
Reagent Effects on the Activated Partial Thromboplastin Time Clot Waveform Analysis: A Multi-Centre Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inter-Lot Variation
2.2. Institutions Involved and Sample Preparation
2.3. Analyzers Used
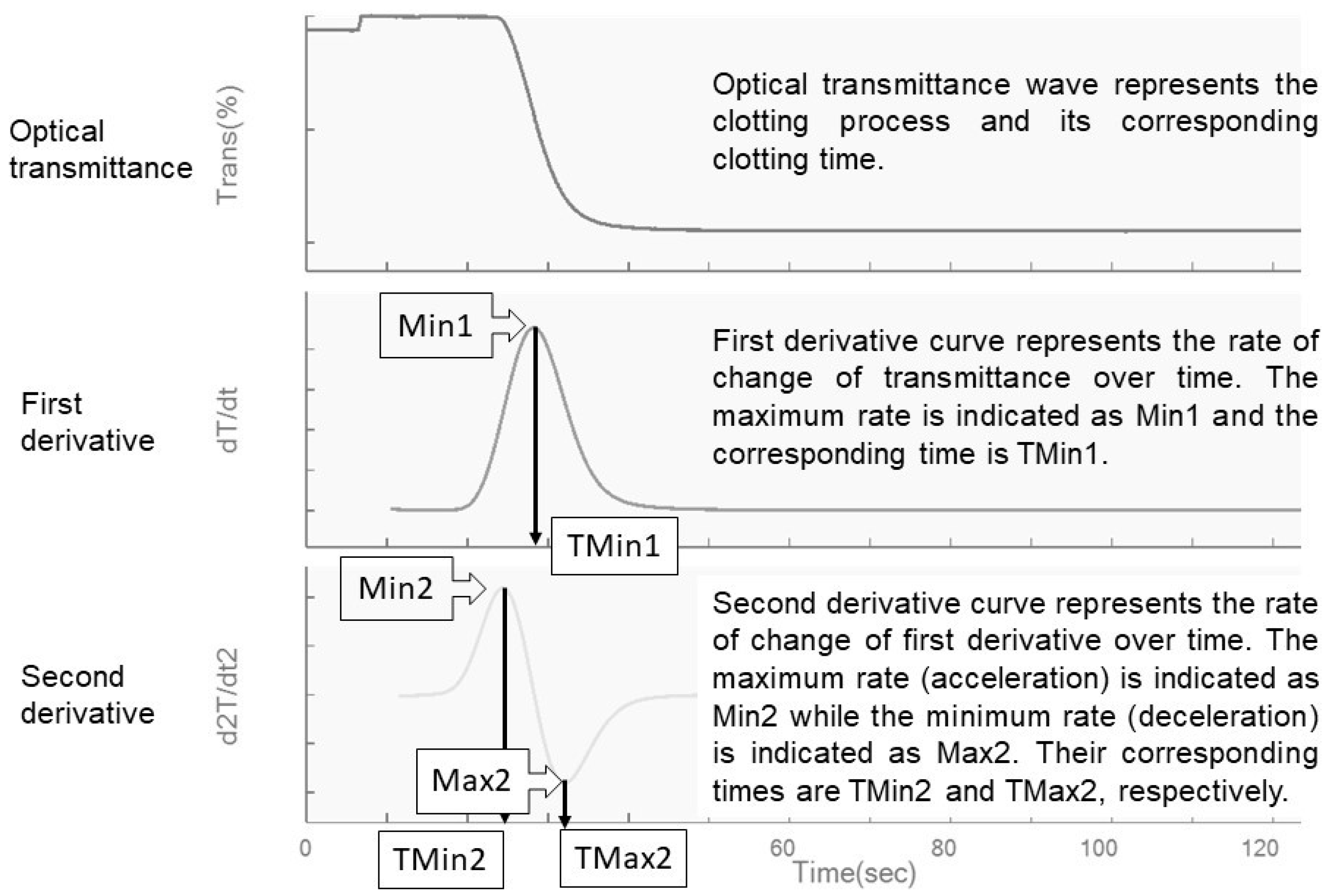
2.4. Clot Waveform Analysis and Reagent Used
2.5. Statistical Analysis
3. Results
3.1. Reagent Lot Variations
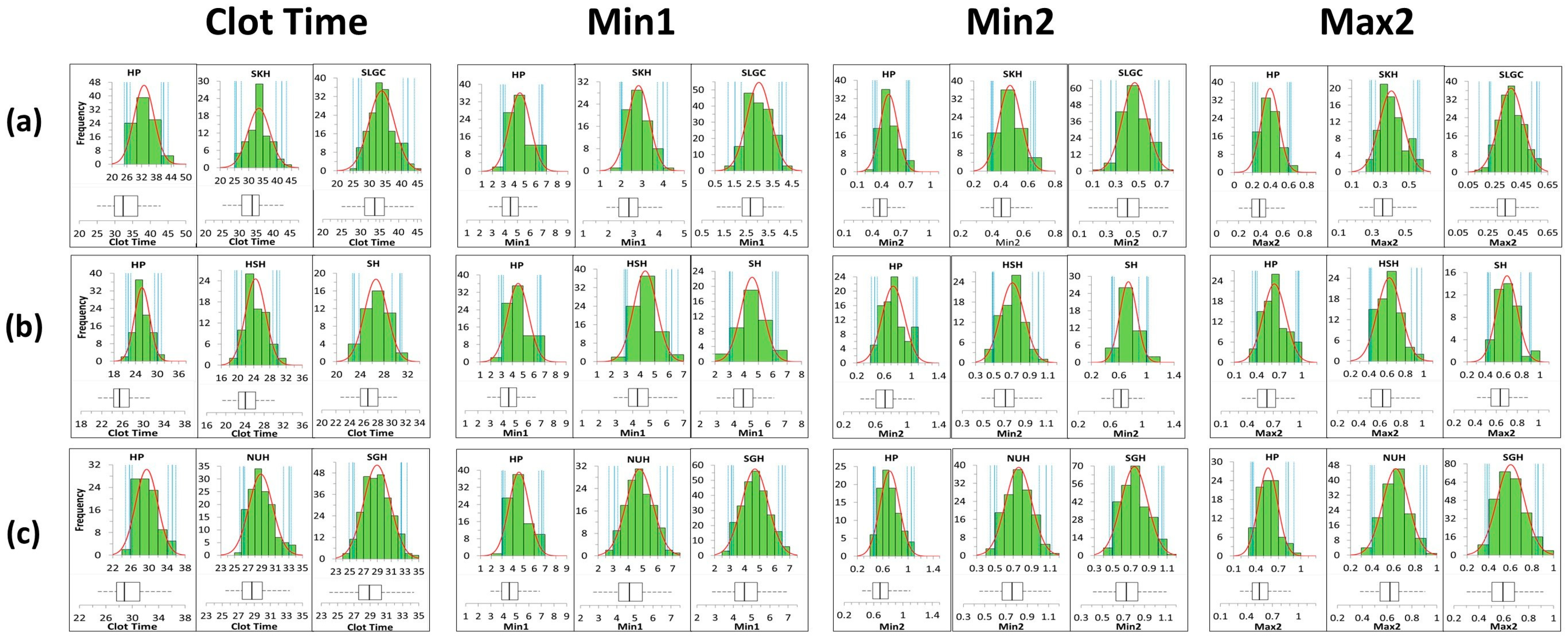
3.2. Distribution of the Reference Population
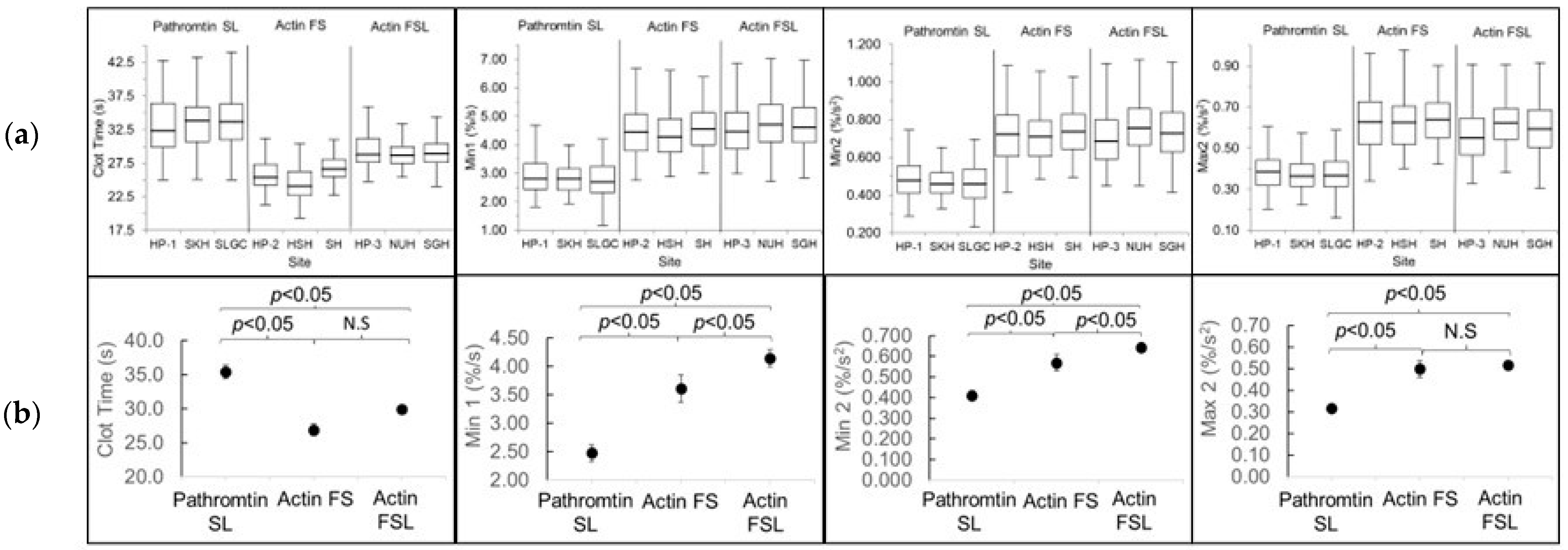
3.3. Reagents and Sites Differences and the Corresponding CWA Reference Intervals
3.4. Influence of Age and Gender
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shima, M.; Thachil, J.; Nair, S.C.; Srivastava, A. Towards standardization of clot waveform analysis and recommendations for its clinical applications. J. Thromb. Haemost. 2013, 11, 1417–1420. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Shima, M.; Takeyama, M.; Yoshida, K.; Tanaka, I.; Sakurai, Y.; Giles, A.R.; Yoshioka, A. The measurement of low levels of factor VIII or factor IX in hemophilia A and hemophilia B plasma by clot waveform analysis and thrombin generation assay. J. Thromb. Haemost. 2006, 4, 377–384. [Google Scholar] [CrossRef]
- Toh, C.H.; Giles, A.R. Waveform analysis of clotting test optical profiles in the diagnosis and management of disseminated intravascular coagulation (DIC). Clin. Lab. Haematol. 2002, 24, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, C.W.; Wong, W.H.; Cheen, M.H.H.; Chu, Y.M.H.; Lim, S.S.; Ng, L.C.K.; Yeo, D.G.D.; Morvil, G.; Lee, L.H.; Ng, H.J. Assesment of aPTT-based clot waveform analysis for the detection of haemostatic changes in different types of infections. Sci. Rep. 2020, 10, 14186. [Google Scholar] [CrossRef] [PubMed]
