
Headache Attributed to Reversible Cerebral Vasoconstriction Syndrome (RCVS)
 , ,
, ,
Abstract
:1. Introduction
- 1
- The appearance of the headaches themselves led to the diagnosis of RCVS and/or;
- 2
- Headaches possess at least one of the following characteristics:
- (i)
- Thunderclap onset;
- (ii)
- They are triggered by sexual activity, exertion, Valsalva maneuvers, emotion, and bathing/showering;
- (iii)
- They are present or recurrent for at most one month after onset and then subside.
2. Materials and Methods
3. Results
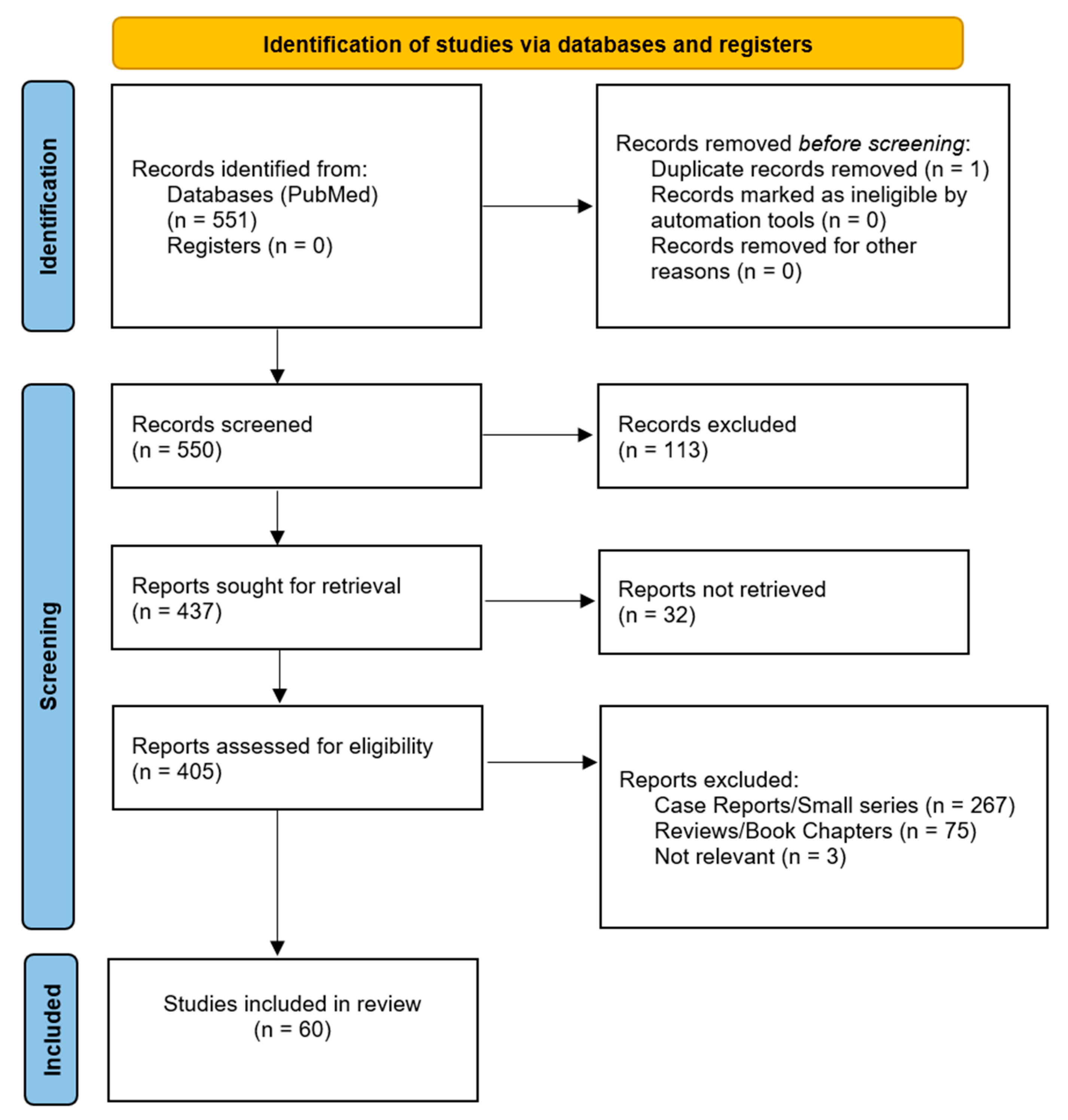
3.1. Results of the Literature Search
3.2. Headache Associated with RCVS
3.2.1. Typical Thunderclap Headache and Thunderclap-like Headache
3.2.2. Presentation with Atypical Headache or No Headache
3.2.3. Accompanying Symptoms of Headaches
3.2.4. Persistent Baseline Headaches
3.2.5. Trigger Factors
3.2.6. Persistent HaRCVS and Recurrency
3.2.7. Focal Neurologic Deficits, Seizures, Strokes, and Other Accompanying Conditions
3.2.8. Diagnosis of HaRCVS and RCVS
3.2.9. Imaging in RCVS and Temporal Relation of Symptomatology and Vasoconstriction
3.3. RCVS Headaches in Children vs. Adults
3.4. RCVS and COVID-19
4. Discussion
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Calic, Z.; Cappelen-Smith, C.; Zagami, A.S. Reversible cerebral vasoconstriction syndrome. Intern. Med. J. 2015, 45, 599–608. [Google Scholar] [CrossRef]
- Call, G.K.; Fleming, M.C.; Sealfon, S.; Levine, H.; Kistler, J.P.; Fisher, C.M. Reversible cerebral segmental vasoconstriction. Stroke 1988, 19, 1159–1170. [Google Scholar] [CrossRef]
- Ducros, A.; Boukobza, M.; Porcher, R.; Sarov, M.; Valade, D.; Bousser, M.G. The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome. A prospective series of 67 patients. Brain 2007, 130, 3091–3101. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, L.H.; Dodick, D.W.; Schwedt, T.J.; Singhal, A.B. Narrative review: Reversible cerebral vasoconstriction syndromes. Ann. Intern. Med. 2007, 146, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Ducros, A. Reversible cerebral vasoconstriction syndrome. Lancet Neurol. 2012, 11, 906–917. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.P.; Fuh, J.L.; Wang, S.J.; Chang, F.C.; Lirng, J.F.; Fang, Y.C.; Shia, B.C.; Wu, J.C. Magnetic resonance angiography in reversible cerebral vasoconstriction syndromes. Ann. Neurol. 2010, 67, 648–656. [Google Scholar] [CrossRef]
- Singhal, A.B.; Hajj-Ali, R.A.; Topcuoglu, M.A.; Fok, J.; Bena, J.; Yang, D.; Calabrese, L.H. Reversible cerebral vasoconstriction syndromes: Analysis of 139 cases. Arch. Neurol. 2011, 68, 1005–1012. [Google Scholar] [CrossRef]
- Katz, B.S.; Fugate, J.E.; Ameriso, S.F.; Pujol-Lereis, V.A.; Mandrekar, J.; Flemming, K.D.; Kallmes, D.F.; Rabinstein, A.A. Clinical worsening in reversible cerebral vasoconstriction syndrome. JAMA Neurol. 2014, 71, 68–73. [Google Scholar] [CrossRef]
- Magid-Bernstein, J.; Omran, S.S.; Parikh, N.S.; Merkler, A.E.; Navi, B.; Kamel, H. RCVS: Symptoms, Incidence, and Resource Utilization in a Population-Based US Cohort. Neurology 2021, 97, e248–e253. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [CrossRef]
- Rocha, E.A.; Topcuoglu, M.A.; Silva, G.S.; Singhal, A.B. RCVS(2) score and diagnostic approach for reversible cerebral vasoconstriction syndrome. Neurology 2019, 92, e639–e647. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Lee, M.J.; Gil, Y.E.; Chung, C.S. RCVS-TCH score can predict reversible cerebral vasoconstriction syndrome in patients with thunderclap headache. Sci. Rep. 2021, 11, 7750. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Alons, I.M.E.; Goudsmit, B.F.J.; Jellema, K.; van Walderveen, M.A.A.; Wermer, M.J.H.; Algra, A. Prediction of vascular abnormalities on CT angiography in patients with acute headache. Brain Behav. 2018, 8, e00997. [Google Scholar] [CrossRef]
- Anzola, G.P.; Brighenti, R.; Cobelli, M.; Giossi, A.; Mazzucco, S.; Olivato, S.; Pari, E.; Piras, M.P.; Padovani, A.; Rinaldi, F.; et al. Reversible cerebral vasoconstriction syndrome in puerperium: A prospective study. J. Neurol. Sci. 2017, 375, 130–136. [Google Scholar] [CrossRef]
