
Occlusal Plane Steepness and Profile Change Following TAD-Based One-Step Retraction on Four-Unit Extraction Cases: A Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Registration
2.2. Sample
2.3. The Study Protocol
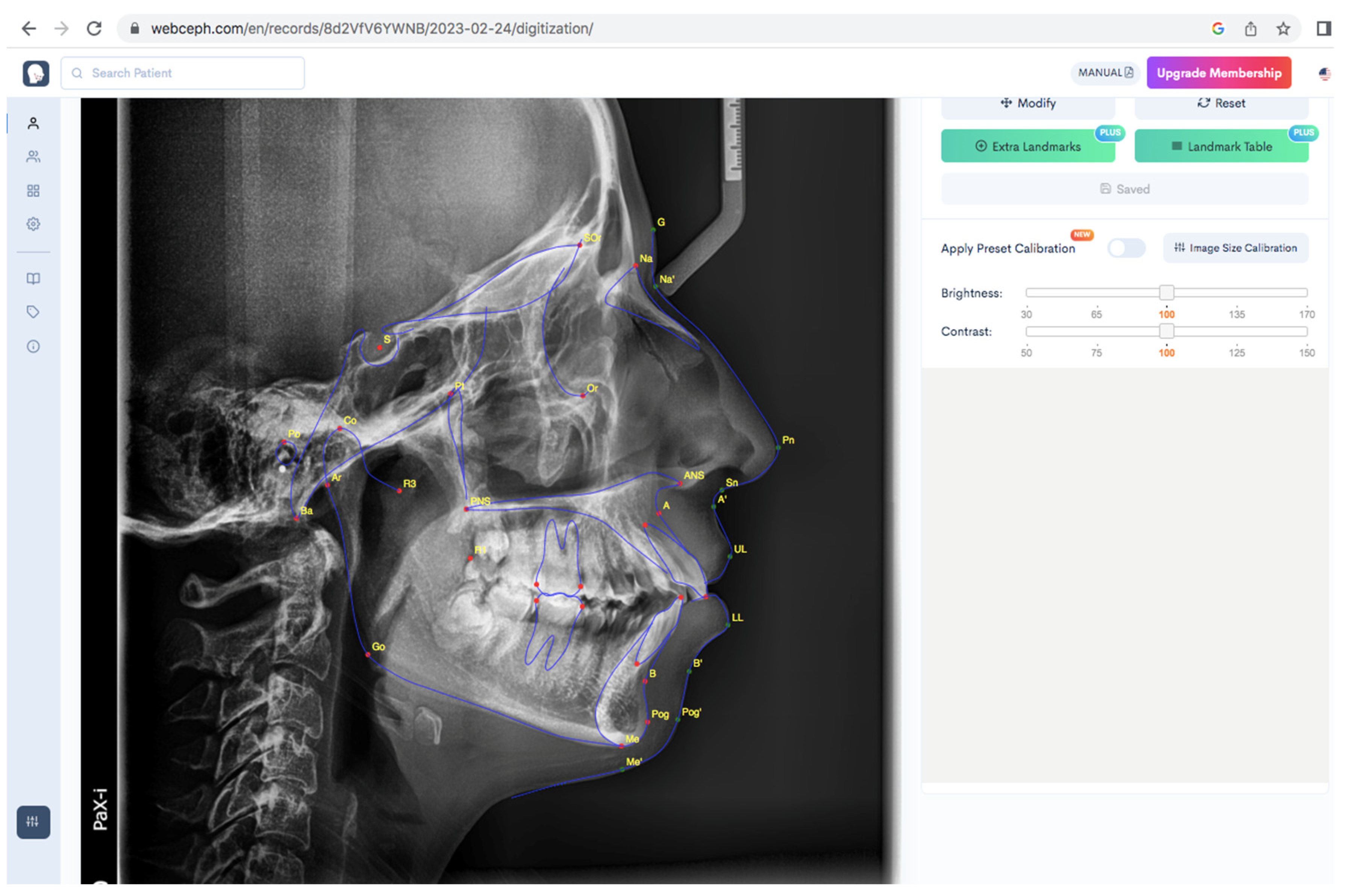
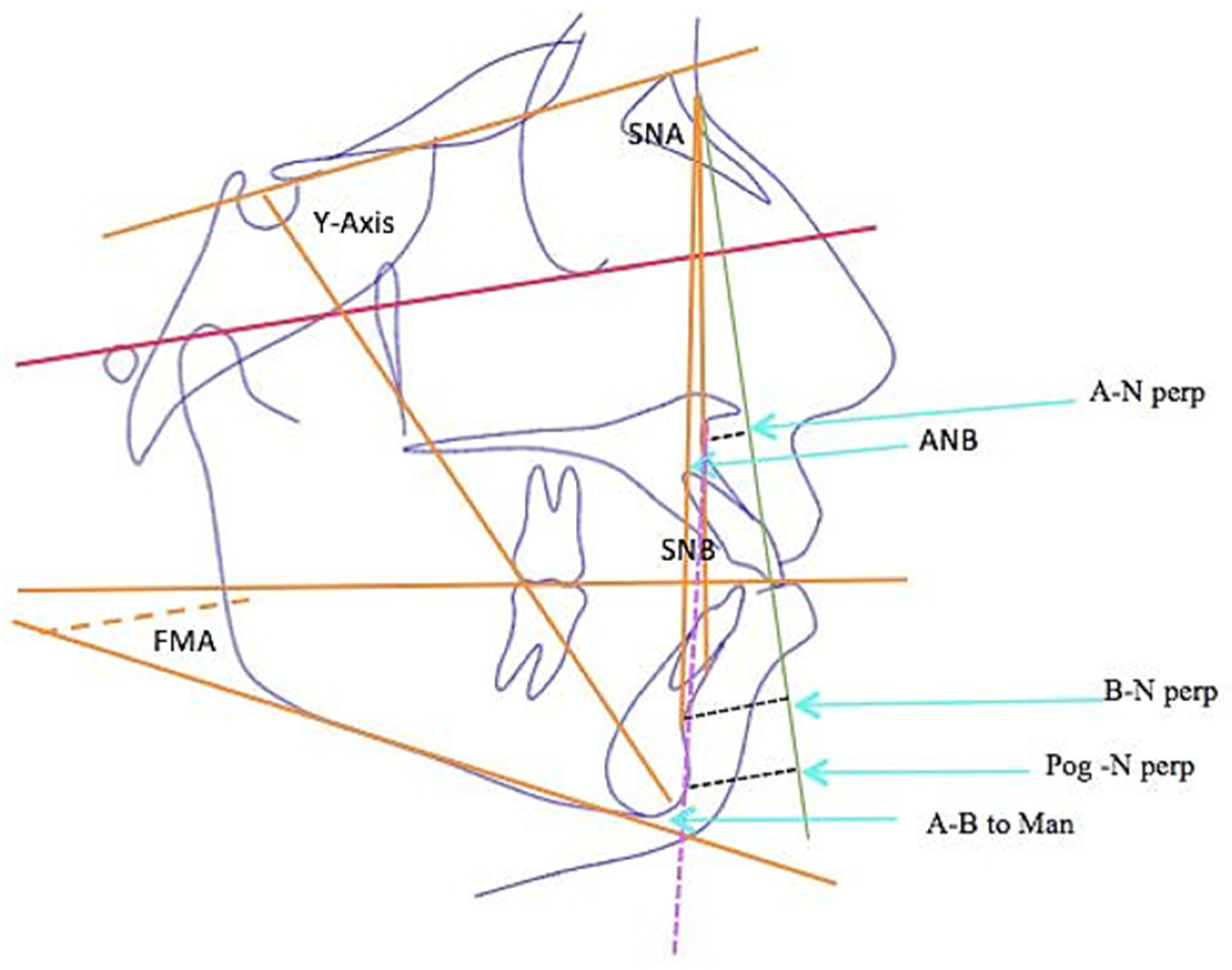
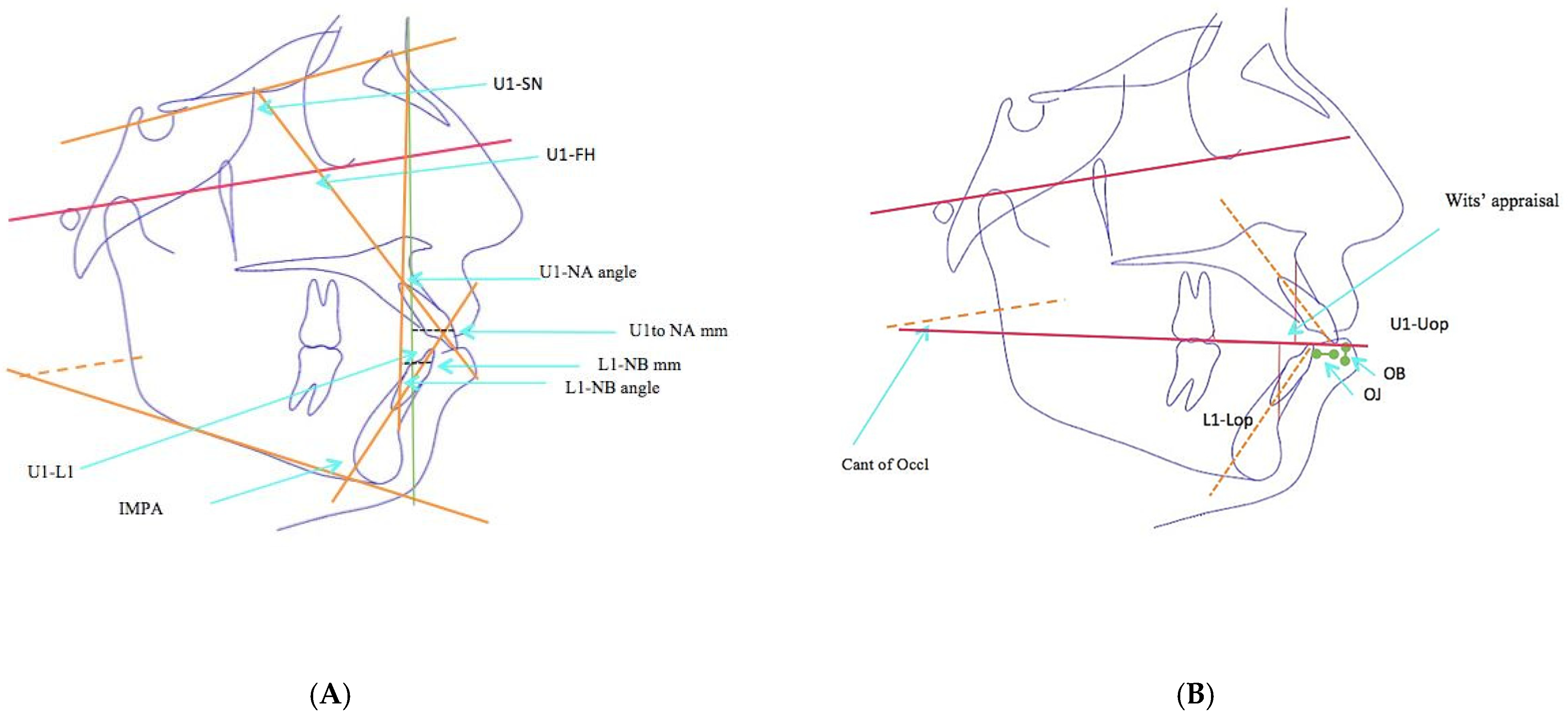
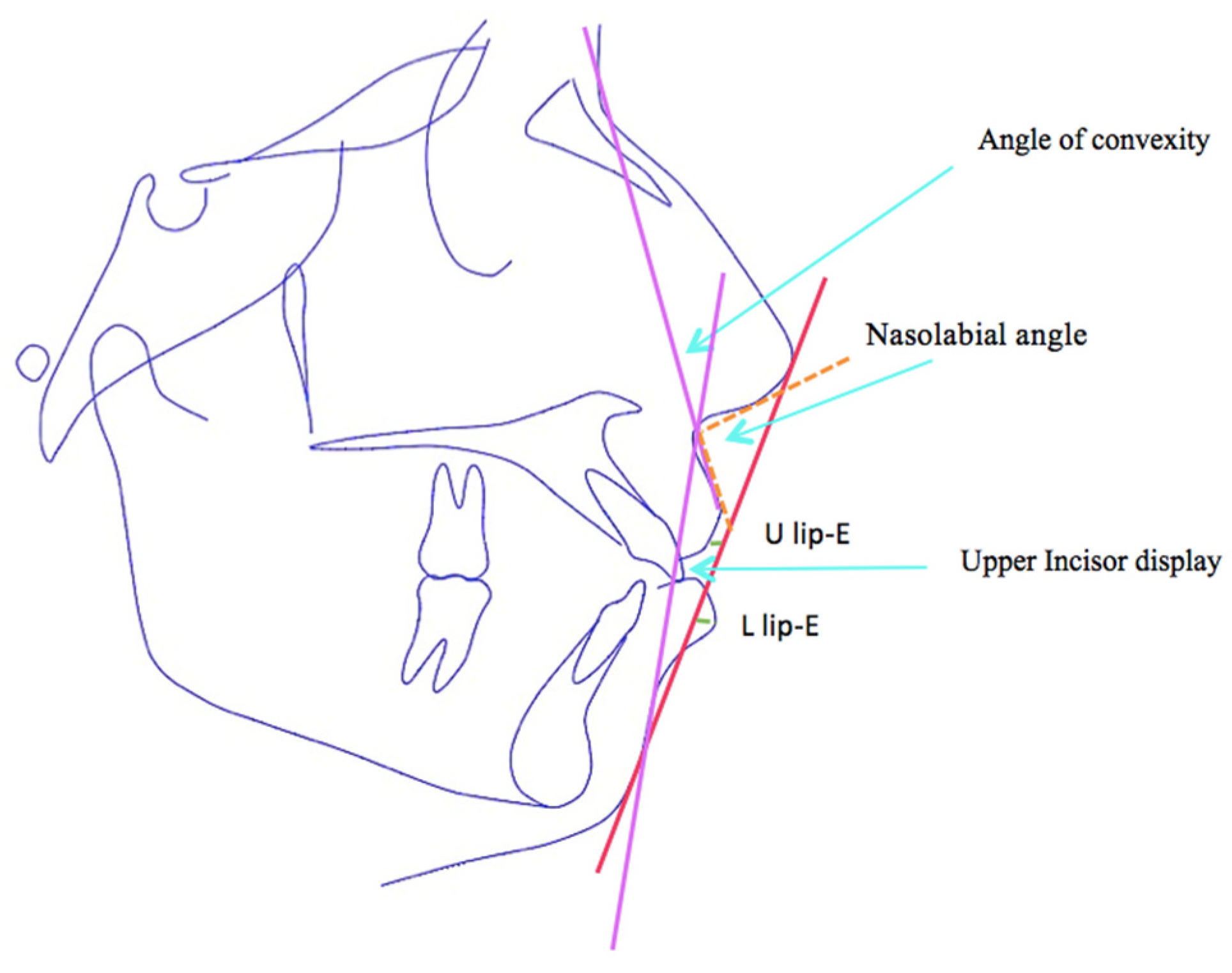
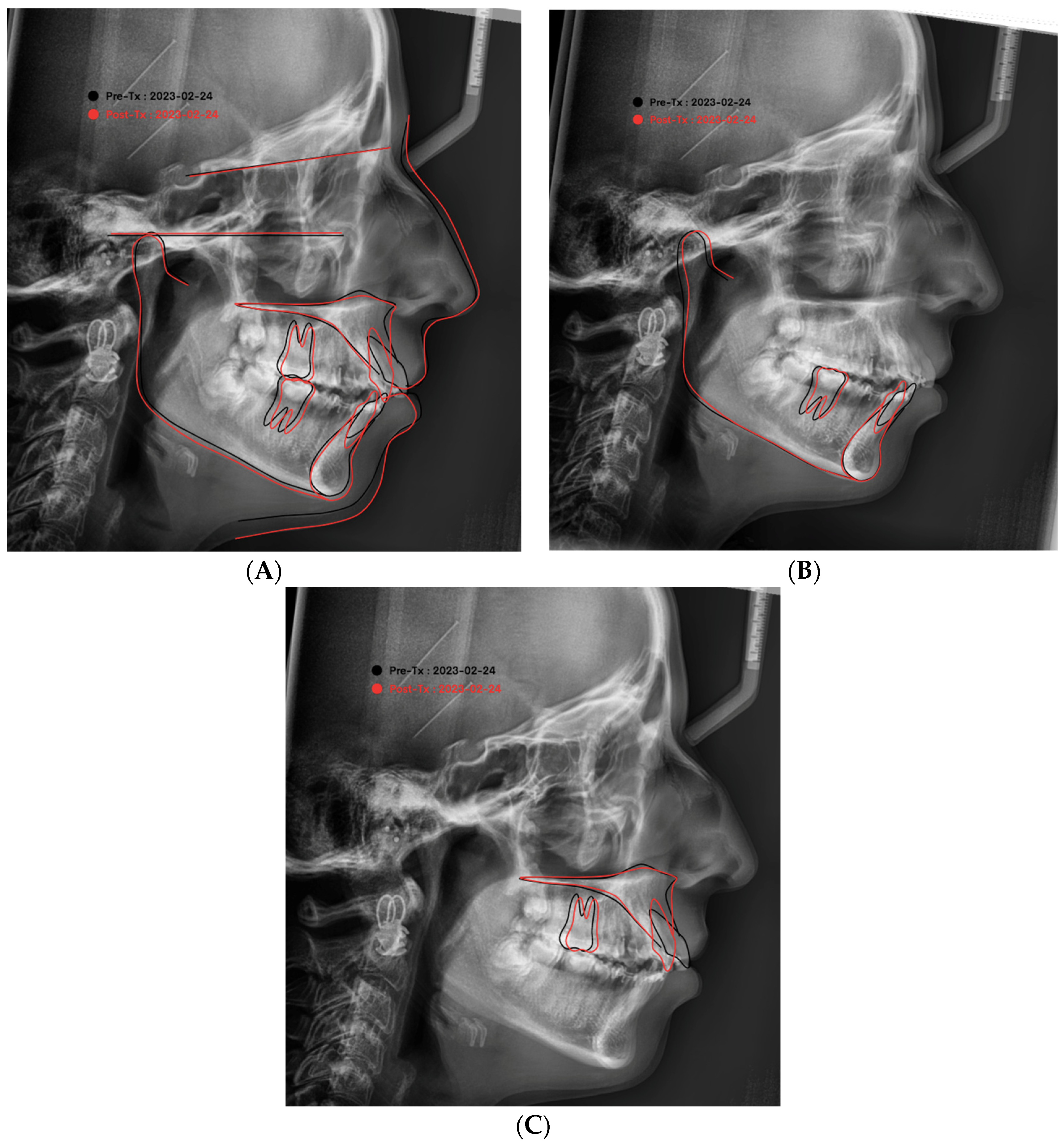
2.4. Cephalometric Analysis
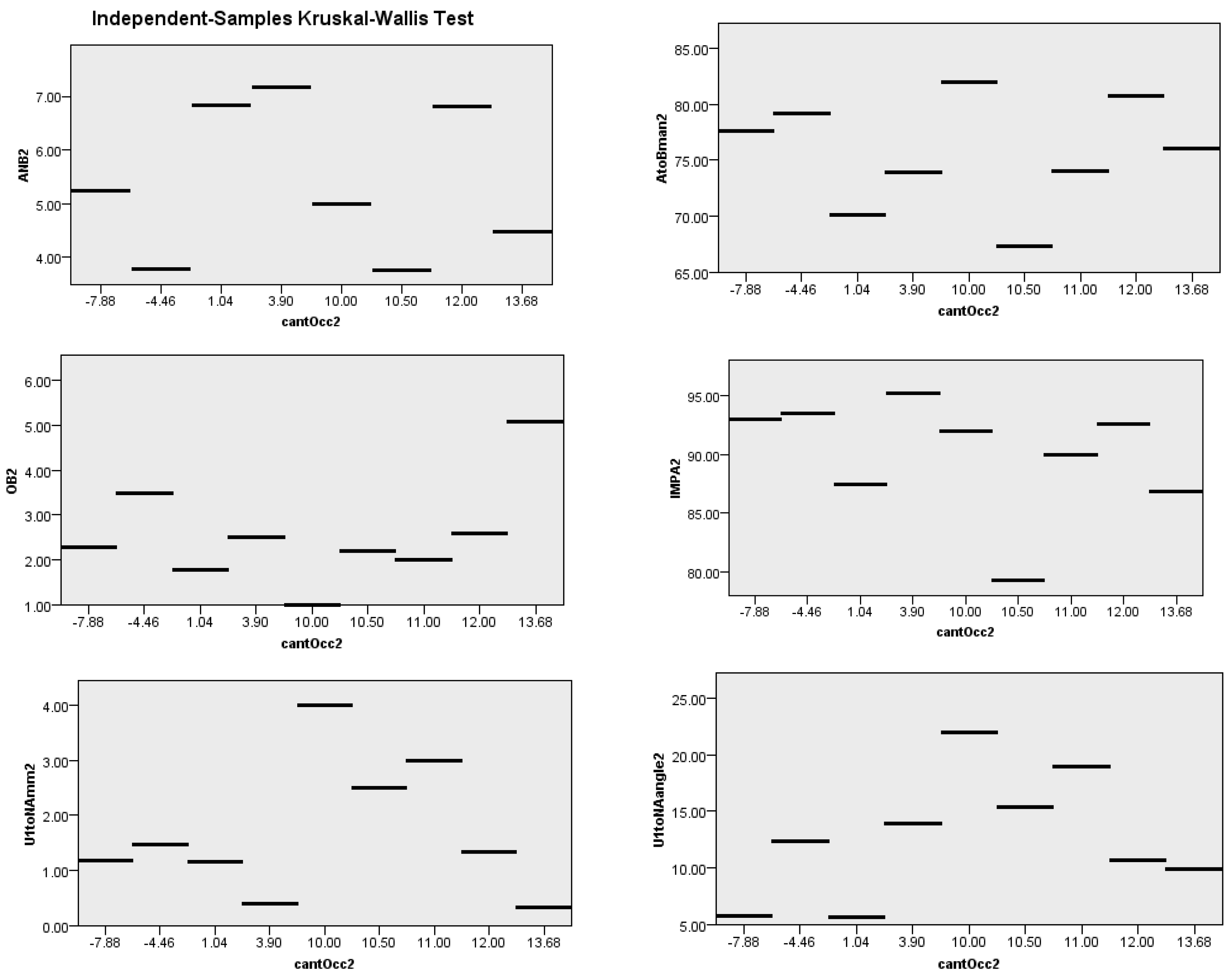
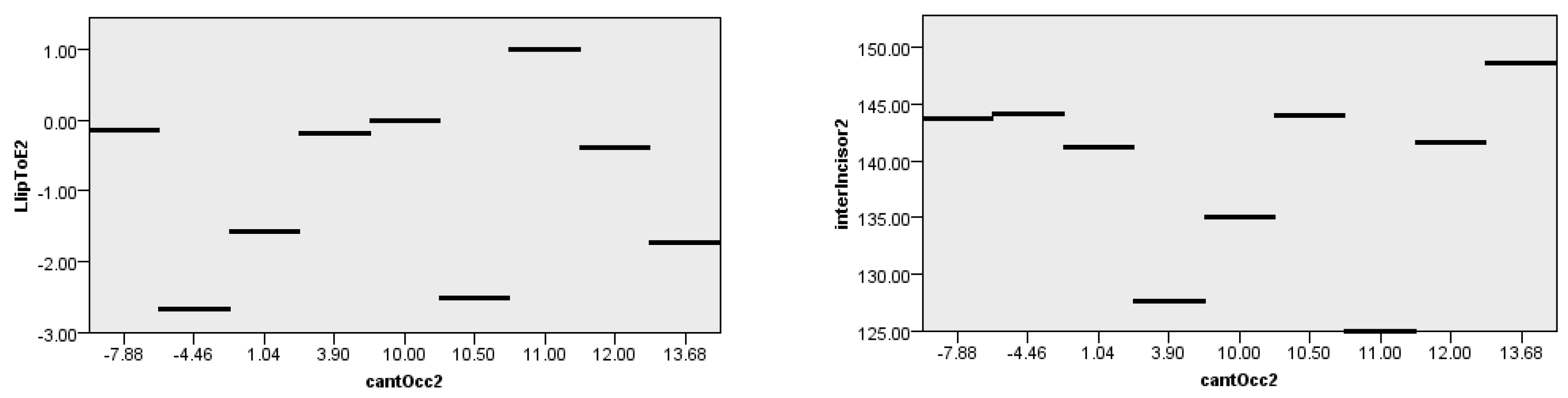
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Description |
| AP-line | The angle between long axis of the most-anteriorly positioned maxillary incisor and the line passing through Point A and the pogonion |
| SNA | The angle between SN-line and NA-line: sagittal position of maxilla |
| SNB | The angle between SN-line and NB-line: sagittal position of mandible |
| ANB | The angle between Point A, nasion, and Point B: sagittal base relation of jaws |
| FMA | The angle between the mandibular plane and Frankfort horizontal plane |
| Y axis-FH | The angle formed by the intersection between the sella gnathion and the FH plane estimate of the mandibular growth direction; also indicates the degree of the downward and forward position of the chin in relation to the upper face |
| A to N perp (FH) | The perpendicular distance from Point A to A-N when it is drawn perpendicular to the FH plane |
| B to N perp (FH) | The perpendicular distance from Point B to B-N when it is drawn perpendicular to the FH plane |
| Pog to N perp (FH) | The perpendicular distance from Pog to Pog-N when it is drawn perpendicular to the FH plane |
| FH to AB | The angle between the line connecting Point A to Point B and the Frankfort horizontal plane |
| A-B to mandibular plane | The angle between the line connecting Point A to Point B and the mandibular plane |
| Wit’s appraisal | The millimeter distance between two perpendicular lines, from Point A and Point B onto the occlusal plane. |