- Wen Tan, C.; Cheen, M.H.H.; Wong, W.H.; Wu, I.Q.; Chua, B.L.W.; Ahamedulla, S.H.; Lee, L.H.; Ng, H.J. Elevated activated partial thromboplastin time-based clot waveform analysis markers have strong positive association with acute venous thromboembolism. Biochem. Medica 2019, 29, 020710. [Google Scholar] [CrossRef]
- Tan, C.W.; Low, J.G.H.; Wong, W.H.; Chua, Y.Y.; Goh, S.L.; Ng, H.J. Critically ill COVID-19 infected patients exhibit increased clot waveform analysis parameters consistent with hypercoagulability. Am. J. Hematol. 2020, 95, E156–E158. [Google Scholar] [CrossRef] [PubMed]
- CAP. Evaluation Criteria, Coagulation, Limited (CGL) Participant Summary; College of American Pathologists (CAP): Northfield, IL, USA, 2020. [Google Scholar]
- Lawrie, A.S.; Iseppi, J.M.; Mackie, I.J.; Machin, S.J. Evaluation of a High Throughput Multi-wavelength Blood Coagulation Analyser—Sysmex CS-5100. Sysmex J. Int. 2011, 21, 1–9. [Google Scholar]
- Siemens Healthcare. Pathromtin SL Reagent Package Insert; Siemens Healthcare: Marburg, Germany, 2015. [Google Scholar]
- Siemens Healthcare. Actin FS Reagent Package Insert; Siemens Healthcare: Marburg, Germany, 2016. [Google Scholar]
- Siemens Healthcare. Actin FSL Reagent Package Insert; Siemens Healthcare: Marburg, Germany, 2012. [Google Scholar]
- Wayne, P.A. Clinical and Laboratory Standards Institute (CLSI). In Defining, Establishing and Verifying Reference Intervals in the Clinical Laboratory; Approved Guideline—Third edition; CLSI EP28-A3c 2016; Clinical and Laboratory Standards Institute (CLSI): Berwyn, PA, USA, 2016. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| HP | HSH | NUH | SH | SGH | SLGC | SKH | |
|---|---|---|---|---|---|---|---|
