
Drug-Associated Gastropathy: Diagnostic Criteria

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Non-Steroid Anti-Inflammatory Drugs/Acetylsalicylic Acid (NSAIDs/Aspirin)
2.1. Epidemiology
2.2. Risk Factors
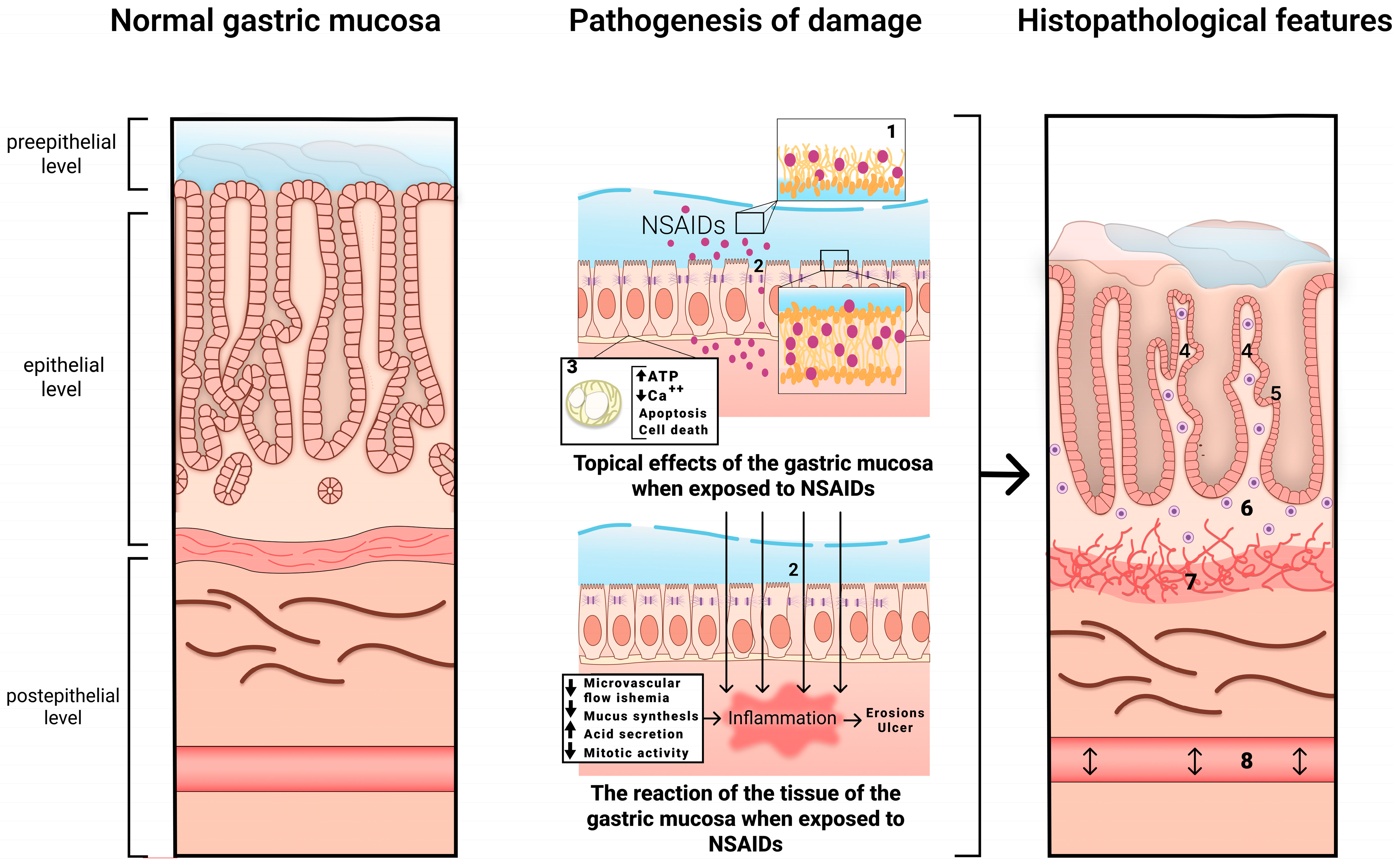
2.3. Mechanism of Gastric Damage
2.4. Clinical Manifestations
2.5. Endoscopic Picture
2.6. Histological Examination
3. Anticoagulants
3.1. Epidemiology
3.2. Risk Factors
- -
- A history of gastrointestinal bleeding;
- -
- A history of gastric and/or duodenal ulcers;
- -
- Gastroesophageal reflux disease, reflux esophagitis;
- -
- Chronic H. pylori-associated gastritis;
- -
- Other pathologies of the gastrointestinal tract: inflammatory bowel disease, diverticula, hemorrhoids and angiodysplasia;
- -
- Neoplasms of the gastrointestinal tract in history;
- -
- Age > 65 years;
- -
- Concomitant use of NSAIDs (including LDA) or other drugs that affect blood coagulation or have a contact damaging effect on the gastrointestinal tract;
- -
- Impaired renal function: glomerular filtration rate (GFR) < 50 mL/min;
- -
- Use of high doses of NOACs (dabigatran 300 mg/day, edoxaban 60 mg/day).
