
Feasibility and Performance of Free-Hand Single-Photon Computed Tomography/Ultrasonography for Preoperative Parathyroid Adenoma Localization: A Pilot Study

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
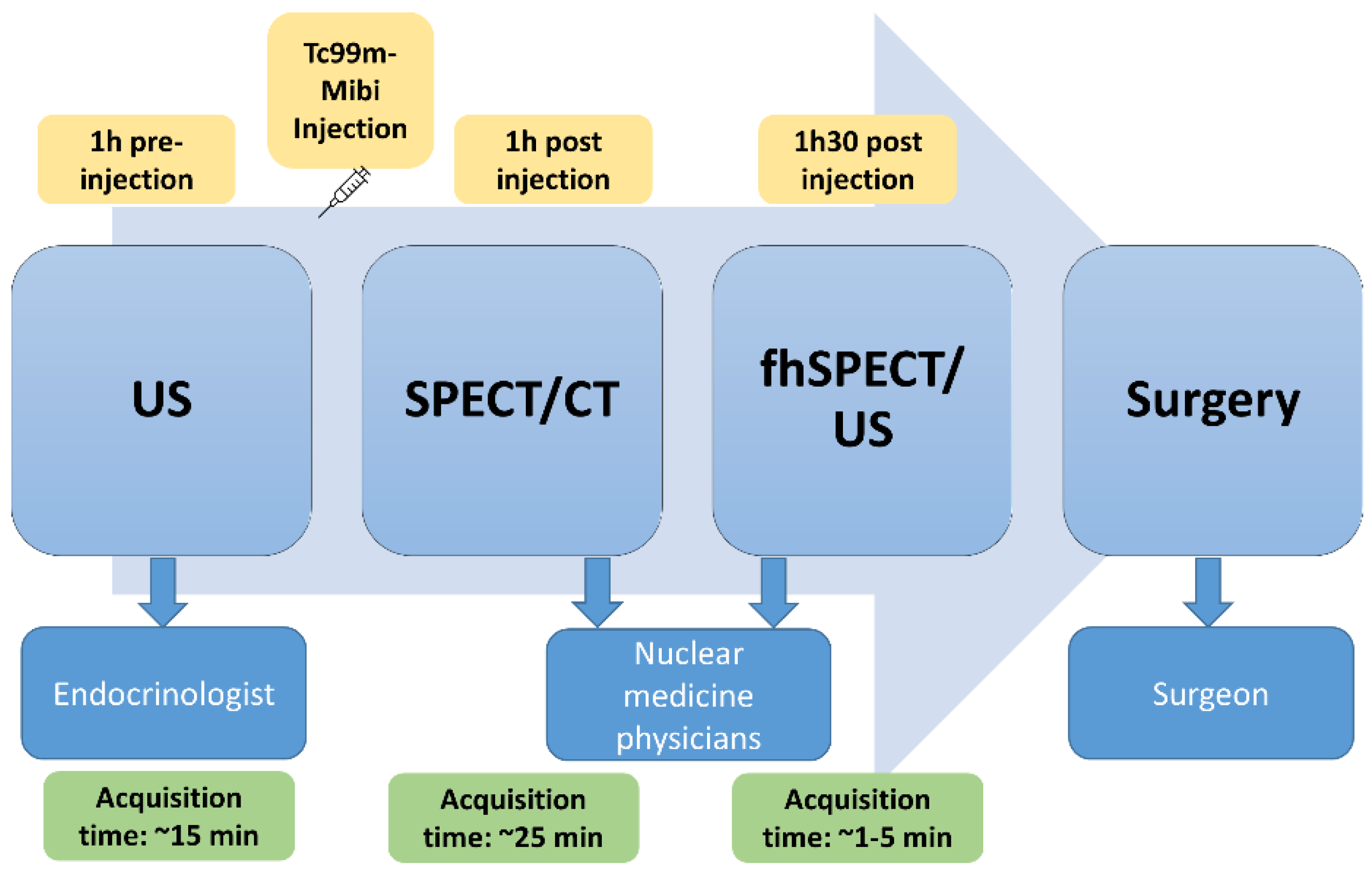
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. Detection Capacity
3.3. Feasibility
4. Discussion
4.1. Feasibility
4.2. Performance
4.3. Limitations and Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ruda, J.M.; Hollenbeak, C.S.; Stack, B.C. A systematic review of the diagnosis and treatment of primary hyperparathyroidism from 1995 to 2003. Otolaryngol. Head Neck Surg. 2005, 132, 359–372. [Google Scholar] [CrossRef] [PubMed]
- Richert, L.; Trombetti, A.; Herrmann, F.R.; Triponez, F.; Meier, C.; Robert, J.H.; Rizzoli, R. Age and gender distribution of primary hyperparathyroidism and incidence of surgical treatment in a European country with a particularly high life expectancy. Swiss Med. Wkly. 2009, 139, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Hindié, E.; Ugur, Ö.; Fuster, D.; O’Doherty, M.; Grassetto, G.; Ureña, P.; Kettle, A.; Gulec, S.A.; Pons, F.; Rubello, D. 2009 EANM parathyroid guidelines. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1201–1216. [Google Scholar] [CrossRef]
- Richard, B. Hyperparathyroïdie primaire: Échographie et scintigraphie. J. Radiol. 2009, 90, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.J. The definitive management of primary hyperparathyroidism who needs an operation? JAMA J. Am. Med. Assoc. 2017, 317, 959–968. [Google Scholar] [CrossRef]
- Treglia, G.; Sadeghi, R.; Schalin-Jäntti, C.; Caldarella, C.; Ceriani, L.; Giovanella, L.; Eisele, D.W. Detection rate of 99m Tc-MIBI single photon emission computed tomography (SPECT)/CT in preoperative planning for patients with primary hyperparathyroidism: A meta-analysis. Head Neck 2016, 38, E2159–E2172. [Google Scholar] [CrossRef]
- Moghadam, R.N.; Amlelshahbaz, A.P.; Namiranian, N.; Sobhan-Ardekani, M.; Emami-Meybodi, M.; Dehghan, A.; Rahmanian, M.; Razavi-Ratki, S.K. Comparative diagnostic performance of ultrasonography and 99mTc-Sestamibi scintigraphy for parathyroid adenoma in primary hyperparathyroidism; Systematic review and meta-analysis. Asian Pacific J. Cancer Prev. 2017, 18, 3195–3200. [Google Scholar] [CrossRef]
- Kim, Y., II; Jung, Y.H.; Hwang, K.T.; Lee, H.Y. Efficacy of 99mTc-sestamibi SPECT/CT for minimally invasive parathyroidectomy: Comparative study with 99mTc-sestamibi scintigraphy, SPECT, US and CT. Ann. Nucl. Med. 2012, 26, 804–810. [Google Scholar] [CrossRef]
- Wong, K.K.; Fig, L.M.; Gross, M.D.; Dwamena, B.A. Parathyroid adenoma localization with 99mTc-sestamibi SPECT/CT: A meta-analysis. Nucl. Med. Commun. 2015, 36, 363–375. [Google Scholar] [CrossRef]