| Institution name, country | Hospital Pulau Pinang, Malaysia | Hasan Sadikin Hospital, Indonesia | National University Hospital, Singapore | Siriraj Hospital, Thailand | Singapore General Hospital, Singapore | St. Luke’s General Hospital, The Philippines | Sengkang General Hospital, Singapore |
| Analyzer | CS2500 | CS2100i | CS5100 | CS2100i | CS2100i | CS2100i | CS2500 |
| APTT reagent | Pathromtin SL (n = 94) Actin FS (n = 90) Actin FSL (n = 93) | Actin FS (n = 79) | Actin FSL (n = 140) | Actin FS (n = 46) | Actin FSL (n = 257) | Pathromtin SL (n = 174) | Pathromtin SL (n = 82) |
| Average % CV for APTT assay | Pathromtin SL: 1.6% Actin FS: 0.9% Actin FSL: 1.0% | 3.8% | 1.5% | 0.9% | 0.6% | 5.4% | 1.2% |
| Blood drawn through | Vacutainer | Vacutainer | Vacutainer | Vacutainer | Vacutainer | Vacutainer | Vacutainer |
| Blood tubes (manufacturer) | 3.2% sodium citrate (Becton-Dickinson Company, Franklin Lakes, NJ, USA) | ||||||
| Sample processing | 4000 rpm, 10 min | 4000 rpm, 10 min | 2800× g, 10 min | 1500× g, 15 min | 3000× g, 15 min | 1500× g, 10 min | 6000 rpm, 3 min |
| External quality assurance accreditation | RCPA 2 | UK IEQAS 3 | CAP 1 | CAP | CAP | CAP | CAP participation only |
| Reagent | Lot | Clot Time, s | Min1, %/s | TMin1, s | Min2, %/s2 | TMin2, s | Max2, %/s2 | TMax2, s |
|---|---|---|---|---|---|---|---|---|
| Pathromtin SL (n = 47) | 1 | 24.60–58.10 | 1.292–6.721 | 24.50–56.20 | 0.214–1.165 | 20.80–51.50 | 0.111–1.005 | 28.00–63.50 |
| 2 | 24.90–57.30 | 1.280–6.710 | 24.90–56.70 | 0.220–1.176 | 21.30–52.00 | 0.116–1.024 | 28.30–62.80 | |
| r | 0.982 | 0.998 | 0.98 | 0.997 | 0.98 | 0.997 | 0.98 | |
| p-value | 0.291 (N.S) | 0.472 (N.S) | 0.261 (N.S) | 0.390 (N.S) | 0.260 (N.S) | 0.518 (N.S) | 0.431 (N.S) | |
| % difference | 1.10% | 0.20% | 1.50% | 0.90% | 1.90% | 4.20% | 0.90% | |
