
Comparison of Ruptured Intracranial Aneurysms Identification Using Different Machine Learning Algorithms and Radiomics

Abstract
:1. Introduction
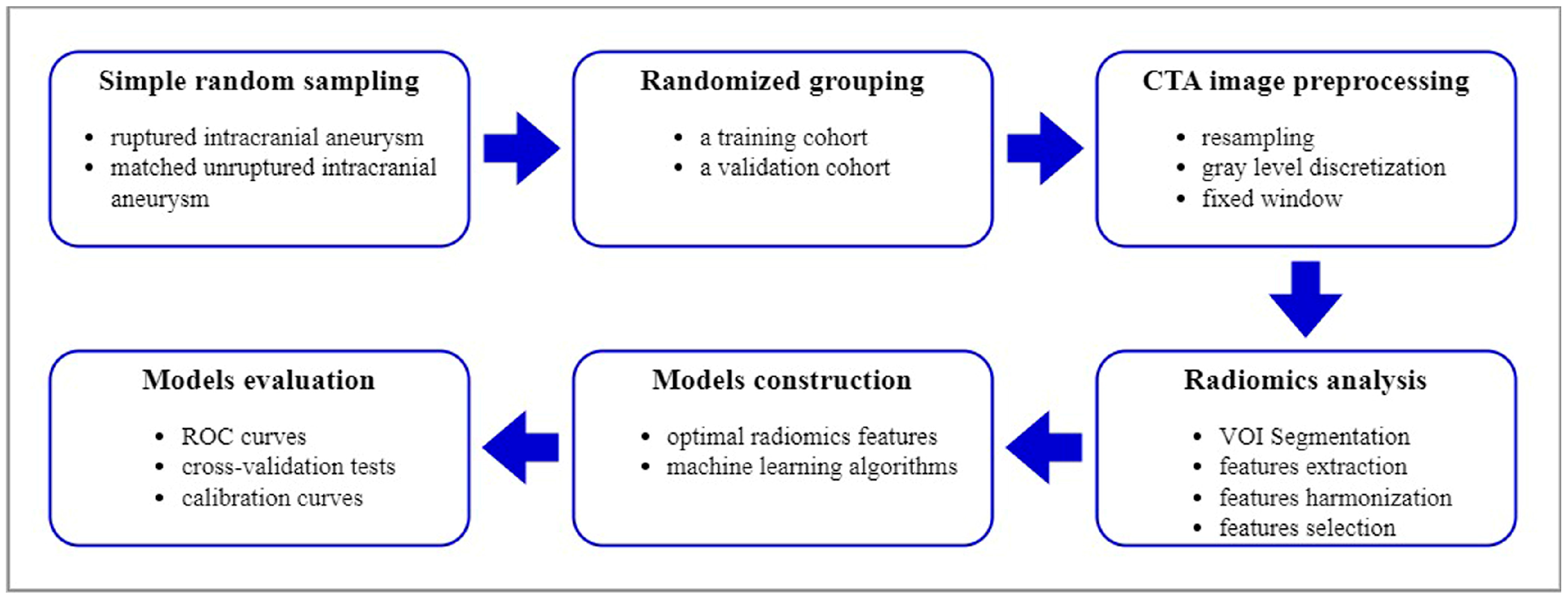
2. Materials and Methods
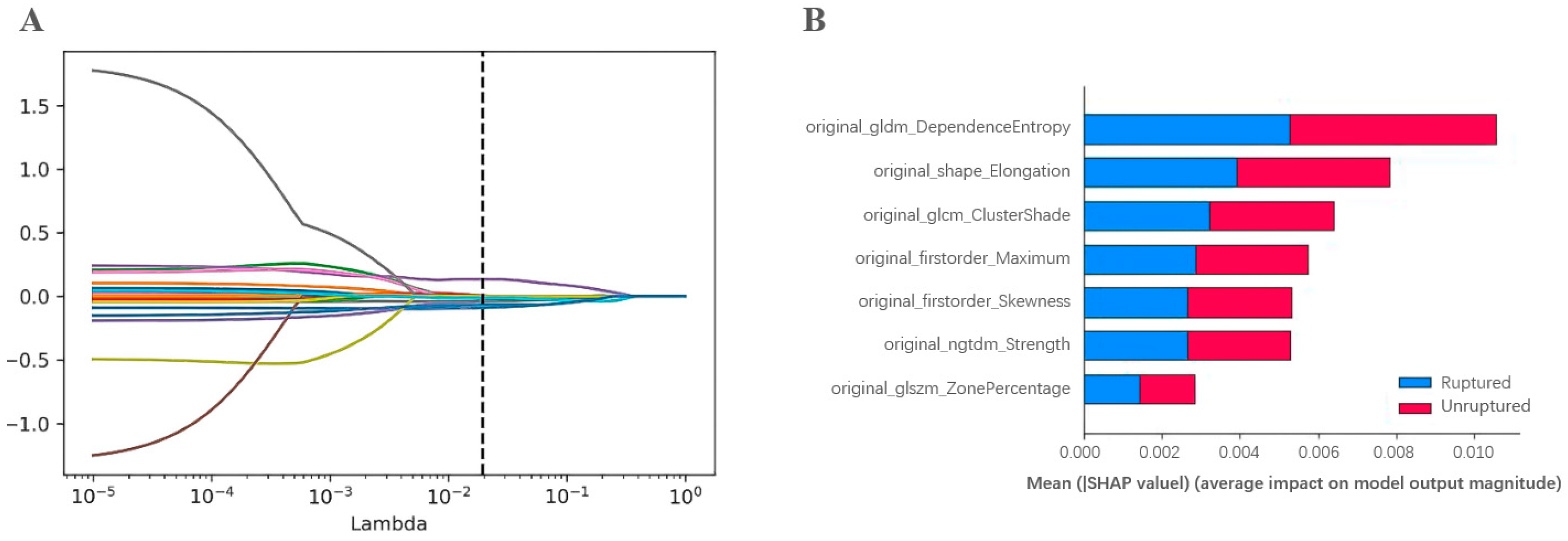
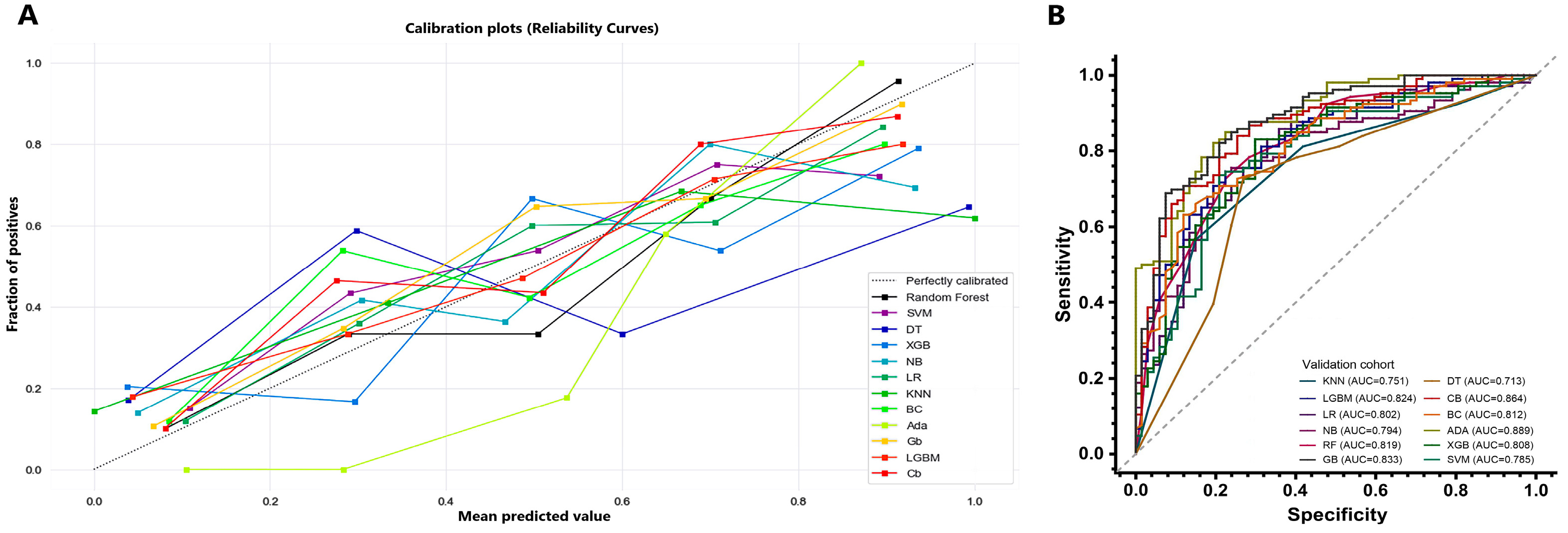
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thompson, B.G.; Brown, R.D., Jr.; Amin-Hanjani, S.; Broderick, J.P.; Cockroft, K.M.; Connolly, E.S., Jr.; Duckwiler, G.R.; Harris, C.C.; Howard, V.J.; Johnston, S.C.; et al. Guidelines for the Management of Patients With Unruptured Intracranial Aneurysms: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2015, 46, 2368–2400. [Google Scholar] [CrossRef] [Green Version]
- Vlak, M.H.; Algra, A.; Brandenburg, R.; Rinkel, G.J. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: A systematic review and meta-analysis. Lancet Neurol. 2011, 10, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Etminan, N.; Rinkel, G.J. Unruptured intracranial aneurysms: Development, rupture and preventive management. Nat. Rev. Neurol. 2016, 12, 699–713. [Google Scholar] [CrossRef] [PubMed]
- Korja, M.; Lehto, H.; Juvela, S. Lifelong rupture risk of intracranial aneurysms depends on risk factors: A prospective Finnish cohort study. Stroke 2014, 45, 1958–1963. [Google Scholar] [CrossRef] [Green Version]
- Greving, J.P.; Wermer, M.J.; Brown, R.D., Jr.; Morita, A.; Juvela, S.; Yonekura, M.; Ishibashi, T.; Torner, J.C.; Nakayama, T.; Rinkel, G.J.; et al. Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: A pooled analysis of six prospective cohort studies. Lancet Neurol. 2014, 13, 59–66. [Google Scholar] [CrossRef]
