
Machine-Learning-Based Diagnostics of Cardiac Sarcoidosis Using Multi-Chamber Wall Motion Analyses
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Cohort
2.2. Cardiac Magnetic Resonance Imaging
2.3. Cardiac Function and Strain Quantification
2.4. Descriptive Statistics
2.5. Cardiac Features
2.6. Correlation Matrix
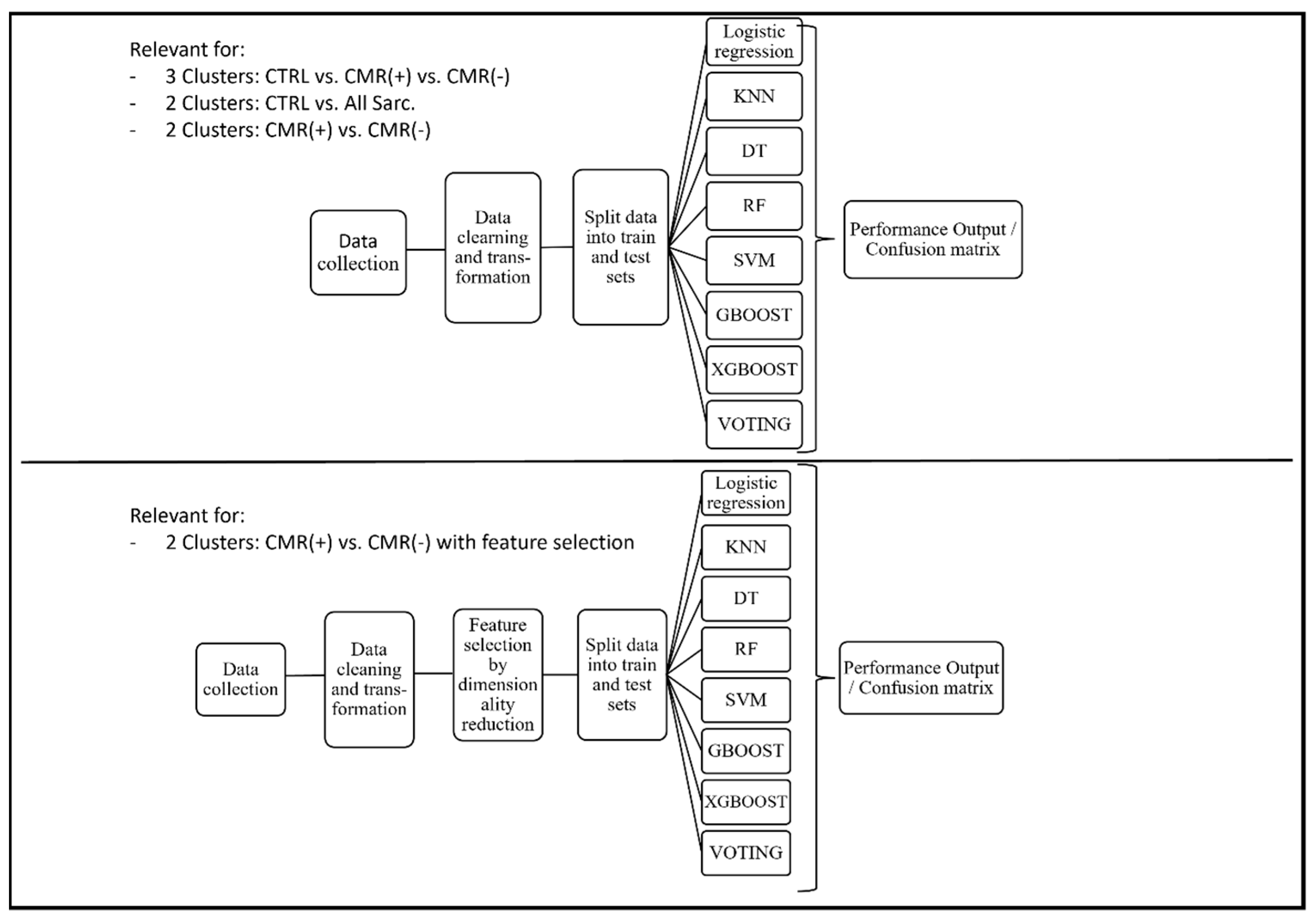
2.7. Classification Algorithms
2.8. Algorithmic Feature Selection
3. Results
3.1. Baseline Features
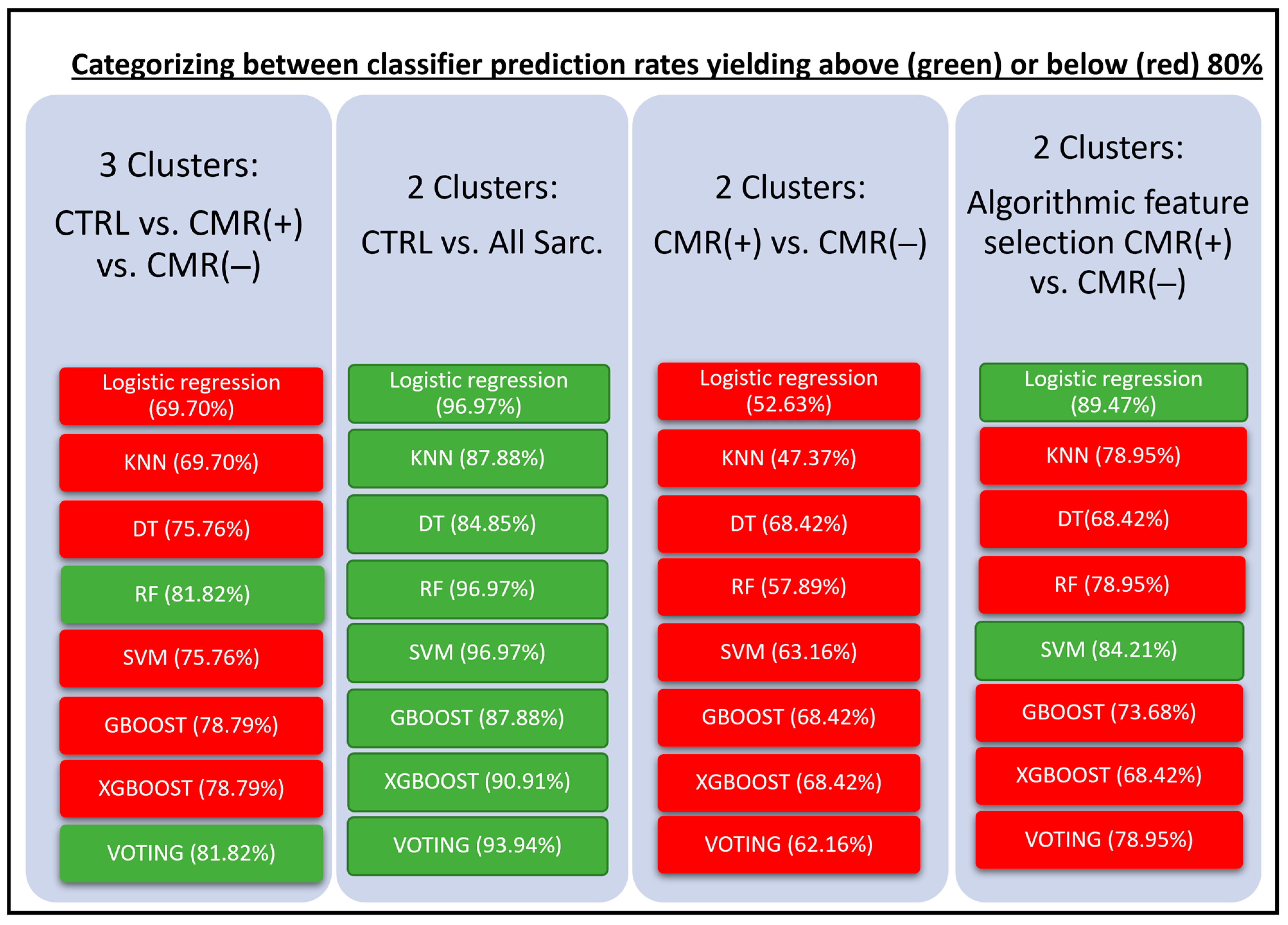
3.2. Diagnostic Accuracy of Machine Learning Models
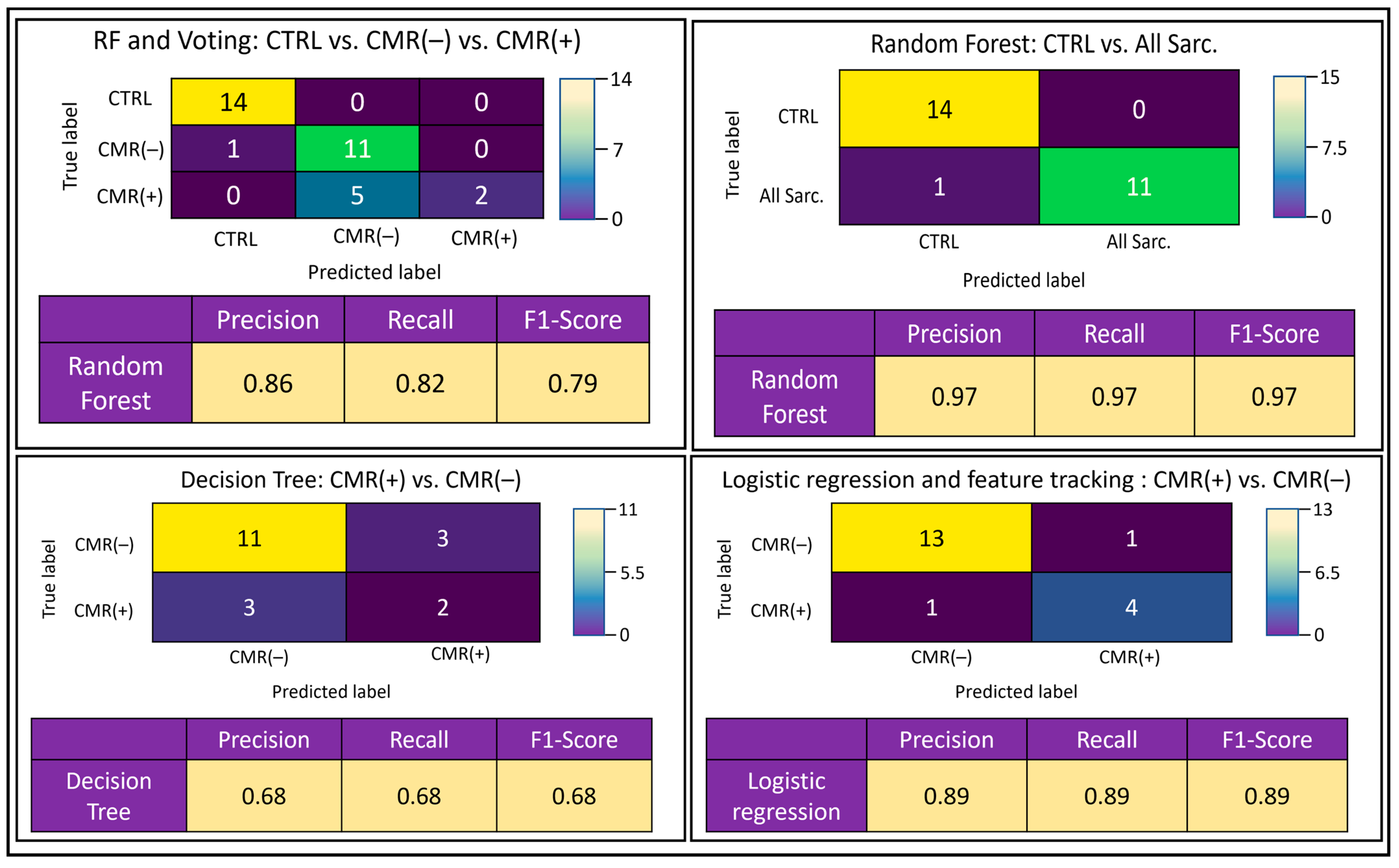
3.3. Confusion Matrices
