
Automated Lung Ultrasound Pulmonary Disease Quantification Using an Unsupervised Machine Learning Technique for COVID-19


Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Information
2.2. Lung Ultrasound Features
2.3. Calculated Lung Ultrasound Algorithm
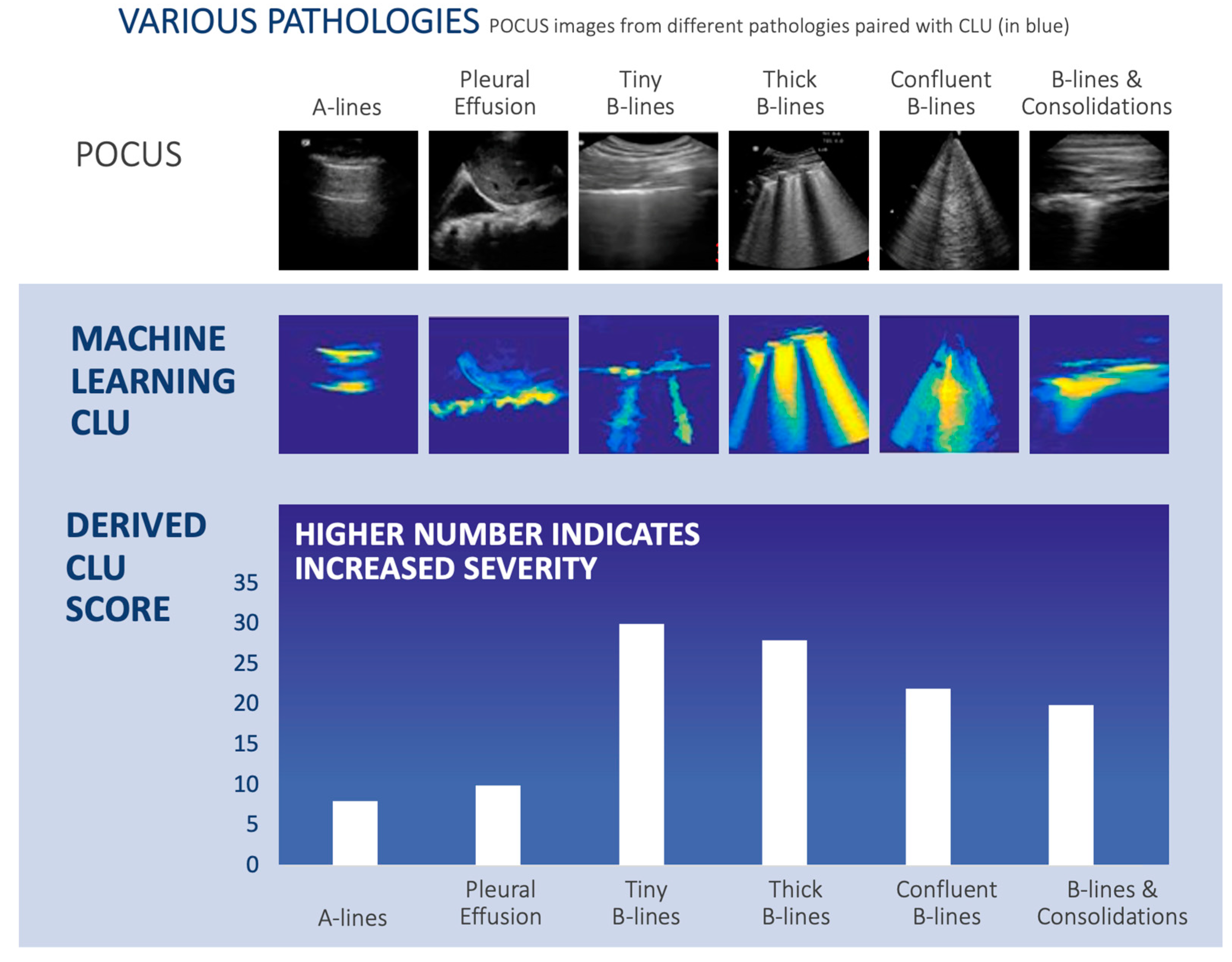
- Computer Vision and Image Segmentation: This component of CLU uses image segmentation and video processing techniques, which include clustering methods and non-linear manifold learning, to detect lung features used by radiologists on lung ultrasound exams [21,22,23,24]. These features were described in Figure 2 and Section 2.2, including A-lines, B-lines, consolidation, pleural effusion, and other findings. The generalized technique for segmentation is described in detail by Akhbardeh (2012) and was previously applied to the topic of breast MRI segmentation [21]. CLU uses the lung ultrasound video series to generate a single image, termed the “integrated image”, which highlights findings within the ultrasound video. Potentially pathological tissue is color-coded, ranging from cyan to orange-red, with normal tissue and background in dark blue. Ultrasound findings were also verified by radiologists with expertise in identifying lung ultrasound findings associated with COVID-19 and other pulmonary disorders.