- Anzola, G.P.; Brighenti, R.; Cobelli, M.; Giossi, A.; Mazzucco, S.; Olivato, S.; Pari, E.; Piras, M.P.; Padovani, A.; Rinaldi, F.; et al. Postpartum Headache: A Prospective Study. J. Oral. Facial Pain. Headache 2017, 31, 346–352. [Google Scholar] [CrossRef]
- Boitet, R.; de Gaalon, S.; Duflos, C.; Marin, G.; Mawet, J.; Burcin, C.; Roos, C.; Fiedler, U.; Bousser, M.G.; Ducros, A. Long-Term Outcomes after Reversible Cerebral Vasoconstriction Syndrome. Stroke 2020, 51, 670–673. [Google Scholar] [CrossRef] [PubMed]
- Caria, F.; Zedde, M.; Gamba, M.; Bersano, A.; Rasura, M.; Adami, A.; Piantadosi, C.; Quartuccio, L.; Azzini, C.; Melis, M.; et al. The clinical spectrum of reversible cerebral vasoconstriction syndrome: The Italian Project on Stroke at Young Age (IPSYS). Cephalalgia 2019, 39, 1267–1276. [Google Scholar] [CrossRef]
- Chen, C.Y.; Chen, S.P.; Fuh, J.L.; Lirng, J.F.; Chang, F.C.; Wang, Y.F.; Wang, S.J. Vascular wall imaging in reversible cerebral vasoconstriction syndrome—A 3-T contrast-enhanced MRI study. J. Headache Pain 2018, 19, 74. [Google Scholar] [CrossRef]
- Chen, S.P.; Chou, K.H.; Fuh, J.L.; Huang, Y.H.; Huang, C.C.; Lirng, J.F.; Wang, Y.F.; Lin, C.P.; Wang, S.J. Dynamic Changes in White Matter Hyperintensities in Reversible Cerebral Vasoconstriction Syndrome. JAMA Neurol. 2018, 75, 1106–1113. [Google Scholar] [CrossRef]
- Chen, S.P.; Fuh, J.L.; Chang, F.C.; Lirng, J.F.; Shia, B.C.; Wang, S.J. Transcranial color doppler study for reversible cerebral vasoconstriction syndromes. Ann. Neurol. 2008, 63, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.P.; Fuh, J.L.; Lirng, J.F.; Wang, Y.F.; Wang, S.J. Recurrence of reversible cerebral vasoconstriction syndrome: A long-term follow-up study. Neurology 2015, 84, 1552–1558. [Google Scholar] [CrossRef]
- Cheng, Y.C.; Kuo, K.H.; Lai, T.H. A common cause of sudden and thunderclap headaches: Reversible cerebral vasoconstriction syndrome. J. Headache Pain 2014, 15, 13. [Google Scholar] [CrossRef]
- Cho, S.; Lee, M.J.; Chung, C.S. Effect of Nimodipine Treatment on the Clinical Course of Reversible Cerebral Vasoconstriction Syndrome. Front. Neurol. 2019, 10, 644. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.A.; Lee, M.J.; Choi, H.; Chung, C.S. Characteristics and demographics of reversible cerebral vasoconstriction syndrome: A large prospective series of Korean patients. Cephalalgia 2018, 38, 765–775. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.A.; Lee, M.J.; Chung, C.S. Cerebral endothelial dysfunction in reversible cerebral vasoconstriction syndrome: A case-control study. J. Headache Pain 2017, 18, 29. [Google Scholar] [CrossRef]
- Dakay, K.B.; Azher, I.; Mahta, A.; Furie, K.; Yaghi, S.; Cutting, S.M. Multifocal Atraumatic Convexity Subarachnoid Hemorrhage. Cureus 2021, 13, e16091. [Google Scholar] [CrossRef]
- de Boysson, H.; Parienti, J.J.; Mawet, J.; Arquizan, C.; Boulouis, G.; Burcin, C.; Naggara, O.; Zuber, M.; Touzé, E.; Aouba, A.; et al. Primary angiitis of the CNS and reversible cerebral vasoconstriction syndrome: A comparative study. Neurology 2018, 91, e1468–e1478. [Google Scholar] [CrossRef]
- Ducros, A.; Fiedler, U.; Porcher, R.; Boukobza, M.; Stapf, C.; Bousser, M.G. Hemorrhagic manifestations of reversible cerebral vasoconstriction syndrome: Frequency, features, and risk factors. Stroke 2010, 41, 2505–2511. [Google Scholar] [CrossRef]
- Forman, R.; Conners, J.J.; Song, S.Y.; John, S.; Garg, R.; Harris, J.; Lee, V.H. The Spectrum of Nontraumatic Convexity Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2019, 28, 104473. [Google Scholar] [CrossRef]
- Fukaguchi, K.; Goto, T.; Fukui, H.; Sekine, I.; Yamagami, H. Reversible cerebral vasoconstriction syndrome: The importance of follow-up imaging within 2 weeks. Acute Med. Surg. 2020, 7, e559. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Starr, M.; Rocha, M.; Ortega-Gutierrez, S. Early Risk of Readmission Following Hospitalization for Reversible Cerebral Vasoconstriction Syndrome. Neurology 2021, 96, e2912–e2919. [Google Scholar] [CrossRef]
- Graff-Radford, J.; Fugate, J.E.; Klaas, J.; Flemming, K.D.; Brown, R.D.; Rabinstein, A.A. Distinguishing clinical and radiological features of non-traumatic convexal subarachnoid hemorrhage. Eur. J. Neurol. 2016, 23, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Grooters, G.S.; Sluzewski, M.; Tijssen, C.C. How often is thunderclap headache caused by the reversible cerebral vasoconstriction syndrome? Headache 2014, 54, 732–735. [Google Scholar] [CrossRef]
