
Radiomics for the Detection of Active Sacroiliitis Using MR Imaging
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. Imaging Section
2.3. Segmentation and Feature Extraction
2.4. Feature Selection
2.5. Machine Learning
2.6. Statistical Analysis
3. Results
3.1. Selected Features
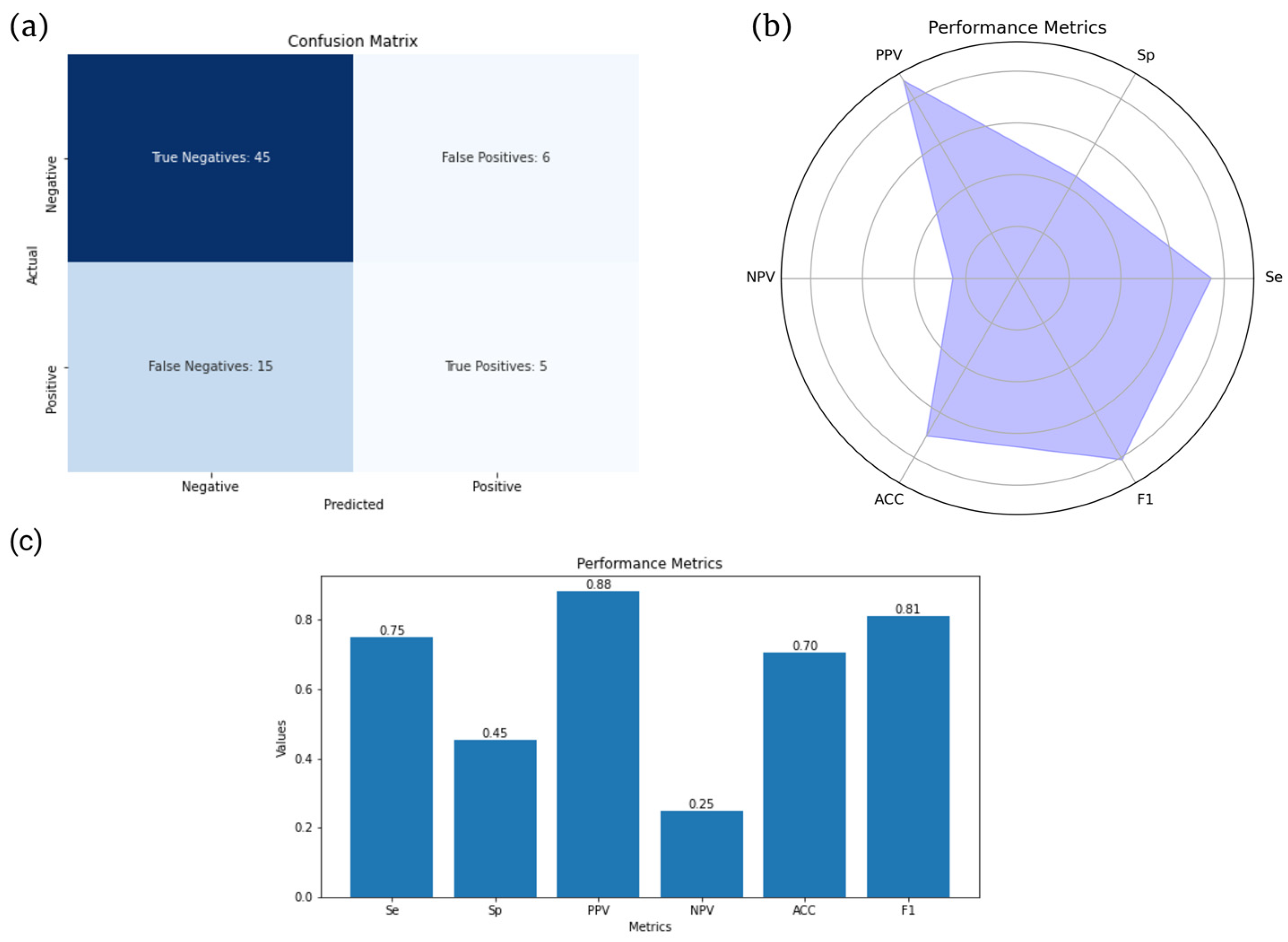
3.2. Model Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rudwaleit, M.; van der Heijde, D.; Landewe, R.; Listing, J.; Akkoc, N.; Brandt, J.; Braun, J.; Chou, C.T.; Collantes-Estevez, E.; Dougados, M.; et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): Validation and final selection. Ann. Rheum. Dis. 2009, 68, 777–783. [Google Scholar] [CrossRef]
- Van Der Linden Hans Valkenburg, S.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum 1984, 27, 361–368. [Google Scholar]
- Khmelinskii, N.; Regel, A.; Baraliakos, X. The role of imaging in diagnosing axial spondyloarthritis. Front. Med. 2018, 5, 106. [Google Scholar] [CrossRef] [Green Version]
- Weaver, J.S.; Omar, I.; Mar, W.; Kauser, A.S.; Mlady, G.W.; Taljanovic, M. Magnetic resonance imaging of rheumatological diseases. Pol. J. Radiol. 2022, 87, e93–e112. [Google Scholar] [CrossRef]
- Diekhoff, T.; Lambert, R.; Hermann, K.G. MRI in axial spondyloarthritis: Understanding an ‘ASAS-positive MRI’ and the ASAS classification criteria. Skelet. Radiol. 2022, 51, 1721–1730. [Google Scholar] [CrossRef]
- Lorenzin, M.; Ortolan, A.; Felicetti, M.; Vio, S.; Favero, M.; Polito, P.; Lacognata, C.; Scapin, V.; Doria, A.; Ramonda, R. Spine and Sacroiliac Joints Lesions on Magnetic Resonance Imaging in Early Axial-Spondyloarthritis During 24-Months Follow-Up (Italian Arm of SPACE Study). Front. Immunol. 2020, 11, 936. [Google Scholar] [CrossRef]
- Bressem, K.K.; Adams, L.C.; Proft, F.; Hermann, K.G.A.; Diekhoff, T.; Spiller, L.; Niehues, S.M.; Makowski, M.R.; Hamm, B.; Protopopov, M.; et al. Deep Learning Detects Changes Indicative of Axial Spondyloarthritis at MRI of Sacroiliac Joints. Radiology 2022, 305, 655–665. [Google Scholar] [CrossRef]