- Decision-Making: The clinically significant findings and segmentations are retained—A-lines, B lines, pleural irregularity and effusion, consolidation, etc. using both the “integrated image” (the step 1 computer vision component that generates a single image) and the geometric/shape features (step 2). This step quantifies each finding: A-lines, B-lines, consolidation, and pleural effusion.
- Calculated Lung Ultrasound Score: The final step calculates the “CLU Score”, with a normalized range from 0–100, by integrating the aforementioned shape and statistical features.
2.4. Performance Evaluation
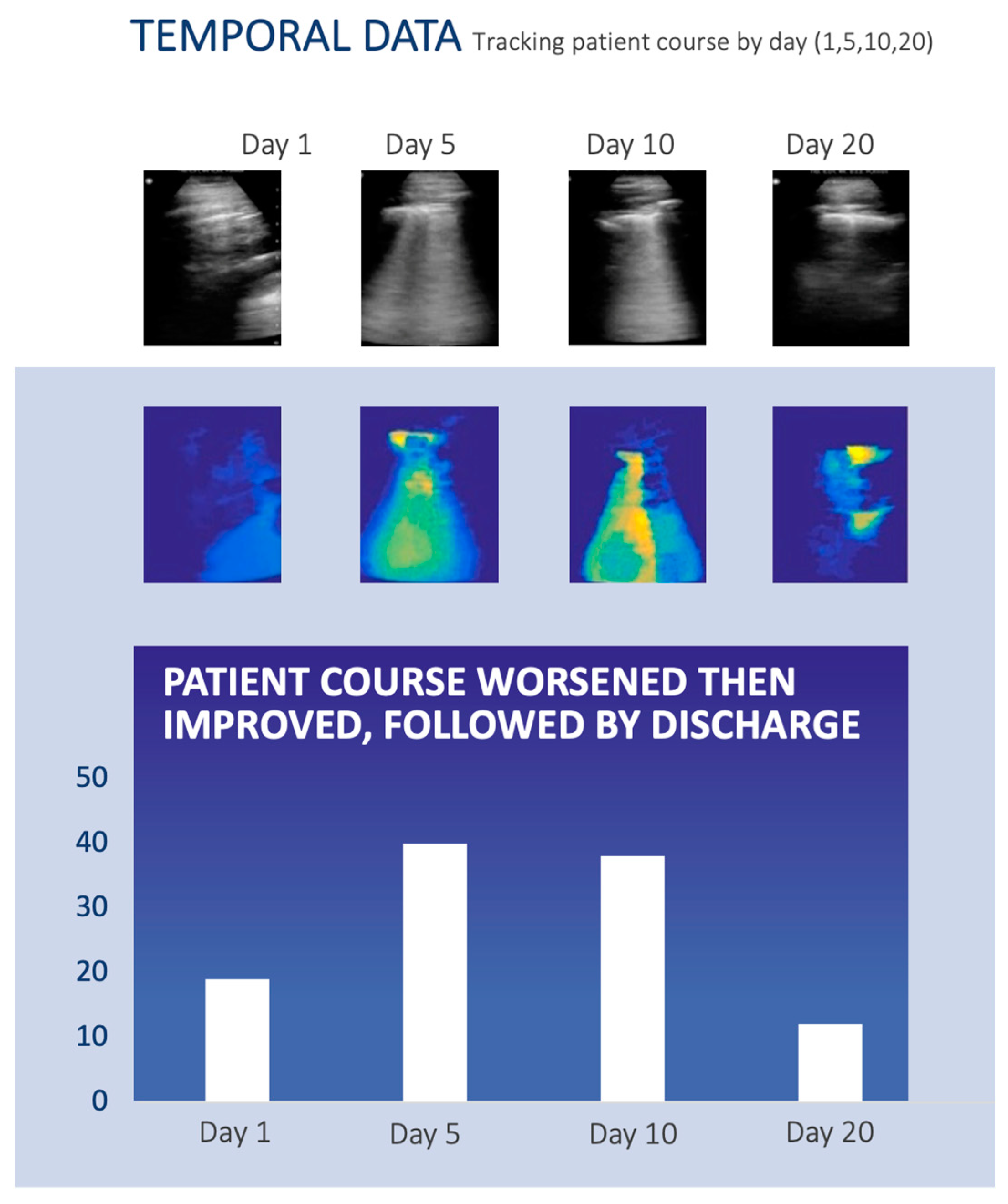
2.5. Example Patient with Longitudinal Monitoring of COVID-19
3. Results
3.1. Comparison of CLU with Different Pathologies
3.2. The Use of CLU for Monitoring Pulmonary Disease Burden Longitudinally
3.3. Comparison of Performance between CLU and Radiologists
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronavirus Resourse Center, Johns Hopkins University. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 19 March 2023).
- Salehi, S.; Abedi, A.; Balakrishnan, S.; Gholamrezanezhad, A. Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. Am. J. Roentgenol. 2020, 215, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C. Portable chest X-ray in coronavirus disease-19 (COVID-19): A pictorial review. Clin. Imaging 2020, 64, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Mossa-Basha, M.; Meltzer, C.C.; Kim, D.C.; Tuite, M.J.; Kolli, K.P.; Tan, B.S. Radiology Department Preparedness for COVID-19: Radiology Scientific Expert Review Panel. Radiology 2020, 296, E106–E112. [Google Scholar] [CrossRef] [PubMed]
- Mutambudzi, M.; Niedwiedz, C.; Macdonald, E.B.; Leyland, A.; Mair, F.; Anderson, J.; Celis-Morales, C.; Cleland, J.; Forbes, J.; Gill, J.; et al. Occupation and risk of severe COVID-19: Prospective cohort study of 120 075 UK Biobank participants. Occup. Environ. Med. 2020, 78, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.A. BLUE-protocol and FALLS-protocol: Two applications of lung ultrasound in the critically ill. Chest 2015, 147, 1659–1670. [Google Scholar] [CrossRef]