| Actin FS (n = 57) | 1 | 23.10–50.30 | 2.814–8.192 | 23.00–49.00 | 0.421–1.378 | 19.30–44.30 | 0.300–1.151 | 26.70–53.80 |
| 2 | 23.40–53.10 | 2.809–8.245 | 23.30–51.90 | 0.427–1.362 | 19.60–47.20 | 0.301–1.156 | 26.80–56.60 | |
| r | 0.978 | 0.998 | 0.976 | 0.995 | 0.976 | 0.994 | 0.977 | |
| p-value | 0.147 (N.S) | 0.475 (N.S) | 0.173 (N.S) | 0.364 (N.S) | 0.288 (N.S) | 0.475 (N.S) | 0.274 (N.S) | |
| % difference | 0.30% | 0.70% | 0.30% | 1.90% | 0.10% | 2.50% | 0.50% | |
| Actin FSL (n = 44) | 1 | 19.10–69.00 | 0.949–8.419 | 19.20–68.40 | 0.118–1.375 | 15.70–63.10 | 0.087–1.205 | 22.50–74.00 |
| 2 | 19.10–63.90 | 1.036–8.543 | 19.20–63.30 | 0.136–1.399 | 15.80–58.20 | 0.099–1.230 | 22.60–68.50 | |
| r | 0.997 | 0.998 | 0.997 | 0.995 | 0.997 | 0.995 | 0.997 | |
| p-value | 0.306 (N.S) | 0.471 (N.S) | 0.268 (N.S) | 0.390 (N.S) | 0.305 (N.S) | 0.429 (N.S) | 0.306 (N.S) | |
| % difference | 3.60% | 4.60% | 3.40% | 7.60% | 3.40% | 8.80% | 3.50% |
| Reagent | Pathromtin SL | Actin FS | Actin FSL | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Site | HP | SKH | SLGC | Total | HP | HSH | SH | Total | HP | NUH | SGH | Total |
| Clot Time, s | ||||||||||||
| Number used | 94 | 80 | 171 | 345 | 89 | 77 | 45 | 211 | 93 | 140 | 255 | 482 |
| Unadjusted mean | 33.00 | 33.59 | 33.82 | 33.54 | 25.82 | 24.45 | 26.65 | 25.49 | 29.49 | 28.88 | 28.95 | 28.96 |
| 2.5th percentile (90% CI) | 25.98 (25.00–27.20) | 25.51 (25.10–27.41) | 26.63 (25.00–27.50) | 26.30 (25.20–26.90) | 21.91 (21.30–22.68) | 19.76 (19.30–20.99) | 23.00 (22.70–23.76) | 21.09 (19.30–21.50) | 25.67 (24.80–26.27) | 26.35 (25.40–26.50) | 25.44 (24.90–25.70) | 25.60 (25.40–26.00) |
