
How Does Anxiety and Depression Affect the Outcome after Periradicular Infiltration Therapy?—A Retrospective Analysis of Patients Undergoing CT-Guided Single-Level Nerve Root Infiltration Due to Chronic Monoradicular Pain

Abstract
:1. Introduction
2. Materials and Methods
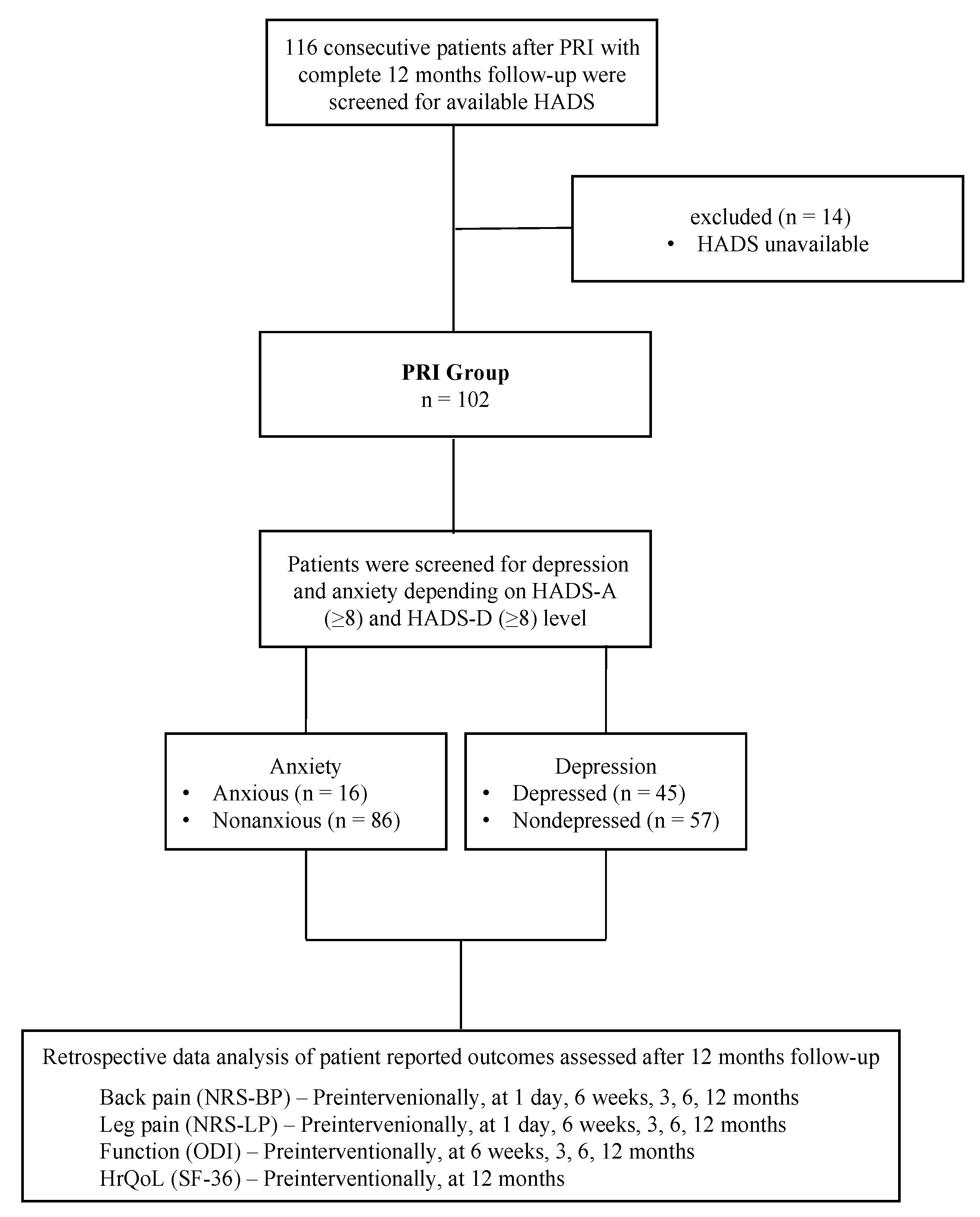
2.1. Patients and Study Design
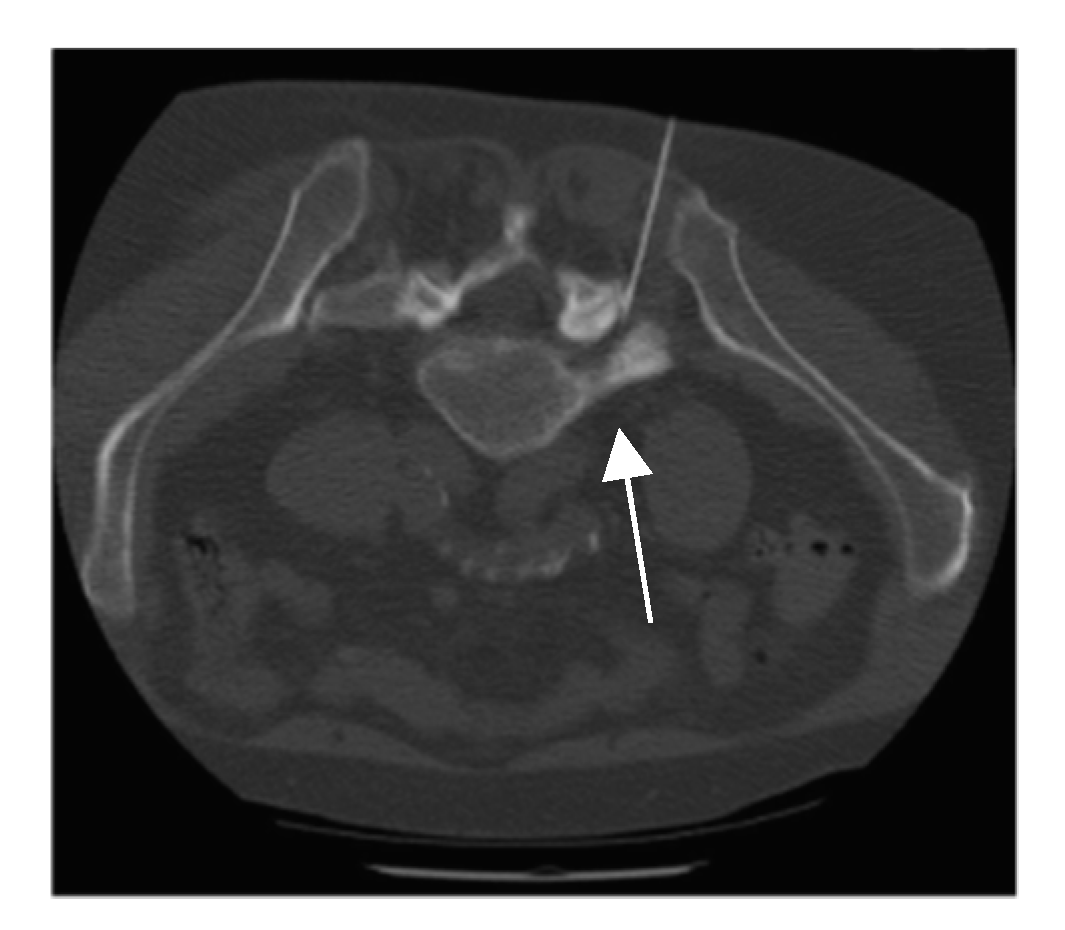
2.2. Intervention
2.3. Clinical Scores
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Baseline Demographics
3.2. Influence of Anxiety and Depression on Baseline PROs

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Anxious | Non-Anxious | p-Value | Depressed | Nondepressed | p-Value | |
|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| NRS-BP | 5.8 ± 2.2 | 7.1 ± 1.9 | 5.5 ± 2.1 | 0.007 | 6.3 ± 2.1 | 5.4 ± 2.2 | 0.026 |
| NRS-LP | 7.1 ± 1.8 | 7.8 ± 1.4 | 6.9 ± 1.8 | 0.083 | 7.8 ± 1.1 | 6.5 ± 2.0 | <0.001 |
| ODI | 47.3 ± 17.3 | 63.1 ± 13.0 | 44.3 ± 16.4 | <0.001 | 58 ± 13.9 | 38.8 ± 14.7 | <0.001 |
| SF-36 (pcs) | 33.0 ± 7.5 | 31.3 ± 7.8 | 33.3 ± 7.4 | 0.344 | 32.1 ± 7.4 | 33.6 ± 7.5 | 0.319 |
| SF-36 (mcs) | 47.8 ± 9.9 | 43.4 ± 10.9 | 48.7 ± 9.6 | 0.053 | 48.1 ± 10.7 | 47.6 ± 9.3 | 0.815 |
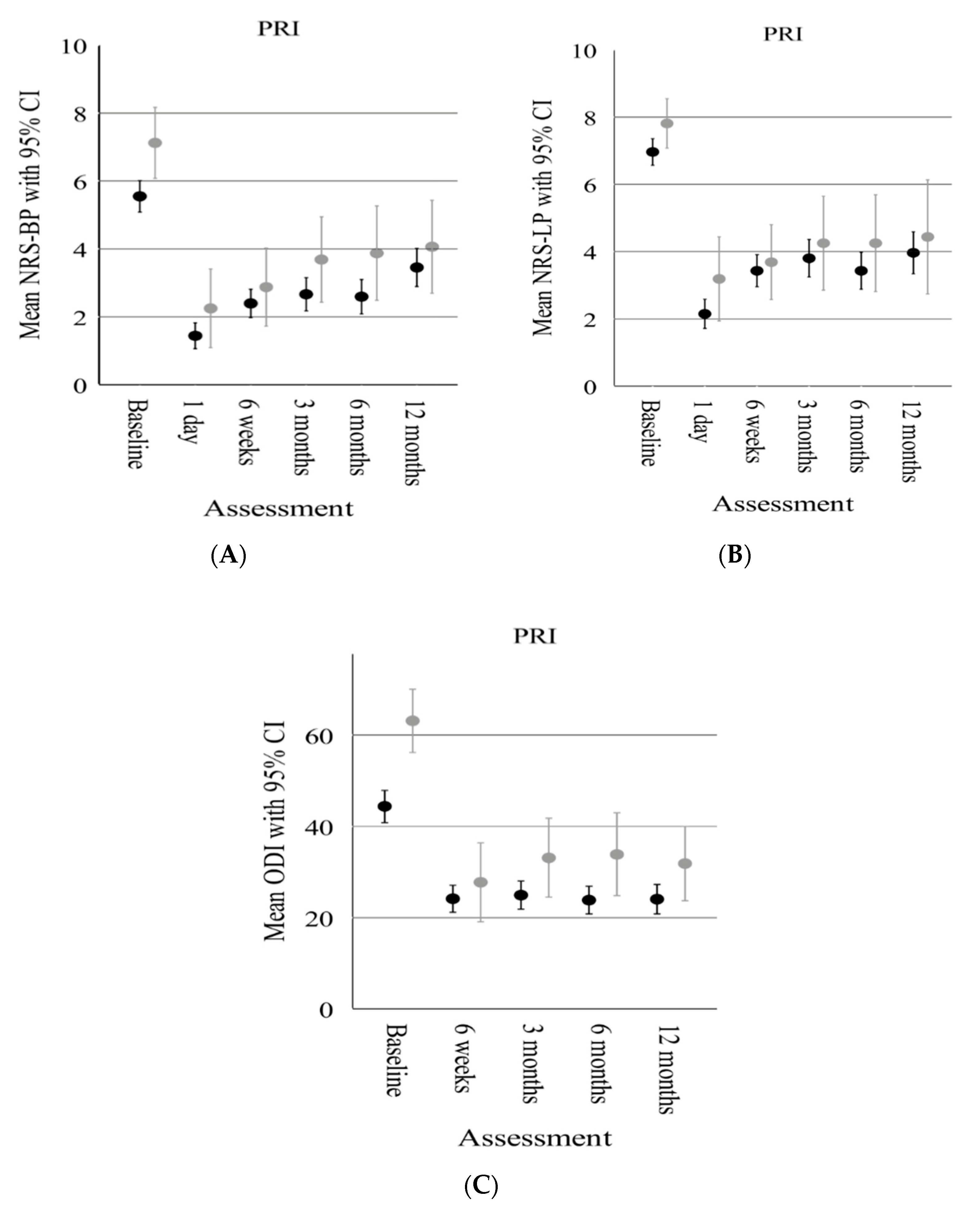
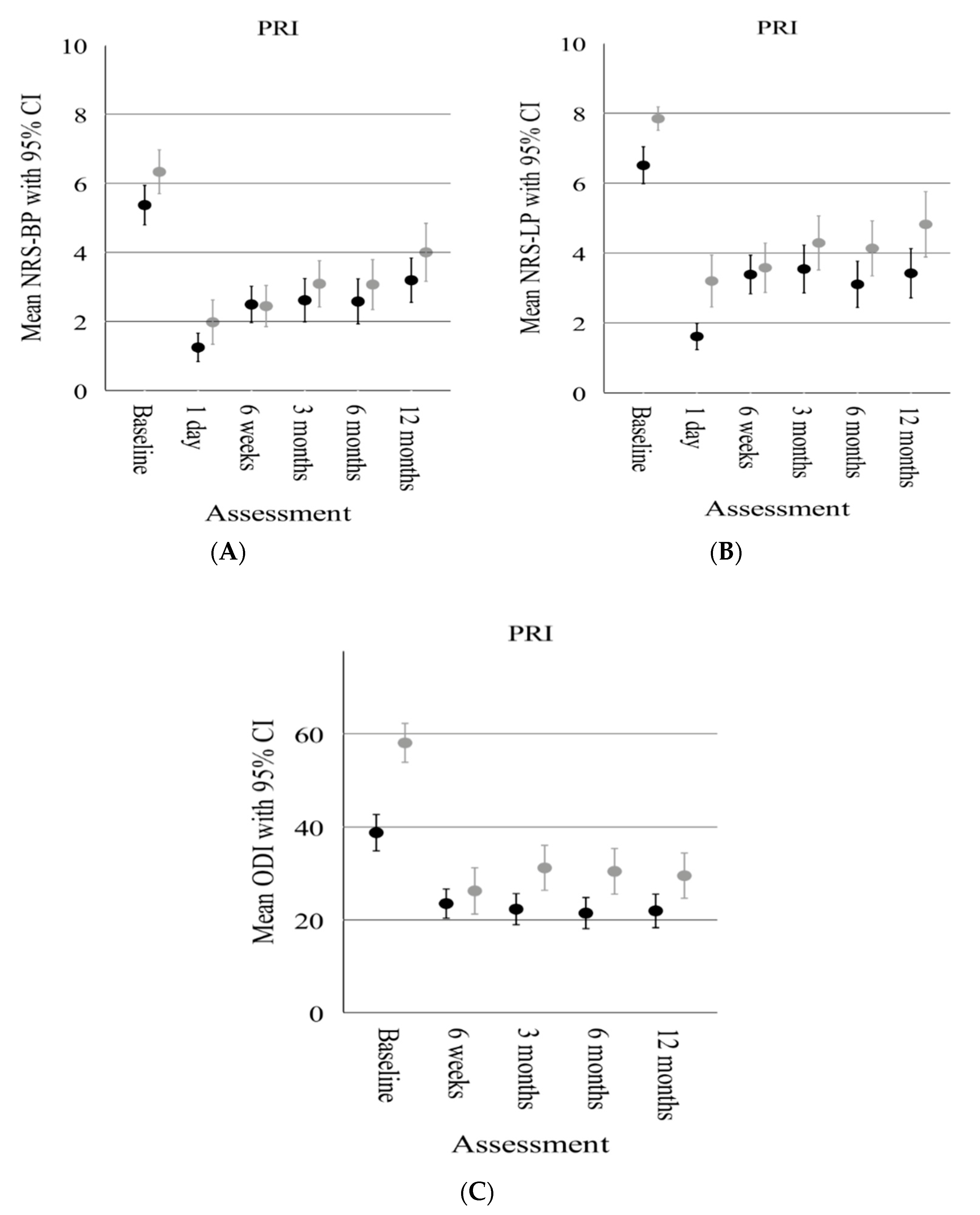
3.3. Influence of Anxiety and Depression on Clinical Improvement
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Manchikanti, L.; Singh, V.; Falco, F.J.; Benyamin, R.M.; Hirsch, J.A. Epidemiology of low back pain in adults. Neuromodulation 2014, 17 (Suppl. 2), 3–10. [Google Scholar] [CrossRef] [PubMed]