3.3. Mechanism of Gastric Damage
3.4. Clinical Manifestations
3.5. Endoscopic Picture
4. Cytostatics
4.1. Epidemiology
4.2. Risk Factors
4.3. Mechanism of Gastric Damage
4.4. Clinical Manifestations
4.5. Endoscopic Picture
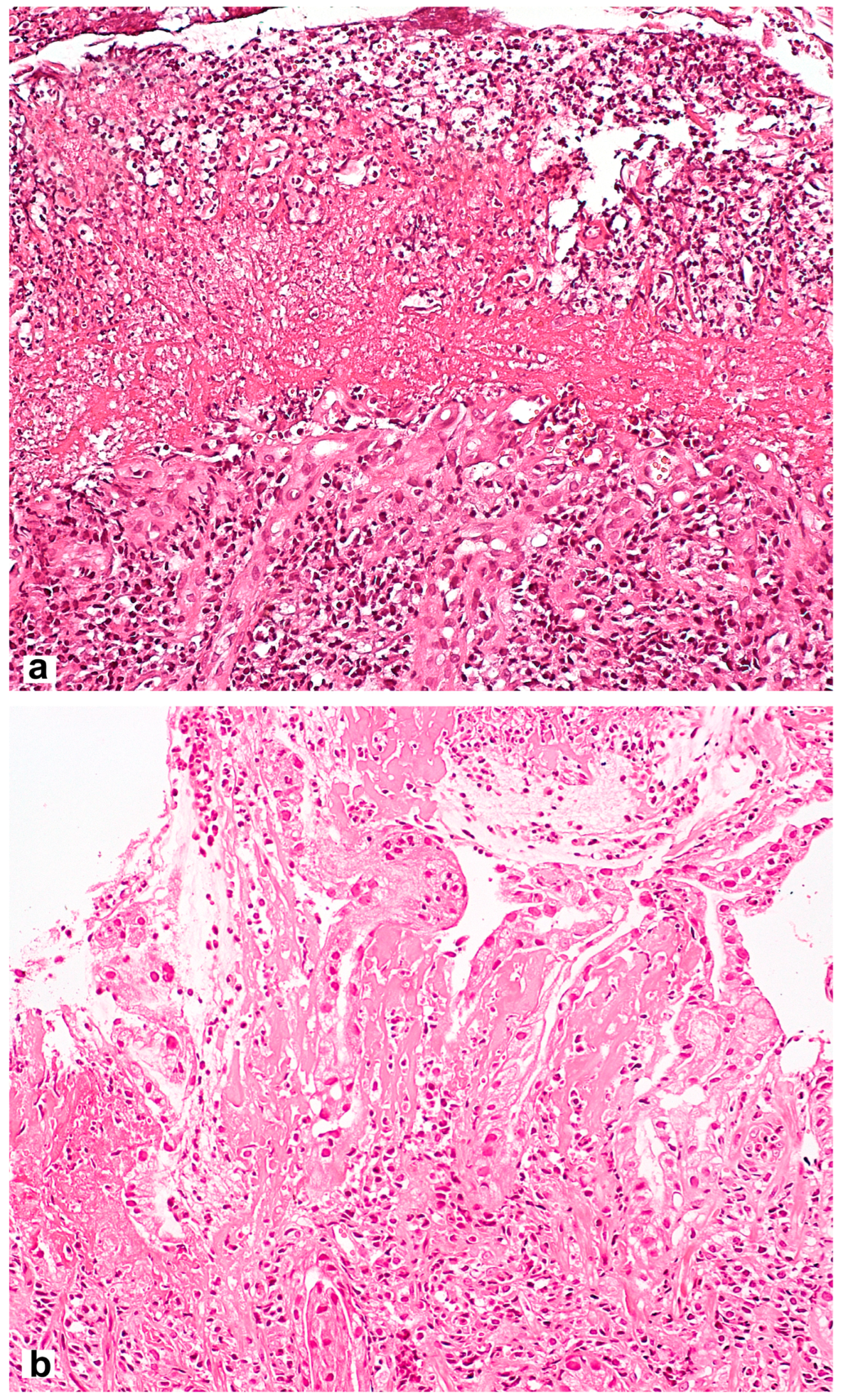
4.6. Histological Examination
5. Immune Checkpoint Inhibitors
5.1. Epidemiology
5.2. Risk Factors
5.3. Mechanism of Gastric Damage
5.4. Clinical Manifestations
5.5. Endoscopic Picture
5.6. Histological Examination
6. Glucocorticosteroids (GCSs)
6.1. Epidemiology
6.2. Risk Factors
6.3. Mechanism of Gastric Damage
6.4. Clinical Manifestations
6.5. Endoscopic Picture
6.6. Histological Examination
7. Iron Drugs
7.1. Epidemiology
7.2. Risk Factors
7.3. Mechanism of Gastric Damage
7.4. Clinical Manifestations
7.5. Endoscopic Picture
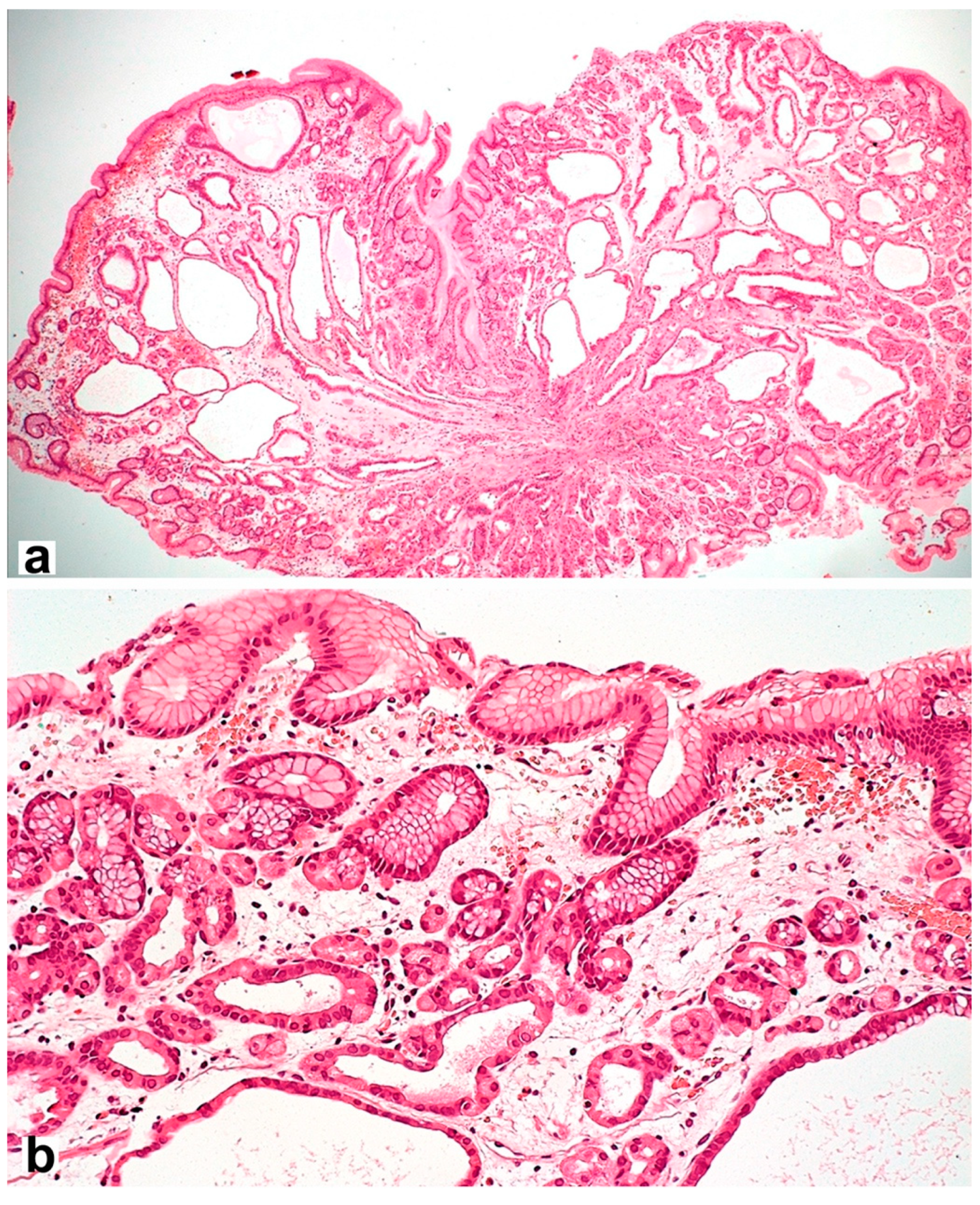
7.6. Histological Examination
8. Proton Pump Inhibitors (PPIs)
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sugano, K.; Tack, J.; Kuipers, E.J.; Graham, D.Y.; El-Omar, E.M.; Miura, S.; Haruma, K.; Asaka, M.; Uemura, N.; Malfertheiner, P.; et al. Kyoto global consensus report on Helicobacter pylori gastritis. Gut 2015, 64, 1353–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douthwaite, A.H.; Lintott, G.A. Gastroscopic observation of the effect of aspirin and certain other substances on the stomach. Lancet 1938, 232, 1222–1225. [Google Scholar] [CrossRef]
- Pilotto, A.; Franceschi, M.; Leandro, G.; Di Mario, F.; Geriatric Gastroenterology Study Group (Societe Italiana Gerontologie Geriatria). NSAID and aspirin use by the elderly in general practice: Effect on gastrointestinal symptoms and therapies. Drugs Aging. 2003, 20, 701–710. [Google Scholar] [CrossRef]
- Laine, L. Approaches to nonsteroidal anti-inflammatory drug use in the high-risk patient. Gastroenterology 2001, 120, 594–606. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.N.M.; Sha, S.; Cnen, L.J.; Holleczek, B.; Brenner, H.; Schottker, B. Strongly increased risk of gastric and duodenal ulcers among new users of low-dose aspirin: Results from two large cohorts with new-user design. Aliment. Pharmacol. Ther. 2022, 56, 251–262. [Google Scholar] [CrossRef]
- Lanas, A.; Perez-Aisa, M.A.; Feu, F.; Ponce, J.; Saperas, E.; Santolaria, S.; Rodrigo, L.; Balanzo, J.; Bajador, E.; Almero, P.; et al. A nationwide study of mortality associated with hospital admission due to severe gastrointestinal events and those associated with nonsteroidal anti-inflammatory drug use. Am. J. Gastroenterol. 2005, 100, 1685–1693. [Google Scholar] [CrossRef]
- Joo, M.K.; Park, C.H.; Kim, J.S.; Park, J.M.; Ahn, J.Y.; Lee, B.E.; Lee, J.H.; Yang, H.J.; Cho, Y.K.; Bang, C.S.; et al. Clinical Guidelines for Drug-Related Peptic Ulcer, 2020 Revised Edition. Gut Liver 2020, 14, 707–726. [Google Scholar] [CrossRef]
- Lanas, A. A review of the gastrointestinal safety data-a gastroenterologist’s perspective. Rheumatology 2010, 49, ii3–ii10. [Google Scholar] [CrossRef] [Green Version]
- Bjarnason, I.; Scarpignato, C.; Holmgren, E.; Olszewski, M.; Rainsford, K.D.; Lanas, A. Mechanisms of Damage to the Gastrointestinal Tract FromNonsteroidal Anti-Inflammatory Drugs. Gastroenterology 2018, 154, 500–514. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.; Huang, H.; Guo, Z.; Chang, Y.; Li, Z. Role of prostaglandin E2 in tissue repair and regeneration. Theranostics 2021, 11, 8836–8854. [Google Scholar] [CrossRef] [PubMed]
