
EEG Correlates of Cognitive Functions in a Child with ASD and White Matter Signal Abnormalities: A Case Report with Two-and-a-Half-Year Follow-Up


 , , ,
, , ,
Abstract
:1. Introduction
2. Case Presentation
2.1. Case Report
2.2. Study Design
2.3. Data Collection
2.4. Statistical Analysis
2.5. Results
2.5.1. Sensory Profile
2.5.2. ASD Symptoms and Cognitive, Speech–Language, Sensorimotor, and Socio-Emotional Profiles
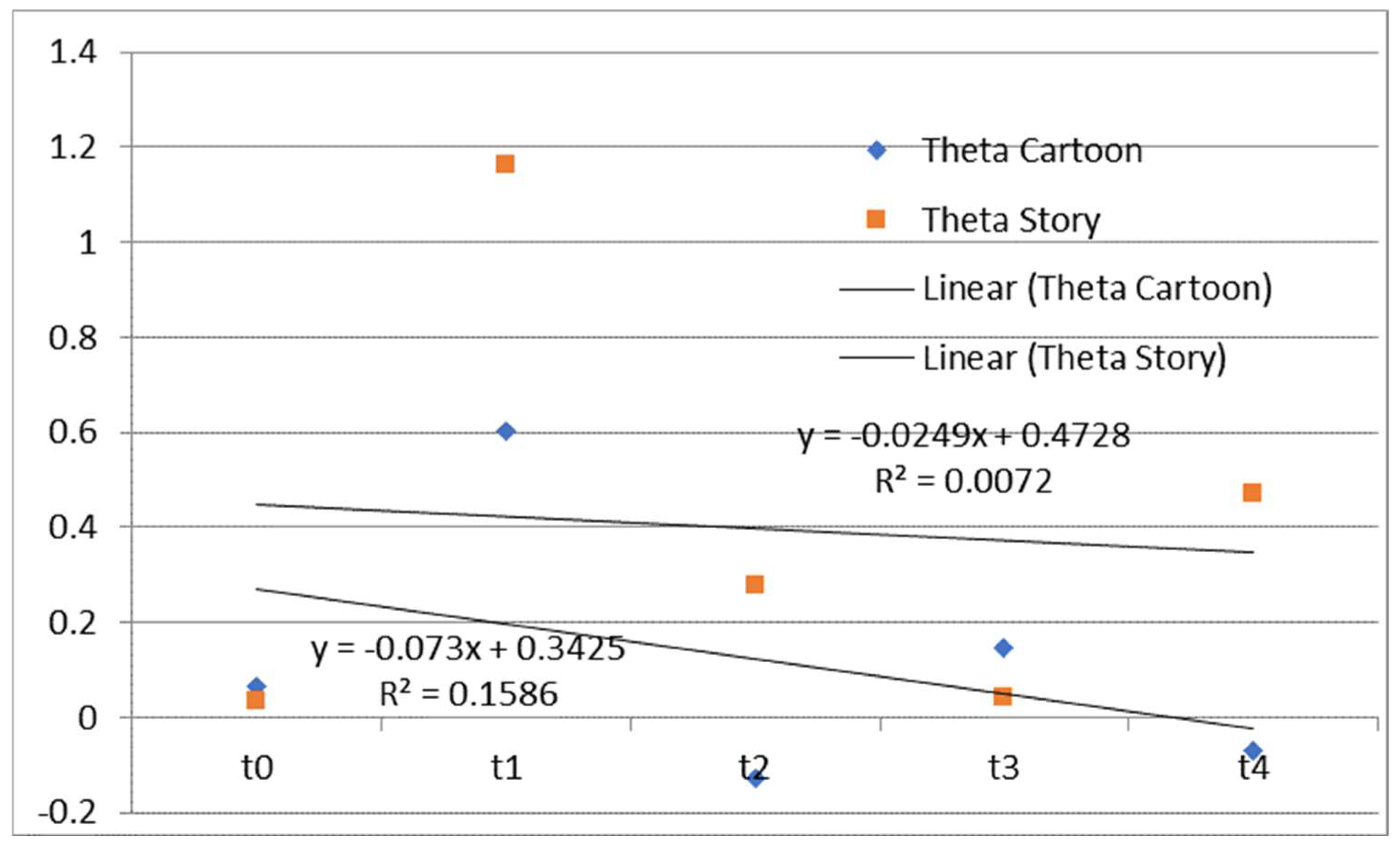
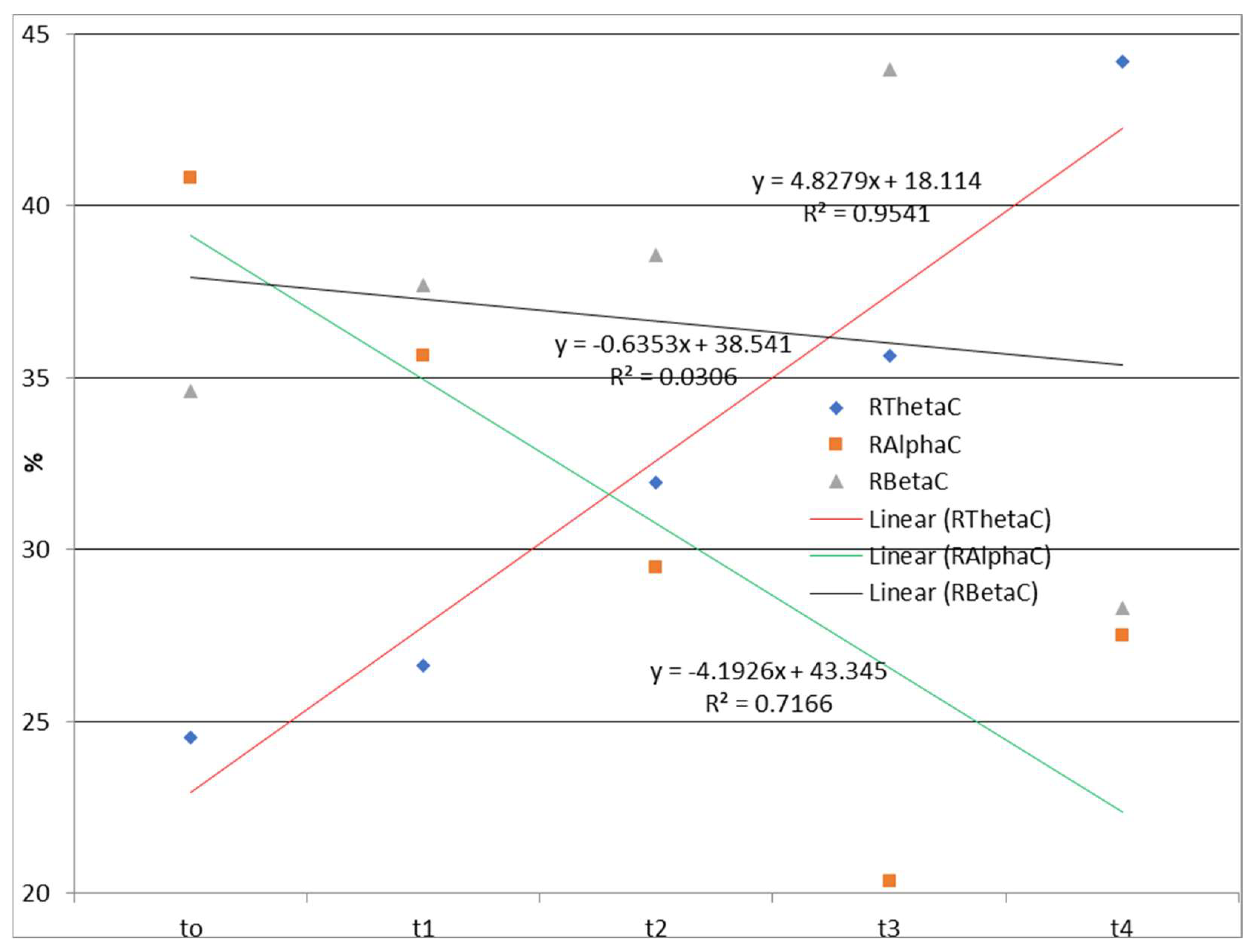
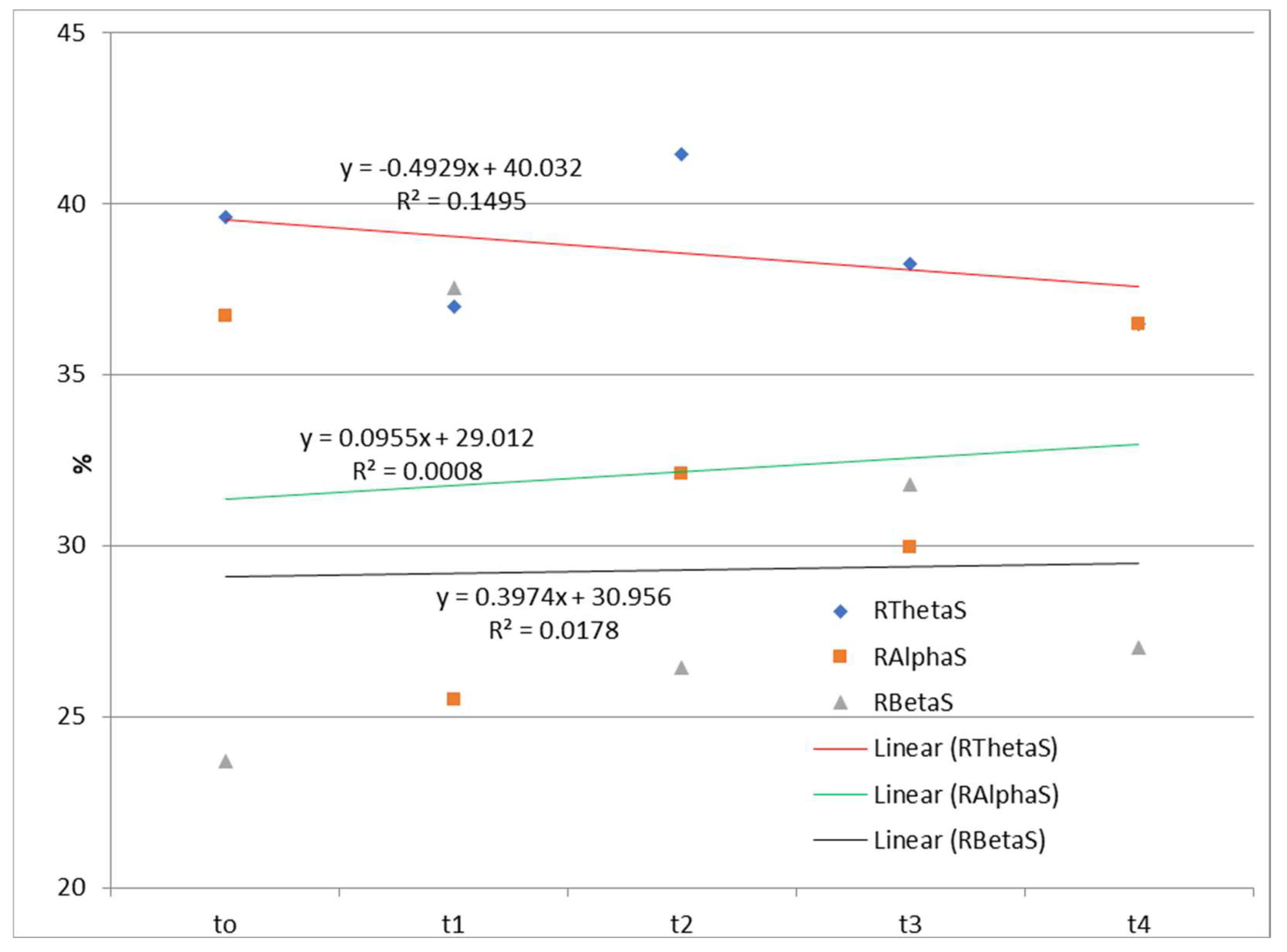
2.5.3. EEG Findings
- N Frequency range—normalized theta, alpha, or beta frequency range;
- Frequency range—theta, alpha, or beta frequency range;
- task—task 2 (listening to a story) or task 3 (watching and listening to a cartoon);
- el—one of the 19 EEG measuring points (Fp1 …Cz);
- Rest—resting state.
- RFrequency range—the relative contribution of the frequency range to the total signal (Rtheta, Ralpha, and Rbeta);
- MFrequency range—the mean normalized spectral power;
- task—task 2 (listening to a story) or task 3 (watching and listening to a cartoon).