- Wettstein, M.; Eich, W.; Bieber, C.; Tesarz, J. Pain Intensity, Disability, and Quality of Life in Patients with Chronic Low Back Pain: Does Age Matter? Pain Med. 2019, 20, 464–475. [Google Scholar] [CrossRef] [PubMed]
- Dagenais, S.; Caro, J.; Haldeman, S. A systematic review of low back pain cost of illness studies in the United States and interna-tionally. Spine J. 2008, 8, 8–20. [Google Scholar] [CrossRef]
- Ivanova, J.I.; Birnbaum, H.G.; Schiller, M.; Kantor, E.; Johnstone, B.M.; Swindle, R.W. Real-world practice patterns, health-care utiliza-tion, and costs in patients with low back pain: The long road to guideline-concordant care. Spine J. 2011, 11, 622–632. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Pampati, V.; Hirsch, J.A. Utilization of Interventional Techniques in Managing Chronic Pain In Medicare Popu-lation from 2000 to 2014: An Analysis of Patterns of Utilization. Pain Physician 2016, 19, E531–E546. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.B.; Maher, C.G.; Ferreira, M.L.; Hancock, M.J.; Oliveira, V.C.; McLachlan, A.J.; Koes, B.W.; Ferreira, P.H.; Cohen, S.P.; Pinto, R.Z. Epidural corticosteroid injections for lumbosacral radicular pain. Cochrane Database Syst. Rev. 2020, 4, Cd013577. [Google Scholar] [CrossRef]
- Verheijen, E.J.A.; Bonke, C.A.; Amorij, E.M.J.; Vleggeert-Lankamp, C.L.A. Epidural steroid compared to placebo injection in sciatica: A systematic review and meta-analysis. Eur. Spine J. 2021, 30, 3255–3264. [Google Scholar] [CrossRef]
- Sivaganesan, A.; Chotai, S.; Parker, S.L.; Asher, A.L.; McGirt, M.J.; Devin, C.J. Predictors of the efficacy of epidural steroid injections for structural lumbar degenerative pathology. Spine J. 2016, 16, 928–934. [Google Scholar] [CrossRef]