- Laporte, J.R.; Ibáñez, L.; Vidal, X.; Vendrell, L.; Leone, R. Upper gastrointestinal bleeding associated with the use of NSAIDs: Newer versus older agents. Drug Saf. 2004, 27, 411–420. [Google Scholar] [CrossRef]
- García Rodríguez, L.A.; Hernández-Díaz, S. Risk of uncomplicated peptic ulcer among users of aspirin and nonaspirin nonsteroidal antiinflammatory drugs. Am. J. Epidemiol. 2004, 159, 23–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorucci, S.; Antonelli, E.; Morelli, A. Mechanism of non-steroidal anti-inflammatory drug-gastropathy. Dig. Liver Dis. 2001, 33, S35–S43. [Google Scholar] [CrossRef] [PubMed]
- Santucci, L.; Fiorucci, S.; Giansanti, M.; Brunori, P.M.; Di Matteo, F.M.; Morelli, A. Pentoxifylline prevents indomethacin induced acute gastric mucosal damage in rats: Role of tumour necrosis factor alpha. Gut 1994, 35, 909–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bresalier, R.S.; Sandler, R.S.; Quan, H.; Bolognese, J.A.; Oxenius, B.; Horgan, K.; Lines, C.; Riddell, R.; Morton, D.; Lanas, A.; et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N. Engl. J. Med. 2005, 352, 1092–1102. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.D.; McMurray, J.J.; Pfeffer, M.A.; Wittes, J.; Fowler, R.; Finn, P.; Anderson, W.F.; Zauber, A.; Hawk, E.; Bertagnolli, M.; et al. Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. N. Engl. J. Med. 2005, 352, 1071–1080. [Google Scholar] [CrossRef] [Green Version]
- Coxib and Traditional NSAID Trialists’ (CNT) Collaboration; Bhala, N.; Emberson, J.; Merhi, A.; Abramson, S.; Arber, N.; Baron, J.A.; Bombardier, C.; Cannon, C.; Farkouh, M.E.; et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: Meta-analyses of individual participant data from randomised trials. Lancet 2013, 382, 769–779. [Google Scholar]
- Maev, I.V.; Andreev, D.N.; Dicheva, D.T.; Partsvania-Vinogradova, E.V. NSAID-induced gastropathies: Pathogenetically substantiated approaches to prevention and therapy. Farmateka 2016, 2, 49–54. [Google Scholar]
- Laine, L. Proton pump inhibitor co-therapy with nonsteroidal anti-inflammatory drugs--nice or necessary? Rev. Gastroenterol. Disord. 2004, 4, S33–S41. [Google Scholar]
- Fries, J.F.; Murtagh, K.N.; Bennett, M.; Zatarain, E.; Lingala, B.; Bruce, B. The rise and decline of nonsteroidal antiinflammatory drug-associated gastropathy in rheumatoid arthritis. Arthritis Rheum. 2004, 50, 2433–2440. [Google Scholar] [CrossRef]
- Lanas, Á.; Carrera-Lasfuentes, P.; Arguedas, Y.; García, S.; Bujanda, L.; Calvet, X.; Ponce, J.; Perez-Aísa, Á.; Castro, M.; Muñoz, M.; et al. Risk of upper and lower gastrointestinal bleeding in patients taking nonsteroidal anti-inflammatory drugs, antiplatelet agents, or anticoagulants. Clin. Gastroenterol. Hepatol. 2015, 13, 906–912.e2. [Google Scholar] [CrossRef] [PubMed]
- Lanza, F.L.; Chan, F.K.; Quigley, E.M.; Practice Parameters Committee of the American College of Gastroenterology. Guidelines for prevention of NSAID-related ulcer complications. Am. J. Gastroenterol. 2009, 104, 728–738. [Google Scholar] [PubMed]