2.5.4. Correlations
3. Discussion
3.1. Sensory Profile
3.2. ASD Symptoms and Cognitive, Speech–Language, Sensorimotor, and Socio-Emotional Profiles
3.3. EEG Findings
3.4. Correlations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASD | Autism spectrum disorder |
| WMSAs | White matter signal abnormalities |
| WM | White matter |
| EEG | Electroencephalography |
| FA | Fractional anisotropy |
| ToM | Theory of mind |
| MD | Mean diffusivity |
| DTI | Diffusion tensor imaging |
| ADHD | Attention-deficit hyperactivity disorder |
| CR | Corona radiata |
| DLD | Developmental language disorder |
| fMRI | Functional magnetic resonance imaging |
| CT | Computed tomography |
| PET | Positron emission tomography |
| EEG | Electroencephalography |
| ADOS | Autism Diagnostic Observation Schedule |
| IEPSP | Institute for Experimental Phonetics and Speech Pathology |
| BERA | Brain stem evoked response audiometry |
| MRT | Magnetic resonance tomography |
| KSAFA | Kostic’s selective auditory filter amplifier |
| RTČ-P | Developmental Test Čuturić |
| REVISK | Serbian adaptation of the Wechsler Intelligence Scale for Children—Revised |
| ADOS-2 | Autism Diagnostic Observation Schedule—Second Edition |
| SEPAC | The Scale for Evaluation of Psychophysiological Abilities of Children |
| EOG | Electrooculograms |
| ICA | Independent component analysis |
| FFT | Fast Fourier transform |
| VIQ | Verbal intelligence quotient |
| PIQ | Performance intelligence quotient |
| TIQ | Total intelligence quotient |
| ESLD | Estimated speech–language development |
| ESMD | Estimated sensorimotor development |
| ESED | Estimated socio-emotional development |
References
- Whitehouse, A. Commentary: A spectrum for all? A response to Green et al.(2023), neurodiversity, autism and health care. Child Adolesc. Ment. Health 2023, 28, 443–445. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, M.; Wang, R.; van der Kouwe, A.; Takahashi, E. White and gray matter fiber pathways in autism spectrum disorder revealed by ex vivo diffusion MR tractography. Brain Behav. 2016, 6, e00483. [Google Scholar] [CrossRef] [PubMed]
- Bach, B.; Vestergaard, M. Differential Diagnosis of ICD-11 Personality Disorder and Autism Spectrum Disorder in Adolescents. Children 2023, 10, 992. [Google Scholar] [CrossRef] [PubMed]
- Amaral, D.G. Examining the causes of autism. In Cerebrum: The Dana Forum on Brain Science; Dana Foundation: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Wolff, J.J.; Gu, H.; Gerig, G.; Elison, J.T.; Styner, M.; Gouttard, S.; Botteron, K.N.; Dager, S.R.; Dawson, G.; Estes, A.M. Differences in white matter fiber tract development present from 6 to 24 months in infants with autism. Am. J. Psychiatry 2012, 169, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Schaer, M.; Ottet, M.-C.; Scariati, E.; Dukes, D.; Franchini, M.; Eliez, S.; Glaser, B. Decreased frontal gyrification correlates with altered connectivity in children with autism. Front. Hum. Neurosci. 2013, 7, 750. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-J.; Hyung, B.; Paquola, C.; Bernhardt, B.C. The superficial white matter in autism and its role in connectivity anomalies and symptom severity. Cereb. Cortex 2019, 29, 4415–4425. [Google Scholar] [CrossRef]
- Thapar, A.; Riglin, L. The importance of a developmental perspective in Psychiatry: What do recent genetic-epidemiological findings show? Mol. Psychiatry 2020, 25, 1631–1639. [Google Scholar] [CrossRef]
- Fields, R.D. Neuroscience. Change in the brain’s white matter. Science 2010, 330, 768–769. [Google Scholar] [CrossRef]
- Buyanova, I.S.; Arsalidou, M. Cerebral white matter myelination and relations to age, gender, and cognition: A selective review. Front. Hum. Neurosci. 2021, 15, 662031. [Google Scholar] [CrossRef]
- Fields, R.D. White matter in learning, cognition and psychiatric disorders. Trends Neurosci. 2008, 31, 361–370. [Google Scholar] [CrossRef]
- Pryweller, J.R.; Schauder, K.B.; Anderson, A.W.; Heacock, J.L.; Foss-Feig, J.H.; Newsom, C.R.; Loring, W.A.; Cascio, C.J. White matter correlates of sensory processing in autism spectrum disorders. NeuroImage Clin. 2014, 6, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Koshiyama, D.; Fukunaga, M.; Okada, N.; Morita, K.; Nemoto, K.; Usui, K.; Yamamori, H.; Yasuda, Y.; Fujimoto, M.; Kudo, N. White matter microstructural alterations across four major psychiatric disorders: Mega-analysis study in 2937 individuals. Mol. Psychiatry 2020, 25, 883–895. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, C.C.; Evans, D.W.; Myers, S.M.; Moore, G.J.; Michael, A.M. A comparison of structural brain imaging findings in autism spectrum disorder and attention-deficit hyperactivity disorder. Neuropsychol. Rev. 2016, 26, 25–43. [Google Scholar] [CrossRef] [PubMed]
- Di, X.; Azeez, A.; Li, X.; Haque, E.; Biswal, B.B. Disrupted focal white matter integrity in autism spectrum disorder: A voxel-based meta-analysis of diffusion tensor imaging studies. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2018, 82, 242–248. [Google Scholar] [CrossRef]
- Zhao, Y.; Yang, L.; Gong, G.; Cao, Q.; Liu, J. Identify aberrant white matter microstructure in ASD, ADHD and other neurodevelopmental disorders: A meta-analysis of diffusion tensor imaging studies. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2022, 113, 110477. [Google Scholar] [CrossRef]