- Kanna, R.M.; Shetty, A.P.; Rajasekaran, S. Predictors of Successful Outcomes of Selective Nerve Root Blocks for Acute Lumbar Disc Herniation. Global Spine J. 2019, 9, 473–479. [Google Scholar] [CrossRef]
- Hruschak, V.; Cochran, G. Psychosocial predictors in the transition from acute to chronic pain: A systematic review. Psychol. Health Med. 2018, 23, 1151–1167. [Google Scholar] [CrossRef]
- Wilhelm, M.; Reiman, M.; Goode, A.; Richardson, W.; Brown, C.; Vaughn, D.; Cook, C. Psychological Predictors of Outcomes with Lumbar Spinal Fusion: A Systematic Literature Review. Physiother. Res. Int. 2017, 22, e1648. [Google Scholar] [CrossRef] [PubMed]
- Sinikallio, S.; Aalto, T.; Airaksinen, O.; Herno, A.; Kroger, H.; Viinamaki, H. Depressive burden in the preoperative and early recov-ery phase predicts poorer surgery outcome among lumbar spinal stenosis patients: A one-year prospective follow-up study. Spine 2009, 34, 2573–2578. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Mukherjee, D.; Adogwa, O.; Cheng, J.S.; McGirt, M.J. Correlation of preoperative depression and somatic perception scales with postoperative disability and quality of life after lumbar discectomy. J. Neurosurg. Spine 2011, 14, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Chotai, S.; Stonko, D.P.; Wick, J.B.; Schneider, B.J.; McGirt, M.J.; Devin, C.J. Patient-reported outcomes after lumbar epidural steroid injection for degenerative spine disease in depressed versus non-depressed patients. Spine J. 2017, 17, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Bahar-Ozdemir, Y.; Sencan, S.; Ercalik, T.; Kokar, S.; Gunduz, O.H. The Effect of Pre-Treatment Depression, Anxiety and Somatiza-tion Levels on Transforaminal Epidural Steroid Injection: A Prospective Observational Study. Pain Physician 2020, 23, E273–E280. [Google Scholar]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef]
- Gossner, J. Safety of CT-Guided Lumbar Nerve Root Infiltrations. Analysis of a Two-Year Period. Interv. Neuroradiol. 2014, 20, 533–537. [Google Scholar] [CrossRef]
- Timpone, V.M.; Hirsch, J.A.; Gilligan, C.J.; Chandra, R.V. Computed tomography guidance for spinal intervention: Basics of technique, pearls, and avoiding pitfalls. Pain Physician 2013, 16, 369–377. [Google Scholar] [CrossRef]
- Fairbank, J.C. Why are there different versions of the Oswestry Disability Index? J. Neurosurg. Spine 2014, 20, 83–86. [Google Scholar] [CrossRef]
- Osthus, H.; Cziske, R.; Jacobi, E. Cross-cultural adaptation of a German version of the Oswestry Disability Index and evaluation of its measurement properties. Spine 2006, 31, E448–E453. [Google Scholar] [CrossRef]
- Müller, H.; Franke, A.; Schuck, P.; Resch, K.L. A hospital suited version of the German SF-36 and its psychometric comparison with the original questionnaire. Soz. Praventivmed. 2001, 46, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Suarez-Almazor, M.E.; Kendall, C.; Johnson, J.A.; Skeith, K.; Vincent, D. Use of health status measures in patients with low back pain in clinical settings. Comparison of specific, generic and preference-based instruments. Rheumatology 2000, 39, 783–790. [Google Scholar] [CrossRef]
