
Low Prevalence of HSV-1 and Helicobacter pylori in HNSCC and Chronic Tonsillitis Patients Compared to Healthy Individuals
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Methods
2.2.1. DNA Preparation
2.2.2. Detection of HSV-1/2 and H. pylori
2.2.3. Statistical Analysis
3. Results
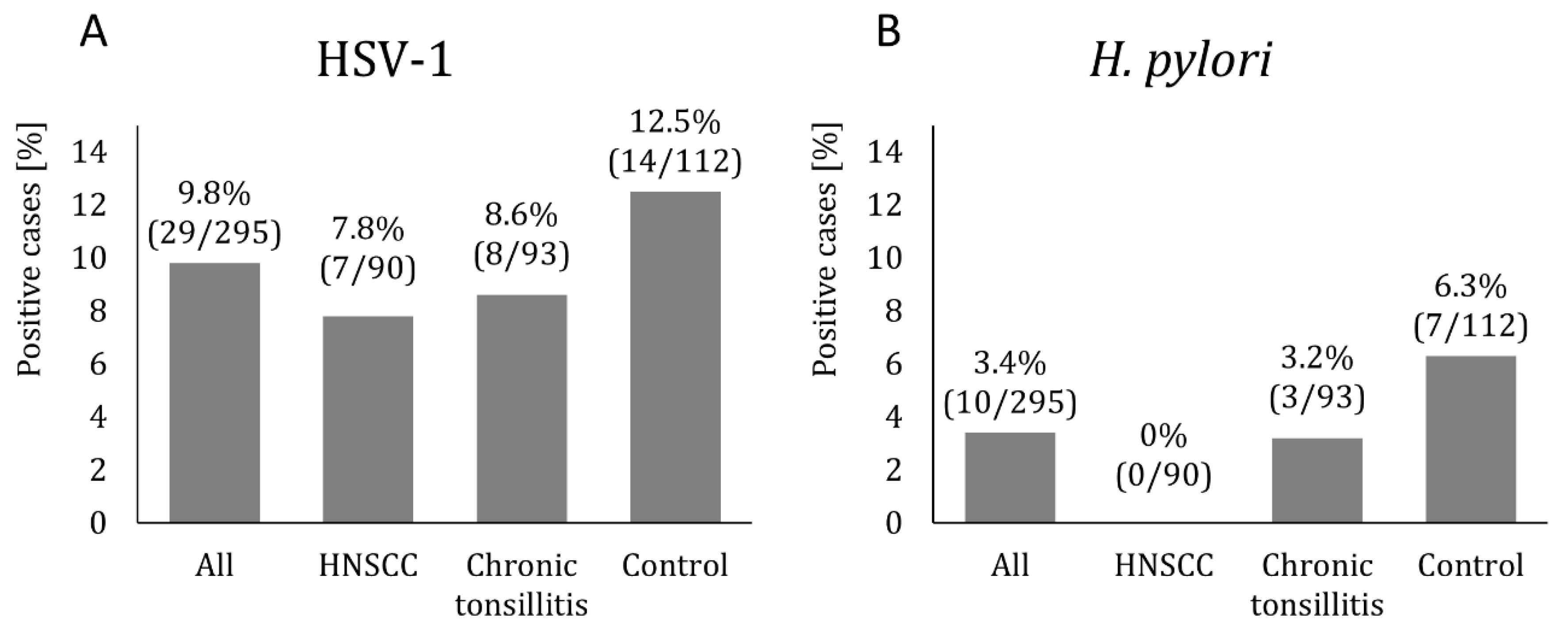
The Prevalence of HSV-1/2 and H. pylori in All Study Groups
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ansari, S.; Yamaoka, Y. Helicobacter pylori Virulence Factors Exploiting Gastric Colonization and its Pathogenicity. Toxins 2019, 11, 677. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Zhu, M.; He, Y.; Wang, T.; Tian, D.; Shu, J. The impacts of probiotics in eradication therapy of Helicobacter pylori. Arch. Microbiol. 2022, 204, 692. [Google Scholar] [CrossRef] [PubMed]
- Khoder, G.; Muhammad, J.S.; Mahmoud, I.; Soliman, S.S.M.; Burucoa, C. Prevalence of Helicobacter pylori and Its Associated Factors among Healthy Asymptomatic Residents in the United Arab Emirates. Pathogens 2019, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Venneman, K.; Huybrechts, I.; Gunter, M.J.; Vandendaele, L.; Herrero, R.; Van Herck, K. The epidemiology of Helicobacter pylori infection in Europe and the impact of lifestyle on its natural evolution toward stomach cancer after infection: A systematic review. Helicobacter 2018, 23, e12483. [Google Scholar] [CrossRef]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef]
- Łaszewicz, W.; Iwanczak, F.; Iwanczak, B. Seroprevalence of Helicobacter pylori infection in Polish children and adults depending on socioeconomic status and living conditions. Adv. Med. Sci. 2014, 59, 147–150. [Google Scholar] [CrossRef]
- Repici, A.; Pellicano, R.; Astegiano, M.; Saracco, G.; De Angelis, C.; Debernardi, W.; Berrutti, M.; Rizzetto, M. La diagnosi “invasiva” dell’infezione da Helicobacter pylori nella pratica clinica del 2006 [Invasive diagnosis of Helicobacter pylori infection in the 2006 clinical practice]. Minerva Med. 2006, 97, 25–29. [Google Scholar]
- Rimbara, E.; Sasatsu, M.; Graham, D.Y. PCR detection of Helicobacter pylori in clinical samples. Methods Mol. Biol. 2013, 943, 279–287. [Google Scholar]
- Jain, M. Assesment of Correlation of Herpes Simplex Virus-1 with Oral Cancer and Precancer-A Comparative Study. J. Clin. Diagn. Res. 2016, 10, ZC14–ZC17. [Google Scholar] [CrossRef]
- Packard, J.E.; Dembowski, J.A. HSV-1 DNA Replication—Coordinated Regulation by Viral and Cellular Factors. Viruses 2021, 13, 2015. [Google Scholar] [CrossRef]
- Starr, J.R.; Daling, J.R.; Fitzgibbons, E.D.; Madeleine, M.M.; Ashley, R.; Galloway, D.A.; Schwartz, S.M. Serologic evidence of herpes simplex virus 1 infection and oropharyngeal cancer risk. Cancer Res. 2001, 61, 8459–8464. [Google Scholar] [PubMed]
- Looker, K.J.; Magaret, A.S.; May, M.T.; Turner, K.M.; Vickerman, P.; Gottlieb, S.L.; Newman, L.M. Global and Regional Estimates of Prevalent and Incident Herpes Simplex Virus Type 1 Infections in 2012. PLoS ONE 2015, 10, e0140765. [Google Scholar] [CrossRef] [PubMed]
