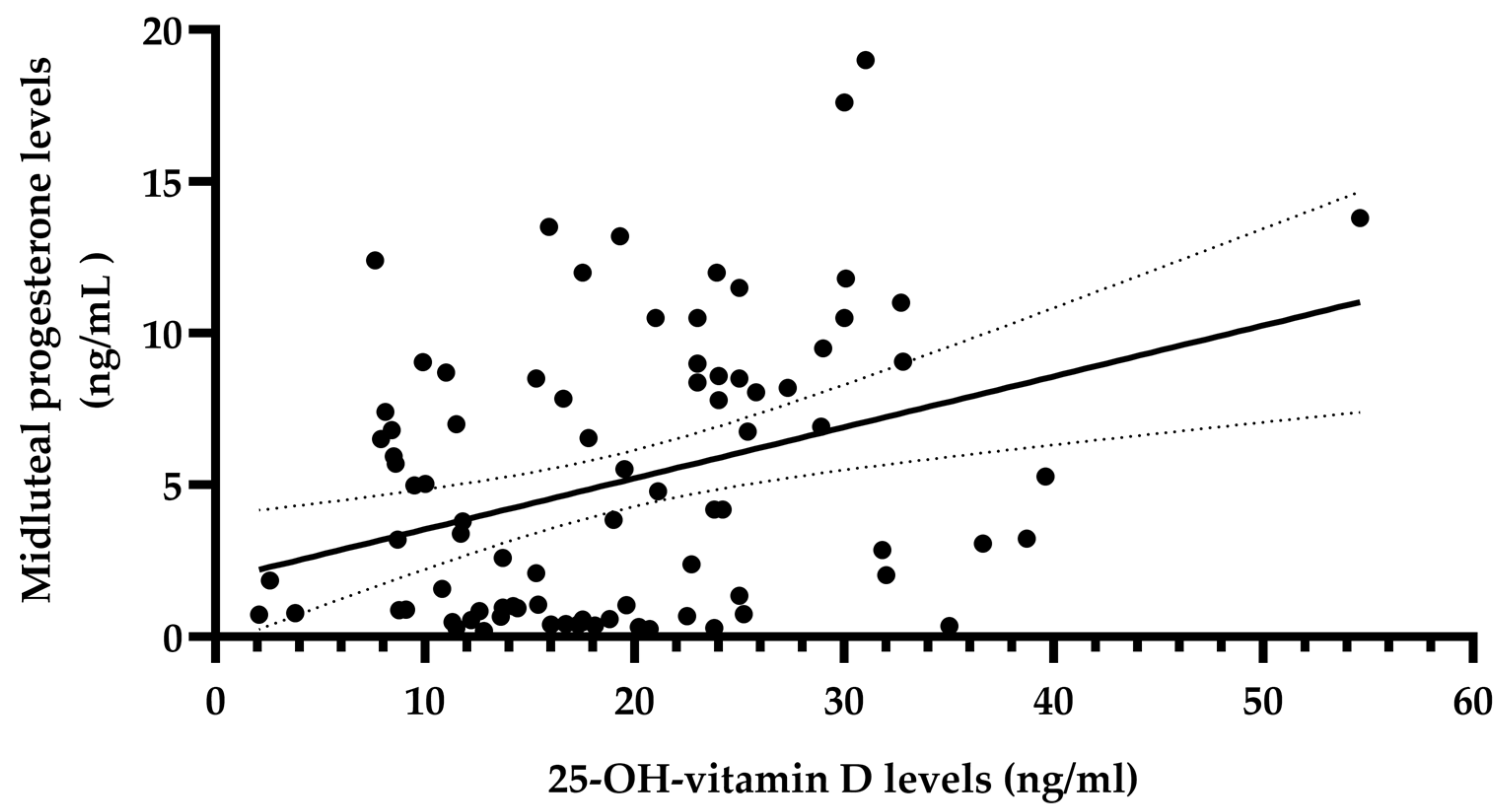
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aghajanova, L.; Hoffman, J.; Mok-Lin, E.; Herndon, C.N. Obstetrics and Gynecology Residency and Fertility Needs: National Survey Results. Reprod. Sci. 2017, 24, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Vander Borght, M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin. Biochem. 2018, 62, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Mulgund, A.; Hamada, A.; Chyatte, M.R. A unique view on male infertility around the globe. Reprod. Biol. Endocrinol. 2015, 13, 37. [Google Scholar] [CrossRef]
- Hanson, B.; Johnstone, E.; Dorais, J.; Silver, B.; Peterson, C.M.; Hotaling, J. Female infertility, infertility-associated diagnoses, and comorbidities: A review. J. Assist. Reprod. Genet. 2017, 34, 167–177. [Google Scholar] [CrossRef]
- Irani, M.; Merhi, Z. Role of vitamin D in ovarian physiology and its implication in reproduction: A systematic review. Fertil. Steril. 2014, 102, 460–468.e3. [Google Scholar] [CrossRef]
- Xu, J.; Lawson, M.S.; Xu, F.; Du, Y.; Tkachenko, O.Y.; Bishop, C.V.; Pejovic-Nezhat, L.; Seifer, D.B.; Hennebold, J.D. Vitamin D3 Regulates Follicular Development and Intrafollicular Vitamin D Biosynthesis and Signaling in the Primate Ovary. Front. Physiol. 2018, 9, 1600. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Altieri, B.; de Angelis, C.; Palomba, S.; Pivonello, R.; Colao, A.; Orio, F. Shedding new light on female fertility: The role of vitamin D. Rev. Endocr. Metab. Disord. 2017, 18, 273–283. [Google Scholar] [CrossRef]
- Wehr, E.; Trummer, O.; Giuliani, A.; Gruber, H.-J.; Pieber, T.R.; Obermayer-Pietsch, B. Vitamin D-associated polymorphisms are related to insulin resistance and vitamin D deficiency in polycystic ovary syndrome. Eur. J. Endocrinol. 2011, 164, 741–749. [Google Scholar] [CrossRef]
- Guo, S.; Tal, R.; Jiang, H.; Yuan, T.; Liu, Y. Vitamin D Supplementation Ameliorates Metabolic Dysfunction in Patients with PCOS: A SystematicReview of RCTs and Insight into the Underlying Mechanism. Int. J. Endocrinol. 2020, 2020, 7850816. [Google Scholar] [CrossRef]
- Morgante, G.; Darino, I.; Spanò, A.; Luisi, S.; Luddi, A.; Piomboni, P.; Governini, L.; De Leo, V. PCOS Physiopathology and Vitamin D Deficiency: Biological Insights and Perspectives for Treatment. J. Clin. Med. 2022, 11, 4509. [Google Scholar] [CrossRef]
- Łagowska, K.; Bajerska, J.; Jamka, M. The Role of Vitamin D Oral Supplementation in Insulin Resistance in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 1637. [Google Scholar] [CrossRef] [PubMed]