- Freesmeyer, M.; Opfermann, T.; Winkens, T. Hybrid Integration of Real-time US and Freehand SPECT: Proof of Concept in Patients with Thyroid Diseases. Radiology 2014, 271, 856–861. [Google Scholar] [CrossRef] [Green Version]
- Freesmeyer, M.; Winkens, T.; Kühnel, C.; Opfermann, T.; Seifert, P. Technetium-99m SPECT/US Hybrid Imaging Compared with Conventional Diagnostic Thyroid Imaging with Scintigraphy and Ultrasound. Ultrasound Med. Biol. 2019, 45, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Gühne, F.; Mothes, H.; Freesmeyer, M. Allocation of parathyroid adenoma and suspicious thyroid nodule by real-time 99mTc-MIBI SPECT/US fusion imaging. Endocrine 2016, 54, 560–561. [Google Scholar] [CrossRef] [PubMed]
- Bluemel, C.; Schnelzer, A.; Okur, A.; Ehlerding, A.; Paepke, S.; Scheidhauer, K.; Kiechle, M. Freehand SPECT for image-guided sentinel lymph node biopsy in breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1656–1661. [Google Scholar] [CrossRef]
- Bluemel, C.; Herrmann, K.; Kübler, A.; Buck, A.K.; Geissinger, E.; Wild, V.; Hartmann, S.; Lapa, C.; Linz, C.; Müller-Richter, U. Intraoperative 3-D imaging improves sentinel lymph node biopsy in oral cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 2257–2264. [Google Scholar] [CrossRef]
- Bluemel, C.; Safak, G.; Cramer, A.; Wöckel, A.; Gesierich, A.; Hartmann, E.; Schmid, J.S.; Kaiser, F.; Buck, A.K.; Herrmann, K. Fusion of freehand SPECT and ultrasound: First experience in preoperative localization of sentinel lymph nodes. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 2304–2312. [Google Scholar] [CrossRef]
- De Bree, R.; Pouw, B.; Heuveling, D.A.; Castelijns, J.A. Fusion of freehand SPECT and ultrasound to perform ultrasound-guided fine-needle aspiration cytology of sentinel nodes in head and neck cancer. Am. J. Neuroradiol. 2015, 36, 2153–2158. [Google Scholar] [CrossRef] [Green Version]
- Engelen, T.; Winkel, B.M.; Rietbergen, D.D.; Kleinjan, G.H.; Vidal-Sicart, S.; Olmos, R.A.V.; Van Den Berg, N.S.; Van Leeuwen, F.W.B. The next evolution in radioguided surgery: Breast cancer related sentinel node localization using a freehandSPECT-mobile gamma camera combination. Am. J. Nucl. Med. Mol. Imaging 2015, 5, 233–245. [Google Scholar]
- Mihaljevic, A.L.; Rieger, A.; Belloni, B.; Hein, R.; Okur, A.; Scheidhauer, K.; Schuster, T.; Friess, H.; Martignoni, M.E. Transferring innovative freehand SPECT to the operating room: First experiences with sentinel lymph node biopsy in malignant melanoma. Eur. J. Surg. Oncol. 2014, 40, 42–48. [Google Scholar] [CrossRef]