| 97.5th percentile (90% CI) | 40.97 (39.96–42.80) | 41.76 (39.60–43.30) | 41.95 (40.50–44.00) | 41.15 (40.50–43.30) | 30.26 (29.45–31.20) | 29.72 (28.44–30.40) | 30.67 (29.36–31.00) | 30.24 (29.40–31.00) | 31.19 (34.15–35.90) | 33.25 (32.20–33.40) | 32.50 (32.40–33.30) | 33.19 (32.50–33.30) |
| Adjusted mean ± SE | 35.40 ± 0.99 | 26.92 ± 0.84 | 29.92 ± 0.33 | |||||||||
| Site-specific comparisons | p = 0.211 (N.S) | |||||||||||
| Min1,%/s | ||||||||||||
| Number used | 91 | 78 | 171 | 343 | 88 | 79 | 44 | 211 | 91 | 140 | 255 | 486 |
| Unadjusted mean | 2.914 | 2.809 | 2.775 | 2.833 | 4.534 | 4.341 | 4.574 | 4.470 | 4.571 | 4.773 | 4.684 | 4.704 |
| 2.5th percentile (90% CI) | 1.931 (1.820–2.078) | 2.002 (1.933–2.044) | 1.533 (1.172–1.857) | 1.792 (1.516–1.919) | 2.981 (2.749–3.186) | 2.991 (2.890–3.103) | 3.046 (2.991–3.211) | 2.993 (2.890–3.092) | 3.069 (2.982–3.222) | 3.086 (2.717–3.306) | 3.129 (2.908–3.252) | 3.118 (3.031–3.202) |
| 97.5th percentile (90% CI) | 4.407 (4.209–4.697) | 3.884 (3.637–3.998) | 3.977 (3.814–4.197) | 4.012 (3.940–4.278) | 6.571 (6.335–6.675) | 6.176 (5.787–6.616) | 6.236 (5.986–6.374) | 6.414 (6.227–6.626) | 6.697 (6.399–6.857) | 6.640 (6.166–7.022) | 6.521 (6.261–6.700) | 6.555 (6.373–6.796) |
| Adjusted mean ± SE | 2.477 ± 0.145 | 3.609 ± 0.241 | 4.144 ± 0.150 | |||||||||
| Site-specific comparisons | p = 0.113 (N.S) | |||||||||||
| Time of min1 (Tmin1), s | ||||||||||||
| Number used | 94 | 80 | 168 | 341 | 89 | 77 | 45 | 211 | 93 | 140 | 255 | 483 |
| Unadjusted mean | 32.93 | 33.45 | 33.54 | 33.36 | 25.68 | 24.40 | 26.51 | 25.39 | 29.15 | 28.64 | 28.69 | 28.70 |
| 2.5th percentile (90% CI) | 26.03 (25.20–27.28) | 25.55 (25.20–27.32) | 26.70 (25.10–27.50) | 26.26 (25.20–27.00) | 21.91 (21.30–22.70) | 19.80 (19.30–20.99) | 22.90 (22.60–23.75) | 21.09 (19.30–21.60) | 25.60 (24.70–26.20) | 26.25 (25.40–26.40) | 25.34 (24.80–25.60) | 25.51 (25.30–25.90) |
