

The Association of Coronary Fat Attenuation Index Quantified by Automated Software on Coronary Computed Tomography Angiography with Adverse Events in Patients with Less than Moderate Coronary Artery Stenosis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Subjects
2.2. Basic Clinical Information of Patients
2.3. Coronary Artery CTA Scanning Protocol
2.4. CCTA Image Analysis
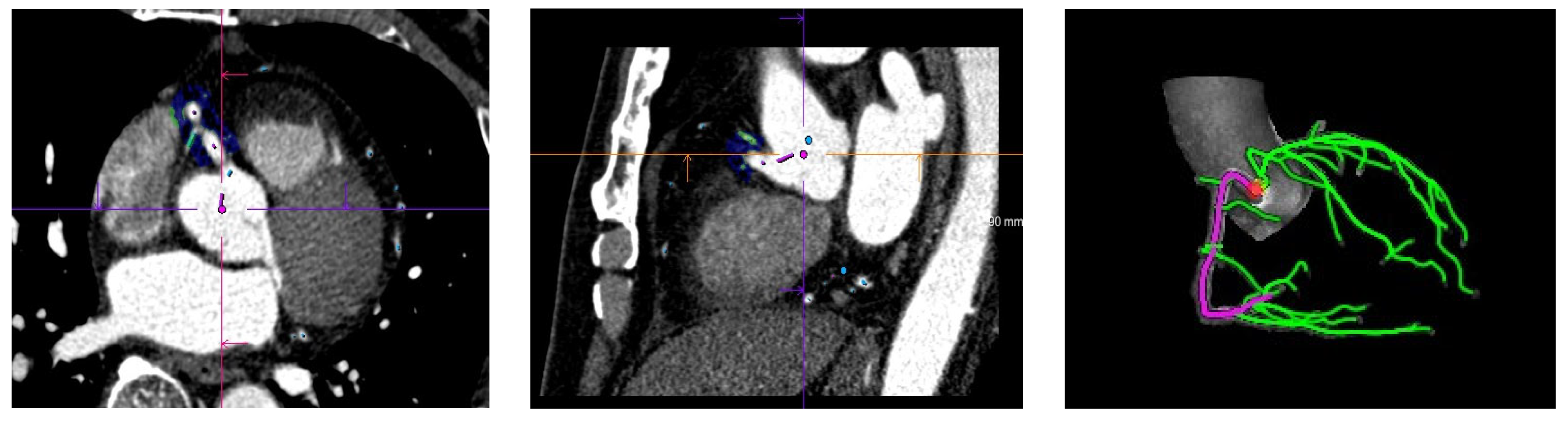
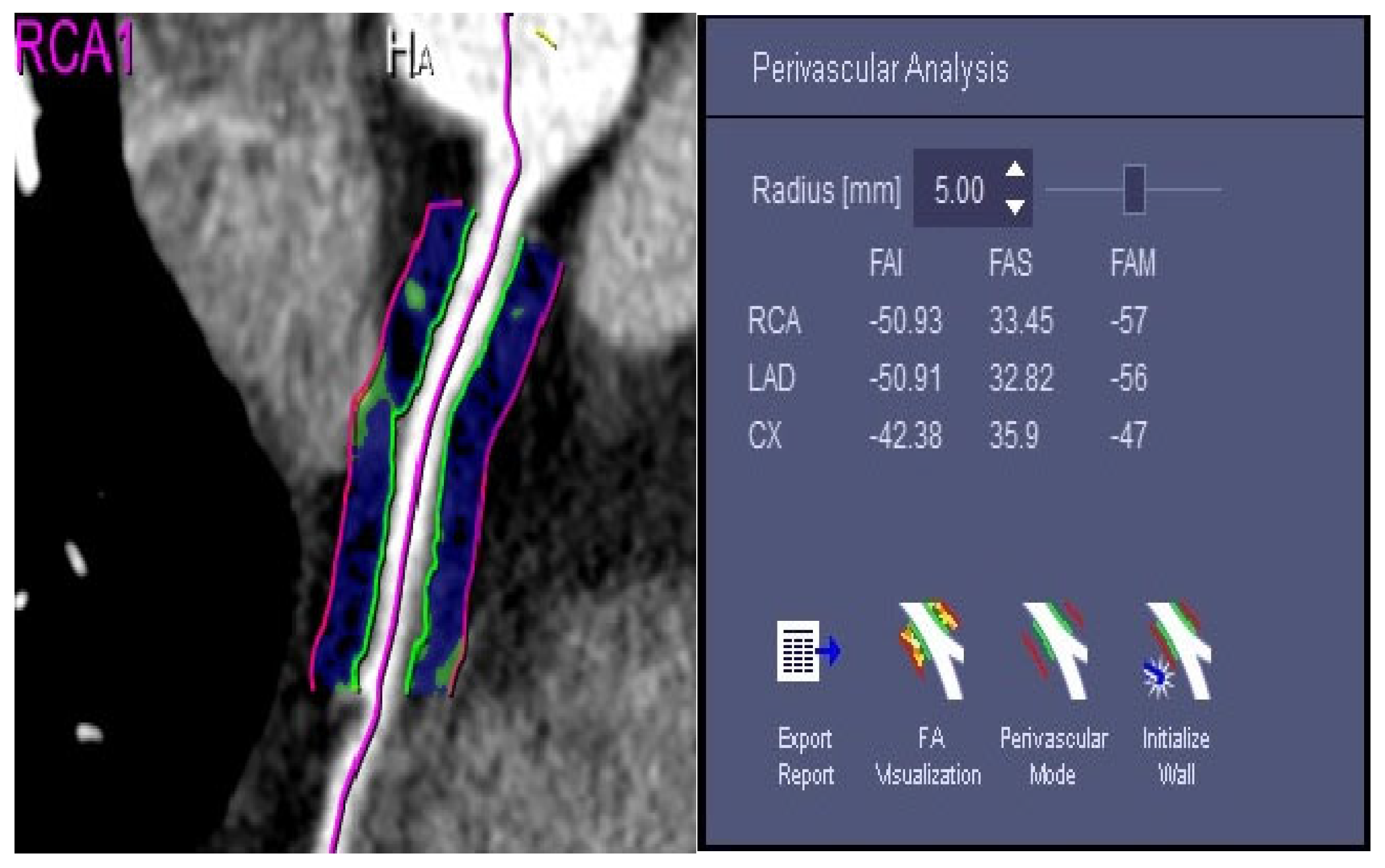
2.5. Measurement of the FAI Value of Fat around the Coronary Artery
2.6. Statistical Analysis
3. Results
3.1. Basic Clinical Information of Patients
3.2. FAIs of Three Coronary Arteries and Adverse Events of Coronary Arteries
4. Discussion
4.1. Pericardium Fat and Coronary Artery Surrounding Fat
4.2. Quantification of Coronary Periarterial Fat and Its Clinical Significance
4.3. The Novelty and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Center for Cardiovascular Diseases. Annual Report on Cardiovascular Health and Diseases in China (2021); China Science Publishing & Media Ltd.: Beijing, China, 2022. [Google Scholar]
- Villines, T.C.; Al’Aref, S.J.; Andreini, D.; Chen, M.Y.; Choi, A.D.; De Cecco, C.N.; Dey, D.; Earls, J.P.; Ferencik, M.; Gransar, H.; et al. The Journal of Cardiovascular Computed Tomography: 2020 Year in review. J. Cardiovasc. Comput. Tomogr. 2021, 15, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Mark, D.B.; Federspiel, J.J.; Cowper, P.A.; Anstrom, K.J.; Hoffmann, U.; Patel, M.R.; Davidson-Ray, L.; Daniels, M.R.; Cooper, L.S.; Knight, J.D.; et al. Economic outcomes of Anatomical versus Functional Testing for Coronary Artery Disease. Ann. Intern. Med. 2016, 165, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Scot-Heart, T. CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): An open-label, parallel-group, multicenter trial. Lancet 2015, 385, 2383–2391. [Google Scholar]
- Park, S.J.; Kang, S.J.; Ahn, J.M.; Shim, E.B.; Kim, Y.T.; Yun, S.C.; Song, H.; Lee, J.Y.; Kim, W.J.; Park, D.W.; et al. Visual-Functional Mismatch Between Coronary Angiography and Fractional Flow Reserve. JCIN 2012, 5, 1029–1036. [Google Scholar]
- Monti, C.B.; Codari, M.; De Cecco, C.N.; Secchi, F.; Sardanelli, F.; Stillman, A.E. Novel imaging biomarkers: Epicardial adipose tissue evaluation. Br. Radiol. 2020, 93, 20190770. [Google Scholar] [CrossRef] [PubMed]