- Hathidara, M.; Patel, N.H.; Flores, A.; Cabrera, Y.; Cabrera, F.; Koch, S. Transcranial Doppler findings in reversible cerebral vasoconstriction syndrome. J. Neuroimaging 2022, 32, 345–351. [Google Scholar] [CrossRef]
- John, S.; Singhal, A.B.; Calabrese, L.; Uchino, K.; Hammad, T.; Tepper, S.; Stillman, M.; Mills, B.; Thankachan, T.; Hajj-Ali, R.A. Long-term outcomes after reversible cerebral vasoconstriction syndrome. Cephalalgia 2016, 36, 387–394. [Google Scholar] [CrossRef]
- Kim, T.; Ahn, S.; Sohn, C.H.; Seo, D.W.; Kim, W.Y. Reversible cerebral vasoconstriction syndrome at the emergency department. Clin. Exp. Emerg. Med. 2015, 2, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Kraayvanger, L.; Berlit, P.; Albrecht, P.; Hartung, H.P.; Kraemer, M. Cerebrospinal fluid findings in reversible cerebral vasoconstriction syndrome: A way to differentiate from cerebral vasculitis? Clin. Exp. Immunol. 2018, 193, 341–345. [Google Scholar] [CrossRef]
- Kumar, N.; Kumar, S.; Rocha, E.; Lioutas, V.A. Vasoconstriction and long-term headache in reversible cerebral vasoconstriction syndrome. J. Neurol. 2023, 270, 1647–1653. [Google Scholar] [CrossRef]
- Kumar, S.; Goddeau, R.P., Jr.; Selim, M.H.; Thomas, A.; Schlaug, G.; Alhazzani, A.; Searls, D.E.; Caplan, L.R. Atraumatic convexal subarachnoid hemorrhage: Clinical presentation, imaging patterns, and etiologies. Neurology 2010, 74, 893–899. [Google Scholar] [CrossRef]
- Kunitake, K.; Ogura, A.; Iwata-Hatanaka, M.; Inagaki, R.; Furukawa, S.; Suzuki, J.; Nakai, N.; Nishida, S.; Katsuno, M.; Ito, Y. Persistent brain damage in reversible cerebral vasoconstriction syndrome on (99m)Tc-ethyl cysteinate dimer single-photon emission computed tomography: A long-term observational study. J. Neurol. Sci. 2022, 442, 120441. [Google Scholar] [CrossRef]
- Lange, K.S.; Forster, O.; Mawet, J.; Tuloup, G.; Burcin, C.; Corti, L.; Duflos, C.; Roos, C.; Ducros, A. Type of headache at onset and risk for complications in reversible cerebral vasoconstriction syndrome. Eur. J. Neurol. 2022, 29, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Lange, K.S.; Tuloup, G.; Duflos, C.; Gobron, C.; Burcin, C.; Corti, L.; Roos, C.; Ducros, A.; Mawet, J. Complications of reversible cerebral vasoconstriction syndrome in relation to age. J. Neurol. 2023, 270, 3584–3594. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Cha, J.; Choi, H.A.; Woo, S.Y.; Kim, S.; Wang, S.J.; Chung, C.S. Blood-brain barrier breakdown in reversible cerebral vasoconstriction syndrome: Implications for pathophysiology and diagnosis. Ann. Neurol. 2017, 81, 454–466. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Choi, H.A.; Choi, H.; Chung, C.S. Serial testing of the ICHD-3 beta diagnostic criteria for probable reversible cerebral vasoconstriction syndrome: A prospective validation study. Cephalalgia 2018, 38, 1665–1671. [Google Scholar] [CrossRef] [PubMed]
- Levin, J.H.; Benavides, J.; Caddick, C.; Laurie, K.; Wilterdink, J.; Yaghi, S.; Silver, B.; Khan, M. Transcranial Doppler Ultrasonography As a Non-Invasive Tool for Diagnosis and Monitoring of Reversible Cerebral Vasoconstriction Syndrome. Rhode Isl. Med. J. 2016, 99, 38–41. [Google Scholar]
- Lin, P.T.; Wang, Y.F.; Fuh, J.L.; Lirng, J.F.; Ling, Y.H.; Chen, S.P.; Wang, S.J. Diagnosis and classification of headache associated with sexual activity using a composite algorithm: A cohort study. Cephalalgia 2021, 41, 1447–1457. [Google Scholar] [CrossRef]
- Ling, Y.H.; Wang, Y.F.; Lirng, J.F.; Fuh, J.L.; Wang, S.J.; Chen, S.P. Post-reversible cerebral vasoconstriction syndrome headache. J. Headache Pain 2021, 22, 14. [Google Scholar] [CrossRef]
- Mathon, B.; Ducros, A.; Bresson, D.; Herbrecht, A.; Mirone, G.; Houdart, E.; Saint-Maurice, J.P.; Di Emidio, P.; George, B.; Chibbaro, S. Subarachnoid and intra-cerebral hemorrhage in young adults: Rare and underdiagnosed. Rev. Neurol. 2014, 170, 110–118. [Google Scholar] [CrossRef]
- Mawet, J.; Boukobza, M.; Franc, J.; Sarov, M.; Arnold, M.; Bousser, M.G.; Ducros, A. Reversible cerebral vasoconstriction syndrome and cervical artery dissection in 20 patients. Neurology 2013, 81, 821–824. [Google Scholar] [CrossRef]