- Okur, A.; Hennersperger, C.; Runyan, B.; Gardiazaball, J.; Keicher, M.; Paepke, S.; Wendler, T.; Navab, N. FhSPECT-US guided needle biopsy of sentinel lymph nodes in the axilla: Is it feasible? Med. Image Comput. Comput. Assist. Interv. 2014, 17, 577–584. [Google Scholar] [PubMed]
- Wendler, T.; Herrmann, K.; Schnelzer, A.; Lasser, T.; Traub, J.; Kutter, O.; Ehlerding, A.; Scheidhauer, K.; Schuster, T.; Kiechle, M.; et al. First demonstration of 3-D lymphatic mapping in breast cancer using freehand SPECT. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1452–1461. [Google Scholar] [CrossRef] [PubMed]
- Bluemel, C.; Kirchner, P.; Kajdi, G.W.; Werner, R.A.; Herrmann, K. Localization of parathyroid adenoma with real-time ultrasound freehand SPECT fusion. Clin. Nucl. Med. 2016, 41, e141–e142. [Google Scholar] [CrossRef] [PubMed]
- Freesmeyer, M.; Winkens, T.; Opfermann, T.; Elsner, P.; Runnebaum, I.; Darr, A. Real-time ultrasound and freehand-SPECT. Nuklearmedizin 2014, 53, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Groch, M.W.; Erwin, W.D. SPECT in the year 2000: Basic principles. J. Nucl. Med. Technol. 2000, 28, 233–244. [Google Scholar] [PubMed]
- Mertelmeier, T.; Ludwig, J.; Zhao, B.; Zhao, W. Optimization of tomosynthesis acquisition parameters: Angular range and number of projections. In Lecture Notes in Computer Science, Digital Mammography, Proceedings of the 9th International Workshop, IWDM 2008, Tucson, AZ, USA, 20–23 July 2008; Springer: Berlin/Heidelberg, Germany, 2008; Volume 5116, pp. 220–227. [Google Scholar] [CrossRef]
- Revel, M.-P. Physique des Ultrasons; Elsevier: Paris, France, 1999. [Google Scholar]
- Esposito, M.; Busam, B.; Hennersperger, C.; Rackerseder, J.; Navab, N.; Frisch, B. Multimodal US–gamma imaging using collaborative robotics for cancer staging biopsies. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 1561–1571. [Google Scholar] [CrossRef]
- Matthies, P.; Gardiazabal, J.; Okur, A.; Vogel, J.; Lasser, T.; Navab, N. Mini gamma cameras for intra-operative nuclear tomographic reconstruction. Med. Image Anal. 2014, 18, 1329–1336. [Google Scholar] [CrossRef]
- Vogel, J.; Lasser, T.; Gardiazabal, J.; Navab, N. Trajectory optimization for intra-operative nuclear tomographic imaging. Med. Image Anal. 2013, 17, 723–731. [Google Scholar] [CrossRef]
- Bruyant, P.P. Analytic and iterative reconstruction algorithms in SPECT. J. Nucl. Med. 2002, 43, 1343–1358. [Google Scholar]
- Chandramohan, A.; Sathyakumar, K.; Irodi, A.; Abraham, D.; Paul, M.J. Causes of discordant or negative ultrasound of parathyroid glands in treatment naïve patients with primary hyperparathyroidism. Eur. J. Radiol. 2012, 81, 3956–3964. [Google Scholar] [CrossRef]