- Taylor, S.J.; Taylor, A.E.; Foy, M.A.; Fogg, A.J. Responsiveness of common outcome measures for patients with low back pain. Spine 1999, 24, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Serbic, D.; Pincus, T. The relationship between pain, disability, guilt and acceptance in low back pain: A mediation analysis. J. Behav. Med. 2017, 40, 651–658. [Google Scholar] [CrossRef]
- Lindemann, C.; Zippelius, T.; Hochberger, F.; Hölzl, A.; Böhle, S.; Strube, P. Local Infiltrations in Patients with Radiculopathy or Chronic Low Back Pain Due to Segment Degeneration—Only A Diagnostic Value? J. Pers. Med. 2022, 12, 1791. [Google Scholar] [CrossRef]
- McKee-Ryan, F.; Song, Z.; Wanberg, C.R.; Kinicki, A.J. Psychological and physical well-being during unemployment: A meta-analytic study. J. Appl. Psychol. 2005, 90, 53–76. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Mayer, T.G. Psychological evaluation of the spine patient. J. Am. Acad. Orthop. Surg. 2008, 16, 107–112. [Google Scholar] [CrossRef]
- Bair, M.J.; Robinson, R.L.; Katon, W.; Kroenke, K. Depression and pain comorbidity: A literature review. Arch. Intern. Med. 2003, 163, 2433–2445. [Google Scholar] [CrossRef]
- Chou, R.; Shekelle, P. Will this patient develop persistent disabling low back pain? J. Am. Med. Assoc. 2010, 303, 1295–1302. [Google Scholar] [CrossRef] [PubMed]
- Bernard, T.N., Jr. Repeat lumbar spine surgery. Factors influencing outcome. Spine 1993, 18, 2196–2200. [Google Scholar] [CrossRef] [PubMed]