| 97.5th percentile (90% CI) | 40.52 (39.20–42.20) | 41.22 (39.30–42.80) | 40.58 (40.00–41.60) | 40.55 (40.10–41.30) | 29.95 (29.15–30.90) | 29.49 (28.38–30.20) | 30.35 (28.90–30.70) | 29.94 (29.20–30.70) | 34.57 (33.20–35.30) | 32.80 (31.80–33.00) | 32.14 (31.80–32.80) | 32.67 (31.90–32.80) |
| Adjusted mean ± SE | 35.88 ± 1.02 | 27.90 ± 0.88 | 29.59 ± 0.32 | |||||||||
| Site-specific comparisons | p = 0.131 (N.S) | |||||||||||
| Min2,%/s2 | ||||||||||||
| Number used | 91 | 78 | 172 | 339 | 88 | 78 | 44 | 210 | 91 | 140 | 255 | 486 |
| Unadjusted mean | 0.488 | 0.467 | 0.464 | 0.471 | 0.732 | 0.707 | 0.737 | 0.724 | 0.710 | 0.758 | 0.740 | 0.740 |
| 2.5th percentile (90% CI) | 0.319 (0.289–0.343) | 0.333 (0.328–0.342) | 0.268 (0.230–0.305) | 0.276 (0.261–0.291) | 0.463 (0.414–0.404) | 0.490 (0.484–0.504) | 0.505 (0.493–0.532) | 0.440 (0.412–0.468) | 0.460 (0.448–0.478) | 0.496 (0.451–0.520) | 0.492 (0.464–0.518) | 0.484 (0.465–0.506) |
| 97.5th percentile (90% CI) | 0.727 (0.700–0.744) | 0.643 (0.619–0.653) | 0.656 (0.640–0.697) | 0.667 (0.652–0.682) | 1.069 (1.029–1.089) | 0.990 (0.9230–1.057) | 1.010 (0.960–1.028) | 1.008 (0.980–1.036) | 1.056 (0.99–1.098) | 1.060 (0.985–1.119) | 1.041 (1.007–1.062) | 1.042 (1.021–1.075) |
| Adjusted mean ± SE | 35.88 ± 1.02 | 27.90 ± 0.88 | 29.59 ± 0.32 | |||||||||
| Site-specific comparisons | p = 0.113 (N.S) | |||||||||||
| Time of min2 (Tmin2), s | ||||||||||||
| Number used | 94 | 79 | 168 | 341 | 89 | 77 | 45 | 211 | 91 | 140 | 254 | 483 |
| Unadjusted mean | 29.19 | 29.55 | 29.79 | 29.57 | 21.87 | 20.68 | 22.68 | 21.61 | 24.98 | 24.74 | 24.78 | 24.78 |