- Madonna, R.; Massaro, M.; Scoditti, E.; Pescetelli, I.; De Caterina, R. The epicardial adipose tissue and the coronary arteries: Dangerous liaisons. Cardiovasc. Res. 2019, 115, 1013–10255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oikonomou, E.K.; Marwan, M.; Desai, M.Y.; Mancio, J.; Alashi, A.; Centeno, E.H.; Thomas, S.; Herdman, L.; Kotanidis, C.P.; Thomas, K.E.; et al. Noninvasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): A post hoc analysis of prospective outcome data. Lancet 2018, 392, 929–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oikonomou, E.K.; West, H.W.; Antoniades, C. Cardiac Computed Tomography: Assessment of Coronary Inflammation and Other Plaque Features. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 2207–2219. [Google Scholar] [CrossRef]
- Bhuiyan, G.R.; Roy, G.C.; Siddique, M.A.; Rahman, M.; Ahmed, K.; Nahar, F. Relationship between echocardiographic epicardial adipose tissue (EAT) thickness and angiographically detected coronary artery disease. Prev. Cardiol. 2017, 26, 498–504. [Google Scholar]
- Commandeur, F.; Goeller, M.; Betancur, J.; Cadet, S.; Doris, M.; Chen, X.; Berman, D.S.; Slomka, P.J.; Tamarappoo, B.K.; Dey, D. Deep learning for quantification of epicardial and thoracic adipose tissue from noncontrast CT. IEEE Trans. Med. Imaging 2018, 37, 1835–1846. [Google Scholar] [CrossRef]
- Denzinger, F.; Wels, M.; Hopfgartner, C.; Lu, J.; Schöbinger, M.; Maier, A.; Sühling, M. Coronary Plaque Analysis for CT Angiography Clinical Research. In Bildverarbeitung für die Medizin 2021. Informatik Aktuell; Palm, C., Deserno, T.M., Handels, H., Maier, A., Maier-Hein, K., Tolxdorff, T., Eds.; Springer: Vieweg, IL, USA; Wiesbaden, Germany, 2021. [Google Scholar] [CrossRef]
- Cury, R.C.; Leipsic, J.; Abbara, S.; Achenbach, S.; Berman, D.; Bittencourt, M.; Budoff, M.; Chinnaiyan, K.; Choi, A.D.; Ghoshhajra, B.; et al. CAD-RADS™ 2.0–2022 Coronary Artery Disease-Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Cardiology (ACC), the American College of Radiology (ACR), and the North America Society of Cardiovascular Imaging (NASCI). Cardiovasc. Comput. Tomogr. 2022, 16, 536–557. [Google Scholar]
- Moser, P.T.; Schernthaner, R.; Loewe, C.; Strassl, A.; Denzinger, F.; Faby, S.; Wels, M.; Nizhnikava, V.; Uyanik-Uenal, K.; Zuckermann, A.; et al. Evaluation of perivascular fat attenuation with coronary CT angiography in cardiac transplantation patients: An imaging biomarker candidate for prediction of cardiac mortality and retransplantation. Eur. Radiol. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Elnabawi, Y.A.; Oikonomou, E.K.; Dey, A.K.; Mancio, J.; Rodante, J.A.; Aksentijevich, M.; Choi, H.; Keel, A.; Erb-Alvarez, J.; Teague, H.L.; et al. Association of biologic therapy withcoronary inflammation in patients with psoriasis as assessed by perivascular fat attenuation index. JAMA Cardiol. 2019, 4, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Antonopoulos, A.S.; Sanna, F.; Sabharwal, N.; Thomas, S.; Oikonomou, E.K.; Herdman, L.; Margaritis, M.; Shirodaria, C.; Kampoli, A.M.; Akoumianakis, I.; et al. Detecting human coronary inflammation by imaging perivascular fat. Sci. Transl. Med. 2017, 9, eaal2658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dweck, M.R.; Puntmann, V.O.; Vesey, A.T.; Fayad, Z.A.; Nagel, E. MR Imaging of coronary arteries and plaques. JACC Cardiovasc. Imaging 2016, 9, 306–316. [Google Scholar] [CrossRef]