- Ekman, P.; Moller, H.; Hedlund, R. Predictive factors for the outcome of fusion in adult isthmic spondylolisthesis. Spine 2009, 34, 1204–1210. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.C.; McCormick, Z.L.; Mattie, R.; MacVicar, J.; Duszynski, B.; Stojanovic, M.P. The Effectiveness of Lumbar Transforaminal Injection of Steroid for the Treatment of Radicular Pain: A Comprehensive Review of the Published Data. Pain Med. 2020, 21, 472–487. [Google Scholar] [CrossRef]




| PRI | Total | Anxious | Nonanxious | p-Value | Depressed | Nondepressed | p-Value |
|---|---|---|---|---|---|---|---|
| n = 102 (%) | 16 (16%) | 86 (84%) | 45 (44%) | 57 (56%) | |||
| Sex: Male | 45 (44%) | 5 (31%) | 40 (46%) | 0.259 | 15 (33%) | 30 (53%) | 0.051 † |
| Female | 57 (56%) | 11 (69%) | 46 (54%) | 30 (67%) | 27 (47%) | ||
| Age [yrs] (Mean ± SD) | 64.1 ± 11.8 | 62.7 ± 16.1 | 64.3 ± 11.0 | 0.622 | 65.4 ± 12.2 | 63.1 ± 11.5 | 0.326 * |
| BMI [kg/m2] (Mean ± SD) | 28.5 ± 5.0 | 29.5 ± 5.7 | 28.4 ± 4.8 | 0.418 | 29.1 ± 4.8 | 28.1 ± 5.1 | 0.297 * |
| HADS-A-level (Mean ± SD) | 4.3 ± 3.2 | 9.9 ± 1.7 | 3.2 ± 2.2 | <0.001 | – | – | |
| HADS-D-level (Mean ± SD) | 6.8 ± 3.9 | – | – | 10.5 ± 2.0 | 3.8 ± 2.1 | <0.001 * |
| Post-Treatment PRO | Anxious | Nonanxious | Mean | (95% CI) | p-Value | |
|---|---|---|---|---|---|---|
| Estimated Overall Mean (SE) | Difference | |||||
| 1 | NRS-BP | 2.7 (0.4) * | 2.6 (0.1) * | 0.1 | (−0.7, 0.9) | 0.757 |
| 1 | NRS-LP | 3.6 (0.4) * | 3.4 (0.2) * | 0.2 | (−0.6, 1.0) | 0.567 |
| 2 | ODI | 28.9 (3.0) † | 24.8 (1.2) † | 4.1 | (−2.5, 10.7) | 0.221 |
| 3 | SF-36 (pcs) | 37.6 (1.1) | 35.8 (0.5) | 1.8 | (−0.7, 4,2) | 0.155 |
| 3 | SF-36 (mcs) | 48.3 (0.4) | 48.4 (1.0) | 0.1 | (−2.1, 2.3) | 0.928 |
| Post-Treatment PRO | Depressed | Nondepressed | Mean | (95% CI) | p-Value | |