- Grineva, E.; Karonova, T.; Micheeva, E.; Belyaeva, O.; Belyaeva, I. Vitamin D deficiency is a risk factor for obesity and diabetes type 2 in women at late reproductive age. Aging 2013, 5, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Krul-Poel, Y.H.M.; Koenders, P.P.; Steegers-Theunissen, R.P.; ten Boekel, E.; ter Wee, M.M.; Louwers, Y.; Lips, P.; Laven, J.S.E.; Simsek, S. Vitamin D and metabolic disturbances in polycystic ovary syndrome (PCOS): A cross-sectional study. PLoS ONE 2018, 13, e0204748. [Google Scholar] [CrossRef]
- Dennis, N.; Houghton, L.; Pankhurst, M.; Harper, M.; McLennan, I. Acute Supplementation with High Dose Vitamin D3 Increases Serum Anti-Müllerian Hormone in Young Women. Nutrients 2017, 9, 719. [Google Scholar] [CrossRef] [PubMed]
- Moridi, I.; Chen, A.; Tal, O.; Tal, R. The Association between Vitamin D and Anti-Müllerian Hormone: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1567. [Google Scholar] [CrossRef]
- Jukic, A.M.Z.; Baird, D.D.; Wilcox, A.J.; Weinberg, C.R.; Steiner, A.Z. 25-Hydroxyvitamin D (25(OH)D) and biomarkers of ovarian reserve. Menopause 2018, 25, 811–816. [Google Scholar] [CrossRef]
- Karimi, E.; Arab, A.; Rafiee, M.; Amani, R. A systematic review and meta-analysis of the association between vitamin D and ovarian reserve. Sci. Rep. 2021, 11, 16005. [Google Scholar] [CrossRef]
- Lou, Y.-R.; Murtola, T.; Tuohimaa, P. Regulation of aromatase and 5α-reductase by 25-hydroxyvitamin D3, 1α,25-dihydroxyvitamin D3, dexamethasone and progesterone in prostate cancer cells. J. Steroid Biochem. Mol. Biol. 2005, 94, 151–157. [Google Scholar] [CrossRef]
- Mahmoudi, T.; Gourabi, H.; Ashrafi, M.; Yazdi, R.S.; Ezabadi, Z. Calciotropic hormones, insulin resistance, and the polycystic ovary syndrome. Fertil. Steril. 2010, 93, 1208–1214. [Google Scholar] [CrossRef]
- He, C.; Lin, Z.; Robb, S.; Ezeamama, A. Serum Vitamin D Levels and Polycystic Ovary syndrome: A Systematic Review and Meta-Analysis. Nutrients 2015, 7, 4555–4577. [Google Scholar] [CrossRef]
- Gáll, Z.; Székely, O. Role of vitamin d in cognitive dysfunction: New molecular concepts and discrepancies between animal and human findings. Nutrients 2021, 13, 3672. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Holick, M.F.; Grant, W.B.; Konstantynowicz, J.; Mascarenhas, M.R.; Haq, A.; Povoroznyuk, V.; Balatska, N.; Barbosa, A.P.; Karonova, T.; et al. Vitamin D supplementation guidelines. J. Steroid Biochem. Mol. Biol. 2018, 175, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Płudowski, P.; Kos-Kudła, B.; Walczak, M.; Fal, A.; Zozulińska-Ziółkiewicz, D.; Sieroszewski, P.; Peregud-Pogorzelski, J.; Lauterbach, R.; Targowski, T.; Lewiński, A.; et al. Guidelines for Preventing and Treating Vitamin D Deficiency: A 2023 Update in Poland. Nutrients 2023, 15, 695. [Google Scholar] [CrossRef] [PubMed]