- Sultan, L.R.; Sehgal, C.M. A Review of Early Experience in Lung Ultrasound in the Diagnosis and Management of COVID-19. Ultrasound Med. Biol. 2020, 46, 2530–2545. [Google Scholar] [CrossRef]
- European Society of Radiology (ESR). ESR statement on portable ultrasound devices. Insights Imaging 2019, 10, 89. [Google Scholar] [CrossRef]
- Poggiali, E.; Dacrema, A.; Bastoni, D.; Tinelli, V.; Demichele, E.; Mateo Ramos, P.; Marciano, T.; Silva, M.; Vercelli, A.; Magnacavallo, A. Can Lung US Help Critical Care Clinicians in the Early Diagnosis of Novel Coronavirus (COVID-19) Pneumonia? Radiology 2020, 295, E6. [Google Scholar] [CrossRef]
- Manivel, V.; Lesnewski, A.; Shamim, S.; Carbonatto, G.; Govindan, T. CLUE: COVID-19 lung ultrasound in emergency department. Emerg. Med. Australas. 2020, 32, 694–696. [Google Scholar] [CrossRef]
- Dargent, A.; Chatelain, E.; Kreitmann, L.; Quenot, J.P.; Cour, M.; Argaud, L.; COVID-LUS study group. Lung ultrasound score to monitor COVID-19 pneumonia progression in patients with ARDS. PLoS ONE 2020, 15, e0236312. [Google Scholar] [CrossRef]
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.E.; et al. Proposal for International Standardization of the Use of Lung Ultrasound for Patients With COVID-19: A Simple, Quantitative, Reproducible Method. J. Ultrasound Med. 2020, 39, 1413–1419. [Google Scholar] [CrossRef]
- Deng, Q.; Zhang, Y.; Wang, H.; Chen, L.; Yang, Z.; Peng, Z.; Liu, Y.; Feng, C.; Huang, X.; Jiang, N.; et al. Semiquantitative lung ultrasound scores in the evaluation and follow-up of critically ill patients with COVID-19: A single-center study. Acad. Radiol. 2020, 27, 1363–1372. [Google Scholar] [CrossRef]
- Lichter, Y.; Topilsky, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Gal Oz, A.; Vine, J.; Goren, O.; Cohen, B.; et al. Lung ultrasound predicts clinical course and outcomes in COVID-19 patients. Intensive Care Med. 2020, 46, 1873–1883. [Google Scholar] [CrossRef]