- Backes, D.; Rinkel, G.J.E.; Greving, J.P.; Velthuis, B.K.; Murayama, Y.; Takao, H.; Ishibashi, T.; Igase, M.; Agid, R.; Jääskeläinen, J.E.; et al. ELAPSS score for prediction of risk of growth of unruptured intracranial aneurysms. Neurology 2017, 88, 1600–1606. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Ou, C.; Chong, W.; Duan, C.; Zhang, X.; Morgan, M.; Qian, Y. A preliminary investigation of radiomics differences between ruptured and unruptured intracranial aneurysms. Eur. Radiol. 2020, 31, 2716–2725. [Google Scholar] [CrossRef]
- Zhu, D.; Chen, Y.; Zheng, K.; Chen, C.; Li, Q.; Zhou, J.; Jia, X.; Xia, N.; Wang, H.; Lin, B.; et al. Classifying Ruptured Middle Cerebral Artery Aneurysms With a Machine Learning Based, Radiomics-Morphological Model: A Multicentral Study. Front. Neurosci. 2021, 15, 721268. [Google Scholar] [CrossRef]
- Ludwig, C.G.; Lauric, A.; Malek, J.A.; Mulligan, R.; Malek, A.M. Performance of Radiomics derived morphological features for prediction of aneurysm rupture status. J. Neurointerv. Surg. 2021, 13, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Salmanpour, M.R.; Rezaeijo, S.M.; Hosseinzadeh, M.; Rahmim, A. Deep versus Handcrafted Tensor Radiomics Features: Prediction of Survival in Head and Neck Cancer Using Machine Learning and Fusion Techniques. Diagnostics 2023, 13, 1696. [Google Scholar] [CrossRef] [PubMed]
- Salmanpour, M.R.; Hosseinzadeh, M.; Rezaeijo, S.M.; Rahmim, A. Fusion-based tensor radiomics using reproducible features: Application to survival prediction in head and neck cancer. Comput. Methods Programs Biomed. 2023, 240, 107714. [Google Scholar] [CrossRef]
- Rezaeijo, S.M.; Jafarpoor Nesheli, S.; Fatan Serj, M.; Tahmasebi Birgani, M.J. Segmentation of the prostate, its zones, anterior fibromuscular stroma, and urethra on the MRIs and multimodality image fusion using U-Net model. Quant. Imaging Med. Surg. 2022, 12, 4786–4804. [Google Scholar] [CrossRef] [PubMed]
- Hosseinzadeh, M.; Gorji, A.; Fathi Jouzdani, A.; Rezaeijo, S.M.; Rahmim, A.; Salmanpour, M.R. Prediction of Cognitive Decline in Parkinson’s Disease Using Clinical and DAT SPECT Imaging Features, and Hybrid Machine Learning Systems. Diagnostics 2023, 13, 1691. [Google Scholar] [CrossRef]