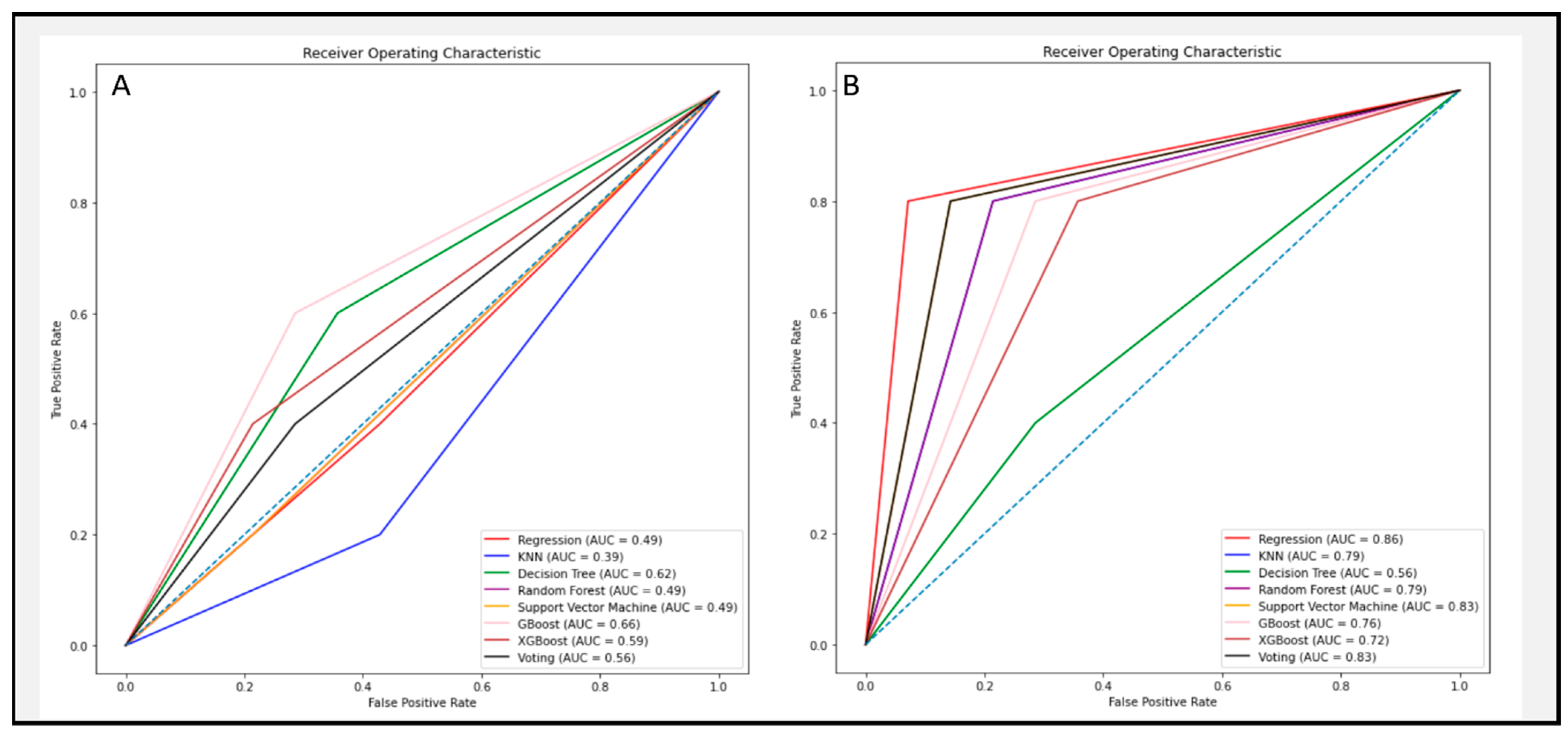
3.4. Algorithmic Feature Selection
4. Discussion
- (i)
- Accurate algorithmic discrimination was achieved between healthy subjects and all sarcoidosis patients, particularly with Voting and RF classifiers;
- (ii)
- Poor algorithmic discrimination of CMR(−) and CMR(+) patients was improved to accurate levels via algorithmic feature selection application, particularly when using logistic regression and SVM classifiers;
- (iii)
- The algorithmic challenge associated with discrimination between both patient groups implies cardiac involvement may be more prevalent than anticipated, potentially evading CMR detection.