- Buonsenso, D.; Piano, A.; Raffaelli, F.; Bonadia, N.; de Gaetano Donati, K.; Franceschi, F. Point-of-Care Lung Ultrasound findings in novel coronavirus disease-19 pnemoniae: A case report and potential applications during COVID-19 outbreak. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2776–2780. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.; Gebo, K. COVID-19: Management of adults with acute illness in the outpatient setting. In UpToDate; Post, T.W., Ed.; UpToDate: Waltham, MA, USA, 2023. [Google Scholar]
- Saraogi, A. Lung ultrasound: Present and future. Lung India 2015, 32, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Kopinski, H.; Davis, L. A—Lines—Normal Lung. Available online: http://www.thepocusatlas.com/lung/5l9jgyaszu0othj5tidg0miqxkmvyv (accessed on 7 May 2023).
- Taylor, T.; Meer, J.; Beck, S. Emergency Ultrasound: Lung Assessment. Lung ultrasound takes 2 to 3 minutes to perform and can help narrow down the differential in a patient with dyspnea. Emerg. Med. 2015, 47, 35–36. [Google Scholar]
- Buda, N.; Cylwik, J.; Mroz, K.; Rudzinska, R.; Dubik, P.; Malczewska, A.; Oraczewska, A.; Skoczynski, S.; Suska, A.; Gorecki, T.; et al. Lung Ultrasound Examination in Patients with SARS-CoV-2 Infection: Multicenter Study. J. Clin. Med. 2021, 10, 3255. [Google Scholar] [CrossRef]
- Akhbardeh, A.; Jacobs, M.A. Comparative analysis of nonlinear dimensionality reduction techniques for breast MRI segmentation. Med. Phys. 2012, 39, 2275–2289. [Google Scholar] [CrossRef]
- Otsu, N. A Threshold Selection Method from Gray-Level Histograms. IEEE Trans. Syst. Man Cybern. 1979, 9, 62–66. [Google Scholar] [CrossRef]
- Arthur, D.; Vassilvitskii, S. K-Means++: The Advantages of Careful Seeding. In Proceedings of the SODA 2007: Proceedings of the Eighteenth Annual ACM-SIAM Symposium on Discrete Algorithms, New Orleans, LO, USA, 7–9 January 2007; pp. 1027–1035. [Google Scholar]
- Meyer, F. Topographic distance and watershed lines. Signal Process. 1994, 38, 113–125. [Google Scholar] [CrossRef]
- Lehmann, G.; Legland, D. Efficient N-Dimensional Surface Estimation Using Crofton Formula and Run-Length Encoding. Available online: https://insight-journal.org/browse/publication/852 (accessed on 18 August 2022).