- Shukla, D.K.; Keehn, B.; Müller, R.A. Tract-specific analyses of diffusion tensor imaging show widespread white matter compromise in autism spectrum disorder. J. Child Psychol. Psychiatry 2011, 52, 286–295. [Google Scholar] [CrossRef]
- Ameis, S.H.; Lerch, J.P.; Taylor, M.J.; Lee, W.; Viviano, J.D.; Pipitone, J.; Nazeri, A.; Croarkin, P.E.; Voineskos, A.N.; Lai, M.-C. A diffusion tensor imaging study in children with ADHD, autism spectrum disorder, OCD, and matched controls: Distinct and non-distinct white matter disruption and dimensional brain-behavior relationships. Am. J. Psychiatry 2016, 173, 1213–1222. [Google Scholar] [CrossRef]
- Wang, Y.; Olson, I.R. The original social network: White matter and social cognition. Trends Cogn. Sci. 2018, 22, 504–516. [Google Scholar] [CrossRef]
- Basser, P.J. Inferring microstructural features and the physiological state of tissues from diffusion-weighted images. NMR Biomed. 1995, 8, 333–344. [Google Scholar] [CrossRef]
- Werring, D.; Brassat, D.; Droogan, A.; Clark, C.; Symms, M.; Barker, G.; MacManus, D.; Thompson, A.; Miller, D. The pathogenesis of lesions and normal-appearing white matter changes in multiple sclerosis: A serial diffusion MRI study. Brain 2000, 123, 1667–1676. [Google Scholar] [CrossRef]
- Ewing-Cobbs, L.; Hasan, K.; Prasad, M.; Kramer, L.; Bachevalier, J. Corpus callosum diffusion anisotropy correlates with neuropsychological outcomes in twins disconcordant for traumatic brain injury. Am. J. Neuroradiol. 2006, 27, 879–881. [Google Scholar] [CrossRef] [PubMed]
- Frazier, T.W.; Hardan, A.Y. A meta-analysis of the corpus callosum in autism. Biol. Psychiatry 2009, 66, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Qiu, T.; Ke, X.; Xiao, X.; Xiao, T.; Liang, F.; Zou, B.; Huang, H.; Fang, H.; Chu, K. Autism spectrum disorder as early neurodevelopmental disorder: Evidence from the brain imaging abnormalities in 2–3 years old toddlers. J. Autism Dev. Disord. 2014, 44, 1633–1640. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.K. Developmental malformation of the corpus callosum: A review of typical callosal development and examples of developmental disorders with callosal involvement. J. Neurodev. Disord. 2011, 3, 3–27. [Google Scholar] [CrossRef] [PubMed]
- Righi, G.; Tierney, A.L.; Tager-Flusberg, H.; Nelson, C.A. Functional connectivity in the first year of life in infants at risk for autism spectrum disorder: An EEG study. PLoS ONE 2014, 9, e105176. [Google Scholar] [CrossRef]
- Karalunas, S.L.; Nigg, J.T. Heterogeneity and subtyping in attention-deficit/hyperactivity disorder—Considerations for emerging research using person-centered computational approaches. Biol. Psychiatry 2020, 88, 103–110. [Google Scholar] [CrossRef]
- Aduen, P.A.; Day, T.N.; Kofler, M.J.; Harmon, S.L.; Wells, E.L.; Sarver, D.E. Social problems in ADHD: Is it a skills acquisition or performance problem? J. Psychopathol. Behav. Assess. 2018, 40, 440–451. [Google Scholar] [CrossRef]
- Soriano-Mas, C.; Pujol, J.; Ortiz, H.; Deus, J.; López-Sala, A.; Sans, A. Age-related brain structural alterations in children with specific language impairment. Hum. Brain Mapp. 2009, 30, 1626–1636. [Google Scholar] [CrossRef]
- Krishnan, S.; Cler, G.J.; Smith, H.J.; Willis, H.E.; Asaridou, S.S.; Healy, M.P.; Papp, D.; Watkins, K.E. Quantitative MRI reveals differences in striatal myelin in children with DLD. eLife 2022, 11, e74242. [Google Scholar] [CrossRef]
- Jäncke, L.; Siegenthaler, T.; Preis, S.; Steinmetz, H. Decreased white-matter density in a left-sided fronto-temporal network in children with developmental language disorder: Evidence for anatomical anomalies in a motor-language network. Brain Lang. 2007, 102, 91–98. [Google Scholar] [CrossRef]
- Bathelt, J.; Scerif, G.; Nobre, A.; Astle, D. Whole-brain white matter organization, intelligence, and educational attainment. Trends Neurosci. Educ. 2019, 15, 38–47. [Google Scholar] [CrossRef]
- Clayden, J.D.; Jentschke, S.; Munoz, M.; Cooper, J.M.; Chadwick, M.J.; Banks, T.; Clark, C.A.; Vargha-Khadem, F. Normative development of white matter tracts: Similarities and differences in relation to age, gender, and intelligence. Cereb. Cortex 2012, 22, 1738–1747. [Google Scholar] [CrossRef]
- Mazoyer, B.; Crivello, F.; Joliot, M.; Mazoyer, B. Biological underpinnings of anatomic consistency and variability in the human brain. In Handbook of Medical Imaging: Processing and Analysis Management; Academic Press: Cambridge, MA, USA, 2000; p. 449. [Google Scholar] [CrossRef]
- Erol, A.; Hunyadi, B. Tensors for neuroimaging: A review on applications of tensors to unravel the mysteries of the brain. In Tensors for Data Processing; Academic Press: Cambridge, MA, USA, 2022; pp. 427–482. [Google Scholar] [CrossRef]
- Chatterjee, D.; Gavas, R.; Samanta, R.; Saha, S.K. Electroencephalogram-based cognitive performance evaluation for mental arithmetic task. In Cognitive Computing for Human-Robot Interaction; Elsevier: Amsterdam, The Netherlands, 2021; pp. 85–101. [Google Scholar] [CrossRef]
- Nunez, P.L.; Srinivasan, R.; Fields, R.D. EEG functional connectivity, axon delays and white matter disease. Clin. Neurophysiol. 2015, 126, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Biasiucci, A.; Franceschiello, B.; Murray, M.M. Electroencephalography. Curr. Biol. 2019, 29, R80–R85. [Google Scholar] [CrossRef] [PubMed]