4.1. The Benefit of Machine Learning in Cardiac Imaging
4.2. Weighting of the Input Features
4.3. Clinical Outlooks
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soto-Gomez, N.; Peters, J.I.; Nambiar, A.M. Diagnosis and Management of Sarcoidosis. Am. Fam. Physician 2016, 93, 840–848. [Google Scholar]
- Hamzeh, N.; Steckman, D.A.; Sauer, W.H.; Judson, M.A. Pathophysiology and clinical management of cardiac sarcoidosis. Nat. Rev. Cardiol. 2015, 12, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Chow, K.L.; O’Donnell, J.L.; Crozier, I. Prevalence, incidence and survival outcomes of cardiac sarcoidosis in the South Island, New Zealand. Int. J. Cardiol. 2022, 357, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Swigris, J.J.; Olson, A.L.; Huie, T.J.; Fernandez-Perez, E.R.; Solomon, J.; Sprunger, D.; Brown, K.K. Sarcoidosis-related mortality in the United States from 1988 to 2007. Am. J. Respir. Crit. Care Med. 2011, 183, 1524–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverman, K.J.; Hutchins, G.M.; Bulkley, B.H. Cardiac sarcoid: A clinicopathologic study of 84 unselected patients with systemic sarcoidosis. Circulation 1978, 58, 1204–1211. [Google Scholar] [CrossRef] [Green Version]
- Kandolin, R.; Lehtonen, J.; Airaksinen, J.; Vihinen, T.; Miettinen, H.; Ylitalo, K.; Kaikkonen, K.; Tuohinen, S.; Haataja, P.; Kerola, T.; et al. Cardiac sarcoidosis: Epidemiology, characteristics, and outcome over 25 years in a nationwide study. Circulation 2015, 131, 624–632. [Google Scholar] [CrossRef]
- Roberts, W.C.; McAllister, H.A., Jr.; Ferrans, V.J. Sarcoidosis of the heart. A clinicopathologic study of 35 necropsy patients (group 1) and review of 78 previously described necropsy patients (group 11). Am. J. Med. 1977, 63, 86–108. [Google Scholar] [CrossRef] [PubMed]
- Uemura, A.; Morimoto, S.-I.; Hiramitsu, S.; Kato, Y.; Ito, T.; Hishida, H. Histologic diagnostic rate of cardiac sarcoidosis: Evaluation of endomyocardial biopsies. Am. Heart J. 1999, 138 Pt 1, 299–302. [Google Scholar] [CrossRef]
- Yazaki, Y.; Isobe, M.; Hiroe, M.; Morimoto, S.-I.; Hiramitsu, S.; Nakano, T.; Izumi, T.; Sekiguchi, M. Prognostic determinants of long-term survival in Japanese patients with cardiac sarcoidosis treated with prednisone. Am. J. Cardiol. 2001, 88, 1006–1010. [Google Scholar] [CrossRef]
- Patel, A.R.; Kramer, C.M. Role of Cardiac Magnetic Resonance in the Diagnosis and Prognosis of Nonischemic Cardiomyopathy. JACC Cardiovasc. Imaging 2017, 10 Pt A, 1180–1193. [Google Scholar] [CrossRef]
- Kouranos, V.; Tzelepis, G.E.; Rapti, A.; Mavrogeni, S.; Aggeli, K.; Douskou, M.; Prasad, S.; Koulouris, N.; Sfikakis, P.; Wells, A.; et al. Complementary Role of CMR to Conventional Screening in the Diagnosis and Prognosis of Cardiac Sarcoidosis. JACC Cardiovasc. Imaging 2017, 10, 1437–1447. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Cawley, P.J.; Heitner, J.F.; Klem, I.; Parker, M.A.; Jaroudi, W.A.; Meine, T.J.; White, J.B.; Elliott, M.D.; Kim, H.W.; et al. Detection of myocardial damage in patients with sarcoidosis. Circulation 2009, 120, 1969–1977. [Google Scholar] [CrossRef] [Green Version]
