
Optimization of Revision Hip Arthroplasty Workflow by Means of Detailed Pre-Surgical Planning Using Computed Tomography Data, Open-Source Software and Three-Dimensional-Printed Models

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Information
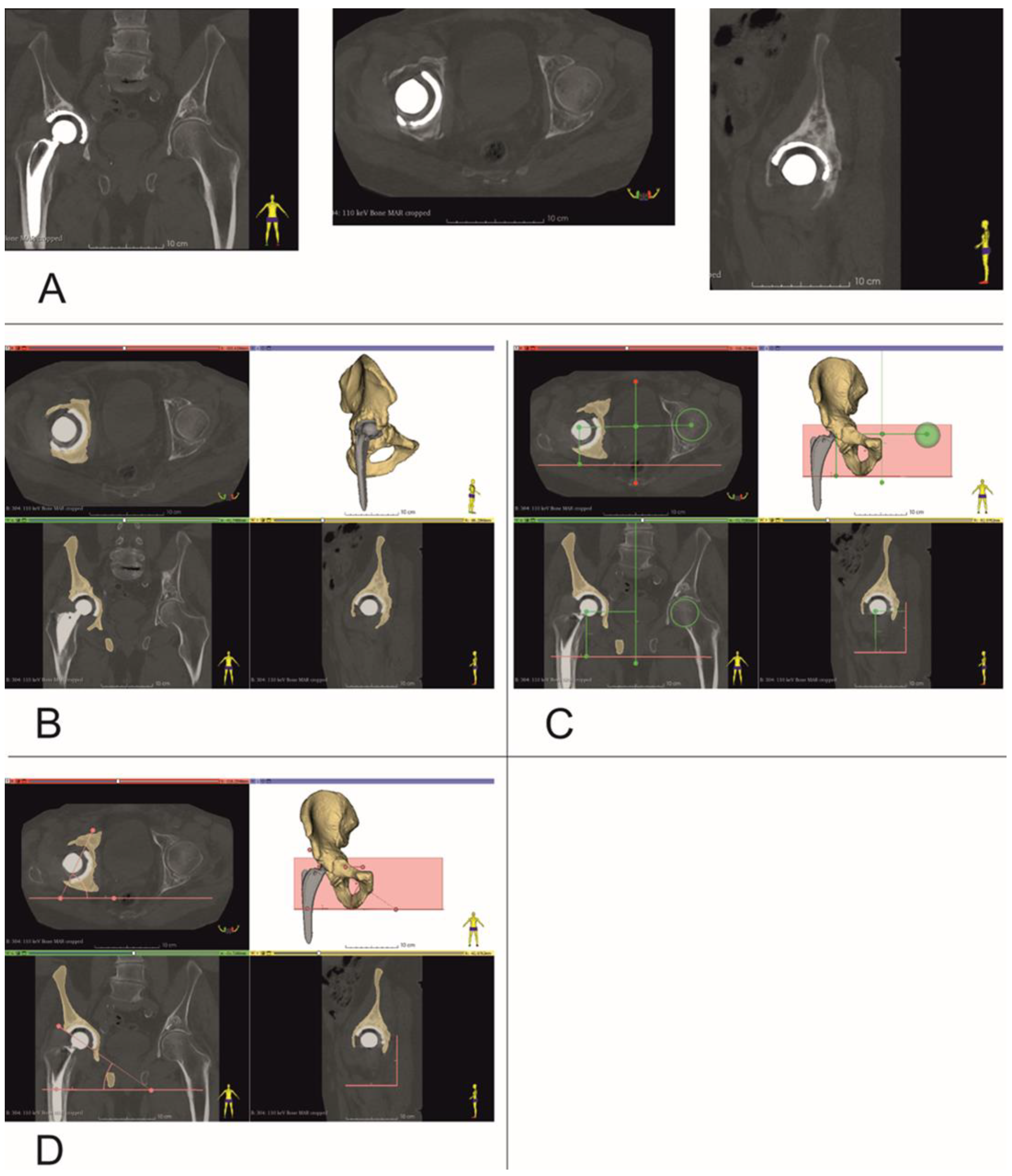
2.2. Determining Center of Rotation, Inclination and Anteversion Angles
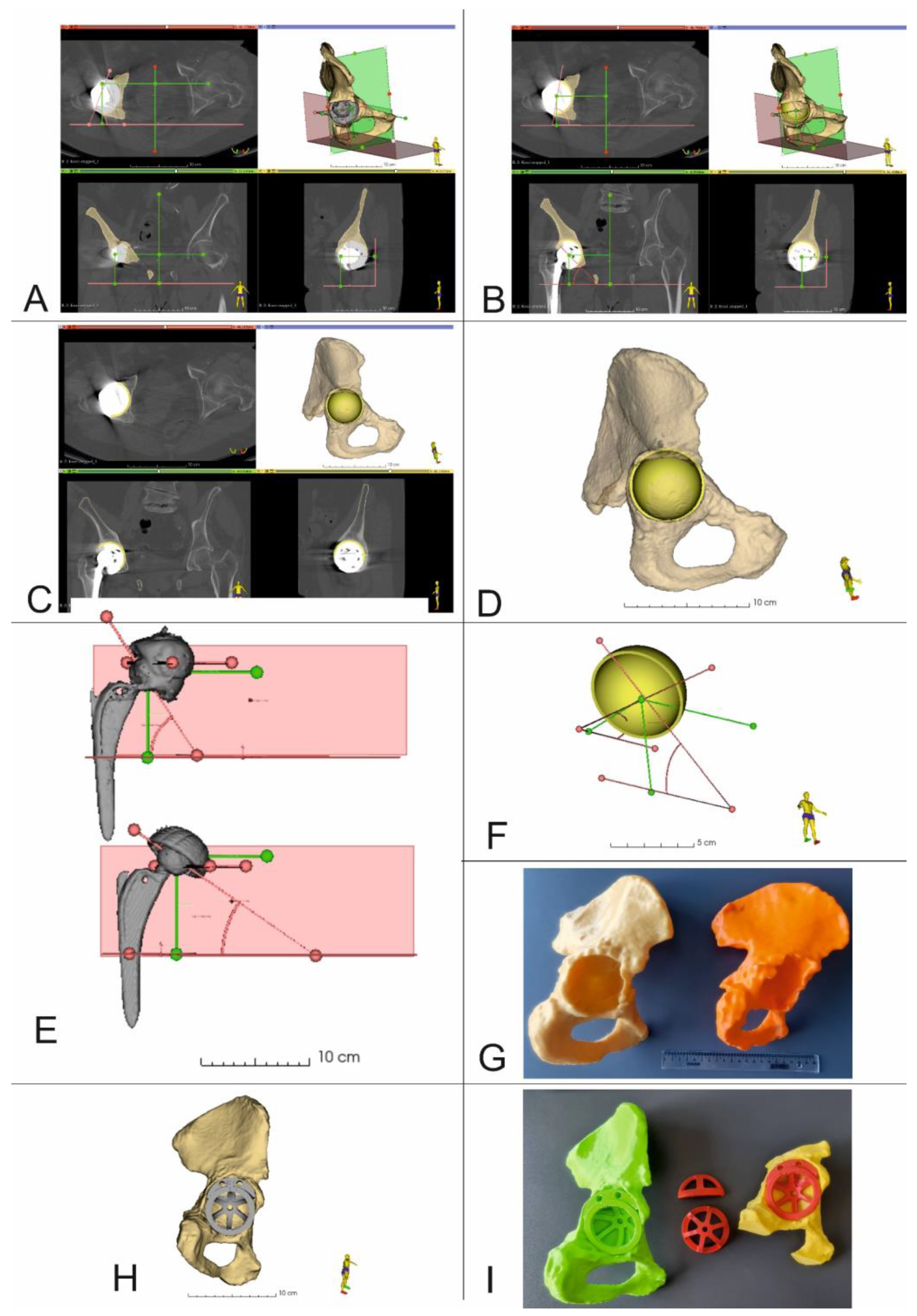
2.3. 3D Virtual Models of Acetabular Cups
2.4. Virtual Presurgical Planning and Post-Op Assessment of the Position of the Acetabular Cup
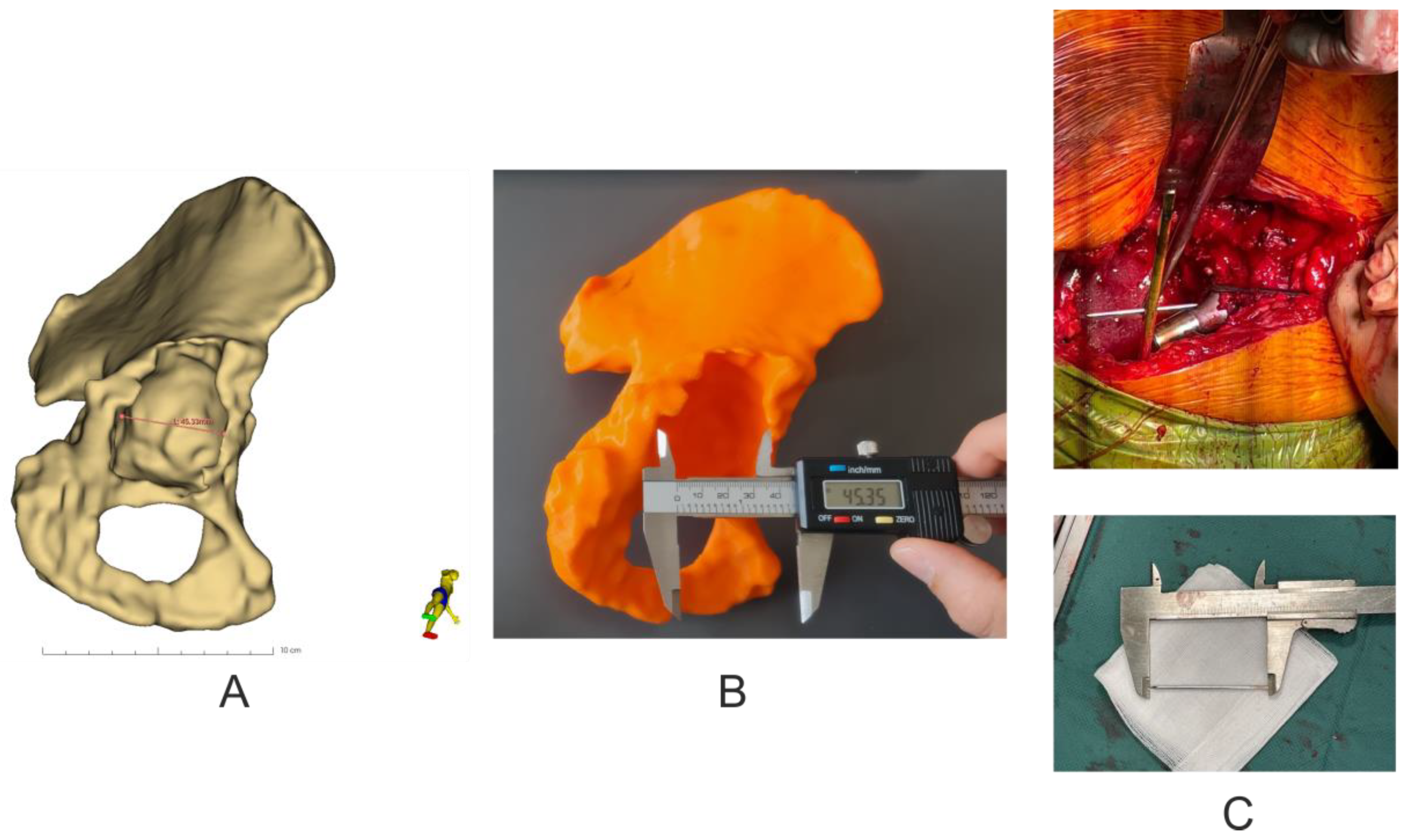
2.5. 3D Printing of Pelvic Models
2.6. Accuracy Analysis of 3D Models
2.7. Statistical Analysis
3. Results
3.1. Revision Acetabular Cup Sizes, Number and Size of Fixing Screws
3.2. Center of Rotation Position (Supplementary Tables S1 and S3) and Accuracy Analysis of 3D Models (Table 3)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Information about Types of Defect (Paprosky Classification) | 3D Virtual Models Measurement/ 3D Model Measurement Results mm (% Difference) | 3D Model Measurement/ Pelvis of Patient Measurement Results mm (% Difference) | 3D Virtual Model Measurement/ Pelvis of Patient Measurement Results mm (% Difference) |
|---|---|---|---|
| Patient 1 (Paprosky IIB) | −0.15/99.66 | 0.25/100.56 | 0.10/100.23 |
| Patient 2 (Paprosky IIC) | −0.04/99.92 | 0.10/100.19 | 0.06/100.12 |
| Patient 3 (Paprosky IIB) | −0.11/99.80 | 0.16/100.30 | 0.05/100.09 |
| Patient 4 (Paprosky IIA) | −0.70/98.59 | 1.50/103.12 | 0.80/101.67 |
| Patient 5 (Paprosky IIB) | −0.21/99.63 | 0.81/101.45 | 0.60/101.07 |
| Patient 6 (Paprosky IIA) | 0.05/100.09 | 0.51/100.93 | 0.56/101.02 |
| Patient 7 (Paprosky IIC) | 0.21/100.36 | 0.40/99.32 | −0.19/99.67 |
| Patient 8 (Paprosky IIA) | −0.05/99.91 | 0.14/99.76 | −0.19/99.67 |
| Patient 9 (Paprosky IIB) | −0.15/99.74 | 0.04/99.93 | −0.19/99.68 |
| Patient 10 (Paprosky IIIA) | −0.03/99.94 | 0.04/99.91 | −0.07/99.85 |