- Li, P.; Liu, Q.; Tang, D.; Zhu, Y.; Xu, L.; Sun, X.; Song, S. Lesion based diagnostic performance of dual phase 99mTc-MIBI SPECT/CT imaging and ultrasonography in patients with secondary hyperparathyroidism. BMC Med. Imaging 2017, 17, 60. [Google Scholar] [CrossRef] [Green Version]
- Freesmeyer, M.; Winkens, T.; Opfermann, T.; Kühnel, C. Radiation exposure of the investigator’s hand during fusion imaging of the thyroid with 99m TcO4-free-hand SPECT and ultrasound. Radiat. Prot. Dosim. 2016, 168, 531–536. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex (%) | Age (years) Mean ± SD | BMI (Kg/m2) Mean ± SD | PTH Level * Pre-Surgery (ng/L) Mean ± SD [12] | PTH Level * Post-Surgery (ng/L) Mean ± SD [9] | Ca Level ** Pre-Surgery (mmol/L) Mean ± SD [12] | Ca Level ** Post-Surgery (mmol/L) Mean ± SD [10] | Number of Lesions Detected on Imaging | Size of Lesions Measured on SPECT/CT (mm) Mean ± SD | Depth of Lesions Measured on SPECT/CT (mm) Mean ± SD |
|---|---|---|---|---|---|---|---|---|---|
| Female 4 (33%) Male 8 (67%) | 60 ± 16 | 25.5 ± 5.2 | 107.5 ± 50.9 | 49.1 ± 29.9 | 2.7 ± 0.1 | 2.3 ± 0.9 | 16 | 11.4 ± 4.2 | 33.1 ± 8.9 |
| Detected (12 Patients) | Undetected According to SPECT/CT (12 Patients) | Undetected According to Surgery (9 Patients) | Undetected According to Gold STD (12 Patients) | |
|---|---|---|---|---|
| Per patient (n = 12) | ||||
| US | 10 | 2 | 1 | 2 |
| SPECT/CT | 12 | – | 0 | 0 |
| fhSPECT/US | 7 | 5 | 3 | 5 |
| Per lesion (n = 17) | ||||
| US | 10 | 6 | 4 | 7 |
| SPECT/CT | 16 | – | 1 | 1 |
| fhSPECT/US | 7 | 9 | 7 | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Champendal, M.; Jreige, M.; Nicod Lalonde, M.; Pires Jorge, J.A.; Matter, M.; Sykiotis, G.P.; Prior, J.O. Feasibility and Performance of Free-Hand Single-Photon Computed Tomography/Ultrasonography for Preoperative Parathyroid Adenoma Localization: A Pilot Study. Diagnostics 2023, 13, 2200. https://doi.org/10.3390/diagnostics13132200
Champendal M, Jreige M, Nicod Lalonde M, Pires Jorge JA, Matter M, Sykiotis GP, Prior JO. Feasibility and Performance of Free-Hand Single-Photon Computed Tomography/Ultrasonography for Preoperative Parathyroid Adenoma Localization: A Pilot Study. Diagnostics. 2023; 13(13):2200. https://doi.org/10.3390/diagnostics13132200
Chicago/Turabian StyleChampendal, Mélanie, Mario Jreige, Marie Nicod Lalonde, José A. Pires Jorge, Maurice Matter, Gerasimos P. Sykiotis, and John O. Prior. 2023. "Feasibility and Performance of Free-Hand Single-Photon Computed Tomography/Ultrasonography for Preoperative Parathyroid Adenoma Localization: A Pilot Study" Diagnostics 13, no. 13: 2200. https://doi.org/10.3390/diagnostics13132200