- Ueda, Y.; Shiga, Y.; Idemoto, Y.; Tashiro, K.; Motozato, K.; Koyoshi, R.; Kuwano, T.; Fujimi, K.; Ogawa, M.; Saku, K.; et al. Association between the presence or severity of coronary artery disease and pericardial fat, paracardial fat, epicardial fat, visceral fat, and subcutaneous fat as assessed by multidetector row computed tomography. Int. Heart J. 2018, 59, 695–704. [Google Scholar] [CrossRef] [Green Version]
- Raț, N.; Opincariu, D.; Márton, E.; Zavate, R.; Pintican, M.; Benedek, T. The Effect of Periplaque Fat on Coronary Plaque Vulnerability in Patients with Stable Coronary Artery Disease—A 128-multislice CT-based Study. Interdiscip. Med. 2018, 3, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Li, Y.; Li, Y.; Ren, X.; Zhang, X.; Hu, D.; Gao, Y.; Xing, Y.; Shang, H. Oxidative Stress-Mediated Atherosclerosis: Mechanisms and Therapies. Front. Physiol. 2017, 8, 60. [Google Scholar] [CrossRef] [Green Version]
- Budoff, M.J.; Dowe, D.; Jollis, J.G.; Gitter, M.; Sutherland, J.; Halamert, E.; Scherer, M.; Bellinger, R.; Martin, A.; Benton, R.; et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: Results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. Am. Coll. Cardiol. 2008, 52, 1724–1732. [Google Scholar]
- Min, J.K.; Dunning, A.; Lin, F.Y.; Achenbach, S.; Al-Mallah, M.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; Chang, H.J.; Cheng, V.; et al. Age- and sex-related differences in all-cause mortality risk based on coronary computed tomography angiography findings results from the International Multicenter CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter Registry) of 23,854 patients without known coronary artery disease. Am. Coll. Cardiol. 2011, 58, 849–860. [Google Scholar]
- Matyas, B.; Polexa, S.; Benedek, I.; Buicu, A.; Benedek, T. Biomarkers of Systemic Versus Local Inflammation During the Acute Phase of Myocardial Infarction, as Predictors of Postinfarction Heart Failure. Cardiovasc. Emerg. 2021, 7, 70–76. [Google Scholar]
- Lin, A.; Kolossváry, M.; Motwani, M.; Išgum, I.; Maurovich-Horvat, P.; Slomka, P.J.; Dey, D. Artificial Intelligence in Cardiovascular Imaging for Risk Stratification in Coronary Artery Disease. Radiol. Cardiothorac. Imaging 2021, 3, e2005. [Google Scholar] [CrossRef]
- Oikonomou, E.K.; Antonopoulos, A.S.; Schottlander, D.; Marwan, M.; Mathers, C.; Tomlins, P. Standardized measurement of coronary inflammation using cardiovascular computed tomography: Integration in clinical care as a prognostic medical device. Cardiovasc. Res. 2021, 117, 2677–2690. [Google Scholar] [CrossRef]