| OJ | The vertical distance between the incisal ridges of the most-anteriorly positioned maxillary and mandibular incisors |
| OB | The sagittal distance between the incisal ridge of the most-anteriorly positioned maxillary incisor and the labial surface of the most-anteriorly positioned mandibular incisor |
| U1 to FH | The angle between the long axis of the most-anteriorly positioned maxillary incisor and the Frankfort plane |
| U1 to SN | The angle between the long axis of the most-anteriorly positioned maxillary incisor and SN plane (inclination of upper incisors) |
| U1 to Uop | The angle between the upper inclination line and the upper occlusal line |
| IMPA | The angle formed by the long axis of the most-anteriorly positioned lower incisor and the mandibular plane (lower incisor inclination) |
| L1 to Lop | The angle between the lower incisor inclination line and the lower occlusal line |
| Interincisal angle | The interincisal angle between the long axes of the most anteriorly positioned maxillary and mandibular incisors |
| Cant of occlusal plane | The steepness of the occlusal plane in relation to the mandibular plane |
| U1 to NA (mm) | The perpendicular distance from the most-prominent point on the labial surface of the upper incisor to the NA-line |
| U1 to NA (deg) | The angle formed by the upper inclination line and the NA-line |
| L1 to NB (mm) | The perpendicular distance from the most-prominent point on the labial surface of the lower incisor to the NB-line |
| L1 to NB (deg) | The angle formed by the lower inclination line and the NB-line |
| Upper lip to E-plane | The distance of the lower lip to the aesthetic line (E-line), perpendicular to the E-line |
| Lower lip to E-plane | The distance of the upper lip to the aesthetic line (E-line), perpendicular to the E-line |
| Nasolabial angle | The angle formed by the two lines passing through the lower edge of the nose (the columella) and the edge of the upper lip |