- Bonaccorso, G. Machine Learning Algorithms; Packt Publishing Ltd.: Birmingham, UK, 2017. [Google Scholar]
- Burkov, A. The Hundred-Page Machine Learning Book; Andriy Burkov: Quebec City, QC, Canada, 2019. [Google Scholar]
- Gollapudi, S. Practical Machine Learning; Packt Publishing Ltd.: Birmingham, UK, 2016. [Google Scholar]
- Alwalid, O.; Long, X.; Xie, M.; Yang, J.; Cen, C.; Liu, H.; Han, P. CT Angiography-Based Radiomics for Classification of Intracranial Aneurysm Rupture. Front. Neurol. 2021, 12, 619864. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.; Even, A.J.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Xia, T.; Zhang, M.; Xia, N.; Liu, J.; Yang, Y. Radiomics in Stroke Neuroimaging: Techniques, Applications, and Challenges. Aging Dis. 2021, 12, 143–154. [Google Scholar] [CrossRef]
- An, X.; He, J.; Di, Y.; Wang, M.; Luo, B.; Huang, Y.; Ming, D. Intracranial Aneurysm Rupture Risk Estimation With Multidimensional Feature Fusion. Front. Neurosci. 2022, 16, 813056. [Google Scholar] [CrossRef]
- Charalambous, S.; Klontzas, M.E.; Kontopodis, N.; Ioannou, C.V.; Perisinakis, K.; Maris, T.G.; Damilakis, J.; Karantanas, A.; Tsetis, D. Radiomics and machine learning to predict aggressive type 2 endoleaks after endovascular aneurysm repair: A proof of concept. Acta Radiol. 2022, 63, 1293–1299. [Google Scholar] [CrossRef]
- Shi, Z.; Chen, G.; Mao, L.; Li, X.; Zhou, C.; Xia, S.; Zhang, Y.X.; Zhang, B.; Hu, B.; Lu, G.M.; et al. Machine Learning-Based Prediction of Small Intracranial Aneurysm Rupture Status Using CTA-Derived Hemodynamics: A Multicenter Study. Am. J. Neuroradiol. 2021, 42, 648–654. [Google Scholar] [CrossRef]