| 2.5th percentile (90% CI) | 22.46 (21.70–23.79) | 22.00 (21.60–23.50) | 23.20 (21.60–23.90) | 22.71 (21.70–23.50) | 18.30 (17.80–18.90) | 16.37 (15.90–17.30) | 19.26 (18.90–20.03) | 17.36 (15.90–18.00) | 21.78 (21.00–22.45) | 22.45 (21.90–22.80) | 21.64 (21.50–22.00) | 21.81 (21.60–22.20) |
| 97.5th percentile (90% CI) | 36.42 (35.61–38.00) | 36.33 (35.30–37.20) | 36.68 (35.90–37.50) | 36.45 (36.00–37.10) | 25.74 (25.00–26.60) | 25.48 (24.81–26.20) | 26.24 (25.00–26.50) | 25.70 (25.00–26.50) | 28.63 (28.10–29.20) | 28.40 (27.60–28.80) | 27.90 (27.50–28.30) | 28.20 (27.90–28.60) |
| Adjusted mean ± SE | 32.07 ± 0.98 | 23.97 ± 0.82 | 25.61 ± 0.29 | |||||||||
| Site-specific comparisons | p = 0.126 (N.S) | |||||||||||
| Max2,%/s2 | ||||||||||||
| Number used | 92 | 81 | 172 | 342 | 88 | 79 | 44 | 211 | 90 | 140 | 255 | 485 |
| Unadjusted mean | 0.394 | 0.377 | 0.372 | 0.378 | 0.634 | 0.624 | 0.638 | 0.631 | 0.561 | 0.619 | 0.603 | 0.600 |
| 2.5th percentile (90% CI) | 0.230 (0.204–0.255) | 0.237 (0.225–0.264) | 0.212 (0.159–0.220) | 0.218 (0.208–0.234) | 0.379 (0.340–0.408) | 0.416 (0.401–0.429) | 0.433 (0.421–0.453) | 0.402 (0.378–0.421) | 0.350 (0.327–0.371) | 0.397 (0.382–0.418) | 0.385 (0.365–0.404) | 0.376 (0.361–0.387) |
| 97.5th percentile (90% CI) | 0.592 (0.568–0.605) | 0.560 (0.532–0.574) | 0.567 (0.528–0.587) | 0.571 (0.559–0.587) | 0.949 (0.923–0.962) | 0.930 (0.866–0.977) | 0.887 (0.793–0.903) | 0.944 (0.902–0.962) | 0.834 (0.800–0.908) | 0.878 (0.847–0.906) | 0.857 (0.833–0.905) | 0.858 (0.838–0.891) |
| Adjusted mean ± SE | 0.316 ± 0.021 | 0.498 ± 0.038 | 0.515 ± 0.021 | |||||||||
| Site-specific comparisons | p = 0.05 (N.S) | |||||||||||
| Time of max2 (Tmax2), s | ||||||||||||
| Number used | 94 | 80 | 168 | 342 | 89 | 77 | 45 | 211 | 93 | 140 | 253 | 481 |
| Unadjusted mean | 36.66 | 37.22 | 37.27 | 37.09 | 29.51 | 28.11 | 30.34 | 29.18 | 33.22 | 32.53 | 32.57 | 32.62 |