- Van Der Heijde, D.; Ramiro, S.; Landewé, R.; Baraliakos, X.; van den Bosch, F.; Sepriano, A.; Regel, A.; Ciurea, A.; Dagfinrud, H.; Dougados, M.; et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann. Rheum. Dis. 2017, 76, 978–991. [Google Scholar] [CrossRef]
- Polly, D.W.; Cher, D.J.; Wine, K.D.; Whang, P.G.; Frank, C.J.; Harvey, C.F.; Lockstadt, H.; Glaser, J.A.; Limoni, R.P.; Sembrano, J.N. Randomized controlled trial of minimally invasive sacroiliac joint fusion using triangular titanium implants vs nonsurgical management for sacroiliac joint dysfunction: 12-month outcomes. Neurosurgery 2015, 77, 674–690. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef] [Green Version]
- Biorender. Available online: https://www.biorender.com (accessed on 27 July 2023).
- 3D Slicer. Available online: https://www.slicer.org (accessed on 27 July 2023).
- Slicer Radiomics. Available online: https://www.radiomics.io/slicerradiomics.html (accessed on 27 July 2023).
- Papanikolaou, N.; Matos, C.; Koh, D.M. How to develop a meaningful radiomic signature for clinical use in oncologic patients. Cancer Imaging 2020, 20, 33. [Google Scholar] [CrossRef]
- Standard Scaler. Available online: https://scikit-learn.org/stable/modules/generated/sklearn.preprocessing.StandardScaler.html (accessed on 27 May 2023).
- Berthelot, J.-M.; le Goff, B.; Maugars, Y.; Laredo, J.-D. Sacroiliac joint edema by MRI: Far more often mechanical than inflammatory? Jt. Bone Spine 2016, 83, 3–5. [Google Scholar] [CrossRef]
- Kepp, F.H.; Huber, F.A.; Wurnig, M.C.; Mannil, M.; Kaniewska, M.; Guglielmi, R.; Del Grande, F.; Guggenberger, R. Differentiation of inflammatory from degenerative changes in the sacroiliac joints by machine learning supported texture analysis. Eur. J. Radiol. 2021, 140, 109755. [Google Scholar] [CrossRef]
- Thakur, G.S.; Daigle, B.J.; Qian, M.; Dean, K.R.; Zhang, Y.; Yang, R.; Kim, T.-K.; Wu, X.; Li, M.; Lee, I.; et al. A Multimetric Evaluation of Stratified Random Sampling for Classification: A Case Study. IEEE Life Sci. Lett. 2016, 2, 43–46. [Google Scholar] [CrossRef]
- Boruta. Available online: https://pypi.org/project/Boruta/ (accessed on 25 May 2023).