| mean ± SD | −0.12 ± 0.24/99.76 ± 0.47 | 0.27 ± 0.55/100.55 ± 1.09 | 0.15 ± 0.37/100.31 ± 0.70 |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moralidou, M.; Di Laura, A.; Henckel, J.; Hothi, H.; Hart, A.J. Three-dimensional pre-operative planning of primary hip arthroplasty: A systematic literature review. EFORT Open Rev. 2020, 5, 845–855. [Google Scholar] [CrossRef]
- Kuijpers, M.F.L.; Hannink, G.; van Steenbergen, L.N.; Schreurs, B.W. Outcome of revision hip arthroplasty in patients younger than 55 years: An analysis of 1,037 revisions in the Dutch Arthroplasty Register. Acta Orthop. 2020, 91, 165–170. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-W.; Won, S.-H.; Moon, S.-Y.; Lee, Y.-K.; Ha, Y.-C.; Koo, K.-H. Burden and future projection of revision Total hip Arthroplasty in South Korea. BMC Musculoskelet. Disord. 2021, 22, 375. [Google Scholar] [CrossRef] [PubMed]
- Komorowski, P.; Sokołowska, P.; Siatkowska, M.; Elgalal, M.; Rosowski, M.; Makowski, K.; Lipińska, L.; Leszczewicz, M.; Styczyński, A.; Fogel, K.; et al. Designing laser-modified surface structures on titanium alloy custom medical implants using a hybrid manufacturing technology. J. Biomed. Mater. Res. 2020, 1, 11. [Google Scholar] [CrossRef]
- Komorowski, P.; Siatkowska, M.; Kamińska, M.; Jakubowski, W.; Walczyńska, M.; Walkowiak-Przybyło, M.; Szymański, W.; Piersa, K.; Wielowski, P.; Sokołowska, P.; et al. Comprehensive Biological Evaluation of Biomaterials Used in Spinal and Orthopedic Surgery. Materials 2020, 13, 4769. [Google Scholar] [CrossRef]
- Jamari, J.; Ammarullah, M.I.; Saad, A.P.M.; Syahrom, A.; Uddin, M.; van der Heide, E.; Basri, H. The Effect of Bottom Profile Dimples on the Femoral Head on Wear in Metal-on-Metal Total Hip Arthroplasty. J. Funct. Biomater. 2021, 12, 38. [Google Scholar] [CrossRef] [PubMed]
- Ammarullah, M.I.; Hartono, R.; Supriyono, T.; Santoso, G.; Sugiharto, S.; Permana, M.S. Polycrystalline Diamond as a Potential Material for the Hard-on-Hard Bearing of Total Hip Prosthesis: Von Mises Stress Analysis. Biomedicines 2023, 11, 951. [Google Scholar] [CrossRef]
- Tauviqirrahman, M.; Ammarullah, M.I.; Jamari, J.; Saputra, E.; Winarni, T.I.; Kurniawan, F.D.; Shiddiq, S.A.; van der Heide, E. Analysis of contact pressure in a 3D model of dual-mobility hip joint prosthesis under a gait cycle. Sci. Rep. 2023, 13, 3564. [Google Scholar] [CrossRef]
- Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Wibowo, D.B.; Kurdi, O.; Tauviqirrahman, M.; Jamari, J. Minimizing Risk of Failure from Ceramic-on-Ceramic Total Hip Prosthesis by Selecting Ceramic Materials Based on Tresca Stress. Sustainability 2022, 14, 13413. [Google Scholar] [CrossRef]
- Rajpura, A.; Asle, S.G.; Selmi, T.A.S.; Board, T. The accuracy of restoration of femoral head centre of rotation in the anteroposterior plane after uncemented total hip arthroplasty. Bone Jt. Res. 2022, 11, 180–188. [Google Scholar] [CrossRef]
- Zhang, H.; Guan, J.; Chen, X.; Ma, X.; Zhao, J.; Zhou, J. Restoring Rotation Center in Total Hip Arthroplasty for Developmental Dysplasia of the Hip with the Assistance of Three Dimensional Printing Technology: A Pilot Study. Orthop. Surg. 2022, 14, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Meermans, G.; Van Doorn, J.; Kats, J.-J. Restoration of the centre of rotation in primary total hip arthroplasty. Bone Jt. J. 2016, 98, 1597–1603. [Google Scholar] [CrossRef] [Green Version]
- Durand-Hill, M.; Henckel, J.; Satchithananda, K.; Sabah, S.; Hua, J.; Hothi, H.; Langstaff, R.J.; Skinner, J.; Hart, A. Calculating the hip center of rotation using contralateral pelvic anatomy. J. Orthop. Res. 2016, 34, 1077–1083. [Google Scholar] [CrossRef] [Green Version]
- Olmedo-Garcia, N.; Sevilla, A. Comparative study of accuracy of Ranawat’s and Pierchon’s methods to determine hip centre with informatics tools. HIP Int. 2010, 20 (Suppl. S7), 48–51. [Google Scholar] [CrossRef]
- Memon, A. Epidemiology of gynecological cancers. In Gynaecological Oncology; Shafi, M., Earl, H., Tan, L., Eds.; Cambridge University Press: Cambridge, UK, 2009; pp. 1–14. [Google Scholar] [CrossRef]
- Leardini, A.; Cappozzo, A.; Catani, F.; Toksvig-Larsen, S.; Petitto, A.; Sforza, V.; Cassanelli, G.; Giannini, S. Validation of a functional method for the estimation of hip joint centre location. J. Biomech. 1999, 32, 99–103. [Google Scholar] [CrossRef]