- Lushchekina, E.; Podreznaya, E.; Lushchekin, V.; Strelets, V. A comparative EEG study in normal and autistic children. Neurosci. Behav. Physiol. 2012, 42, 236–243. [Google Scholar] [CrossRef]
- Dawson, G.; Klinger, L.G.; Panagiotides, H.; Lewy, A.; Castelloe, P. Subgroups of autistic children based on social behavior display distinct patterns of brain activity. J. Abnorm. Child Psychol. 1995, 23, 569–583. [Google Scholar] [CrossRef] [PubMed]
- Orekhova, E.; Stroganova, T.; Nygren, G.; Tsetlin, M.; Posikera, I.; Gillberg, C.; Elam, M. Excess of high frequency electroencephalogram oscillations in boys with autism. Biol. Psychiatry 2007, 62, 1022–1029. [Google Scholar] [CrossRef] [PubMed]
- Daoust, A.-M.; Limoges, É.; Bolduc, C.; Mottron, L.; Godbout, R. EEG spectral analysis of wakefulness and REM sleep in high functioning autistic spectrum disorders. Clin. Neurophysiol. 2004, 115, 1368–1373. [Google Scholar] [CrossRef] [PubMed]
- Elhabashy, H.; Raafat, O.; Afifi, L.; Raafat, H.; Abdullah, K. Quantitative EEG in autistic children. Egypt. J. Neurol. Psychiatry Neurosurg. 2015, 52, 176. [Google Scholar]
- Coben, R.; Clarke, A.R.; Hudspeth, W.; Barry, R.J. EEG power and coherence in autistic spectrum disorder. Clin. Neurophysiol. 2008, 119, 1002–1009. [Google Scholar] [CrossRef]
- Van Diessen, E.; Senders, J.; Jansen, F.E.; Boersma, M.; Bruining, H. Increased power of resting-state gamma oscillations in autism spectrum disorder detected by routine electroencephalography. Eur. Arch. Psychiatry Clin. Neurosci. 2015, 265, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Murias, M.; Webb, S.J.; Greenson, J.; Dawson, G. Resting state cortical connectivity reflected in EEG coherence in individuals with autism. Biol. Psychiatry 2007, 62, 270–273. [Google Scholar] [CrossRef]
- Wang, J.; Barstein, J.; Ethridge, L.E.; Mosconi, M.W.; Takarae, Y.; Sweeney, J.A. Resting state EEG abnormalities in autism spectrum disorders. J. Neurodev. Disord. 2013, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.M.; Taquet, M.; Vega, C.; Jeste, S.S.; Fernández, I.S.; Tan, J.; Nelson, C.A.; Sahin, M.; Warfield, S.K. Brain functional networks in syndromic and non-syndromic autism: A graph theoretical study of EEG connectivity. BMC Med. 2013, 11, 54. [Google Scholar] [CrossRef]
- Mak-Fan, K.M.; Morris, D.; Vidal, J.; Anagnostou, E.; Roberts, W.; Taylor, M.J. White matter and development in children with an autism spectrum disorder. Autism 2013, 17, 541–557. [Google Scholar] [CrossRef] [PubMed]
- Yuk, V.; Dunkley, B.T.; Anagnostou, E.; Taylor, M.J. Alpha connectivity and inhibitory control in adults with autism spectrum disorder. Mol. Autism 2020, 11, 95. [Google Scholar] [CrossRef]
- Jaime, M.; McMahon, C.M.; Davidson, B.C.; Newell, L.C.; Mundy, P.C.; Henderson, H.A. Brief report: Reduced temporal-central EEG alpha coherence during joint attention perception in adolescents with autism spectrum disorder. J. Autism Dev. Disord. 2016, 46, 1477–1489. [Google Scholar] [CrossRef]
- Maksimović, S.; Jeličić, L.; Marisavljević, M.; Fatić, S.; Gavrilović, A.; Subotić, M. Can EEG Correlates Predict Treatment Efficacy in Children with Overlapping ASD and SLI Symptoms: A Case Report. Diagnostics 2022, 12, 1110. [Google Scholar] [CrossRef] [PubMed]
- Maksimović, S.; Stanojević, N.; Fatić, S.; Punišić, S.; Adamović, T.; Petrović, N.; Nenadović, V. Multidisciplinary speech and language therapy approach in a child with multiple disabilities including blindness due to retinopathy of prematurity: A case study with a one year follow-up. Logop. Phoniatr. Vocol. 2021, 48, 98–110. [Google Scholar] [CrossRef]
- Dunn, W. Child Sensory Profile–2 User’s Manual; Pearson: Bloomington, MN, USA, 2014. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism diagnostic observation schedule: ADOS-2. West Psychol. J. Psychoeduc. Assess. 2012, 32, 88–92. [Google Scholar]
- Čuturić, N. Ljestvica Psihičkog Razvoja Rane Dječje Dobi Brunet-Lezine: Priručnik; Zavod za Produktivnost Dela SR Slovenije: Ljubljana, Slovenija, 1973. [Google Scholar]
- Biro, M. Priručnik za REVISK (II Revidirano i Dopunjeno Izdanje); Društvo Psihologa Srbije: Beograd, Serbia, 1998. [Google Scholar]
- Bogavac, I.; Jeličić, L.; Nenadović, V.; Subotić, M.; Janjić, V. The speech and language profile of a child with turner syndrome—A case study. Clin. Linguist. Phon. 2021, 36, 565–578. [Google Scholar] [CrossRef] [PubMed]
- Jeličić, L.; Sovilj, M.; Bogavac, I.; Drobnjak, A.e.; Gouni, O.; Kazmierczak, M.; Subotić, M. The Impact of Maternal Anxiety on Early Child Development During the COVID-19 Pandemic. Front. Psychol. 2021, 12, 792053. [Google Scholar] [CrossRef]
- Rakonjac, M.; Cuturilo, G.; Stevanovic, M.; Jelicic, L.; Subotic, M.; Jovanovic, I.; Drakulic, D. Differences in speech and language abilities between children with 22q11. 2 deletion syndrome and children with phenotypic features of 22q11. 2 deletion syndrome but without microdeletion. Res. Dev. Disabil. 2016, 55, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Shlens, J. A tutorial on independent component analysis. arXiv 2014, arXiv:1404.2986. [Google Scholar]
- Pfeiffer, B.; Clark, G.F.; Arbesman, M. Effectiveness of cognitive and occupation-based interventions for children with challenges in sensory processing and integration: A systematic review. Am. J. Occup. Ther. 2018, 72, 7201190020p1–7201190020p9. [Google Scholar] [CrossRef]