- Gáll, Z.; Csukor, B.; Urkon, M.; Farczádi, L.; Kolcsár, M. Vitamin D Status Assessment: Lack of Correlation between Serum and Hair 25-Hydroxycholecalciferol Levels in Healthy Young Adults. Diagnostics 2022, 12, 1229. [Google Scholar] [CrossRef] [PubMed]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- González-Gross, M.; Valtueña, J.; Breidenassel, C.; Moreno, L.A.; Ferrari, M.; Kersting, M.; De Henauw, S.; Gottrand, F.; Azzini, E.; Widhalm, K.; et al. Vitamin D status among adolescents in Europe: The Healthy Lifestyle in Europe by Nutrition in Adolescence study. Br. J. Nutr. 2012, 107, 755–764. [Google Scholar] [CrossRef]
- Chirita-Emandi, A.; Socolov, D.; Haivas, C.; Calapiș, A.; Gheorghiu, C.; Puiu, M. Vitamin D Status: A Different Story in the Very Young versus the Very Old Romanian Patients. PLoS ONE 2015, 10, e0128010. [Google Scholar] [CrossRef]
- Zhao, J.; Fu, S.; Chen, Q. Association between the serum vitamin D level and prevalence of obesity/abdominal obesity in women with infertility: A cross-sectional study of the National Health and Nutrition Examination Survey data. Gynecol. Endocrinol. 2023, 39, 2217251. [Google Scholar] [CrossRef]
- Kalaitzopoulos, D.R.; Samartzis, N.; Daniilidis, A.; Leeners, B.; Makieva, S.; Nirgianakis, K.; Dedes, I.; Metzler, J.M.; Imesch, P.; Lempesis, I.G. Effects of vitamin D supplementation in endometriosis: A systematic review. Reprod. Biol. Endocrinol. 2022, 20, 176. [Google Scholar] [CrossRef]
- Ciebiera, M.; Włodarczyk, M.; Ciebiera, M.; Zaręba, K.; Łukaszuk, K.; Jakiel, G. Vitamin D and Uterine Fibroids—Review of the Literature and Novel Concepts. Int. J. Mol. Sci. 2018, 19, 2051. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Dai, M.; Zhong, Z.; Zhu, S.; Gong, G.; Chen, M.; Guo, J.; Zhang, Y. The association between vitamin D and uterine fibroids: A mendelian randomization study. Front. Genet. 2022, 13, 1013192. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, S.; Jindal, S.; Greenseid, K.; Shu, J.; Zeitlian, G.; Hickmon, C.; Pal, L. Replete vitamin D stores predict reproductive success following in vitro fertilization. Fertil. Steril. 2010, 94, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Baldini, D.; Malvasi, A.; Kosmas, I.; Baldini, G.M.; Silvestris, E. Increased bioavailability of Vitamin D improved pregnancy outcomes in in vitro fertilization cycles, only in patients over 36 years: A cross-sectional study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4964–4972. [Google Scholar] [CrossRef] [PubMed]
- Cimadomo, D.; de los Santos, M.J.; Griesinger, G.; Lainas, G.; Le Clef, N.; McLernon, D.J.; Montjean, D.; Toth, B.; Vermeulen, N.; Macklon, N. ESHRE good practice recommendations on recurrent implantation failure. Hum. Reprod. Open 2023, 2023, hoad023. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Diagnostic evaluation of the infertile female: A committee opinion. Fertil. Steril. 2015, 103, e44–e50. [Google Scholar] [CrossRef]
- Practice Committees of the American Society for Reproductive Medicine and the Society for Reproductive Endocrinology and Infertility. Diagnosis and treatment of luteal phase deficiency: A committee opinion. Fertil. Steril. 2021, 115, 1416–1423. [Google Scholar] [CrossRef]