- Otani, K.; Tanigawa, T.; Watanabe, T.; Shimada, S.; Nadatani, Y.; Nagami, Y.; Tanaka, F.; Kamata, N.; Yamagami, H.; Shiba, M.; et al. Microbiota Plays a Key Role in Non-Steroidal Anti-Inflammatory Drug-Induced Small Intestinal Damage. Digestion 2017, 95, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Maiden, L.; Thjodleifsson, B.; Theodors, A.; Gonzalez, J.; Bjarnason, I. A quantitative analysis of NSAID-induced small bowel pathology by capsule enteroscopy. Gastroenterology 2005, 128, 1172–1178. [Google Scholar] [CrossRef]
- Zhao, B.; Sanati, S.; Eltorky, M. Diaphragm disease: Complete small bowel obstruction after long-term nonsteroidal anti-inflammatory drugs use. Ann. Diagn. Pathol. 2005, 9, 169–173. [Google Scholar] [CrossRef]
- Grattagliano, I.; Ubaldi, E.; Portincasa, P. Drug-induced enterocolitis: Prevention and management in primary care. J. Dig. Dis. 2018, 19, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Gillen, D.; McColl, K.E. Problems associated with the clinical use of proton pump inhibitors. Pharmacol. Toxicol. 2001, 89, 281–286. [Google Scholar] [CrossRef]
- Stolte, M.; Panayiotou, S.; Schmitz, J. Can NSAID/ASA-induced erosions of the gastric mucosa be identified at histology? Pathol. Res. Pract. 1999, 195, 137–142. [Google Scholar] [CrossRef]
- Mihalkanin, L.; Stancak, B. The Impact of Novel Anticoagulants on the Upper Gastrointestinal Tract Mucosa. Medicina 2020, 56, 363. [Google Scholar] [CrossRef]
- Moudallel, S.; Eynde, C.v.D.; Malý, J.; Rydant, S.; Steurbaut, S. Retrospective analysis of gastrointestinal bleedings with direct oral anticoagulants reported to EudraVigilance. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2023, 396, 1143–1153. [Google Scholar] [CrossRef]
- Sobieraj, D.M.; White, C.M.; Alikhanov, S.; Winkler, S.; Mediouni, M.; Kluger, J.; Coleman, C.I. The impact of antiplatelet and anticoagulant therapies on gastrointestinal symptoms in patients with atrial fibrillation: A systematic review. Ann. Pharmacother. 2012, 46, 1220–1231. [Google Scholar] [CrossRef]
- Gu, Z.C.; Wei, A.H.; Zhang, C.; Wang, X.H.; Zhang, L.; Shen, L.; Li, Z.; Pan, M.M.; Liu, X.Y.; Pu, J.; et al. Risk of Major Gastrointestinal Bleeding With New vs Conventional Oral Anticoagulants: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2020, 18, 792–799.e61. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.S.; Leung, W.K. Gastrointestinal bleeding in patients on novel oral anticoagulants: Risk, prevention and management. World J. Gastroenterol. 2017, 23, 1954–1963. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; O’Morain, C.; et al. Management of Helicobacter pylori infection: The Maastricht VI/Florence consensus report. Gut 2022, 71, 1724–1762. [Google Scholar] [CrossRef] [PubMed]
- Desai, J.; Kolb, J.M.; Weitz, J.I.; Aisenberg, J. Gastrointestinal bleeding with the new oral anticoagulants-defining the issues and the management strategies. Thromb. Haemost. 2013, 110, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Vanassche, T.; Hirsh, J.; Eikelboom, J.W.; Ginsberg, J.S. Organ-specific bleeding patterns of anticoagulant therapy: Lessons from clinical trials. Thromb. Haemost. 2014, 112, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Kundu, A.; Sardar, P.; Sen, P.; Chatterjee, S.; Huston, J.; Nairooz, R.; Ryan, J.J.; Aronow, W.S. Patient Taking A Novel Oral Anticoagulant Presents with Major GI Bleeding. J. Atr. Fibrillation. 2015, 8, 1218. [Google Scholar]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar]