- Salimi Ashkezari, S.F.; Mut, F.; Slawski, M.; Cheng, B.; Yu, A.K.; White, T.G.; Woo, H.H.; Koch, M.J.; Amin-Hanjani, S.; Charbel, F.T.; et al. Prediction of bleb formation in intracranial aneurysms using machine learning models based on aneurysm hemodynamics, geometry, location, and patient population. J. Neurointerv. Surg. 2021, 14, 1002–1007. [Google Scholar] [CrossRef]
- Xiong, W.; Chen, T.; Li, J.; Xiang, L.; Zhang, C.; Xiang, L.; Li, Y.; Chu, D.; Wu, Y.; Jie, Q.; et al. Interpretable machine learning model to predict rupture of small intracranial aneurysms and facilitate clinical decision. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2022, 43, 6371–6379. [Google Scholar] [CrossRef]
- Viola, P. Rapid Object Detection using a Boosted Cascade of Simple Features. In Proceedings of the 2001 IEEE Computer Society Conference on Computer Vision and Pattern Recognition, CVPR 2001, Kauai, HI, USA, 8–14 December 2001. [Google Scholar]
- Vezhnevets, A.; Vezhnevets, V. (Eds.) Modest AdaBoost-Teaching AdaBoost to Generalize Better; Graphicon: Indianapolis, IN, USA, 2005. [Google Scholar]
- Schapire, R.E. Explaining Adaboost. Empirical Inference; Springer: Berlin/Heidelberg, Germany, 2013; pp. 37–52. [Google Scholar]
- Schapire, R.E. The boosting approach to machine learning: An overview. In Nonlinear Estimation and Classification; Springer: New York, NY, USA, 2003; pp. 149–171. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Training Cohort | p-Value | Validation Cohort | p-Value | ||
|---|---|---|---|---|---|---|
| Ruptured Aneurysm (n = 125) | Unruptured Aneurysm (n = 278) | Ruptured Aneurysm (n = 67) | Unruptured Aneurysm (n = 106) | |||
| Age, y, mean ± SD | 58.28 ± 12.04 | 64.12 ± 11.88 | <0.001 | 58.37 ± 11.76 | 64.23 ± 13.18 | 0.003 |
| Gender | 0.190 | 0.533 | ||||
| Male, n (%) | 45 (36.0) | 120 (43.2) | 27 (40.3) | 48 (45.3) | ||
| Female, n (%) | 80 (64.0) | 158 (56.8) | 40 (59.7) | 58 (54.7) | ||
| Hypertension, n (%) | 66 (52.8) | 177 (63.7) | 0.047 | 34 (50.7) | 69 (65.1) | 0.080 |