| 2.5th percentile (90% CI) | 29.58 (28.50–30.89) | 29.03 (28.60–31.01) | 30.20 (28.40–31.10) | 29.80 (28.70–30.50) | 25.24 (24.70–26.30) | 23.29 (22.70–24.40) | 26.54 (26.20–27.40) | 24.49 (22.80–25.20) | 29.19 (28.40–29.77) | 29.90 (28.90–30.10) | 29.00 (28.40–29.30) | 29.11 (28.90–29.60) |
| 97.5th percentile (90% CI) | 44.80 (43.60–46.01) | 45.57 (43.20–47.10) | 44.50 (44.10–46.00) | 44.64 (44.20–45.60) | 34.31 (33.43–35.30) | 33.58 (32.53–34.10) | 34.61 (33.16–35.00) | 34.10 (33.30–35.00) | 37.39 (36.81–37.90) | 37.20 (36.00–37.50) | 36.37 (36.10–37.10) | 36.90 (36.30–37.30) |
| Adjusted mean ± SE | 39.92 ± 1.09 | 25.93 ± 1.40 | 33.66 ± 0.72 | |||||||||
| Site-specific comparisons | p = 0.121 (N.S) | |||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, W.H.; Tan, C.W.; Abdul Khalid, N.B.; Dalimoenthe, N.Z.; Yip, C.; Tantanate, C.; Lim, R.D.; Kim, J.H.; Ng, H.J. Reagent Effects on the Activated Partial Thromboplastin Time Clot Waveform Analysis: A Multi-Centre Study. Diagnostics 2023, 13, 2447. https://doi.org/10.3390/diagnostics13142447
Wong WH, Tan CW, Abdul Khalid NB, Dalimoenthe NZ, Yip C, Tantanate C, Lim RD, Kim JH, Ng HJ. Reagent Effects on the Activated Partial Thromboplastin Time Clot Waveform Analysis: A Multi-Centre Study. Diagnostics. 2023; 13(14):2447. https://doi.org/10.3390/diagnostics13142447
Chicago/Turabian StyleWong, Wan Hui, Chuen Wen Tan, Nabeelah Binti Abdul Khalid, Nadjwa Zamalek Dalimoenthe, Christina Yip, Chaicharoen Tantanate, Rodelio D. Lim, Ji Hyun Kim, and Heng Joo Ng. 2023. "Reagent Effects on the Activated Partial Thromboplastin Time Clot Waveform Analysis: A Multi-Centre Study" Diagnostics 13, no. 14: 2447. https://doi.org/10.3390/diagnostics13142447