- Camarata, S.; Miller, L.J.; Wallace, M.T. Evaluating sensory integration/sensory processing treatment: Issues and analysis. Front. Integr. Neurosci. 2020, 14, 55. [Google Scholar] [CrossRef]
- Kashefimehr, B.; Kayihan, H.; Huri, M. The effect of sensory integration therapy on occupational performance in children with autism. OTJR: Occup. Particip. Health 2018, 38, 75–83. [Google Scholar] [CrossRef]
- May-Benson, T.A.; Koomar, J.A. Systematic review of the research evidence examining the effectiveness of interventions using a sensory integrative approach for children. Am. J. Occup. Ther. 2010, 64, 403–414. [Google Scholar] [CrossRef]
- Liu, T.; ElGarhy, S. Psychomotor training program as a treatment intervention for children with autism spectrum disorder. In Physical Education Research: Role of School Programs, Children’s Attitudes and Health Implications; Nova Publishers: New York, NY, USA, 2014; pp. 73–89. [Google Scholar]
- De Barros, I.M.; Coutinho, D.J.G. The contribution of psychomotricity in the development of autistic children: A literature review. Rev. Ibero Am. Humanid. Ciênc. Educ. 2023, 9, 230–242. [Google Scholar]
- Swanson, M.R.; Hazlett, H.C. White matter as a monitoring biomarker for neurodevelopmental disorder intervention studies. J. Neurodev. Disord. 2019, 11, 33. [Google Scholar] [CrossRef]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1. [Google Scholar] [CrossRef]
- Van Naarden Braun, K.; Christensen, D.; Doernberg, N.; Schieve, L.; Rice, C.; Wiggins, L.; Schendel, D.; Yeargin-Allsopp, M. Trends in the prevalence of autism spectrum disorder, cerebral palsy, hearing loss, intellectual disability, and vision impairment, metropolitan Atlanta, 1991–2010. PLoS ONE 2015, 10, e0124120. [Google Scholar] [CrossRef] [PubMed]
- Charman, T.; Pickles, A.; Simonoff, E.; Chandler, S.; Loucas, T.; Baird, G. IQ in children with autism spectrum disorders: Data from the Special Needs and Autism Project (SNAP). Psychol. Med. 2011, 41, 619–627. [Google Scholar] [CrossRef]
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018. MMWR Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Girault, J.B.; Cornea, E.; Goldman, B.D.; Knickmeyer, R.C.; Styner, M.; Gilmore, J.H. White matter microstructural development and cognitive ability in the first 2 years of life. Hum. Brain Mapp. 2019, 40, 1195–1210. [Google Scholar] [CrossRef] [PubMed]
- O’Muircheartaigh, J.; Dean III, D.C.; Ginestet, C.E.; Walker, L.; Waskiewicz, N.; Lehman, K.; Dirks, H.; Piryatinsky, I.; Deoni, S.C. White matter development and early cognition in babies and toddlers. Hum. Brain Mapp. 2014, 35, 4475–4487. [Google Scholar] [CrossRef]
- Swanson, M.R.; Wolff, J.J.; Elison, J.T.; Gu, H.; Hazlett, H.C.; Botteron, K.; Styner, M.; Paterson, S.; Gerig, G.; Constantino, J. Splenium development and early spoken language in human infants. Dev. Sci. 2017, 20, e12360. [Google Scholar] [CrossRef]
- Deoni, S.C.; O’Muircheartaigh, J.; Elison, J.T.; Walker, L.; Doernberg, E.; Waskiewicz, N.; Dirks, H.; Piryatinsky, I.; Dean, D.C.; Jumbe, N. White matter maturation profiles through early childhood predict general cognitive ability. Brain Struct. Funct. 2016, 221, 1189–1203. [Google Scholar] [CrossRef]
- Hofstetter, S.; Friedmann, N.; Assaf, Y. Rapid language-related plasticity: Microstructural changes in the cortex after a short session of new word learning. Brain Struct. Funct. 2017, 222, 1231–1241. [Google Scholar] [CrossRef]
- Schlaug, G.; Marchina, S.; Norton, A. Evidence for plasticity in white-matter tracts of patients with chronic Broca’s aphasia undergoing intense intonation-based speech therapy. Ann. N. Y. Acad. Sci. 2009, 1169, 385–394. [Google Scholar] [CrossRef]
- Scholz, J.; Klein, M.C.; Behrens, T.E.; Johansen-Berg, H. Training induces changes in white-matter architecture. Nat. Neurosci. 2009, 12, 1370–1371. [Google Scholar] [CrossRef]
- Subramaniam, K.; Gill, J.; Fisher, M.; Mukherjee, P.; Nagarajan, S.; Vinogradov, S. White matter microstructure predicts cognitive training-induced improvements in attention and executive functioning in schizophrenia. Schizophr. Res. 2018, 193, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Tymofiyeva, O.; Gaschler, R. Training-induced neural plasticity in youth: A systematic review of structural and functional MRI studies. Front. Hum. Neurosci. 2021, 14, 497245. [Google Scholar] [CrossRef] [PubMed]
- Weyandt, L.L.; Clarkin, C.M.; Holding, E.Z.; May, S.E.; Marraccini, M.E.; Gudmundsdottir, B.G.; Shepard, E.; Thompson, L. Neuroplasticity in Children and Adolescents in Response to Treatment Intervention: A Systematic Review of the Literature. Clin. Transl. Neurosci. 2020, 4, 21. [Google Scholar] [CrossRef]
- Hoekzema, E.; Carmona, S.; Ramos-Quiroga, J.A.; Barba, E.; Bielsa, A.; Tremols, V.; Rovira, M.; Soliva, J.C.; Casas, M.; Bulbena, A. Training-induced neuroanatomical plasticity in ADHD: A tensor-based morphometric study. Hum. Brain Mapp. 2011, 32, 1741–1749. [Google Scholar] [CrossRef]
- Iuculano, T.; Rosenberg-Lee, M.; Richardson, J.; Tenison, C.; Fuchs, L.; Supekar, K.; Menon, V. Cognitive tutoring induces widespread neuroplasticity and remediates brain function in children with mathematical learning disabilities. Nat. Commun. 2015, 6, 8453. [Google Scholar] [CrossRef]