| aSAH history, n (%) | 1 (0.8) | 0 (0) | 0.310 | 0 (0) | 0 (0) | - |
| Aneurysm size, mm, median [IQR] | 4.8 [3.7, 6.5] | 2.6 [2.0, 3.7] | <0.001 | 4.9 [3.8, 6.8] | 2.6 [2.1, 3.5] | <0.001 |
| PHASES score, median [IQR] | 4.0 [2.0, 5.0] | 1.0 [1.0, 2.0] | <0.001 | 4.0 [1.0, 5.0] | 1.0 [0.8, 2.0] | <0.001 |
| Location | <0.001 | <0.001 | ||||
| ICA, n (%) | 54 (43.2) | 226 (81.3) | 29 (43.3) | 90 (84.9) | ||
| ACA/ACOM, n (%) | 32 (25.6) | 16 (5.8) | 18 (26.9) | 6 (5.7) | ||
| MCA, n (%) | 27 (21.6) | 21 (7.6) | 12 (17.9) | 5 (4.7) | ||
| PCOM/Posterior circulation, n (%) | 12 (9.6) | 15 (5.4) | 8 (11.9) | 5 (4.7) | ||
| Validation Cohorts | AUC | Sensitivity | Specificity | PPV | NPV | Predictive Accuracy |
|---|---|---|---|---|---|---|
| RF | 0.819 (0.754–0.883) | 0.552 (0.426–0.672) | 0.877 (0.796–0.930) | 0.740 (0.594–0.850) | 0.756 (0.669–0.827) | 0.751 (0.682–0.810) |
| SVM | 0.785 (0.713–0.856) | 0.552 (0.426–0.672) | 0.877 (0.796–0.930) | 0.740 (0.594–0.849) | 0.756 (0.669–0.827) | 0.751 (0.682–0.810) |
| DT | 0.713 (0.631–0.795) | 0.493 (0.370–0.616) | 0.811 (0.721–0.878) | 0.623 (0.479–0.749) | 0.717 (0.626–0.793) | 0.688 (0.615–0.752) |
| XGB | 0.808 (0.742–0.875) | 0.627 (0.500–0.739) | 0.849 (0.763–0.909) | 0.724 (0.589–0.830) | 0.783 (0.694–0.852) | 0.763 (0.694–0.821) |
| GNB | 0.794 (0.726–0.861) | 0.627 (0.500–0.739) | 0.811 (0.721–0.878) | 0.677 (0.545–0.787) | 0.775 (0.684–0.846) | 0.740 (0.670–0.800) |
| LR | 0.802 (0.733–0.870) | 0.552 (0.426–0.672) | 0.887 (0.807–0.938) | 0.755 (0.608–0.862) | 0.758 (0.671–0.828) | 0.757 (0.688–0.815) |
| KNN | 0.751 (0.676–0.826) | 0.582 (0.455–0.699) | 0.811 (0.721–0.878) | 0.661 (0.525–0.776) | 0.754 (0.663–0.828) | 0.722 (0.651–0.784) |
| BC | 0.812 (0.748–0.877) | 0.597 (0.470–0.713) | 0.849 (0.763–0.909) | 0.714 (0.576–0.823) | 0.769 (0.680–0.840) | 0.751 (0.682–0.810) |