- Lauffenburger, J.C.; Rhoney, D.H.; Farley, J.F.; Gehi, A.K.; Fang, G. Predictors of gastrointestinal bleeding among patients with atrial fibrillation after initiating dabigatran therapy. Pharmacotherapy 2015, 35, 560–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlowski, A.; Gale, C.P.; Ashton, R.; Petrungaro, B.; Slater, R.; Nadarajah, R.; Cowan, J.C.; Buck, J.; Smith, W.; Wu, J. Clinical and budget impacts of changes in oral anticoagulation prescribing for atrial fibrillation. Heart Br. Card. Soc. 2021, 107, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Sarajlic, P.; Simonsson, M.; Jernberg, T.; Bäck, M.; Hofmann, R. Incidence, associated outcomes, and predictors of upper gastrointestinal bleeding following acute myocardial infarction: A SWEDEHEART-based nationwide cohort study. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 483–491. [Google Scholar] [CrossRef]
- Holster, I.L.; Valkhoff, V.E.; Kuipers, E.J.; Tjwa, E.T.T.L. New oral anticoagulants increase risk for gastrointestinal bleeding: A systematic review and meta-analysis. Gastroenterology 2013, 145, 105–112.e15. [Google Scholar] [CrossRef] [Green Version]
- Guo, W.-Q.; Chen, X.-H.; Tian, X.-Y.; Li, L. Differences In Gastrointestinal Safety Profiles Among Novel Oral Anticoagulants: Evidence From A Network Meta-Analysis. Clin. Epidemiol. 2019, 11, 911–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugisaki, N.; Iwakiri, R.; Tsuruoka, N.; Sakata, Y.; Shimoda, R.; Fujimoto, S.; Eguchi, Y.; Fujimoto, K. A case-control study of the risk of upper gastrointestinal mucosal injuries in patients prescribed concurrent NSAIDs and antithrombotic drugs based on data from the Japanese national claims database of 13 million accumulated patients. J. Gastroenterol. 2018, 53, 1253–1260. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, C.; Passerini, P. Gastrointestinal complications in renal transplant recipients. Transpl. Int. 2005, 18, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason, I. Enteric coating of mycophenolate sodium: A rational approach to limit topical gastrointestinal lesions and extend the therapeutic index of mycophenolate. Transplant. Proc. 2001, 33, 3238–3240. [Google Scholar] [CrossRef] [PubMed]
- Telkes, G.; Peter, A.; Tulassay, Z.; Asderakis, A. High frequency of ulcers, not associated with Helicobacter pylori, in the stomach in the first year after kidney transplantation. Nephrol. Dial. Transplant. 2011, 26, 727–732. [Google Scholar] [CrossRef] [Green Version]
- Pennelli, G.; Grillo, F.; Galuppini, F.; Ingravallo, G.; Pilozzi, E.; Rugge, M.; Fiocca, R.; Fassan, M.; Mastracci, L. Gastritis: Update on etiological features and histological practical approach. Pathologica 2020, 112, 153–165. [Google Scholar] [CrossRef]
- Staatz, C.E.; Tett, S.E. Clinical pharmacokinetics and pharmacodynamics of mycophenolate in solid organ transplant recipients. Clin. Pharmacokinet. 2007, 46, 13–58. [Google Scholar] [CrossRef]
- Abbass, A.; Khalid, S.; Boppana, V.; Hanson, J.; Lin, H.; McCarthy, D. Giant Gastric Ulcers: An Unusual Culprit. Dig. Dis. Sci. 2020, 65, 2811–2817. [Google Scholar] [CrossRef]
- Chang, V.C.; Mai, D.; Park, M.; Lee, D.; Samarasena, J. Mycophenolate mofetil-induced non-healing gastric and duodenal ulcers. Am. J. Gastroenterol. 2018, 113, S1089–S1090. [Google Scholar] [CrossRef]