- Maximo, J.O.; Murdaugh, D.L.; O’Kelley, S.; Kana, R.K. Changes in intrinsic local connectivity after reading intervention in children with autism. Brain Lang. 2017, 175, 11–17. [Google Scholar] [CrossRef]
- Saaybi, S.; AlArab, N.; Hannoun, S.; Saade, M.; Tutunji, R.; Zeeni, C.; Shbarou, R.; Hourani, R.; Boustany, R.-M. Pre-and post-therapy assessment of clinical outcomes and white matter integrity in autism spectrum disorder: Pilot study. Front. Neurol. 2019, 10, 877. [Google Scholar] [CrossRef]
- Andrews, D.S.; Lee, J.K.; Harvey, D.J.; Waizbard-Bartov, E.; Solomon, M.; Rogers, S.J.; Nordahl, C.W.; Amaral, D.G. A longitudinal study of white matter development in relation to changes in autism severity across early childhood. Biol. Psychiatry 2021, 89, 424–432. [Google Scholar] [CrossRef]
- Waizbard-Bartov, E.; Ferrer, E.; Young, G.S.; Heath, B.; Rogers, S.; Wu Nordahl, C.; Solomon, M.; Amaral, D.G. Trajectories of autism symptom severity change during early childhood. J. Autism Dev. Disord. 2021, 51, 227–242. [Google Scholar] [CrossRef]
- Haesen, B.; Boets, B.; Wagemans, J. A review of behavioural and electrophysiological studies on auditory processing and speech perception in autism spectrum disorders. Res. Autism Spectr. Disord. 2011, 5, 701–714. [Google Scholar] [CrossRef]
- Holland, S.K.; Vannest, J.; Mecoli, M.; Jacola, L.M.; Tillema, J.-M.; Karunanayaka, P.R.; Schmithorst, V.J.; Yuan, W.; Plante, E.; Byars, A.W. Functional MRI of language lateralization during development in children. Int. J. Audiol. 2007, 46, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Olulade, O.A.; Seydell-Greenwald, A.; Chambers, C.E.; Turkeltaub, P.E.; Dromerick, A.W.; Berl, M.M.; Gaillard, W.D.; Newport, E.L. The neural basis of language development: Changes in lateralization over age. Proc. Natl. Acad. Sci. USA 2020, 117, 23477–23483. [Google Scholar] [CrossRef] [PubMed]
- Groen, W.B.; Zwiers, M.P.; van der Gaag, R.-J.; Buitelaar, J.K. The phenotype and neural correlates of language in autism: An integrative review. Neurosci. Biobehav. Rev. 2008, 32, 1416–1425. [Google Scholar] [CrossRef]
- Jolliffe, T.; Baron-Cohen, S. Linguistic processing in high-functioning adults with autism or Asperger’s syndrome. Is global coherence impaired? Psychol. Med. 2000, 30, 1169–1187. [Google Scholar] [CrossRef]
- Baird, G.; Norbury, C.F. Social (pragmatic) communication disorders and autism spectrum disorder. Arch. Dis. Child. 2016, 101, 745–751. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, C.; Lewis, J.D.; Elsabbagh, M. Is functional brain connectivity atypical in autism? A systematic review of EEG and MEG studies. PLoS ONE 2017, 12, e0175870. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.; Da Fonseca, D.; Esteves, F.; Deruelle, C. Motivational approach and avoidance in autism spectrum disorder: A comparison between real photographs and cartoons. Res. Autism Spectr. Disord. 2015, 17, 13–24. [Google Scholar] [CrossRef]
- Rosset, D.B.; Rondan, C.; Da Fonseca, D.; Santos, A.; Assouline, B.; Deruelle, C. Typical emotion processing for cartoon but not for real faces in children with autistic spectrum disorders. J. Autism Dev. Disord. 2008, 38, 919–925. [Google Scholar] [CrossRef]
- Grelotti, D.J.; Klin, A.J.; Gauthier, I.; Skudlarski, P.; Cohen, D.J.; Gore, J.C.; Volkmar, F.R.; Schultz, R.T. fMRI activation of the fusiform gyrus and amygdala to cartoon characters but not to faces in a boy with autism. Neuropsychologia 2005, 43, 373–385. [Google Scholar] [CrossRef]
- Ressler, K.J. Amygdala activity, fear, and anxiety: Modulation by stress. Biol. Psychiatry 2010, 67, 1117–1119. [Google Scholar] [CrossRef] [PubMed]
- Čeponienė, R.; Lepistö, T.; Shestakova, A.; Vanhala, R.; Alku, P.; Näätänen, R.; Yaguchi, K. Speech–sound-selective auditory impairment in children with autism: They can perceive but do not attend. Proc. Natl. Acad. Sci. USA 2003, 100, 5567–5572. [Google Scholar] [CrossRef] [PubMed]
- Dunn, M.A.; Gomes, H.; Gravel, J. Mismatch negativity in children with autism and typical development. J. Autism Dev. Disord. 2008, 38, 52–71. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.S.; Sharp, J. Fascination and isolation: A grounded theory exploration of unusual sensory experiences in adults with Asperger syndrome. J. Autism Dev. Disord. 2013, 43, 891–910. [Google Scholar] [CrossRef]
- Quandt, F.; Fischer, F.; Schröder, J.; Heinze, M.; Lettow, I.; Frey, B.M.; Kessner, S.S.; Schulz, M.; Higgen, F.L.; Cheng, B. Higher white matter hyperintensity lesion load is associated with reduced long-range functional connectivity. Brain Commun. 2020, 2, fcaa111. [Google Scholar] [CrossRef]
- Chan, A.S.; Han, Y.M.; Sze, S.L.; Cheung, M.-C.; Leung, W.W.-M.; Chan, R.C.; To, C.Y. Disordered connectivity associated with memory deficits in children with autism spectrum disorders. Res. Autism Spectr. Disord. 2011, 5, 237–245. [Google Scholar] [CrossRef]
- Sperdin, H.F.; Coito, A.; Kojovic, N.; Rihs, T.A.; Jan, R.K.; Franchini, M.; Plomp, G.; Vulliemoz, S.; Eliez, S.; Michel, C.M. Early alterations of social brain networks in young children with autism. eLife 2018, 7, e31670. [Google Scholar] [CrossRef]
- Huberty, S.; Carter Leno, V.; van Noordt, S.J.; Bedford, R.; Pickles, A.; Desjardins, J.A.; Webb, S.J.; Team, B.; Elsabbagh, M. Association between spectral electroencephalography power and autism risk and diagnosis in early development. Autism Res. 2021, 14, 1390–1403. [Google Scholar] [CrossRef]