- Degenhardt, F.; Seifert, S.; Szymczak, S. Evaluation of variable selection methods for random forests and omics data sets. Brief. Bioinform. 2019, 20, 492–503. [Google Scholar] [CrossRef] [Green Version]
- Python. Available online: https://docs.python.org/3/ (accessed on 23 July 2023).
- Faleiros, M.C.; Nogueira-Barbosa, M.H.; Dalto, V.; Junior, J.R.F.; Tenorio, A.P.M.; Luppino-Assad, R.; Louzada-Junior, P.; Rangayyan, R.M.; De Azevedo-Marques, P.M. Machine learning techniques for computer-aided classification of active inflammatory sacroiliitis in magnetic resonance imaging. Adv. Rheumatol. 2020, 60, 25. [Google Scholar] [CrossRef]
- Hong, J.H.; Jung, J.-Y.; Jo, A.; Nam, Y.; Pak, S.; Lee, S.-Y.; Park, H.; Lee, S.E.; Kim, S. Development and validation of a radiomics model for differentiating bone islands and osteoblastic bone metastases at abdominal CT. Radiology 2021, 299, 626–632. [Google Scholar] [CrossRef]
- Horvat, N.; Veeraraghavan, H.; Khan, M.; Blazic, I.; Zheng, J.; Capanu, M.; Sala, E.; Garcia-Aguilar, J.; Gollub, M.J.; Petkovska, I. Mr imaging of rectal cancer: Radiomics analysis to assess treatment response after neoadjuvant therapy. Radiology 2018, 287, 833–843. [Google Scholar] [CrossRef] [Green Version]
- Klontzas, M.E.; Manikis, G.C.; Nikiforaki, K.; Vassalou, E.E.; Spanakis, K.; Stathis, I.; Kakkos, G.A.; Matthaiou, N.; Zibis, A.H.; Marias, K.; et al. Radiomics and machine learning can differentiate transient osteoporosis from avascular necrosis of the hip. Diagnostics 2021, 11, 1686. [Google Scholar] [CrossRef]
- Xu, X.; Zhang, J.; Yang, K.; Wang, Q.; Chen, X.; Xu, B. Prognostic prediction of hypertensive intracerebral hemorrhage using CT radiomics and machine learning. Brain Behav. 2021, 11, e02085. [Google Scholar] [CrossRef]
- Numpy. Available online: https://numpy.org (accessed on 27 May 2023).
- Matplotlib. Available online: https://matplotlib.org (accessed on 27 May 2023).
- XGBoost. Available online: https://xgboost.readthedocs.io/en/stable/tutorials/model.html (accessed on 25 May 2023).
- Rudwaleit, M.; Jurik, A.G.; A Hermann, K.-G.; Landewe, R.; van der Heijde, D.; Baraliakos, X.; Marzo-Ortega, H.; Ostergaard, M.; Braun, J.; Sieper, J. Defining active sacroiliitis on magnetic resonance imaging (MRI) for classification of axial spondyloarthritis: A consensual approach by the ASAS/OMERACT MRI group. Ann. Rheum Dis. 2009, 68, 1520–1527. [Google Scholar] [CrossRef]
- Mandl, P.; Navarro-Compán, V.; Terslev, L.; Aegerter, P.; Van Der Heijde, D.; D’Agostino, M.A.; Baraliakos, X.; Pedersen, S.J.; Jurik, A.G.; Naredo, E.; et al. EULAR recommendations for the use of imaging in the diagnosis and management of spondyloarthritis in clinical practice. Ann. Rheum. Dis. 2015, 74, 1327–1339. [Google Scholar] [CrossRef]
- Ramachandran, A.; Fox, T.; Wolfson, A.; Banks, J.; Subhawong, T.K. Superficial fibromatosis: MRI radiomics and T2 mapping correlate with treatment response. Magn. Reson. Imaging 2021, 81, 53–59. [Google Scholar] [CrossRef]
- Althoff, C.E.; Feist, E.; Burova, E.; Eshed, I.; Bollow, M.; Hamm, B.; Hermann, K.-G.A. Magnetic resonance imaging of active sacroiliitis: Do we really need gadolinium? Eur. J. Radiol. 2009, 71, 232–236. [Google Scholar] [CrossRef]