- Coleman, G.C.; Shaw, P.W.; Balfour, P.C., Jr.; Gonzalez, J.A.; Kramer, C.M.; Patel, A.R.; Salerno, M. Prognostic Value of Myocardial Scarring on CMR in Patients With Cardiac Sarcoidosis. JACC Cardiovasc. Imaging 2017, 10, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.R. Detection of Cardiac Sarcoidosis: A Balancing Act Between Symptoms and Imaging Findings. JACC Cardiovasc. Imaging 2017, 10, 1448–1450. [Google Scholar] [CrossRef]
- Tigen, K.; Sunbul, M.; Karaahmet, T.; Tasar, O.; Dundar, C.; Yalcinsoy, M.; Takir, M.; Akkaya, E. Early Detection of Bi-ventricular and Atrial Mechanical Dysfunction Using Two-Dimensional Speckle Tracking Echocardiography in Patients with Sarcoidosis. Lung 2015, 193, 669–675. [Google Scholar] [CrossRef]
- Kusunose, K.; Fujiwara, M.; Yamada, H.; Nishio, S.; Saijo, Y.; Yamada, N.; Hirata, Y.; Torii, Y.; Ise, T.; Yamaguchi, K.; et al. Deterioration of biventricular strain is an early marker of cardiac involvement in confirmed sarcoidosis. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Dabir, D.; Meyer, D.; Kuetting, D.; Luetkens, J.; Homsi, R.; Pizarro, C.; Nadal, J.; Thomas, D. Diagnostic Value of Cardiac Magnetic Resonance Strain Analysis for Detection of Cardiac Sarcoidosis. Rofo 2018, 190, 712–721. [Google Scholar] [CrossRef] [Green Version]
- Eckstein, J.; Moghadasi, N.; Körperich, H.; Valdés, E.W.; Sciacca, V.; Paluszkiewicz, L.; Burchert, W.; Piran, M. A Machine Learning Challenge: Detection of Cardiac Amyloidosis Based on Bi-Atrial and Right Ventricular Strain and Cardiac Function. Diagnostics 2022, 12, 2693. [Google Scholar] [CrossRef] [PubMed]
- Correia, F.A.S.C.; Marchini, G.S.; Torricelli, F.C.; Danilovic, A.; Vicentini, F.C.; Srougi, M.; Nahas, W.C.; Mazzucchi, E. Renal manifestations of sarcoidosis: From accurate diagnosis to specific treatment. Int. Braz. J. Urol. 2020, 46, 15–25. [Google Scholar] [CrossRef] [Green Version]
- Casella, F.J.; Allon, M. The kidney in sarcoidosis. J. Am. Soc. Nephrol. 1993, 3, 1555–1562. [Google Scholar] [CrossRef]
- Birnie, D.H.; Sauer, W.H.; Bogun, F.; Cooper, J.M.; Culver, D.A.; Duvernoy, C.S.; Judson, M.A.; Kron, J.; Mehta, D.; Nielsen, J.C.; et al. HRS expert consensus statement on the diagnosis and management of arrhythmias associated with cardiac sarcoidosis. Heart Rhythm 2014, 11, 1305–1323. [Google Scholar] [CrossRef] [PubMed]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2018, 72, e91–e220. [Google Scholar] [PubMed]
- Weise Valdés, E.; Barth, P.; Piran, M.; Laser, K.T.; Burchert, W.; Körperich, H. Left-Ventricular Reference Myocardial Strain Assessed by Cardiovascular Magnetic Resonance Feature Tracking and fSENC-Impact of Temporal Resolution and Cardiac Muscle Mass. Front. Cardiovasc. Med. 2021, 8, 764496. [Google Scholar] [CrossRef] [PubMed]