- Lefebvre, A.; Delorme, R.; Delanoë, C.; Amsellem, F.; Beggiato, A.; Germanaud, D.; Bourgeron, T.; Toro, R.; Dumas, G. Alpha waves as a neuromarker of autism spectrum disorder: The challenge of reproducibility and heterogeneity. Front. Neurosci. 2018, 12, 662. [Google Scholar] [CrossRef]
- Shephard, E.; Tye, C.; Ashwood, K.L.; Azadi, B.; Asherson, P.; Bolton, P.F.; McLoughlin, G. Resting-state neurophysiological activity patterns in young people with ASD, ADHD, and ASD+ ADHD. J. Autism Dev. Disord. 2018, 48, 110–122. [Google Scholar] [CrossRef]
- Dickinson, A.; DiStefano, C.; Senturk, D.; Jeste, S.S. Peak alpha frequency is a neural marker of cognitive function across the autism spectrum. Eur. J. Neurosci. 2018, 47, 643–651. [Google Scholar] [CrossRef]
- Jan, R.K.; Rihs, T.A.; Kojovic, N.; Sperdin, H.F.; Franchini, M.; Custo, A.; Tomescu, M.I.; Michel, C.M.; Schaer, M. Neural processing of dynamic animated social interactions in young children with autism spectrum disorder: A high-density electroencephalography study. Front. Psychiatry 2019, 10, 582. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, R.A.; Segers, M.; Ferber, S.; Barense, M.D.; Camarata, S.; Wallace, M.T. Keeping time in the brain: Autism spectrum disorder and audiovisual temporal processing. Autism Res. 2016, 9, 720–738. [Google Scholar] [CrossRef] [PubMed]
- Bolton, T.A.; Jochaut, D.; Giraud, A.L.; Van De Ville, D. Brain dynamics in ASD during movie-watching show idiosyncratic functional integration and segregation. Hum. Brain Mapp. 2018, 39, 2391–2404. [Google Scholar] [CrossRef] [PubMed]
- Rehman, A.; Al Khalili, Y. Neuroanatomy, Occipital Lobe; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Karunanayaka, P.R.; Holland, S.K.; Schmithorst, V.J.; Solodkin, A.; Chen, E.E.; Szaflarski, J.P.; Plante, E. Age-related connectivity changes in fMRI data from children listening to stories. Neuroimage 2007, 34, 349–360. [Google Scholar] [CrossRef]
- Jochaut, D.; Lehongre, K.; Saitovitch, A.; Devauchelle, A.-D.; Olasagasti, I.; Chabane, N.; Zilbovicius, M.; Giraud, A.-L. Atypical coordination of cortical oscillations in response to speech in autism. Front. Hum. Neurosci. 2015, 9, 171. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sensory Profile | Time and Age (in Months) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| t0 | t1 | t2 | t3 | t4 | |||||||
| 38 | 44 | 54 | 60 | 66 | |||||||
| Score | SD | Score | SD | Score | SD | Score | SD | Score | SD | ||
| Quadrants | Seeking | 53 | +1 | 50 | +1 | 39 | 36 | 32 | |||
| Avoiding | 40 | 40 | 38 | 31 | 24 | ||||||
| Sensitivity | 68 | +2 | 65 | +2 | 61 | +2 | 47 | +1 | 35 | ||
| Registration | 66 | +2 | 65 | +2 | 57 | +2 | 50 | +1 | 42 | ||
| Sensory section | Auditory | 15 | 14 | 14 | 13 | 11 | |||||
| Visual | 5 | −1 | 5 | −1 | 5 | −1 | 7 | −1 | 9 | ||
| Tactile | 42 | +2 | 42 | +2 | 38 | +2 | 34 | +2 | 23 | +1 | |
| Body position | 23 | +2 | 23 | +2 | 21 | +2 | 17 | +1 | 12 | ||
| Movement | 38 | +2 | 38 | +2 | 24 | +2 | 18 | +1 | 17 | +1 | |
| Oral | 38 | +2 | 32 | +1 | 23 | 16 | 10 | ||||
| Behavioral section | Conduct | 15 | 15 | 13 | 11 | 8 | −1 | ||||
| Social-Emotional | 30 | 30 | 30 | 24 | 20 | ||||||
| Attentional | 40 | +2 | 40 | +2 | 40 | +2 | 32 | +2 | 27 | +1 | |
| Assessment Points | Data | ||||
|---|---|---|---|---|---|
| t0 | t1 | t2 | t3 | t4 | |
| Age (in Months) | 38 | 44 | 54 | 60 | 66 |
| Sensory profile 2 (Number of standard deviations) | 16 | 15 | 13 | 9 | 4 |
| Cognitive assessment (TIQ) Age in months | 70 | 68 | 66 | 63 | 59 |
| SEPAC- Estimated speech–language development (ESLD) Age in months | 7 | 14 | 20 | 20 | 27 |
| SEPAC- estimated sensorimotor development (ESMD) Age in months | 12 | 23 | 26 | 27 | 33 |
| SEPAC- estimated socio-emotional development (ESED) Age in months | 10 | 11 | 36 | 36 | 42 |
| ADOS score | 32 | 32 | 31 | 29 | 29 |
| EEG Theta/Alpha Frequency Range | Sensory Profile | TIQ | ESLD | ESMD | ESED | ADOS | |
|---|---|---|---|---|---|---|---|
| RThetaC | Pearson Correlation | −0.990 | −0.994 | 0.944 | 0.889 | 0.896 | −0.913 |
| Sig. (2-tailed) | 0.001 | 0.001 | 0.016 | 0.044 | 0.040 | 0.030 | |
| RAlphaC | Pearson Correlation | 0.890 | |||||
| Sig. (2-tailed) | 0.043 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ćirović, M.; Jeličić, L.; Maksimović, S.; Fatić, S.; Marisavljević, M.; Bošković Matić, T.; Subotić, M. EEG Correlates of Cognitive Functions in a Child with ASD and White Matter Signal Abnormalities: A Case Report with Two-and-a-Half-Year Follow-Up. Diagnostics 2023, 13, 2878. https://doi.org/10.3390/diagnostics13182878
Ćirović M, Jeličić L, Maksimović S, Fatić S, Marisavljević M, Bošković Matić T, Subotić M. EEG Correlates of Cognitive Functions in a Child with ASD and White Matter Signal Abnormalities: A Case Report with Two-and-a-Half-Year Follow-Up. Diagnostics. 2023; 13(18):2878. https://doi.org/10.3390/diagnostics13182878
Chicago/Turabian StyleĆirović, Milica, Ljiljana Jeličić, Slavica Maksimović, Saška Fatić, Maša Marisavljević, Tatjana Bošković Matić, and Miško Subotić. 2023. "EEG Correlates of Cognitive Functions in a Child with ASD and White Matter Signal Abnormalities: A Case Report with Two-and-a-Half-Year Follow-Up" Diagnostics 13, no. 18: 2878. https://doi.org/10.3390/diagnostics13182878