- Shoemake, K. Graphics Gems IV; Heckbert, P.S., Ed.; Morgan Kaufmann: Burlington, MA, USA, 1994. [Google Scholar]
- Macias, M.; Riscinti, M. Ultrasound in COVID-19. Available online: http://www.thepocusatlas.com/covid19 (accessed on 30 April 2023).
- Peng, Q.Y.; Wang, X.T.; Zhang, L.N.; Chinese Critical Care Ultrasound Study Group. Findings of lung ultrasonography of novel corona virus pneumonia during the 2019–2020 epidemic. Intensive Care Med. 2020, 46, 849–850. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Bellows, B.A.; Adedipe, A.A.; Totten, J.E.; Backlund, B.H.; Sajed, D. Perceived barriers in the use of ultrasound in developing countries. Crit. Ultrasound J. 2015, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Y.; He, Q.; Liao, H.; Luo, J. Quantitative Analysis of Pleural Line and B-Lines in Lung Ultrasound Images for Severity Assessment of COVID-19 Pneumonia. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2022, 69, 73–83. [Google Scholar] [CrossRef]
- Diaz-Escobar, J.; Ordonez-Guillen, N.E.; Villarreal-Reyes, S.; Galaviz-Mosqueda, A.; Kober, V.; Rivera-Rodriguez, R.; Lozano Rizk, J.E. Deep-learning based detection of COVID-19 using lung ultrasound imagery. PLoS ONE 2021, 16, e0255886. [Google Scholar] [CrossRef] [PubMed]
- Mento, F.; Perrone, T.; Fiengo, A.; Smargiassi, A.; Inchingolo, R.; Soldati, G.; Demi, L. Deep learning applied to lung ultrasound videos for scoring COVID-19 patients: A multicenter study. J. Acoust. Soc. Am. 2021, 149, 3626. [Google Scholar] [CrossRef]
- Roshankhah, R.; Karbalaeisadegh, Y.; Greer, H.; Mento, F.; Soldati, G.; Smargiassi, A.; Inchingolo, R.; Torri, E.; Perrone, T.; Aylward, S.; et al. Investigating training-test data splitting strategies for automated segmentation and scoring of COVID-19 lung ultrasound images. J. Acoust. Soc. Am. 2021, 150, 4118. [Google Scholar] [CrossRef]
- Barros, B.; Lacerda, P.; Albuquerque, C.; Conci, A. Pulmonary COVID-19: Learning Spatiotemporal Features Combining CNN and LSTM Networks for Lung Ultrasound Video Classification. Sensors 2021, 21, 5486. [Google Scholar] [CrossRef] [PubMed]
- Horry, M.J.; Chakraborty, S.; Paul, M.; Ulhaq, A.; Pradhan, B.; Saha, M.; Shukla, N. COVID-19 Detection Through Transfer Learning Using Multimodal Imaging Data. IEEE Access 2020, 8, 149808–149824. [Google Scholar] [CrossRef]
- Karnes, M.; Perera, S.; Adhikari, S.; Yilmaz, A. Adaptive Few-Shot Learning PoC Ultrasound COVID-19 Diagnostic System. In Proceedings of the 2021 IEEE Biomedical Circuits and Systems Conference (BioCAS), Berlin, Germany, 7–9 October 2021; pp. 1–6. [Google Scholar]
- Wang, J.; Yang, X.; Zhou, B.; Sohn, J.J.; Zhou, J.; Jacob, J.T.; Higgins, K.A.; Bradley, J.D.; Liu, T. Review of Machine Learning in Lung Ultrasound in COVID-19 Pandemic. J. Imaging 2022, 8, 65. [Google Scholar] [CrossRef]
- Hunter, T. Diagnostics, Monitoring, Drug Discovery: How AI Is Fighting COVID-19. Available online: https://builtin.com/artificial-intelligence/ai-coronavirus (accessed on 30 April 2023).