- Muehlschlegel, S.; Kursun, O.; Topcuoglu, M.A.; Fok, J.; Singhal, A.B. Differentiating reversible cerebral vasoconstriction syndrome with subarachnoid hemorrhage from other causes of subarachnoid hemorrhage. JAMA Neurol. 2013, 70, 1254–1260. [Google Scholar] [CrossRef] [PubMed]
- Néel, A.; Auffray-Calvier, E.; Guillon, B.; Fontenoy, A.M.; Loussouarn, D.; Pagnoux, C.; Hamidou, M.A. Challenging the diagnosis of primary angiitis of the central nervous system: A single-center retrospective study. J. Rheumatol. 2012, 39, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.D.; Topiwala, K.; Saini, V.; Patel, N.; Pervez, M.; Al-Mufti, F.; Hassan, A.E.; Khandelwal, P.; Starke, R.M. Hemorrhagic reversible cerebral vasoconstriction syndrome: A retrospective observational study. J. Neurol. 2021, 268, 632–639. [Google Scholar] [CrossRef]
- Rico, M.; Benavente, L.; Para, M.; Santamarta, E.; Pascual, J.; Calleja, S. Headache as a crucial symptom in the etiology of convexal subarachnoid hemorrhage. Headache 2014, 54, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.C.; Chen, S.P.; Fuh, J.L.; Wang, Y.F.; Wang, S.J. Influence of Climate on the Incidence of RCVS—A Retrospective Study from Taiwan. Headache 2019, 59, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Shimoda, M.; Oda, S.; Hirayama, A.; Imai, M.; Komatsu, F.; Hoshikawa, K.; Shigematsu, H.; Nishiyama, J.; Osada, T. Centripetal Propagation of Vasoconstriction at the Time of Headache Resolution in Patients with Reversible Cerebral Vasoconstriction Syndrome. AJNR Am. J. Neuroradiol. 2016, 37, 1594–1598. [Google Scholar] [CrossRef]
- Shimoda, M.; Oda, S.; Shigematsu, H.; Hoshikawa, K.; Imai, M.; Komatsu, F.; Hirayama, A.; Osada, T. Clinical significance of centripetal propagation of vasoconstriction in patients with reversible cerebral vasoconstriction syndrome: A retrospective case-control study. Cephalalgia 2018, 38, 1864–1875. [Google Scholar] [CrossRef]
- Singhal, A.B.; Topcuoglu, M.A. Glucocorticoid-associated worsening in reversible cerebral vasoconstriction syndrome. Neurology 2017, 88, 228–236. [Google Scholar] [CrossRef]
- Singhal, A.B.; Topcuoglu, M.A.; Fok, J.W.; Kursun, O.; Nogueira, R.G.; Frosch, M.P.; Caviness, V.S., Jr. Reversible cerebral vasoconstriction syndromes and primary angiitis of the central nervous system: Clinical, imaging, and angiographic comparison. Ann. Neurol. 2016, 79, 882–894. [Google Scholar] [CrossRef]
- Smith, J.H.; Amer, M.A.; Schwedt, T.J. Characterization of thunderclap headache in a reversible cerebral vasoconstriction syndrome case series. Headache 2021, 61, 396–398. [Google Scholar] [CrossRef]
- Strunk, D.; Veltkamp, R.; Meuth, S.G.; Chapot, R.; Kraemer, M. Intra-arterial application of nimodipine in reversible cerebral vasoconstriction syndrome: A neuroradiological method to help differentiate from primary central nervous system vasculitis. Neurol. Res. Pract. 2022, 4, 8. [Google Scholar] [CrossRef] [PubMed]
- Topcuoglu, M.A.; Chan, S.T.; Silva, G.S.; Smith, E.E.; Kwong, K.K.; Singhal, A.B. Cerebral vasomotor reactivity in reversible cerebral vasoconstriction syndrome. Cephalalgia 2017, 37, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Topcuoglu, M.A.; Kursun, O.; Singhal, A.B. Coexisting vascular lesions in reversible cerebral vasoconstriction syndrome. Cephalalgia 2017, 37, 29–35. [Google Scholar] [CrossRef]
- Topcuoglu, M.A.; McKee, K.E.; Singhal, A.B. Gender and hormonal influences in reversible cerebral vasoconstriction syndrome. Eur. Stroke J. 2016, 1, 199–204. [Google Scholar] [CrossRef]
- Topcuoglu, M.A.; Singhal, A.B. Hemorrhagic Reversible Cerebral Vasoconstriction Syndrome: Features and Mechanisms. Stroke 2016, 47, 1742–1747. [Google Scholar] [CrossRef]
- Wang, S.J.; Fuh, J.L.; Wu, Z.A.; Chen, S.P.; Lirng, J.F. Bath-related thunderclap headache: A study of 21 consecutive patients. Cephalalgia 2008, 28, 524–530. [Google Scholar] [CrossRef]
- Wolff, V.; Armspach, J.P.; Lauer, V.; Rouyer, O.; Ducros, A.; Marescaux, C.; Gény, B. Ischaemic strokes with reversible vasoconstriction and without thunderclap headache: A variant of the reversible cerebral vasoconstriction syndrome? Cerebrovasc. Dis. 2015, 39, 31–38. [Google Scholar] [CrossRef] [PubMed]