- Aswini, R.; Jayapalan, S. Modified Ferriman–Gallwey score in hirsutism and its association with metabolic syndrome. Int. J. Trichology 2017, 9, 7. [Google Scholar] [CrossRef]
- Committee on Gynecologic Practice; American Society for Reproductive Medicine. Infertility Workup for the Women’s Health Specialist: ACOG Committee Opinion, Number 781. Obstet. Gynecol. 2019, 133, e377–e384. [Google Scholar] [CrossRef]
- Simental-Mendía, L.E.; Rodríguez-Morán, M.; Guerrero-Romero, F. The Product of Fasting Glucose and Triglycerides as Surrogate for Identifying Insulin Resistance in Apparently Healthy Subjects. Metab. Syndr. Relat. Disord. 2008, 6, 299–304. [Google Scholar] [CrossRef]
- Vasques, A.C.J.; Novaes, F.S.; de Oliveira, M.d.S.; Matos Souza, J.R.; Yamanaka, A.; Pareja, J.C.; Tambascia, M.A.; Saad, M.J.A.; Geloneze, B. TyG index performs better than HOMA in a Brazilian population: A hyperglycemic clamp validated study. Diabetes Res. Clin. Pract. 2011, 93, e98–e100. [Google Scholar] [CrossRef] [PubMed]
- Voulgaris, N.; Papanastasiou, L.; Piaditis, G.; Angelousi, A.; Kaltsas, G.; Mastorakos, G.; Kassi, E. Vitamin D and aspects of female fertility. Hormones 2017, 16, 5–21. [Google Scholar] [PubMed]
- Várbíró, S.; Takács, I.; Tűű, L.; Nas, K.; Sziva, R.E.; Hetthéssy, J.R.; Török, M. Effects of Vitamin D on Fertility, Pregnancy and Polycystic Ovary Syndrome—A Review. Nutrients 2022, 14, 1649. [Google Scholar] [CrossRef] [PubMed]
- Bednarska-Czerwińska, A.; Olszak-Wąsik, K.; Olejek, A.; Czerwiński, M.; Tukiendorf, A. Vitamin D and Anti-Müllerian Hormone Levels in Infertility Treatment: The Change-Point Problem. Nutrients 2019, 11, 1053. [Google Scholar] [CrossRef]
- Grzeczka, A.; Graczyk, S.; Skowronska, A.; Skowronski, M.T.; Kordowitzki, P. Relevance of Vitamin D and Its Deficiency for the Ovarian Follicle and the Oocyte: An Update. Nutrients 2022, 14, 3712. [Google Scholar] [CrossRef]
- Wathen, N.C.; Perry, L.; Lilford, R.J.; Chard, T. Interpretation of single progesterone measurement in diagnosis of anovulation and defective luteal phase: Observations on analysis of the normal range. BMJ 1984, 288, 7–9. [Google Scholar] [CrossRef]
- Leiva, R.; Bouchard, T.; Boehringer, H.; Abulla, S.; Ecochard, R. Random serum progesterone threshold to confirm ovulation. Steroids 2015, 101, 125–129. [Google Scholar] [CrossRef]
- Filicori, M.; Butler, J.P.; Crowley, W.F. Neuroendocrine regulation of the corpus luteum in the human. Evidence for pulsatile progesterone secretion. J. Clin. Investig. 1984, 73, 1638–1647. [Google Scholar] [CrossRef]
- Mesen, T.B.; Young, S.L. Progesterone and the Luteal Phase. Obstet. Gynecol. Clin. N. Am. 2015, 42, 135–151. [Google Scholar] [CrossRef]