| Upper incisal display | The display of the upper incisor on the lateral cephalogram |
References
- Soheilifar, S.; Ataei, H.; Mollabashi, V.; Amini, P.; Bakhshaei, A.; Naghdi, N. Extraction versus non-extraction orthodontic treatment: Soft tissue profile changes in borderline class I patients. Dent. Med. Probl. 2020, 57, 275–283. [Google Scholar]
- Alqahtani, N.D.; Alqasir, A.; Al-Jewair, T.; Almoammar, K.; Albarakati, S.F. Dental and soft tissue changes following extraction of second premolars in females with bimaxillary protrusion: A retrospective study. Niger. J. Clin. Pract. 2020, 23, 1110. [Google Scholar] [CrossRef] [PubMed]
- Benson, P.E.; Alshawy, E.; Fenton, G.D.; Frawley, T.; Misra, S.; Ng, T.; O’Malley, P.; Smith, G. Extraction vs. nonextraction of premolars for orthodontic treatment: A scoping review examining the extent, range, and characteristics of the literature. Am. J. Orthod. Dentofac. Orthop. 2023. [Google Scholar] [CrossRef] [PubMed]
- Baik, W.; Choi, S.H.; Cha, J.Y.; Yu, H.S.; Lee, K.J. Comparison of soft tissue changes between incisor tipping and translation after premolar extraction. Korean J. Orthod. 2022, 52, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Thakral, R.; Kapoor, S.; Shukla, P.; Sharma, V.K.; Bhagchandani, J.; Agarwal, S.; Jaiswal, R. Perception of facial esthetics in young North Indian population. J. Orthod. Sci. 2022, 11, 21. [Google Scholar] [PubMed]
- Proffit, W.R.; Fields, H.W.; Sarver, D.M. Contemporary Orthodontics, 6th ed.; Mosby: St Louis, MO, USA, 2019; Volume 88–90, pp. 301–302. [Google Scholar]
- Ramaut, L.; Tonnard, P.; Verpaele, A.; Verstraete, K.; Blondeel, P. Aging of the upper lip: Part I: A retrospective analysis of metric changes in soft tissue on magnetic resonance imaging. Plast. Reconstr. Surg. 2019, 143, 440–446. [Google Scholar] [CrossRef]