- Parfitt, J.R.; Jayakumar, S.; Driman, D.K. Mycophenolate mofetil-related gastrointestinal mucosal injury: Variable injury patterns, including graft-versus-host disease-like changes. Am. J. Surg. Pathol. 2008, 32, 1367–1372. [Google Scholar] [CrossRef]
- Bunnapradist, S.; Ambühl, P.M. Impact of gastrointestinal-related side effects on mycophenolate mofetil dosing and potential therapeutic strategies. Clin. Transplant. 2008, 22, 815–821. [Google Scholar] [CrossRef]
- Parfitt, J.R.; Driman, D.K. Pathological effects of drugs on the gastrointestinal tract: A review. Hum. Pathol. 2007, 38, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Chehade, M.; Benkov, K. Gastrointestinal issues in children with rheumatologic disease. Curr. Rheumatol. Rep. 2002, 4, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Schadendorf, D.; Hodi, F.S.; Robert, C.; Weber, J.S.; Margolin, K.; Hamid, O.; Patt, D.; Chen, T.T.; Berman, D.M.; Wolchok, J.D. Pooled Analysis of Long-Term Survival Data From Phase II and Phase III Trials of Ipilimumab in Unresectable or Metastatic Melanoma. J. Clin. Oncol. 2015, 33, 1889–1894. [Google Scholar] [CrossRef] [Green Version]
- Beck, K.E.; Blansfield, J.A.; Tran, K.Q.; Feldman, A.L.; Hughes, M.S.; Royal, R.E.; Kammula, U.S.; Topalian, S.L.; Sherry, R.M.; Kleiner, D.; et al. Enterocolitis in patients with cancer after antibody blockade of cytotoxic T-lymphocyte-associated antigen 4. J. Clin. Oncol. 2006, 24, 2283–2289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.A.; Reed, K.; et al. Nivolumab plus ipilimumab in advanced melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef] [Green Version]
- Postow, M.A.; Chesney, J.; Pavlick, A.C.; Robert, C.; Grossmann, K.; McDermott, D.; Linette, G.P.; Meyer, N.; Giguere, J.K.; Agarwala, S.S.; et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N. Engl. J. Med. 2015, 372, 2006–2017. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, Y.; Yasuda, M.; Ocho, K.; Iwamuro, M.; Yamasaki, O.; Tanaka, T.; Otsuka, F. Severe Gastritis after Administration of Nivolumab and Ipilimumab. Case Rep. Oncol. 2018, 11, 549–556. [Google Scholar] [CrossRef]
- Johncilla, M.; Grover, S.; Zhang, X.; Jain, D.; Srivastava, A. Morphological spectrum of immune check-point inhibitor therapy-associated gastritis. Histopathology 2020, 76, 531–539. [Google Scholar] [CrossRef]
- Martins, F.; Sofiya, L.; Sykiotis, G.P.; Lamine, F.; Maillard, M.; Fraga, M.; Shabafrouz, K.; Ribi, C.; Cairoli, A.; Guex-Crosier, Y.; et al. Adverse effects of immune-checkpoint inhibitors: Epidemiology, management and surveillance. Nat. Rev. Clin. Oncol. 2019, 16, 563–580. [Google Scholar] [CrossRef] [PubMed]
- Berman, D.; Parker, S.M.; Siegel, J.; Chasalow, S.D.; Weber, J.; Galbraith, S.; Targan, S.R.; Wang, H.L. Blockade of cytotoxic T-lymphocyte antigen-4 by ipilimumab results in dysregulation of gastrointestinal immunity in patients with advanced melanoma. Cancer Immun. 2010, 10, 11. [Google Scholar] [PubMed]
- Fessas, P.; Possamai, L.A.; Clark, J.; Daniels, E.; Gudd, C.; Mullish, B.H.; Alexander, J.L.; Pinato, D.J. Immunotoxicity from checkpoint inhibitor therapy: Clinical features and underlying mechanisms. Immunology 2020, 159, 167–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saito, K.; Ozono, D.; Nagumo, H.; Yoshimura, M.; Masuzawa, Y. Temporal observation of endoscopic and histological findings of gastritis after administration of an immune checkpoint inhibitor: A case report. Clin. J. Gastroenterol. 2022, 15, 368–373. [Google Scholar] [CrossRef]