- Sangeux, M.; Peters, A.; Baker, R. Hip joint centre localization: Evaluation on normal subjects in the context of gait analysis. Gait Posture 2011, 34, 324–328. [Google Scholar] [CrossRef]
- Piazza, S.J.; Erdemir, A.; Okita, N.; Cavanagh, P.R. Assessment of the functional method of hip joint center location subject to reduced range of hip motion. J. Biomech. 2004, 37, 349–356. [Google Scholar] [CrossRef]
- Ehrig, R.M.; Taylor, W.R.; Duda, G.N.; Heller, M.O. A survey of formal methods for determining the centre of rotation of ball joints. J. Biomech. 2006, 39, 2798–2809. [Google Scholar] [CrossRef]
- Mehrotra, D.; Markus, A.F. Emerging simulation technologies in global craniofacial surgical training. J. Oral Biol. Craniofacial Res. 2021, 11, 486–499. [Google Scholar] [CrossRef]
- Zhuang, Y.; Zhou, M.; Liu, S.; Wu, J.; Wang, R.; Chen, C. Effectiveness of personalized 3D printed models for patient education in degenerative lumbar disease. Patient Educ. Couns. 2019, 102, 10. [Google Scholar] [CrossRef]
- Chen, J.V.; Dang, A.B.C.; Dang, A. Comparing cost and print time estimates for six commercially-available 3D printers obtained through slicing software for clinically relevant anatomical models. 3D Print Med. 2021, 7, 1. [Google Scholar] [CrossRef]
- Andrzejewski, K.; Elgalal, M.; Komorowski, P.; Poszepczyński, J.; Rokita, B.; Domżalski, M. Fast-Track-Protocol for Optimization of Presurgical Planning in Acute Surgical Treatment of Acetabular Quadrilateral Plate Fractures Using 3D Printing Technology and Pre-Contoured Reconstruction Plates. Appl. Sci. 2022, 12, 3492. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Akilapa, O.; Pollet, V.; Van Dijk, L.; Reijman, M.; Castelein, R.M.C.; Sakkers, R.J.B. The medial approach open reduction for developmental dysplasia of the hip: Do the long-term outcomes validate this approach? A systematic review of the literature. J. Child. Orthop. 2014, 8, 387–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.; Pavlou, G.; Mújica-Mota, R.E.; Toms, A.D. The epidemiology of revision total knee and hip arthroplasty in England and Wales. Bone Jt. J. 2015, 97-B, 1076–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Gao, X.; Yang, G.; Zhang, Y. Using acetabular foss as a guide for anticipated inclination of ancemented cup in total hip replacement. Int. J. Clin. Exp. Med. 2015, 8, 181–187. [Google Scholar] [PubMed]