- The International Classification of Headache Disorders: 2nd edition. Cephalalgia 2004, 24 (Suppl. S1), 9–160. [CrossRef]
- Chen, S.P.; Fuh, J.L.; Wang, S.J. Reversible cerebral vasoconstriction syndrome: An under-recognized clinical emergency. Ther. Adv. Neurol. Disord. 2010, 3, 161–171. [Google Scholar] [CrossRef]
- Wolff, V.; Ducros, A. Reversible Cerebral Vasoconstriction Syndrome without Typical Thunderclap Headache. Headache 2016, 56, 674–687. [Google Scholar] [CrossRef]
- Ducros, A.; Wolff, V. The Typical Thunderclap Headache of Reversible Cerebral Vasoconstriction Syndrome and Its Various Triggers. Headache 2016, 56, 657–673. [Google Scholar] [CrossRef] [PubMed]
- Erhart, D.K.; Ludolph, A.C.; Althaus, K. RCVS: By clinicians for clinicians–A narrative review. J. Neurol. 2023, 270, 673–688. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.R.; Shivashankar, R.; Mossa-Basha, M.; Gandhi, D. Reversible Cerebral Vasoconstriction Syndrome, Part 1: Epidemiology, Pathogenesis, and Clinical Course. AJNR Am. J. Neuroradiol. 2015, 36, 1392–1399. [Google Scholar] [CrossRef] [PubMed]
- Singhal, A.B.; Bernstein, R.A. Postpartum angiopathy and other cerebral vasoconstriction syndromes. Neurocrit Care 2005, 3, 91–97. [Google Scholar] [CrossRef]
- Roth, J.; Deck, G. Neurovascular disorders in pregnancy: A review. Obstet. Med. 2019, 12, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Fugate, J.E.; Ameriso, S.F.; Ortiz, G.; Schottlaender, L.V.; Wijdicks, E.F.; Flemming, K.D.; Rabinstein, A.A. Variable presentations of postpartum angiopathy. Stroke 2012, 43, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Song, T.J.; Lee, K.H.; Li, H.; Kim, J.Y.; Chang, K.; Kim, S.H.; Han, K.H.; Kim, B.Y.; Kronbichler, A.; Ducros, A.; et al. Reversible cerebral vasoconstriction syndrome: A comprehensive systematic review. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3519–3529. [Google Scholar] [CrossRef]
- Abruzzo, T.; Patino, M.; Leach, J.; Rahme, R.; Geller, J. Cerebral vasoconstriction triggered by sympathomimetic drugs during intra-atrerial chemotherapy. Pediatr. Neurol. 2013, 48, 139–142. [Google Scholar] [CrossRef]
- Short, K.; Emsley, H.C.A. Illicit Drugs and Reversible Cerebral Vasoconstriction Syndrome. Neurohospitalist 2021, 11, 40–44. [Google Scholar] [CrossRef]
- Perillo, T.; Paolella, C.; Perrotta, G.; Serino, A.; Caranci, F.; Manto, A. Reversible cerebral vasoconstriction syndrome: Review of neuroimaging findings. Radiol. Med. 2022, 127, 981–990. [Google Scholar] [CrossRef]
- Pilato, F.; Distefano, M.; Calandrelli, R. Posterior Reversible Encephalopathy Syndrome and Reversible Cerebral Vasoconstriction Syndrome: Clinical and Radiological Considerations. Front. Neurol. 2020, 11, 34. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, K.; Ortiz, J.F.; Parwani, J.; Cruz, C.; Yépez, M.; Buj, M.; Khurana, M.; Ojeda, D.; Iturburu, A.; Aguirre, A.S.; et al. Reversible Cerebral Vasoconstriction Syndrome in the Postpartum Period: A Systematic Review and Meta-Analysis. Neurol. Int. 2022, 14, 488–496. [Google Scholar] [CrossRef]
- Paliwal, P.R.; Teoh, H.L.; Sharma, V.K. Association between reversible cerebral vasoconstriction syndrome and thrombotic thrombocytopenic purpura. J. Neurol. Sci. 2014, 338, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Hajj-Ali, R.A.; Furlan, A.; Abou-Chebel, A.; Calabrese, L.H. Benign angiopathy of the central nervous system: Cohort of 16 patients with clinical course and long-term followup. Arthritis Rheum. 2002, 47, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Rozen, T.D.; Beams, J.L. New daily persistent headache with a thunderclap headache onset and complete response to nimodipine (a new distinct subtype of NDPH). J. Headache Pain 2013, 14, 100. [Google Scholar] [CrossRef]
- Jamali, S.A.; Rozen, T.D. An RCVS Spectrum Disorder? New Daily Persistent Headache Starting as a Single Thunderclap Headache (3 New Cases). Headache 2019, 59, 789–794. [Google Scholar] [CrossRef]
- Ling, Y.H.; Chen, S.P. Narrative Review: Headaches After Reversible Cerebral Vasoconstriction Syndrome. Curr. Pain Headache Rep. 2020, 24, 74. [Google Scholar] [CrossRef]
- Guryildirim, M.; Kontzialis, M.; Ozen, M.; Kocak, M. Acute Headache in the Emergency Setting. Radiographics 2019, 39, 1739–1759. [Google Scholar] [CrossRef]