- Xing, L.; Zhang, X.; Guo, Y.; Bai, D.; Xu, H. XGBoost-aided prediction of lip prominence based on hard-tissue measurements and demographic characteristics in an Asian population. Am. J. Orthod. Dentofac. Orthop. 2023. [Google Scholar] [CrossRef]
- Srisuk, N. Profile Perception and Preference in Australian Groups. Master’s Thesis, University of Sydney, Sydney, Australia, 1982. [Google Scholar]
- Akyalcin, S.; Hazar, S.; Guneri, P.; Gogus, S.; Erdinc, A.M. Extraction versus non-extraction: Evaluation by digital subtraction radiography. Eur. J. Orthod 2007, 29, 639–647. [Google Scholar] [CrossRef] [Green Version]
- Bishara, S.E.; Cummins, D.M.; Jakobsen, J.R.; Zaher, A.R. Dentofacial and soft tissue changes in class II, division 1 cases treated with and without extractions. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 28–37. [Google Scholar] [CrossRef]
- Luppanapornlarp, S.; Johnston, L.E., Jr. The effects of premolar-extraction: A long-term comparison of outcomes in “clear-cut” extraction and nonextraction class II patients. Angle Orthod. 1993, 63, 257–272. [Google Scholar]
- Razin, S.M.A.; Ghani, S.H.A.; Norman, N.H. Bimaxillary Protrusion in Malay Population: Cephalometric Analysis of Skeletal, Dental and Soft Tissue Components. J. Int. Dent. Med. Res. 2019, 12, 203. [Google Scholar]
- Ribeiro, G.L.; Jacob, H.B. Understanding the basis of space closure in Orthodontics for a more efficient orthodontic treatment. Dent. Press J. Orthod. 2016, 21, 115–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobson, A.; Jacobson, R.L. Radiographic cephalometry technique. In Rdiographic Cephalometry: From Basics to 3-D Imaging, 2nd ed.; Jacobson, A., Jacobson, R.L., Eds.; Quintessence Publishing: Chicago, IL, USA, 2006; pp. 33–45. [Google Scholar]
- Solem, R.C.; Marasco, R.; Guiterrez-Pulido, L.; Nielsen, I.; Kim, S.H.; Nelson, G. Three-dimensional soft-tissue and hard-tissue changes in the treatment of bimaxillary protrusion. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 218–228. [Google Scholar] [CrossRef]