|---|---|---|---|---|---|---|
| Estimated Overall Mean (SE) | Difference | |||||
| 1 | NRS-BP | 2.7 (0.2) * | 2.6 (0.2) * | 0.1 | (−0.5, 0.6) | 0.863 |
| 1 | NRS-LP | 3.7 (0.2) * | 3.2 (0.2) * | 0.5 | (−0.2, 1.1) | 0.150 |
| 2 | ODI | 27.8 (1.9) † | 23.5 (1.6) † | 4.3 | (−1.0, 9.7) | 0.110 |
| 3 | SF-36 (pcs) | 36.1 (0.7) | 36.1 (0.6) | 0 | (−1.9, 1.8) | 0.942 |
| 3 | SF-36 (mcs) | 48.2 (0.6) | 48.4 (0.5) | 0.2 | (−1.8, 1.3) | 0.731 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindemann, C.; Hölzl, A.; Böhle, S.; Zippelius, T.; Strube, P. How Does Anxiety and Depression Affect the Outcome after Periradicular Infiltration Therapy?—A Retrospective Analysis of Patients Undergoing CT-Guided Single-Level Nerve Root Infiltration Due to Chronic Monoradicular Pain. Diagnostics 2023, 13, 2882. https://doi.org/10.3390/diagnostics13182882
Lindemann C, Hölzl A, Böhle S, Zippelius T, Strube P. How Does Anxiety and Depression Affect the Outcome after Periradicular Infiltration Therapy?—A Retrospective Analysis of Patients Undergoing CT-Guided Single-Level Nerve Root Infiltration Due to Chronic Monoradicular Pain. Diagnostics. 2023; 13(18):2882. https://doi.org/10.3390/diagnostics13182882
Chicago/Turabian StyleLindemann, Chris, Alexander Hölzl, Sabrina Böhle, Timo Zippelius, and Patrick Strube. 2023. "How Does Anxiety and Depression Affect the Outcome after Periradicular Infiltration Therapy?—A Retrospective Analysis of Patients Undergoing CT-Guided Single-Level Nerve Root Infiltration Due to Chronic Monoradicular Pain" Diagnostics 13, no. 18: 2882. https://doi.org/10.3390/diagnostics13182882