- Van Onna, M.; Van Tubergen, A.; Van Der Heijde, D.; Jurik, A.G.; Landewé, R. Gadolinium contrast-enhanced MRI sequence does not have an incremental value in the assessment of sacroiliitis in patients with early inflammatory back pain by using MRI in combination with pelvic radiographs: A 2-year follow-up study. Clin. Exp. Rheumatol. 2014, 32, 225–230. [Google Scholar]
- Sung, S.; Kim, H.S.; Kwon, J.W. MRI assessment of sacroiliitis for the diagnosis of axial spondyloarthropathy: Comparison of fat-saturated T2, STIR and contrast-enhanced sequences. Br. J. Radiol. 2017, 90, 20170090. [Google Scholar] [CrossRef]
- Tenório, A.P.M.; Faleiros, M.C.; Junior, J.R.F.; Dalto, V.F.; Assad, R.L.; Louzada-Junior, P.; Yoshida, H.; Nogueira-Barbosa, M.H.; de Azevedo-Marques, P.M. A study of MRI-based radiomics biomarkers for sacroiliitis and spondyloarthritis. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 1737–1748. [Google Scholar] [CrossRef]
- Ye, L.; Miao, S.; Xiao, Q.; Liu, Y.; Tang, H.; Li, B.; Liu, J.; Chen, D. A predictive clinical-radiomics nomogram for diagnosing of axial spondyloarthritis using MRI and clinical risk factors. Rheumatology 2022, 61, 1440–1447. [Google Scholar] [CrossRef]
- D’Antonoli, T.A.; Mercaldo, N.D. Obsolescence of nomograms in radiomics research. Eur. Radiol. 2023. [CrossRef]
- Zheng, M.; Miao, S.; Chen, D.; Yao, F.; Xiao, Q.; Zhu, G.; Pan, C.; Lei, T.; Ye, C.; Yang, Y.; et al. Can radiomics replace the SPARCC scoring system in evaluating bone marrow edema of sacroiliac joints in patients with axial spondyloarthritis? Clin. Rheumatol. 2023, 42, 1675–1682. [Google Scholar] [CrossRef]
- Maksymowych, W.P.; Mallon, C.; Morrow, S.; Shojania, K.; Olszynski, W.P.; Wong, R.L.; Sampalis, J.; Conner-Spady, B. Development and validation of the Spondyloarthritis Research Consortium of Canada (SPARCC) Enthesitis Index. Ann. Rheum. Dis. 2009, 68, 948–953. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification Model | AUC-ROC | 95% CI |
|---|---|---|
| Logistic Regression | 0.61 | 0.47–0.75 |
| Support Vector Machine | 0.61 | 0.48–0.75 |
| Random Forest | 0.66 | 0.52–0.79 |
| Extreme Gradient Boosting | 0.71 | 0.58–0.84 |
| Study Details | Kepp et al. [17] | Faleiros et al. [22] | Ye et al. [37] | Current Study |
|---|---|---|---|---|
| No. of participants | 90 | 56 | 638 | 177 |
| MRI sequences | T1W-CE, STIR(T2W) * | STIR (T2W) | T2W-FS ** | STIR (T2W), PD-FS *** |
| Positive/negative cases | 33% | 43% | 67% | 26% |
| Methodology | Feature-based ML | Feature-based ML | Feature-based ML | Feature-based ML |
| Classification models | Log Reg | SVM, k-NN, ANN | Multivariate Log Reg | Log Reg, SVM, RF, XGBoost |
| Optimal performance (AUC or accuracy in validation set) | 0.89 | 0.80 | 0.90 | 0.71 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triantafyllou, M.; Klontzas, M.E.; Koltsakis, E.; Papakosta, V.; Spanakis, K.; Karantanas, A.H. Radiomics for the Detection of Active Sacroiliitis Using MR Imaging. Diagnostics 2023, 13, 2587. https://doi.org/10.3390/diagnostics13152587
Triantafyllou M, Klontzas ME, Koltsakis E, Papakosta V, Spanakis K, Karantanas AH. Radiomics for the Detection of Active Sacroiliitis Using MR Imaging. Diagnostics. 2023; 13(15):2587. https://doi.org/10.3390/diagnostics13152587
Chicago/Turabian StyleTriantafyllou, Matthaios, Michail E. Klontzas, Emmanouil Koltsakis, Vasiliki Papakosta, Konstantinos Spanakis, and Apostolos H. Karantanas. 2023. "Radiomics for the Detection of Active Sacroiliitis Using MR Imaging" Diagnostics 13, no. 15: 2587. https://doi.org/10.3390/diagnostics13152587