- Trisnawaty, N.; Ioi, H.; Kitahara, T.; Suzuki, A.; Takahashi, I. Effects of extraction of four premolars on vermilion height and lip area in patients with bimaxillary protrusion. Eur. J. Orthod. 2013, 35, 521–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghafari, J.; Engel, F.E.; Laster, L.L. Cephalometric superimposition on the cranial base: A review and a comparison of four methods. Am. J. Orthod. Dentofac. Orthop. 1987, 91, 403–413. [Google Scholar] [CrossRef]
- Antony PP, V.; Francis, P.G. A Retrospective Evaluation of Treatment Outcomes Obtained with Two Orthodontic Appliance Systems in the Treatment of Class I Bimaxillary Dento-Alveolar Protrusion Patients. J. Res. Adv. Dent. 2018, 7, 65–72. [Google Scholar]
- Allgayer, S.; Mezomo, M.B. Do premolar extractions necessarily result in a flat face? No, when properly indicated. Dent. Press J. Orthod. 2018, 23, 82–92. [Google Scholar] [CrossRef]
- Nance, H.N. The removal of second premolars in orthodontic treatment. Am. J. Orthod. 1949, 35, 685–696. [Google Scholar] [CrossRef]
- Flores-Mir, C.; Silva, E.; Barriga, M.I.; Lagravere, M.O.; Major, P.W. Lay person’s perception of smile aesthetics in dental and facial views. J. Orthod. 2004, 31, 204–209. [Google Scholar] [CrossRef]
- Beukes, S.; Dawjee, S.M.; Hlongwa, P. Soft tissue profile analysis in a sample of South African Blacks with bimaxillary protrusion. SADJ 2007, 62, 206–212, 206, 208–210, 212. [Google Scholar]
- Guimarães, A.; Lacerda-Santos, R.; Braga, E. Does the aesthetic perception of protrusion correction change if the face is evaluated from the frontal or profile perspectives? Res. Soc. Dev. 2023, 12, e20712441195. [Google Scholar] [CrossRef]
- Ren, H.; Chen, X.; Zhang, Y. Correlation between facial attractiveness and facial components assessed by laypersons and orthodontists. J. Dent. Sci. 2021, 16, 431–436. [Google Scholar] [CrossRef]