- Conn, H.O.; Blitzer, B.L. Nonassociation of adrenocorticosteroid therapy and peptic ulcer. N. Engl. J. Med. 1976, 294, 473–479. [Google Scholar] [CrossRef]
- Conn, H.O.; Poynard, T. Corticosteroids and peptic ulcer: Meta-analysis of adverse events during steroid therapy. J. Intern. Med. 1994, 236, 619–632. [Google Scholar] [CrossRef]
- Liu, D.; Ahmet, A.; Ward, L.; Krishnamoorthy, P.; Mandelcorn, E.D.; Leigh, R.; Brown, J.P.; Cohen, A.; Kim, H. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin. Immunol. 2013, 9, 30. [Google Scholar] [CrossRef] [Green Version]
- Narum, S.; Westergren, T.; Klemp, M. Corticosteroids and risk of gastrointestinal bleeding: A systematic review and meta-analysis. BMJ Open 2014, 4, e004587. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Clinical Excellence (NICE). Clinical Knowledge Summaries: Corticosteroids-Oral. 2012. Available online: http://www.cks.nhs.uk/corticosteroids_oral (accessed on 6 November 2022).
- Piper, J.M.; Ray, W.A.; Daugherty, J.R.; Griffin, M.R. Corticosteroid use and peptic ulcer disease: Role of nonsteroidal anti-inflammatory drugs. Ann. Intern. Med. 1991, 114, 735–740. [Google Scholar] [CrossRef]
- Aalykke, C.; Lauritsen, K. Epidemiology of NSAID-related gastroduodenal mucosal injury. Best Pract. Res. Clin. Gastroenterol. 2001, 15, 705–722. [Google Scholar] [CrossRef]
- Moghadam-Kia, S.; Werth, V.P. Prevention and treatment of systemic glucocorticoid side effects. Int. J. Dermatol. 2010, 49, 239–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpani de Kaski, M.; Rentsch, R.; Levi, S.; Hodgson, H.J. Corticosteroids reduce regenerative repair of epithelium in experimental gastric ulcers. Gut 1995, 37, 613–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.C.; Shin, V.Y.; Liu, E.S.; Ye, Y.N.; Wu, W.K.; So, W.H.; Chang, F.Y.; Cho, C.H. Dexamethasone delays ulcer healing by inhibition of angiogenesis in rat stomachs. Eur. J. Pharmacol. 2004, 485, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, U.; Biswas, K.; Bandyopadhyay, D.; Ganguly, C.K.; Banerjee, R.K. Dexamethasone makes the gastric mucosa susceptible to ulceration by inhibiting prostaglandin synthetase and peroxidase–two important gastroprotective enzymes. Mol. Cell. Biochem. 1999, 202, 31–36. [Google Scholar] [CrossRef]
- Tsujimoto, S.; Mokuda, S.; Matoba, K.; Yamada, A.; Jouyama, K.; Murata, Y.; Ozaki, Y.; Ito, T.; Nomura, S.; Okuda, Y. The prevalence of endoscopic gastric mucosal damage in patients with rheumatoid arthritis. PLoS ONE 2018, 13, e0200023. [Google Scholar] [CrossRef]
- Cushman, P., Jr. Glucocorticoids and the gastrointestinal tract: Current status. Gut 1970, 11, 534–539. [Google Scholar] [CrossRef] [Green Version]
- Alan, I.S.; Alan, B. Side Effects of Glucocorticoids. In Pharmacokinetics and Adverse Effects of Drugs–Mechanisms and Risks Factors; InTech: London, UK, 2018. [Google Scholar]
- Hernández-Díaz, S.; Rodríguez, L.A. Steroids and risk of upper gastrointestinal complications. Am. J. Epidemiol. 2017, 153, 1089–1093. [Google Scholar] [CrossRef] [Green Version]
- Conte, D.; Velio, P.; Brunelli, L.; Mandelli, C.; Cesana, M.; Ferrario, L.; Quatrini, M.; Bianchi, P.A. Stainable iron in gastric and duodenal mucosa of primary hemochromatosis patients and alcoholics. Am. J. Gastroenterol. 1987, 82, 237–240. [Google Scholar]