- Kameda, T.; Mizuma, Y.; Taniguchi, H.; Fujita, M.; Taniguchi, N. Point-of-care lung ultrasound for the assessment of pneumonia: A narrative review in the COVID-19 era. J. Med. Ultrason. 2021, 48, 31–43. [Google Scholar] [CrossRef]
- Safiri, S.; Carson-Chahhoud, K.; Noori, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Ahmadian Heris, J.; Ansarin, K.; Mansournia, M.A.; Collins, G.S.; Kolahi, A.A.; et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: Results from the Global Burden of Disease Study 2019. BMJ 2022, 378, e069679. [Google Scholar] [CrossRef] [PubMed]
- WHO. Pneumonia in Children. Available online: https://www.who.int/news-room/fact-sheets/detail/pneumonia (accessed on 20 March 2023).
- Giannelli, F.; Cozzi, D.; Cavigli, E.; Campolmi, I.; Rinaldi, F.; Giache, S.; Rogasi, P.G.; Miele, V.; Bartolucci, M. Lung ultrasound (LUS) in pulmonary tuberculosis: Correlation with chest CT and X-ray findings. J. Ultrasound 2022, 25, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.Q.; Zhang, W.W.; Sun, S.; Chen, X.M.; Yuan, S.F.; Gong, Z.H.; Liu, L. A simplified lung ultrasound for the diagnosis of interstitial lung disease in connective tissue disease: A meta-analysis. Arthritis Res. Ther. 2019, 21, 93. [Google Scholar] [CrossRef] [PubMed]
- Allen, B.; Dreyer, K.; Stibolt, R., Jr.; Agarwal, S.; Coombs, L.; Treml, C.; Elkholy, M.; Brink, L.; Wald, C. Evaluation and Real-World Performance Monitoring of Artificial Intelligence Models in Clinical Practice: Try It, Buy It, Check It. J. Am. Coll. Radiol. 2021, 18, 1489–1496. [Google Scholar] [CrossRef]
- Giovannetti, G.; De Michele, L.; De Ceglie, M.; Pierucci, P.; Mirabile, A.; Vita, M.; Palmieri, V.O.; Carpagnano, G.E.; Scardapane, A.; D’Agostino, C. Lung ultrasonography for long-term follow-up of COVID-19 survivors compared to chest CT scan. Respir. Med. 2021, 181, 106384. [Google Scholar] [CrossRef]
- Jacobs, M.A.; Akhbardeh, A. Multiparametric Non-Linear Dimension Reduction Methods and Systems Related Thereto. U.S. Patent 9,256,966 B2, 9 February 2016. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Finding | CLU Finding | Radiologist Finding |
|---|---|---|
| A-Lines | 12 | 12 |
| Patchy B-lines | 19 | 19 |
| Confluent B-lines | 17 | 17 |
| Thickened, Irregular Pleural Lines | 13 | 13 |
| Pleural Effusion | 6 | 6 |
| Subpleural Consolidations | 12 | 12 |
| Consolidations with Air Bronchogram | 9 | 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sagreiya, H.; Jacobs, M.A.; Akhbardeh, A. Automated Lung Ultrasound Pulmonary Disease Quantification Using an Unsupervised Machine Learning Technique for COVID-19. Diagnostics 2023, 13, 2692. https://doi.org/10.3390/diagnostics13162692
Sagreiya H, Jacobs MA, Akhbardeh A. Automated Lung Ultrasound Pulmonary Disease Quantification Using an Unsupervised Machine Learning Technique for COVID-19. Diagnostics. 2023; 13(16):2692. https://doi.org/10.3390/diagnostics13162692
Chicago/Turabian StyleSagreiya, Hersh, Michael A. Jacobs, and Alireza Akhbardeh. 2023. "Automated Lung Ultrasound Pulmonary Disease Quantification Using an Unsupervised Machine Learning Technique for COVID-19" Diagnostics 13, no. 16: 2692. https://doi.org/10.3390/diagnostics13162692