- Kohchi, K.; Takebayashi, S.; Hiroki, T.; Nobuyoshi, M. Significance of adventitial inflammation of the coronary artery in patients with unstable angina: Results at autopsy. Circulation 1985, 71, 709–716. [Google Scholar] [CrossRef] [Green Version]
- Thornton, E.; Mendiratta-Lala, M.; Siewert, B.; Eisenberg, R.L. Patterns of fat stranding. Am. J. Roentgenol. 2011, 197, W1–W14. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Barbu, A.; Georgescu, B.; Scheuering, M.; Comaniciu, D. Four-chamber heart modeling and automatic segmentation for 3-D cardiac CT volumes using marginal space learning and steerable features. IEEE Trans. Med. Imaging 2008, 27, 1668–1681. [Google Scholar] [CrossRef]
- Zheng, Y.; Tek, H.; Funka-Lea, G. Robust and accurate coronary artery centerline extraction in CTA by combining model-driven and data-driven approaches. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2013: 16th International Conference, Nagoya, Japan, 22–26 September 2013; Springer: Berlin/Heidelberg, Germany, 2013; pp. 74–81. [Google Scholar]
- Schaap, M.; Metz, C.T.; van Walsum, T.; van der Giessen, A.G.; Weustink, A.C.; Mollet, N.R.; Bauer, C.; Bogunović, H.; Castro, C.; Deng, X.; et al. Standardized evaluation methodol- ogy and reference database for evaluating coronary artery centerline extraction algorithms. Med. Image Anal. 2009, 13, 701–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wels, M.; Lades, F.; Hopfgartner, C.; Schwemmer, C.; Sühling, M. Intuitive and Accurate Patient-Specific Coronary Tree Modeling from Cardiac Computed-Tomography Angiography. In Proceedings of the 3rd Interactive MIC Workshop, Athens, Greece, 17 October 2016; pp. 86–93. [Google Scholar]
- Mazurek, T.; Kochman, J.; Kobylecka, M.; Wilimski, R.; Filipiak, K.J.; Królicki, L.; Opolski, G. Inflammatory activity of pericoronary adipose tissue may affect plaque composition in patients with acute coronary syndrome without persistent ST-segment elevation: Preliminary results. Kardiol. Pol. 2014, 72, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, T.; Kobylecka, M.; Zielenkiewicz, M.; Kurek, A.; Kochman, J.; Filipiak, K.J.; Mazurek, K.; Huczek, Z.; Królicki, L.; Opolski, G. PET/CT evaluation of 18F-FDG uptake in pericoronary adipose tissue in patients with stable coronary artery disease: Independent predictor of atherosclerotic lesions’ formation? J. Nucl. Cardiol. 2017, 24, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Hirata, Y.; Tabata, M.; Kurobe, H.; Motoki, T.; Akaike, M.; Nishio, C.; Higashida, M.; Mikasa, H.; Nakaya, Y.; Takanashi, S.; et al. Coronary atherosclerosis is associated with macrophage polarization in epicardial adipose tissue. J. Am. Coll. Cardiol. 2011, 58, 248–255. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Without Adverse (n = 87) | With Adverse (n = 85) |