- Idrissi, M.E.; Elibrahim, A.; Shimi, M.; Elmirini, A. Acetubular orientation in total hip arthroplasty: The role of acetabular transvere ligment. Acta Ortop. Bras. 2016, 24, 267–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Archbold, H.A.P.; Mockford, B.; Molloy, D.; McConway, J.; Ogonda, L.; Beverland, D. The transverse acetabular ligament: An aid to orientation of the acetabular component during primary total hip replacement. J. Bone Jt. Surg. 2006, 88, 883–886. [Google Scholar] [CrossRef] [Green Version]
- Epstein, N.J.; Woolson, S.T.; Giori, N.J. Acetabular component positioning using the transverse acetabular ligament: Can you find it and does it help? Clin. Orthop. Relat. Res. 2011, 429, 412–416. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.S.; Wang, Z.Y.; Xiao, Y.Z.; Zhang, C.C.; Guan, J.Z.; Wu, M.; Zhou, X.S.; Liu, Z.H. Reconstruction of rotation center tn revision hip arthroplasty. Chin. J. Orthop. 2010, 31, 475–479. [Google Scholar]
- Zhang, H.; Zhou, J.; Guan, J.; Ding, H.; Wang, Z.; Dong, Q. How to restore rotation center in total hip arthroplasty for developmental dysplasia of the hip by recognizing the pathomorphology of acetabulum and Harris fossa? J. Orthop. Surg. Res. 2019, 14, 339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sculco, P.K.; Wright, T.; Malahias, M.-A.; Gu, A.; Bostrom, M.; Haddad, F.; Jerabek, S.; Bolognesi, M.; Fehring, T.; DellaValle, A.G.; et al. The Diagnosis and Treatment of Acetabular Bone Loss in Revision Hip Arthroplasty: An International Consensus Symposium. HSS J. 2022, 18, 8–41. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Chen, X.; Lin, B.; Ma, Y.; Kiao, J.X.; Zheng, Q. Three-diemensional technology assisted trabecular metal cup and augments postionnign in revision total hip arthroplasty with complex acetabular defects. J. Orthop. Surg. Res. 2019, 14, 431. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Liu, Q.; Fu, M.; Zhang, Z.; He, S.; Liao, W.; Kang, Y. Value of Computed Tomography-Based Three-Dimensional Pre-operative Planning in Cup Placement in Total Hip Arthroplasty With Dysplastic Acetabulum. J. Investig. Surg. 2019, 32, 607–613. [Google Scholar] [CrossRef]
- Ravi, P.; Chepelev, L.; Lawera, N.; Haque, K.M.A.; Chen, V.C.; Ali, A.; Rybicki, F.J. A systematic evaluation of medical 3D printing accuracy of multi-pathological anatomical models for surgical planning manufactured in elastic and rigid material using desktop inverted vat photopolymerization. Med. Phys. 2021, 48, 3223–3233. [Google Scholar] [CrossRef] [PubMed]
- Msallem, B.; Sharma, N.; Cao, S.; Halbeisen, F.S.; Zeilhofer, H.-F.; Thieringer, F.M. Evaluation of the Dimensional Accuracy of 3D-Printed Anatomical Mandibular Models Using FFF, SLA, SLS, MJ, and BJ Printing Technology. J. Clin. Med. 2020, 9, 817. [Google Scholar] [CrossRef] [Green Version]
- Brouwers, L.; Teutelink, A.; van Tilborg, F.A.J.B.; de Jongh, M.A.C.; Lansink, K.W.W.; Bemelman, M. Validation study of 3D-printed anatomical models using 2 PLA printers for preoperative planning in trauma surgery, a human cadaver study. Eur. J. Trauma Emerg. Surg. 2019, 45, 1013–1020. [Google Scholar] [CrossRef]
- Zeng, Y.; Lai, O.-J.; Shen, B.; Yang, J.; Zhou, Z.-K.; Kang, P.-D.; Pei, F.-X.; Zhou, X. Three-dimensional Computerized Preoperative Planning of Total Hip Arthroplasty with High-Riding Dislocation Developmental Dysplasia of the Hip. Orthop. Surg. 2014, 6, 95–102. [Google Scholar] [CrossRef]
- Kavalerskiy, G.M.; Murylev, V.Y.; Rukin, Y.A.; Elizarov, P.M.; Lychagin, A.V.; Tselisheva, E.Y. Three-Dimensional Models in Planning of Revision Hip Arthroplasty with Complex Acetabular Defects. Indian J. Orthop. 2018, 52, 625–630. [Google Scholar] [CrossRef]
- Ding, H.; Hai, Y.; Zhou, L.; Liu, Y.; Zhang, Y.; Han, C.; Zhang, Y. Clinical Application of Personalized Digital Surgical Planning and Precise Execution for Severe and Complex Adult Spinal Deformity Correction Utilizing 3D Printing Techniques. J. Pers. Med. 2023, 13, 602. [Google Scholar] [CrossRef] [PubMed]