- Mella, N.V.V.P.; Pentakoti, V.M. Crop yield prediction and Fertilizer Recommendation using Voting Based Ensemble Classifier. J. Eng. Sci. 2022, 13, 262–270. [Google Scholar]
- Hastie, T.; Tibshirani, R.; Friedman, J.H.; Friedman, J.H. The Elements of Statistical Learning, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Ali, N.F.M.; Sadullah, A.F.M.; Majeed, A.P.A.; Razman, M.A.M.; Musa, R.M. The identification of significant features towards travel mode choice and its prediction via optimised random forest classifier: An evaluation for active commuting behavior. J. Transp. Health 2022, 25, 101362. [Google Scholar]
- Karr, J.; Cohen, M.; McQuiston, S.A.; Poorsala, T.; Malozzi, C. Validation of a deep-learning semantic segmentation approach to fully automate MRI-based left-ventricular deformation analysis in cardiotoxicity. Br. J. Radiol. 2021, 94, 20201101. [Google Scholar] [CrossRef]
- Neisius, U.; El-Rewaidy, H.; Nakamori, S.; Rodriguez, J.; Manning, W.J.; Nezafat, R. Radiomic Analysis of Myocardial Native T(1) Imaging Discriminates Between Hypertensive Heart Disease and Hypertrophic Cardiomyopathy. JACC Cardiovasc. Imaging 2019, 12, 1946–1954. [Google Scholar] [CrossRef]
- Huang, S.; Shi, K.; Zhang, Y.; Yan, W.-F.; Guo, Y.-K.; Li, Y.; Yang, Z.-G. Texture analysis of T2-weighted cardiovascular magnetic resonance imaging to discriminate between cardiac amyloidosis and hypertrophic cardiomyopathy. BMC Cardiovasc. Disord. 2022, 22, 235. [Google Scholar] [CrossRef]
- Joyce, E.; Ninaber, M.K.; Katsanos, S.; Debonnaire, P.; Kamperidis, V.; Bax, J.J.; Taube, C.; Delgado, V.; Marsan, N.A. Subclinical left ventricular dysfunction by echocardiographic speckle-tracking strain analysis relates to outcome in sarcoidosis. Eur. J. Heart Fail. 2015, 17, 51–62. [Google Scholar] [CrossRef]
- Aggeli, C.; Felekos, I.; Tousoulis, D.; Gialafos, E.; Rapti, A.; Stefanadis, C. Myocardial mechanics for the early detection of cardiac sarcoidosis. Int. J. Cardiol. 2013, 168, 4820–4821. [Google Scholar] [CrossRef]
- Katsushika, S.; Kodera, S.; Nakamoto, M.; Ninomiya, K.; Kakuda, N.; Shinohara, H.; Matsuoka, R.; Ieki, H.; Uehara, M.; Higashikuni, Y.; et al. Deep Learning Algorithm to Detect Cardiac Sarcoidosis from Echocardiographic Movies. Circ. J. 2021, 86, 87–95. [Google Scholar] [CrossRef]
- Togo, R.; Hirata, K.; Manabe, O.; Ohira, H.; Tsujino, I.; Magota, K.; Ogawa, T.; Haseyama, M.; Shiga, T. Cardiac sarcoidosis classification with deep convolutional neural network-based features using polar maps. Comput. Biol. Med. 2019, 104, 81–86. [Google Scholar] [CrossRef] [Green Version]
- Di Stefano, C.; Bruno, G.; Calle, M.C.A.; Acharya, G.A.; Fussner, L.M.; Ungprasert, P.; Cooper, L.T.; Blauwet, L.A.; Ryu, J.H.; Pellikka, P.A.; et al. Diagnostic and predictive value of speckle tracking echocardiography in cardiac sarcoidosis. BMC Cardiovasc. Disord. 2020, 20, 21. [Google Scholar] [CrossRef]