- Sadry, S.; Koru, B.E.; Kayalar, E. Analyzing the effects of tooth extraction on the lip in orthodontic treatment. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e126–e132. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wen, J.; Huang, L.; Zhang, L.; Han, L.; Li, H. Comparisons of maxillary incisor retraction effects for patients with first premolar extractions between Damon Q and Invisalign®: A retrospective study. Medicine 2022, 101, e30919. [Google Scholar] [CrossRef] [PubMed]
- Knigge, R.P.; McNulty, K.P.; Oh, H.; Hardin, A.M.; Leary, E.V.; Duren, D.L.; Valiathan, M.; Sherwood, R.J. Geometric morphometric analysis of growth patterns among facial types. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 430–441. [Google Scholar] [CrossRef] [PubMed]
- Kirschneck, C.; Proff, P.; Reicheneder, C.; Lippold, C. Short-term effects of systematic premolar extraction on lip profile, vertical dimension and cephalometric parameters in borderline patients for extraction therapy—A retrospective cohort study. Clin. Oral Investig. 2016, 20, 865–874. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Skeletal Parameters | Normal Values | No. | Results | Mean Diff. | Sig. (2-Tailed) | Wilcoxon Related Test | ||
|---|---|---|---|---|---|---|---|---|
| Mean ± Sd | Mean | Sd | ||||||
| 1. | SNA | 81.08 ± 3.7 | 20 | 81.88° | 4.05 | 1.36 | 0.000 * | |
| SNA2 | 20 | 80.52° | 3.64 | |||||
| 2. | SNB | 79.17 ± 3.8 | 20 | 76.23° | 3.55 | 0.53 | 0.001 * | |
| SNB2 | 20 | 74.70° | 2.72 | |||||
| 3. | ANB | 2.46 ± 1.8 | 20 | 5.47° | 1.58 | 0.02 | 0.863 | |
| ANB2 | 18 | 5.45° | 1.30 | |||||
| 4. | Y axis-FH | 59 ± 6 | 20 | 61.95° | 4.78 | 4.83 | 0.014 * | |
| Y axis-FH 2 | 20 | 57.12° | 11.16 | |||||
| 5. | FMA | 25 ± 4 | 20 | 25.7° | 6.14 | 2.1 | 0.000 * | |
| FMA2 | 20 | 23.58° | 6.51 | |||||
| 6. | A-N perp | 0.4 ± 2.3 | 20 | 2.3 | 5.62 | 0.23 | 0.654 | |
| A-N perp2 | 20 | 2.07 | 5.41 | |||||
| 7. | B-N prep | −3.5 ± 2 | 20 | −4.49 | 8.99 | −10.29 | 0.167 | |
| B-N perp2 | 20 | −5.8 | 8.36 | |||||
| 8. | Pog-N perp | −1.8 ± 4.5 | 20 | −4.12 | 10.03 | 1.5 | 0.231 | |