- Ribas, M.Z.; Paticcié, G.F.; de Medeiros, S.D.P.; de Oliveira Veras, A.; Noleto, F.M.; Dos Santos, J.C.C. Reversible cerebral vasoconstriction syndrome: Literature review. Egypt. J. Neurol. Psychiatr. Neurosurg. 2023, 59, 5. [Google Scholar] [CrossRef]
- Arrigan, M.T.; Heran, M.K.S.; Shewchuk, J.R. Reversible cerebral vasoconstriction syndrome: An important and common cause of thunderclap and recurrent headaches. Clin. Radiol. 2018, 73, 417–427. [Google Scholar] [CrossRef]
- Santos, L.; Azevedo, E. Reversible cerebral vasoconstriction syndrome—A narrative revision of the literature. Porto Biomed. J. 2016, 1, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Camus-Jacqmin, M.; Stapf, C.; Ducros, A.; Viswanathan, A.; Berthet, K.; Bousser, M.G. Postpartum cervicocephalic artery dissection. Stroke 2008, 39, 2377–2379. [Google Scholar] [CrossRef] [PubMed]
- Burton, T.M.; Bushnell, C.D. Reversible Cerebral Vasoconstriction Syndrome. Stroke 2019, 50, 2253–2258. [Google Scholar] [CrossRef] [PubMed]
- Kano, Y.; Inui, S.; Uchida, Y.; Sakurai, K.; Muto, M.; Sugiyama, H.; Takeshima, T.; Yuasa, H.; Yamada, K.; Matsukawa, N. Quantitative arterial spin labeling magnetic resonance imaging analysis of reversible cerebral vasoconstriction syndrome: A case series. Headache 2021, 61, 687–693. [Google Scholar] [CrossRef]
- Oliveira, R.; Inácio, N.; Baptista, P.; Gil-Gouveia, R. Transcranial Doppler findings in a population with clinical probable reversible cerebral vasoconstriction syndrome. Rev. Neurol. 2022, 178, 385–390. [Google Scholar] [CrossRef]
- Chen, S.P.; Wang, S.J. Hyperintense vessels: An early MRI marker of reversible cerebral vasoconstriction syndrome? Cephalalgia 2014, 34, 1038–1039. [Google Scholar] [CrossRef]
- Levitt, A.; Zampolin, R.; Burns, J.; Bello, J.A.; Slasky, S.E. Posterior Reversible Encephalopathy Syndrome and Reversible Cerebral Vasoconstriction Syndrome: Distinct Clinical Entities with Overlapping Pathophysiology. Radiol. Clin. North. Am. 2019, 57, 1133–1146. [Google Scholar] [CrossRef]
- Maldonado-Soto, A.R.; Fryer, R.H. Reversible cerebral vasoconstriction syndrome in children: An update. Semin. Pediatr. Neurol. 2021, 40, 100936. [Google Scholar] [CrossRef] [PubMed]
- Kuga, S.; Goto, H.; Okanari, K.; Maeda, T.; Ihara, K. Reversible cerebral vasoconstriction syndrome manifesting as focal seizures without a thunderclap headache: A pediatric case report. Brain Dev. 2016, 38, 880–883. [Google Scholar] [CrossRef]
- Haffner, D.N.; Rollins, N.K.; Dowling, M.M. Reversible Cerebral Vasoconstriction Syndrome: A Novel Mechanism for Neurological Complications in Schimke Immuno-Osseous Dysplasia. Pediatr. Neurol. 2019, 92, 67–70. [Google Scholar] [CrossRef]
- Taylor, C.S.; Kelly, B.M.; Nichols, T.A. Fear the reaper: Reversible cerebrovascular vasoconstriction syndrome after hot pepper ingestion. Radiol. Case Rep. 2020, 15, 641–643. [Google Scholar] [CrossRef] [PubMed]
- Bliss, L.; McGowan, B.; Rahman, A. A Rare Pediatric Case of Marijuana-Induced Reversible Cerebral Vasoconstriction Syndrome. Pediatr. Neurol. 2021, 120, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Fikse, D.J.; Grenz, P.M.; Wheatley, S.M.; Fugok, K.L. Posterior reversible encephalopathy syndrome associated with Henoch Schonlein Purpura in a pediatric patient. Am. J. Emerg. Med. 2021, 43, 291.e5–291.e7. [Google Scholar] [CrossRef] [PubMed]
- Manuel, A.R.; Gonçalves, C.; Silva, A.; Escobar, C.; Manaças, R.; Luís, C. Reversible Cerebral Vasoconstriction Syndrome in a Previously Healthy Child: A Case Report. Neurol. Clin. Pract. 2022, 12, e116–e120. [Google Scholar] [CrossRef]
- Sadeghizadeh, A.; Pourmoghaddas, Z.; Zandifar, A.; Tara, S.Z.; Rahimi, H.; Saleh, R.; Ramezani, S.; Ghazavi, M.; Yaghini, O.; Hosseini, N.; et al. Reversible Cerebral Vasoconstriction Syndrome and Multisystem Inflammatory Syndrome in Children with COVID-19. Pediatr. Neurol. 2022, 129, 1–6. [Google Scholar] [CrossRef]
- Rizzati, F.; Marie, G.; Chanez, V.; Ferry, T.; Natterer, J.; Longchamp, D.; Saliou, G.; Perez, M.H. Intra-arterial vasodilators infusion for management of reversible cerebral vasoconstriction syndrome in a 12-year-old girl: A case report. Front. Pediatr. 2023, 11, 1042509. [Google Scholar] [CrossRef] [PubMed]