- Parikh, G.; Varadinova, M.; Suwandhi, P.; Araki, T.; Rosenwaks, Z.; Poretsky, L.; Seto-Young, D. Vitamin D Regulates Steroidogenesis and Insulin-like Growth Factor Binding Protein-1 (IGFBP-1) Production in Human Ovarian Cells. Horm. Metab. Res. 2010, 42, 754–757. [Google Scholar] [CrossRef]
- Chu, C.; Tsuprykov, O.; Chen, X.; Elitok, S.; Krämer, B.K.; Hocher, B. Relationship Between Vitamin D and Hormones Important for Human Fertility in Reproductive-Aged Women. Front. Endocrinol. 2021, 12, 666687. [Google Scholar] [CrossRef] [PubMed]
- Chu, J.; Gallos, I.; Tobias, A.; Robinson, L.; Kirkman-Brown, J.; Dhillon-Smith, R.; Harb, H.; Eapen, A.; Rajkhowa, M.; Coomarasamy, A. Vitamin D and assisted reproductive treatment outcome: A prospective cohort study. Reprod. Health 2019, 16, 106. [Google Scholar] [CrossRef] [PubMed]
- Ota, K.; Dambaeva, S.; Han, A.-R.; Beaman, K.; Gilman-Sachs, A.; Kwak-Kim, J. Vitamin D deficiency may be a risk factor for recurrent pregnancy losses by increasing cellular immunity and autoimmunity. Hum. Reprod. 2014, 29, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Bender Atik, R.; Christiansen, O.B.; Elson, J.; Kolte, A.M.; Lewis, S.; Middeldorp, S.; Mcheik, S.; Peramo, B.; Quenby, S.; Nielsen, H.S.; et al. ESHRE guideline: Recurrent pregnancy loss: An update in 2022. Hum. Reprod. Open 2022, 2023, hoad002. [Google Scholar] [CrossRef]
- Meng, X.; Zhang, J.; Wan, Q.; Huang, J.; Han, T.; Qu, T.; Yu, L. Influence of Vitamin D supplementation on reproductive outcomes of infertile patients: A systematic review and meta-analysis. Reprod. Biol. Endocrinol. 2023, 21, 17. [Google Scholar] [CrossRef] [PubMed]
- Sablok, A.; Batra, A.; Thariani, K.; Batra, A.; Bharti, R.; Aggarwal, A.R.; Kabi, B.C.; Chellani, H. Supplementation of vitamin D in pregnancy and its correlation with feto-maternal outcome. Clin. Endocrinol. 2015, 83, 536–541. [Google Scholar] [CrossRef]
- Rostami, M.; Tehrani, F.R.; Simbar, M.; Bidhendi Yarandi, R.; Minooee, S.; Hollis, B.W.; Hosseinpanah, F. Effectiveness of Prenatal Vitamin D Deficiency Screening and Treatment Program: A Stratified Randomized Field Trial. J. Clin. Endocrinol. Metab. 2018, 103, 2936–2948. [Google Scholar] [CrossRef]
- Mumford, S.L.; Garbose, R.A.; Kim, K.; Kissell, K.; Kuhr, D.L.; Omosigho, U.R.; Perkins, N.J.; Galai, N.; Silver, R.M.; Sjaarda, L.A.; et al. Association of preconception serum 25-hydroxyvitamin D concentrations with livebirth and pregnancy loss: A prospective cohort study. Lancet Diabetes Endocrinol. 2018, 6, 725–732. [Google Scholar] [CrossRef]
- Bialy, L.; Fenton, T.; Shulhan-Kilroy, J.; Johnson, D.W.; McNeil, D.A.; Hartling, L. Vitamin D supplementation to improve pregnancy and perinatal outcomes: An overview of 42 systematic reviews. BMJ Open 2020, 10, e032626. [Google Scholar] [CrossRef]