| Pog-N perp2 | 20 | −5.62 | 9.10 | |||||
| 9. | A-B to Man1 | 69.3 ± 2.5 | 20 | 74.71 | 5.71 | −1.31 | 0.002 * | |
| A-B to Man2 | 20 | 76.02 | 4.62 | |||||
| Dental Variables | Normal Values | No. | Results | Mean Diff. | Sig. (2-Tailed) | Wilcoxon Related Test | ||
|---|---|---|---|---|---|---|---|---|
| Mean ± Sd | Mean | Sd | ||||||
| 1. | Wit’s appraisal | −2.74 ± 0.3 | 20 | 3.05 | 1.69 | 0.65 | 0.057 | |
| Wit’s appraisal2 | 20 | 2.40 | 2.46 | |||||
| 2. | OJ | 2 ± 2 | 20 | 4.01 | 1.73 | 1.23 | 0.002 * | |
| OJ2 | 20 | 2.78 | 1.21 | |||||
| 3. | OB | 2 ± 2 | 20 | 1.22 | 2.59 | −1.32 | 0.038 * | |
| OB2 | 20 | 2.54 | 1.07 | |||||
| 4. | U1-FH | 113.8 ± 6.4 | 20 | 118.82° | 4.75 | 16.08 | 0.000 * | |
| U1-FH2 | 20 | 102.74° | 5.42 | |||||
| 5. | U1-SN | 105.28 ± 6.6 | 20 | 109.88° | 5.94 | 18.03 | 0.000 * | |
| U1-SN2 | 20 | 91.85° | 5.88 | |||||
| 6. | U1-Uop2 | 55 ± 4 | 20 | 54.39° | 3.92 | 9 | 0.000 * | |
| U1-Uop | 20 | 63.37° | 6.83 | |||||
| 7. | IMPA | 90 ± 3.5 | 20 | 104.02° | 7.37 | 13.76 | 0.000 * | |
| IMPA2 | 20 | 90.26° | 4.57 | |||||
| 8. | L1-Lop | 66 ± 5 | 20 | 55.8 | 5 | −10.51 | 0.000 | |
| L1 to Lop | 20 | 55.81° | 4.90 | |||||
| L1-Lop2 | 20 | 66.32° | 4.87 | |||||
| 9. | U1-L1 | 130 ± 5.8 | 20 | 116.84° | 13.62 | −13.69 | 0.000 * | |
| Interincisal angle2 | 20 | 130.53° | 15.67 | |||||
| 10. | Cant of Occl | 9.3 ± 3.8 | 20 | 6.31° | 4.63 | −1.24 | 0.282 | |
| Cant of Occl2 | 20 | 7.55° | 6.03 | |||||
| 11. | U1-NA mm | 4 ± 3 | 20 | 5.70 | 2.36 | 4.04 | 0.000 * | |
| U1-NA mm2 | 20 | 1.66 | 1.13 | |||||
| 12. | U1-NA angle | 22 ± 5 | 20 | 25.29° | 6.57 | 13 | 0.000 * | |
| U1-NA angle2 | 20 | 12.29° | 5.33 | |||||
| 13. | L1-NB mm | 4 ± 2 | 20 | 9.14 | 1.70 | 4.11 | 0.000 * | |
| L1-NB mm2 | 20 | 5.03 | 1.43 | |||||
| 14. | L1-NB angle | 25 ± 5 | 20 | 36.2° | 4.72 | 13.41 | 0.000 * | |
| L1-NB angle2 | 20 | 22.79° | 4.39 | |||||
| Soft Tissue Variables | Normal Values | No. | Results | Mean Diff. | Sig. (2-Tailed) | Wilcoxon Related Test | ||