|---|---|---|
| Basic clinical data | ||
| Age (years) | 61.26 ± 9.41 | 65.01 ± 12.43 |
| Sex (male:female) | 47:40 | 47:38 |
| Smoking history (Yes:No) | 31:56 | 31:54 |
| Biochemical indicators | ||
| Fasting blood glucose (mmol/L) | 5.80 ± 1.74 | 5.66 ± 1.41 |
| Total cholesterol (mmol/L) | 4.63 ± 1.07 | 4.13 ± 1.05 |
| Low-density cholesterol (mmol/L) | 2.63 ± 0.83 | 2.42 ± 0.87 |
| High-density cholesterol (mmol/L) | 1.41 ± 0.45 | 1.33 ± 0.39 |
| Triglycerides (mmol/L) | 1.76 ± 1.66 | 1.39 ± 0.88 |
| Without Adverse | With Adverse | t | p | |||||
|---|---|---|---|---|---|---|---|---|
| n | S | n | S | |||||
| LAD | 87 | −44.95 | 4.10 | 85 | −39.36 | 5.89 | −7.212 | <0.001 |
| LCX | 86 | −36.52 | 4.11 | 84 | −33.72 | 5.32 | −3.844 | <0.001 |
| RCA | 86 | −44.71 | 6.61 | 84 | −41.70 | 7.59 | −2.752 | 0.022 |
| Without Adverse | With Adverse | F | p | |||||
|---|---|---|---|---|---|---|---|---|
| n | S | n | S | |||||
| LAD | 88 | −44.99 | 4.18 | 85 | −39.38 | 5.93 | 52.19 | <0.001 |
| LCX | 88 | −36.44 | 4.12 | 84 | −33.76 | 5.42 | 14.90 | <0.001 |
| RCA | 87 | −44.70 | 6.63 | 84 | −41.91 | 7.50 | 7.60 | <0.001 |
| Zhang et al. | Hirata et al. [34] | |
|---|---|---|
| Study measurements | Coronary artery FAI | EAT was taken from the anterior wall of the left ventricle |
| Study method | Machine learning | Surgical intervention |
| Traumatic examination methods | No | Yes |
| Ease of operation | Easy | Difficult |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, W.; Li, P.; Chen, X.; He, L.; Zhang, Q.; Yu, J. The Association of Coronary Fat Attenuation Index Quantified by Automated Software on Coronary Computed Tomography Angiography with Adverse Events in Patients with Less than Moderate Coronary Artery Stenosis. Diagnostics 2023, 13, 2136. https://doi.org/10.3390/diagnostics13132136
Zhang W, Li P, Chen X, He L, Zhang Q, Yu J. The Association of Coronary Fat Attenuation Index Quantified by Automated Software on Coronary Computed Tomography Angiography with Adverse Events in Patients with Less than Moderate Coronary Artery Stenosis. Diagnostics. 2023; 13(13):2136. https://doi.org/10.3390/diagnostics13132136
Chicago/Turabian StyleZhang, Wenzhao, Peiling Li, Xinyue Chen, Liyi He, Qiang Zhang, and Jianqun Yu. 2023. "The Association of Coronary Fat Attenuation Index Quantified by Automated Software on Coronary Computed Tomography Angiography with Adverse Events in Patients with Less than Moderate Coronary Artery Stenosis" Diagnostics 13, no. 13: 2136. https://doi.org/10.3390/diagnostics13132136