- Cavoretto, P.I.; Viganò, P. Time to implement vitamin D assessment and supplementation into routine obstetric practice? Fertil. Steril. 2022, 118, 123–124. [Google Scholar] [CrossRef]
- Mohan, A.; Haider, R.; Fakhor, H.; Hina, F.; Kumar, V.; Jawed, A.; Majumder, K.; Ayaz, A.; Lal, P.M.; Tejwaney, U.; et al. Vitamin D and polycystic ovary syndrome (PCOS): A review. Ann. Med. Surg. 2023, 85, 3506–3511. [Google Scholar] [CrossRef] [PubMed]
- Szymczak-Pajor, I.; Śliwińska, A. Analysis of Association between Vitamin D Deficiency and Insulin Resistance. Nutrients 2019, 11, 794. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.; Seidler, K.; Neil, J. Vitamin D deficiency and female infertility: A mechanism review examining the role of vitamin D in ovulatory dysfunction as a symptom of polycystic ovary syndrome. J. Reprod. Immunol. 2022, 151, 103633. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lacy, M.E.; Jankowich, M.; Correa, A.; Wu, W.-C. Association between obesity phenotypes of insulin resistance and risk of type 2 diabetes in African Americans: The Jackson Heart Study. J. Clin. Transl. Endocrinol. 2020, 19, 100210. [Google Scholar] [CrossRef]
- Placzkowska, S.; Pawlik-Sobecka, L.; Kokot, I.; Piwowar, A. Indirect insulin resistance detection: Current clinical trends and laboratory limitations. Biomed. Pap. 2019, 163, 187–199. [Google Scholar] [CrossRef]
- Sánchez-Íñigo, L.; Navarro-González, D.; Fernández-Montero, A.; Pastrana-Delgado, J.; Martínez, J.A. The TyG index may predict the development of cardiovascular events. Eur. J. Clin. Investig. 2016, 46, 189–197. [Google Scholar] [CrossRef]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef]


{kind=link}
| Variable (N = 86) | Mean (±SEM)/Median (Interquartile Range) |
|---|---|
| Age (years) | 31 (±0.66) |
| BMI (kg/m2) | 23 (21–26) |
| Total cholesterol (mg/dL) | 159 (147–202) |
| Triglyceride (mg/dL) | 150 (141–171) |
| Plasma glucose (mg/dL) | 93 (89–96) |
| TyG index | 8.9 (8.8–9) |
| TSH (mIU/L) | 1.8 (1–2.8) |
| ATPO antibody (µIU/mL) | 28 (15–48) |
| Mid-luteal phase progesterone (ng/mL) | 4 (0.88–8.5) |
| Early follicular phase LH (IU/L) * | 7.57 (±0.35) |
| Early follicular phase FSH (IU/L) * | 2.2 (1.8–3.1) |
| Follicular phase total testosterone (ng/mL) * | 31 (21–44) |
| Prolactin (ng/mL) | 15 (11–18) |
| 25-OH-VD (ng/mL) | 19 (±1) |
| Variable (N = 86) | R | 95% CI | p |
|---|---|---|---|
| Age (years) | 0.021 | −0.197 to 0.238 | 0.846 |
| BMI (kg/m2) | −0.131 | −0.340 to 0.088 | 0.225 |
| Total cholesterol (mg/dL) | 0.031 | −0.187 to 0.247 | 0.771 |
| TyG index | 0.035 | −0.184 to 0.251 | 0.748 |
| TSH (mIU/L) | −0.07 | −0.282 to 0.151 | 0.526 |
| ATPO antibody (µIU/mL) | 0.005 | −0.212 to 0.223 | 0.961 |
| Prolactin (ng/mL) | 0.116 | −0.104 to 0.325 | 0.287 |
| 25-OH-VD (ng/mL) | 0.280 | 0.0668 to 0.469 | 0.009 |
| Variables | Ovulatory Cycles (N = 49) | Anovulatory Cycles (N = 37) | p |