- Abraham, S.C.; Yardley, J.H.; Wu, T.T. Erosive injury to the upper gastrointestinal tract in patients receiving iron medication: An underrecognized entity. Am. J. Surg. Pathol. 1999, 23, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Kaye, P.; Abdulla, K.; Wood, J.; James, P.; Foley, S.; Ragunath, K.; Atherton, J. Iron-induced mucosal pathology of the upper gastrointestinal tract: A common finding in patients on oral iron therapy. Histopathology 2008, 53, 311–317. [Google Scholar] [CrossRef]
- Morais, R.; Ribeiro, A.; Paiva, D.; Rios, E.; Rodrigues, S.; Macedo, G. Iron pill-induced gastroduodenopathy. Porto Biomed. J. 2017, 2, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Marginean, E.C.; Bennick, M.; Cyczk, J.; Robert, M.E.; Jain, D. Gastric siderosis: Patterns and significance. Am. J. Surg. Pathol. 2006, 30, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.; Yardley, J.H. Iron medication-associated gastric mucosal injury. Arch. Pathol. Lab. Med. 2004, 128, 821–822. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Pantopoulos, K. Regulation of cellular iron metabolism. Biochem. J. 2011, 434, 365–381. [Google Scholar] [CrossRef] [Green Version]
- Angoro, B.; Motshakeri, M.; Hemmaway, C.; Svirskis, D.; Sharma, M. Non-transferrin bound iron. Clin. Chim. Acta Int. J. Clin. Chem. 2022, 531, 157–167. [Google Scholar] [CrossRef]
- Onorati, M.; Nicola, M.; Renda, A.; Lancia, M.; Di Nuovo, F. Iron Overload in Gastric Mucosa: Underdiagnosed Condition Rarely Documented in Clinical and Pathology Reports. Cureus 2020, 12, e8234. [Google Scholar] [CrossRef]
- Cimino-Mathews, A.; Broman, J.H.; Westra, W.H.; Illei, P.B. Iron pill-induced tumefactive mucosal injury of the hypopharynx. Am. J. Surg. Pathol. 2010, 34, 1720–1722. [Google Scholar] [CrossRef]
- Tran-Duy, A.; Spaetgens, B.; Hoes, A.W.; de Wit, N.J.; Stehouwer, C.D. Use of Proton Pump Inhibitors and Risks of Fundic Gland Polyps and Gastric Cancer: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 1706–1719.e5. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Peptic Ulcers (OR) | Bleeding from the Upper GI Tract (OR) | |
|---|---|---|
| NSAIDs | 1.45 | 1.76 |
| Coxibs | 1.31 | 1.62 |
| Aspirin (in small doses) | 1.50 | 1.96 |
| Antiplatelet agents (except aspirin) | 1.53 | 1.82 |
| Anticoagulants | 1.62 | 2.38 |
| Medications | Clinical Manifestations | Endoscopic Signs | Histological Features |
|---|---|---|---|
| NSAIDs/Aspirin |
|
|
|
| Anticoagulants |
|
|
|
| Glucocorticosteroids |
|
|
|
| Mycophenolate mofetil (cytostatics) |
|
|
|
| Immune checkpoint inhibitors |
|
|
|
| Iron preparations |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bordin, D.S.; Livzan, M.A.; Gaus, O.V.; Mozgovoi, S.I.; Lanas, A. Drug-Associated Gastropathy: Diagnostic Criteria. Diagnostics 2023, 13, 2220. https://doi.org/10.3390/diagnostics13132220
Bordin DS, Livzan MA, Gaus OV, Mozgovoi SI, Lanas A. Drug-Associated Gastropathy: Diagnostic Criteria. Diagnostics. 2023; 13(13):2220. https://doi.org/10.3390/diagnostics13132220
Chicago/Turabian StyleBordin, Dmitry S., Maria A. Livzan, Olga V. Gaus, Sergei I. Mozgovoi, and Angel Lanas. 2023. "Drug-Associated Gastropathy: Diagnostic Criteria" Diagnostics 13, no. 13: 2220. https://doi.org/10.3390/diagnostics13132220