- Freeman, A.M.; Curran-Everett, D.; Weinberger, H.D.; Fenster, B.E.; Buckner, J.K.; Gottschall, E.B.; Sauer, W.H.; Maier, L.A.; Hamzeh, N.Y. Predictors of cardiac sarcoidosis using commonly available cardiac studies. Am. J. Cardiol. 2013, 112, 280–285. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CRTL | CMR(−) | CMR(+) | Comparison | p-Values | |
|---|---|---|---|---|---|
| Number | 44 | 45 | 18 | ||
| Male | 23 | 19 | 12 | ||
| Age c | 56.5(53.0;63.0) § | 56.5(53.0;63.0) § | 64.0(57.8;67.0) § | n.s. | |
| Weight b | 74.2 ± 12.5 | 81.9 ± 15.1 | 85.6 ± 17.0 | CTRL—CMR(−) CRTL—CMR(+) | 0.036 0.016 |
| Height c | 172 ± 10 | 168(164;177) § | 177 ± 10 | n.s. | |
| Heart rate b | 65 ± 10 | 72 ± 13 | 71 ± 13 | CTRL—CMR(−) | 0.015 |
| BMI c | 24.8 ± 2.6 | 28.0 ± 4.5 | 27.3 ± 4.8 | CTRL—CMR(−) | <0.001 |
| LV_EF c | 67 ± 5 | 61(50;65) | 49 ± 15 | CTRL—CMR(−) CRTL—CMR(+) | <0.001 <0.001 |
| LV_ESVi c | 23.0(20.9;26.8) § | 27.9(21.1;38.3) § | 50.2 ± 21.2 | CTRL—CMR(−) CRTL—CMR(+) CMR(−)—CMR(+) | 0.022 <0.001 0.004 |
| LV_EDVi c | 71.6 ± 9.6 | 69.3(60.0;83.7) § | 96.5 ± 26.0 | CRTL—CMR(+) CMR(−)—CMR(+) | <0.001 <0.001 |
| LV_longitudinal_strain c | −16.5 ± 2.4 | −15.9(−17.5;−14.4) § | −10.9 ± 3.8 | CRTL—CMR(+) CMR(−)—CMR(+) | <0.001 0.001 |
| LV_radial_strain b | 29.5 ± 7.4 | 26.7 ± 8.5 | 19.9 ± 7.5 | CRTL—CMR(+) CMR(−)—CMR(+) | <0.001 0.007 |
| LV_circumferential_strain c | −17.3 ± 3.1 | −17.1(−18.7;−15.2) § | −12.8 ± 4.0 | CRTL—CMR(+) CMR(−)—CMR(+) | <0.001 0.005 |
| RV_EF c | 61 ± 6 | 49.5(40.7;56.3) § | 44.1 (26.2;53.6) § | CTRL—CMR(−) CRTL—CMR(+) | <0.001 <0.001 |
| RV_ESVi c | 30.1 ± 8.1 | 38.4(29.2;48.7) § | 44.4 (36.7;74.7) § | CTRL—CMR(−) CRTL—CMR(+) | 0.003 <0.001 |
| RV_EDVi c | 76.0 ± 12.7 | 71.1(63.7;88.5) § | 83.1 (66.1;92.2) § | n.s. |
| Parameter | Feature Rates |
|---|---|
| LV_ESVi | 0.045 |
| LV_syst_radial_LAX_SR | 0.045 |
| LV_diast_radial_LAX_SR | 0.049 |
| LV_radial_LAX_S | 0.056 |
| LA_syst_long_LAX_SR | 0.060 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eckstein, J.; Moghadasi, N.; Körperich, H.; Akkuzu, R.; Sciacca, V.; Sohns, C.; Sommer, P.; Berg, J.; Paluszkiewicz, J.; Burchert, W.; et al. Machine-Learning-Based Diagnostics of Cardiac Sarcoidosis Using Multi-Chamber Wall Motion Analyses. Diagnostics 2023, 13, 2426. https://doi.org/10.3390/diagnostics13142426
Eckstein J, Moghadasi N, Körperich H, Akkuzu R, Sciacca V, Sohns C, Sommer P, Berg J, Paluszkiewicz J, Burchert W, et al. Machine-Learning-Based Diagnostics of Cardiac Sarcoidosis Using Multi-Chamber Wall Motion Analyses. Diagnostics. 2023; 13(14):2426. https://doi.org/10.3390/diagnostics13142426
Chicago/Turabian StyleEckstein, Jan, Negin Moghadasi, Hermann Körperich, Rehsan Akkuzu, Vanessa Sciacca, Christian Sohns, Philipp Sommer, Julian Berg, Jerzy Paluszkiewicz, Wolfgang Burchert, and et al. 2023. "Machine-Learning-Based Diagnostics of Cardiac Sarcoidosis Using Multi-Chamber Wall Motion Analyses" Diagnostics 13, no. 14: 2426. https://doi.org/10.3390/diagnostics13142426