- Cortese, A.; Spirito, F.; Claudio, P.P.; Muzio, L.L.; Ruggiero, A.; Gargiulo, M. Mandibular Reconstruction after Resection of Ameloblastoma by Custom-Made CAD/CAM Mandibular Titanium Prosthesis: Two Case Reports, Finite Element Analysis and Discussion of the Technique. Dent. J. 2023, 11, 106. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, T.N.; Hagens, M.J.; Veerman, H.; Yakar, D.; Mertens, L.S.; Heijmink, S.W.T.P.J.; van der Poel, H.G.; van Leeuwen, P.J.; Schoots, I.G.; van Dijk-de Haan, M.C. Prostate MRI for Improving Personalized Risk Prediction of Incontinence and Surgical Planning: The Role of Membranous Urethral Length Measurements and the Use of 3D Models. Life 2023, 13, 830. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, F.; Gligor, A.; Bataga, T. Structured Integration and Alignment Algorithm: A Tool for Personalized Surgical Treatment of Tibial Plateau Fractures. J. Pers. Med. 2021, 11, 190. [Google Scholar] [CrossRef] [PubMed]
- Innocenti, B.; Radyul, Y.; Bori, E. The Use of Artificial Intelligence in Orthopedics: Applications and Limitations of Machine Learning in Diagnosis and Prediction. Appl. Sci. 2022, 12, 10775. [Google Scholar] [CrossRef]
- Wu, D.; Zhi, X.; Liu, X.; Zhang, Y.; Chai, W. Utility of a novel integrated deep convolutional neural network for the segmentation of hip joint from computed tomography images in the preoperative planning of total hip arthroplasty. J. Orthop. Surg. Res. 2022, 17, 164. [Google Scholar] [CrossRef]
- Hiasa, Y.; Otake, Y.; Takao, M.; Ogawa, T.; Sugano, N.; Sato, Y. Automated muscle segmentation from clinical CT using Bayesian U-net for personalized muscu-loskeletal modeling. IEEE Trans. Med. Imaging 2019, 39, 1030–1040. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Lv, Y.; Wang, J.; Ma, F.; Du, Y.; Fan, X.; Wang, M.; Ke, J. Fully automated segmentation in temporal bone CT with neural network: A preliminary assessment study. BMC Med. Imaging 2021, 21, 166. [Google Scholar] [CrossRef]