|---|---|---|---|---|---|---|---|---|
| Mean ± Sd | Mean | Sd | ||||||
| 1. | U lip to E | −4.7 ± 2 | 20 | −1.12 | 1.41 | 2.91 | 0.000 * | |
| U lip to E2 | 20 | −3.65 | 1.03 | |||||
| 2. | L lip to E | −2 ± 2 | 20 | 1.61 | 1.55 | 2.46 | 0.000 * | |
| L lip to E2 | 20 | −0.85 | 1.17 | |||||
| 3. | Nasolabial angle | 95 ± 5 | 20 | 94.85° | 9.66 | −1.6 | 0.55 | |
| Nasolabial angle 2 | 20 | 96.45° | 6.96 | |||||
| 4. | Angle of Conv | 0 ± 5.1 | 20 | 10.92° | 3.54 | 1.13 | 0.02 * | |
| Angle of Conv2 | 20 | 9.79° | 3.24 | |||||
| 5. | U incisor display | 2.5 ± 1.5 | 20 | 3.18 | 2.43 | 0.38 | 0.145 | |
| U incisor disply2 | 20 | 2.80 | 1.13 | |||||
| Spearman’s Rank Cant Occlusal | N | Correlation Coefficient | Sig. (2-Tailed) |
|---|---|---|---|
| SNA2 | 20 | −0.142 | 0.550 |
| FMA2 | 20 | 0.717 ** | 0.000 |
| Gon angle2 | 20 | 0.322 | 0.167 |
| OJ2 | 20 | 309 | 0.185 |
| U1 to FH2 | 20 | −0.894 ** | 0.000 |
| U1 to SN2 | 20 | 0.007 | 0.977 |
| U1 to Uop2 | 20 | −0.325 | 0.162 |
| L1 to Lop2 | 20 | 0.422 | 0.064 |
| L1 to NBmm2 | 20 | −0.130 | 0.585 |
| L1 to NBangle2 | 20 | −0.072 | 0.761 |
| Angle convex2 | 20 | 0.107 | 0.653 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmood, T.M.A. Occlusal Plane Steepness and Profile Change Following TAD-Based One-Step Retraction on Four-Unit Extraction Cases: A Retrospective Study. Diagnostics 2023, 13, 2395. https://doi.org/10.3390/diagnostics13142395
Mahmood TMA. Occlusal Plane Steepness and Profile Change Following TAD-Based One-Step Retraction on Four-Unit Extraction Cases: A Retrospective Study. Diagnostics. 2023; 13(14):2395. https://doi.org/10.3390/diagnostics13142395
Chicago/Turabian StyleMahmood, Trefa Mohammed Ali. 2023. "Occlusal Plane Steepness and Profile Change Following TAD-Based One-Step Retraction on Four-Unit Extraction Cases: A Retrospective Study" Diagnostics 13, no. 14: 2395. https://doi.org/10.3390/diagnostics13142395