| ADA | 0.889 (0.842–0.936) | 0.716 (0.591–0.817) | 0.868 (0.785–0.923) | 0.774 (0.647–0.867) | 0.829 (0.743–0.891) | 0.809 (0.744–0.861) |
| GB | 0.883 (0.833–0.934) | 0.657 (0.530–0.766) | 0.896 (0.818–0.945) | 0.800 (0.720–0.870) | 0.805 (0.720–0.870) | 0.804 (0.738–0.856) |
| LGBM | 0.824 (0.761–0.886) | 0.597 (0.470–0.713) | 0.868 (0.785–0.923) | 0.741 (0.601–0.846) | 0.773 (0.685–0.843) | 0.763 (0.694–0.821) |
| CB | 0.864 (0.809–0.919) | 0.627 (0.500–0.739) | 0.887 (0.807–0.938) | 0.778 (0.641–0.875) | 0.790 (0.704–0.857) | 0.786 (0.719–0.841) |
| Folds, Repeats | Scores | Area Under Curves |
|---|---|---|
| 1, 1 | 0.807 | 0.896 |
| 1, 2 | 0.781 | 0.863 |
| 1, 3 | 0.766 | 0.842 |
| 1, 4 | 0.807 | 0.879 |
| 1, 5 | 0.771 | 0.862 |
| 2, 1 | 0.833 | 0.898 |
| 2, 2 | 0.776 | 0.865 |
| 2, 3 | 0.844 | 0.904 |
| 2, 4 | 0.865 | 0.910 |
| 2, 5 | 0.813 | 0.918 |
| 3, 1 | 0.807 | 0.888 |
| 3, 2 | 0.833 | 0.898 |
| 3, 3 | 0.813 | 0.897 |
| 3, 4 | 0.807 | 0.873 |
| 3, 5 | 0.833 | 0.910 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, B.; Li, W.; Wu, X.; Zhong, W.; Wang, J.; Zhou, Y.; Huang, T.; Zhou, L.; Zhou, Z. Comparison of Ruptured Intracranial Aneurysms Identification Using Different Machine Learning Algorithms and Radiomics. Diagnostics 2023, 13, 2627. https://doi.org/10.3390/diagnostics13162627
Yang B, Li W, Wu X, Zhong W, Wang J, Zhou Y, Huang T, Zhou L, Zhou Z. Comparison of Ruptured Intracranial Aneurysms Identification Using Different Machine Learning Algorithms and Radiomics. Diagnostics. 2023; 13(16):2627. https://doi.org/10.3390/diagnostics13162627
Chicago/Turabian StyleYang, Beisheng, Wenjie Li, Xiaojia Wu, Weijia Zhong, Jing Wang, Yu Zhou, Tianxing Huang, Lu Zhou, and Zhiming Zhou. 2023. "Comparison of Ruptured Intracranial Aneurysms Identification Using Different Machine Learning Algorithms and Radiomics" Diagnostics 13, no. 16: 2627. https://doi.org/10.3390/diagnostics13162627