- Chu, C.; Bai, J.; Wu, X.; Zheng, G. Fully automatic segmentation of hip CT images. In Computational Radiology for Orthopedic Interventions; Zheng, H., Li, S., Eds.; Springer: Cham, Switzerland, 2016; pp. 91–110. [Google Scholar]





| Computed Tomography Scanning Protocol | |
|---|---|
| Type of study | Single Phase, Non-contrast Enhanced Computed Tomography |
| Region | Pelvis |
| Patient position | Supine, lower limbs positioned symetrically |
| Image reconstruction | Reconstruction algorithms (Kernels): GE: Standard, Bone, Bone Plus; Siemens: B30f, B30s, B60s, B70s; |
| Slice Thickness | ≤1.0 mm (isometric voxel) |
| Resolution | 512 × 512 |
| Pitch | ≤1.0 |
| Gantry Tilt Angle | 0° |
| Data Format | Uncompressed DICOM files |
| 3D Printing Parameters | |
|---|---|
| Printing temperature | 205 °C |
| Build plate temperature | 60 °C |
| Layer high | 0.2 mm |
| Infill | 60% |
| Support material | Polyvinyl alcohol (PVA) (Ultimaker B.V, Utrecht, The Netherlands) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrzejewski, K.; Domżalski, M.; Komorowski, P.; Poszepczyński, J.; Rokita, B.; Elgalal, M. Optimization of Revision Hip Arthroplasty Workflow by Means of Detailed Pre-Surgical Planning Using Computed Tomography Data, Open-Source Software and Three-Dimensional-Printed Models. Diagnostics 2023, 13, 2516. https://doi.org/10.3390/diagnostics13152516
Andrzejewski K, Domżalski M, Komorowski P, Poszepczyński J, Rokita B, Elgalal M. Optimization of Revision Hip Arthroplasty Workflow by Means of Detailed Pre-Surgical Planning Using Computed Tomography Data, Open-Source Software and Three-Dimensional-Printed Models. Diagnostics. 2023; 13(15):2516. https://doi.org/10.3390/diagnostics13152516
Chicago/Turabian StyleAndrzejewski, Krzysztof, Marcin Domżalski, Piotr Komorowski, Jan Poszepczyński, Bożena Rokita, and Marcin Elgalal. 2023. "Optimization of Revision Hip Arthroplasty Workflow by Means of Detailed Pre-Surgical Planning Using Computed Tomography Data, Open-Source Software and Three-Dimensional-Printed Models" Diagnostics 13, no. 15: 2516. https://doi.org/10.3390/diagnostics13152516