- Kirton, A.; Diggle, J.; Hu, W.; Wirrell, E. A pediatric case of reversible segmental cerebral vasoconstriction. Can J. Neurol. Sci. 2006, 33, 250–253. [Google Scholar] [CrossRef]
- Liu, H.Y.; Fuh, J.L.; Lirng, J.F.; Chen, S.P.; Wang, S.J. Three paediatric patients with reversible cerebral vasoconstriction syndromes. Cephalalgia 2010, 30, 354–359. [Google Scholar] [CrossRef]
- Probert, R.; Saunders, D.E.; Ganesan, V. Reversible cerebral vasoconstriction syndrome: Rare or underrecognized in children? Dev. Med. Child. Neurol. 2013, 55, 385–389. [Google Scholar] [CrossRef]
- Guerriero, R.M.; Rivkin, M.J. Reversible vasoconstriction syndrome involving the basilar artery in an adolescent: Imaging and clinical features. Pediatr. Neurol. 2015, 52, 635–637. [Google Scholar] [CrossRef]
- Coffino, S.W.; Fryer, R.H. Reversible Cerebral Vasoconstriction Syndrome in Pediatrics: A Case Series and Review. J. Child Neurol. 2017, 32, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Kamide, T.; Tsutsui, T.; Misaki, K.; Sano, H.; Mohri, M.; Uchiyama, N.; Nakada, M. A Pediatric Case of Reversible Cerebral Vasoconstriction Syndrome with Similar Radiographic Findings to Posterior Reversible Encephalopathy Syndrome. Pediatr. Neurol. 2017, 71, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Kazato, Y.; Fujii, K.; Oba, H.; Hino, M.; Ochiai, H.; Uchikawa, H.; Kohno, Y. Reversible cerebral vasoconstriction syndrome associated with brain parenchymal hemorrhage. Brain Dev. 2012, 34, 696–699. [Google Scholar] [CrossRef] [PubMed]
- Ueki, H.; Sanayama, Y.; Miyajima, A.; Tsuchimochi, T.; Igarashi, S.; Sunami, S. Reversible Cerebral Vasoconstriction Syndrome Promptly Diagnosed with Magnetic Resonance Imaging Including Magnetic Resonance Angiography During Immunosuppressive Therapy in a 16-Year-Old Girl with Refractory Cytopenia of Childhood. Hematol. Rep. 2016, 8, 6673. [Google Scholar] [CrossRef]
- Oikawa, Y.; Okubo, Y.; Numata-Uematsu, Y.; Aihara, Y.; Kitamura, T.; Takayanagi, M.; Takahashi, Y.; Kure, S.; Uematsu, M. Initial vasodilatation in a child with reversible cerebral vasoconstriction syndrome. J. Clin. Neurosci. 2017, 39, 108–110. [Google Scholar] [CrossRef]
- Arandela, K.; Samudrala, S.; Abdalkader, M.; Anand, P.; Daneshmand, A.; Dasenbrock, H.; Nguyen, T.; Ong, C.; Takahashi, C.; Shulman, J.; et al. Reversible Cerebral Vasoconstriction Syndrome in Patients with Coronavirus Disease: A Multicenter Case Series. J. Stroke Cerebrovasc. Dis. 2021, 30, 106118. [Google Scholar] [CrossRef]
- Dakay, K.; Kaur, G.; Gulko, E.; Santarelli, J.; Bowers, C.; Mayer, S.A.; Gandhi, C.D.; Al-Mufti, F. Reversible cerebral vasoconstriction syndrome and dissection in the setting of COVID-19 infection. J. Stroke Cerebrovasc. Dis. 2020, 29, 105011. [Google Scholar] [CrossRef]
- Mansoor, T.; Alsarah, A.A.; Mousavi, H.; Khader Eliyas, J.; Girotra, T.; Hussein, O. COVID-19 Associated Reversible Cerebral Vasoconstriction Syndrome Successfully Treated with Nimodipine and Aspirin. J. Stroke Cerebrovasc. Dis. 2021, 30, 105822. [Google Scholar] [CrossRef]
- Srinivasan, A.; Wilson, B.C.; Bear, M.; Hasan, A.; Ezzeldin, O.; Alim, S.; Elfallal, S.; Fang, X.; Ezzeldin, M. Intracerebral Hemorrhage and Reversible Cerebral Vasoconstriction Syndrome in a Patient with COVID-19. Cureus 2021, 13, e17408. [Google Scholar] [CrossRef]
- Harahsheh, E.; Gritsch, D.; Mbonde, A.; Apolinario, M.; Hoxworth, J.M.; Demaerschalk, B.M. Reversible Cerebral Vasoconstriction Syndrome in the Setting of COVID-19 and Pleomorphic Sarcoma: A Case Report. Neurologist 2022, 27, 135–138. [Google Scholar] [CrossRef]
- Ray, S.; Kamath, V.V.; Raju, A.; Rajesh, K.N.; Shalini, N. Fulminant Reversible Cerebral Vasoconstriction Syndrome in Breakthrough COVID-19 Infection. J. Stroke Cerebrovasc. Dis. 2022, 31, 106238. [Google Scholar] [CrossRef] [PubMed]
- Scheer, M.; Harder, A.; Wagner, S.; Ibe, R.; Prell, J.; Scheller, C.; Strauss, C.; Simmermacher, S. Case report of a fulminant non-aneurysmal convexity subarachnoid hemorrhage after COVID-19. Interdiscip. Neurosurg. 2022, 27, 101437. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 mRNA Pfizer-BioNTech Vaccine Analysis Print. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1072043/COVID-19_mRNA_Pfizer-_BioNTech_vaccine_analysis_print.pdf (accessed on 25 June 2023).