|---|---|---|---|
| Age (years) | 31.06 ± 0.85 | 30.54 ± 1.05 | 0.790 (t test) |
| BMI (kg/m2) | 22.00 (20.50–25.00) | 23.00 (20.50–27.50 d) | 0.344 (MW-test) |
| Total cholesterol (mg/dL) | 158 (146.5–204) | 160 (147–200) | 0.919 (MW test) |
| TyG index | 8.86 (8.77–8.95) | 8.82 (8.73–8.99) | 0.619 (MW test) |
| TSH (mIU/L) | 1.89 ± 0.14 | 2.07 ± 0.16 | 0.423 (t test) |
| ATPO antibody (µIU/mL) | 22.9 (20.9–25.3) | 25 (15–45) | 0.730 (MW-test) |
| Prolactin (ng/mL) | 14.79 ± 0.64 | 13.68 ± 0.71 | 0.251 (t test) |
| 25-OH-VD (ng/mL) | 21.38 ± 1.44 | 16.70 ± 1.23 | 0.020 (t test) |
| Variables | VIF | R2 with Other Variables |
|---|---|---|
| Age (years) | 1.078 | 0.0719 |
| BMI (kg/m2) | 1.150 | 0.1305 |
| Total cholesterol (mg/dL) | 1.103 | 0.0937 |
| TyG index | 1.106 | 0.0954 |
| TSH (mIU/L) | 1.054 | 0.0508 |
| ATPO antibody (µIU/mL) | 1.074 | 0.0686 |
| Prolactin (ng/mL) | 1.071 | 0.0663 |
| 25-OH-VD (ng/mL) | 1.085 | 0.0781 |
| Variables | Estimate | SE | 95% CI | |t| | p |
|---|---|---|---|---|---|
| Age (years) | 0.031 | 0.080 | −0.129 to 0.191 | 0.385 | 0.700 |
| BMI (kg/m2) | −0.069 | 0.102 | −0.273 to 0.133 | 0.681 | 0.497 |
| Total cholesterol (mg/dL) | 0.016 | 0.014 | −0.011 to 0.044 | 1.173 | 0.244 |
| TyG index | −0.138 | 2.406 | −4.929 to 4.654 | 0.057 | 0.954 |
| TSH (mIU/L) | −0.591 | 0.493 | −1.574 to 0.390 | 1.200 | 0.233 |
| ATPO antibody (µIU/mL) | 0.001 | 0.003 | −0.005 to 0.008 | 0.438 | 0.662 |
| Prolactin (ng/mL) | 0.056 | 0.111 | −0.165 to 0.278 | 0.504 | 0.615 |
| 25-OH-VD (ng/mL) | 0.173 | 0.053 | 0.067 to 0.278 | 3.259 | 0.001 |
| Variables | Δ (Means/Medians) ± SEM | Effect Size (d) | A Posteriori Power Data |
|---|---|---|---|
| Age (years) | −0.5207 ± 1.341 | 0.084 | 0.103 |
| BMI (kg/m2) | −1.00 | 0.268 | 0.229 |
| Total cholesterol (mg/dL) | 2.00 | 0.020 | 0.060 |
| TyG index | 0.049 | 0.005 | 0.052 |
| TSH (mIU/L) | 0.1738 ± 0.2158 | 0.175 | 0.199 |
| ATPO antibody (µIU/mL) | 0.00 | 0.434 | 0.486 |
| Prolactin (ng/mL) | −1.111 ± 0.9600 | 0.252 | 0.208 |
| 25-OH-VD (ng/mL) | −4.680 ± 1.978 | 0.526 | 0.773 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolcsár, M.; Berecki, B.; Gáll, Z. Relationship between Serum 25-Hydroxyvitamin D Levels and Hormonal Status in Infertile Women: A Retrospective Study. Diagnostics 2023, 13, 3024. https://doi.org/10.3390/diagnostics13193024
Kolcsár M, Berecki B, Gáll Z. Relationship between Serum 25-Hydroxyvitamin D Levels and Hormonal Status in Infertile Women: A Retrospective Study. Diagnostics. 2023; 13(19):3024. https://doi.org/10.3390/diagnostics13193024
Chicago/Turabian StyleKolcsár, Melinda, Bernadett Berecki, and Zsolt Gáll. 2023. "Relationship between Serum 25-Hydroxyvitamin D Levels and Hormonal Status in Infertile Women: A Retrospective Study" Diagnostics 13, no. 19: 3024. https://doi.org/10.3390/diagnostics13193024