- Finsterer, J. First Reported Case of Reversible Cerebral Vasoconstriction Syndrome after a SARS-CoV-2 Vaccine. Cureus 2021, 13, e19987. [Google Scholar] [CrossRef] [PubMed]
- Lund, A.M.; Al-Karagholi, M.A. COVID-19 Vaccination Might Induce Reversible Cerebral Vasoconstriction Syndrome Attacks: A Case Report. Vaccines 2022, 10, 823. [Google Scholar] [CrossRef]
- Mawet, J.; Debette, S.; Bousser, M.G.; Ducros, A. The Link Between Migraine, Reversible Cerebral Vasoconstriction Syndrome and Cervical Artery Dissection. Headache 2016, 56, 645–656. [Google Scholar] [CrossRef]
- Chen, S.P.; Chang, Y.A.; Chou, C.H.; Juan, C.C.; Lee, H.C.; Chen, L.K.; Wu, P.C.; Wang, Y.F.; Fuh, J.L.; Lirng, J.F.; et al. Circulating microRNAs Associated with Reversible Cerebral Vasoconstriction Syndrome. Ann. Neurol. 2021, 89, 459–473. [Google Scholar] [CrossRef]
- Lange, K.S.; Choi, S.Y.; Ling, Y.H.; Chen, S.P.; Mawet, J.; Duflos, C.; Lee, M.J.; Ducros, A.; Wang, S.J.; Pezzini, A. Reversible cerebral Vasoconstriction syndrome intERnational CollaborativE (REVERCE) network: Study protocol and rationale of a multicentre research collaboration. Eur. Stroke J. 2023. [Google Scholar] [CrossRef]


{kind=link}
| Type of Study, Population, and Aim | RCVS Cohort Size | TCH n (%) | TCH Definition Used | Baseline Headaches n (%) | Non-TCH Headaches n (%) | Non-TCH Characteristics | Accompanying Symptoms | Absence of Headaches n (%) | |
|---|---|---|---|---|---|---|---|---|---|
| Studies with general RCVS Cohorts 1 | |||||||||
| Ducros 2007 [3] | Prospective description of RCVS patients | 67 | 66 (98.5) | HIS 2004 | (73) | 1 (1.5%) | Acute, severe, >1 min to reach peak | Nausea (57%), vomiting (38%), agitation (32%), photophobia (30%) | 0 |
| Chen 2008 [21] | Prospective analysis of TCD in RCVS cohort vs. controls | 32 | 32 (100) (by design) | BACNS ICHD-2 | 17 (53) | NR | NR | Nausea (63%), photophobia (41%), vomiting (38%), phonophobia (34%) | 0 (by design) |
| Chen 2010 [6] | Prospective analysis of MRA findings in RCVS | 77 | 77 (100) (by design) | BACNS ICHD-2 | NR | 0 (by design) | NR | NR | 0 (by design) |
| Singhal 2011 [7] | Retrospective analysis of MRA findings in RCVS | 139 | (85) | Severe, acute headache | NR | (10) | NR | NR | (5) |
| Choi 2018 [25] | Prospective description of a Korean RCVS cohort | 104 | 90 (86.5) | Onset-to-peak <1 min | NR | 11 (10.6) | Severe headache of gradual onset (peak from 2 to 120 min). Two wake-up | NR | 3 (2.9) |
| Caria 2019 [18] | Retrospective description of an Italian RCVS population | 102 | 69 (67.6) | Onset-to-peak <1 min | Yes, in most patients of mild severity | 33 (32.4) | severe headaches of gradual onset, 14.7%. Throbbing headaches, 7.4%. Persistent headaches of variable severity, acute headaches peaking >1 min | Nausea and vomiting in 81.2% of TCH patients | 0 |
| Strunk 2022 [61] | Retrospective RCVS population, angiographic nimodipine test | 13 | 8 (61.5) | NR | NR | 5 (38.5) | NR | NR | 0 |
| Lange 2022 [42] | RCVS TCH/Non-TCH | 345 | 281 (81.4) | Reaching a maximum intensity above 7/10 in <1 min | NR | 55 (15.9) 2 27 (7.8) 3 | Excruciating reaching max <10 min n = 13, >1 h n = 2, unusual progressive n = 22, mild n = 2, wake-up n = 13 | NR | 9 (2.6) |
| Studies with an RCVS sub-cohort 1 | |||||||||
| Neel 2012 [52] | Retrospective, RCVS vs. PACNS | 13 | 10 (76.9) | “Similar to thunderclap” | NR | 3 (23.1) | NR | NR | 0 |
| Cheng 2014 [23] | Prospective, patients with sudden headache | 25 | 11 (45.8) | ICHD-2 | 11 (44) | 14 (45.2) | Sudden headache | NR | 5 (26%) |
| Wolff 2015 [67] | Prospective, young patients with AIS and RCVS | 21 | 0 | NR | 11 (44%) | 14 (74) | Unusual and severe | NR | 0 |
| Kim 2015 [37] | Retrospective, RCVS in TCH patients that did imaging | 18 | 18 (100) (by design) | Sudden severe headaches that reached maximum intensity within minutes | All (unclear) | 0 (by design) | NR | Nausea (7/18), ocular pain (2/18), vomiting (2/18), dizziness (1/18), phonophobia (1/18) | 0 (by design) |
| Singhal 2016 [59] | Retrospective RCVS vs. PACNS | 159 | (89) 1 | NR | NR | (7) 1 | NR | NR | (3) 1 |
| Graff-Radford 2016 [33] | Retrospective, convex SAH patients | 26 | 21 (80.7) | NR | NR | 2 | NR | NR | 3 (unclear) |
| de Boysson 2018 [28] | Retro-prospective, RCVS vs. PACNS | 173 | 163 (94) | NR | NR | NR | NR | NR | NR |
| Smith 2021 [60] | Retrospective RCVS cohort with acute headaches | 56 | 56 (100) (by design) | Any increase in headache intensity occurring within a 1 min timespan. | 10 (17.8) | 0 (by design) | Peak pain intensity as neither severe nor 8/10 or greater (in some episodes) | NE | 0 (by design) |
| Lin 2021 [47] | Prospective cohort study, headache after sexual activity | 174 | 151 (86.8) | Onset-to-peak <1 min | NR | NR | NR | Nausea 31%, vomiting 14.9%, photophobia 14.4%, phonophobia 27% | 0 (by design) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tentolouris-Piperas, V.; Lymperopoulos, L.; Tountopoulou, A.; Vassilopoulou, S.; Mitsikostas, D.D. Headache Attributed to Reversible Cerebral Vasoconstriction Syndrome (RCVS). Diagnostics 2023, 13, 2730. https://doi.org/10.3390/diagnostics13172730
Tentolouris-Piperas V, Lymperopoulos L, Tountopoulou A, Vassilopoulou S, Mitsikostas DD. Headache Attributed to Reversible Cerebral Vasoconstriction Syndrome (RCVS). Diagnostics. 2023; 13(17):2730. https://doi.org/10.3390/diagnostics13172730
Chicago/Turabian StyleTentolouris-Piperas, Vasileios, Loukas Lymperopoulos, Argyro Tountopoulou, Sophia Vassilopoulou, and Dimos D. Mitsikostas. 2023. "Headache Attributed to Reversible Cerebral Vasoconstriction Syndrome (RCVS)" Diagnostics 13, no. 17: 2730. https://doi.org/10.3390/diagnostics13172730