- Arshad, Z.; Alturkistani, A.; Brindley, D.; Lam, C.; Foley, K.; Meinert, E. Tools for the Diagnosis of Herpes Simplex Virus 1/2: Systematic Review of Studies Published Between 2012 and 2018. JMIR Public Health Surveill. 2019, 5, e14216. [Google Scholar] [CrossRef]
- Ramchandani, M.; Kong, M.; Tronstein, E.; Selke, S.; Mikhaylova, A.; Magaret, A.; Huang, M.L.; Johnston, C.; Corey, L.; Wald, A. Herpes Simplex Virus Type 1 Shedding in Tears and Nasal and Oral Mucosa of Healthy Adults. Sex. Transm. Dis. 2016, 43, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Prim. 2020, 6, 92. [Google Scholar] [CrossRef]
- Dayama, A.; Srivastava, V.; Shukla, M.; Singh, R.; Pandey, M. Helicobacter pylori and oral cancer: Possible association in a preliminary case control study. Asian Pac. J. Cancer Prev. 2011, 12, 1333–1336. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Jalouli, J.; Ibrahim, S.O.; Mehrotra, R.; Jalouli, M.M.; Sapkota, D.; Larsson, P.A.; Hirsch, J.M. Prevalence of viral (HPV, EBV, HSV) infections in oral submucous fibrosis and oral cancer from India. Acta Oto-Laryngol. 2010, 130, 1306–1311. [Google Scholar] [CrossRef]
- Kuo, Y.C.; Yu, L.Y.; Wang, H.Y.; Chen, M.J.; Wu, M.S.; Liu, C.J.; Lin, Y.C.; Shih, S.C.; Hu, K.C. Effects of Helicobacter pylori infection in gastrointestinal tract malignant diseases: From the oral cavity to rectum. World J. Gastrointest. Oncol. 2022, 14, 55–74. [Google Scholar] [CrossRef]
- Smith, E.M.; Ritchie, J.M.; Summersgill, K.F.; Hoffman, H.T.; Wang, D.H.; Haugen, T.H.; Turek, L.P. Human papillomavirus in oral exfoliated cells and risk of head and neck cancer. J. Natl. Cancer Inst. 2004, 96, 449–455. [Google Scholar] [CrossRef]
- Golusiński, W.; Leemans, C.R.; Dietz, A. HPV Infection in Head and Neck Cancer, 1st ed.; Springer: Cham, Switzerland, 2017; pp. 4–18, 58, 73–78, 113–123. [Google Scholar]
- Cocuzza, S.; Marino, S.; Gulino, A.; Pustorino, E.; Murabito, P.; Maniaci, A.; Sabino, L.; Taibi, R.; Di Luca, M.; Falsaperla, R.; et al. ENT involvement and orobuccal movements’ disorders in Pandas patients: Assessment and rehabilitations tools. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 4110–4117. [Google Scholar] [PubMed]
- Pytko-Polonczyk, J.; Konturek, S.J.; Karczewska, E.; Bielański, W.; Kaczmarczyk-Stachowska, A. Oral cavity as permanent reservoir of Helicobacter pylori and potential source of reinfection. J. Physiol. Pharmacol. 1996, 47, 121–129. [Google Scholar] [PubMed]
- Kim, N.; Lim, S.H.; Lee, K.H.; You, J.Y.; Kim, J.M.; Lee, N.R.; Jung, H.C.; Song, I.S.; Kim, C.Y. Helicobacter pylori in dental plaque and saliva. Korean J. Intern. Med. 2000, 15, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Bulut, Y.; Agacayak, A.; Karlidag, T.; Toraman, Z.A.; Yilmaz, M. Association of cagA+ Helicobacter pylori with adenotonsillar hypertrophy. Tohoku J. Exp. Med. 2006, 209, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Jelavic, B.; Bevanda, M.; Ostojic, M.; Leventic, M.; Vasilj, M.; Knezevic, E. Tonsillar colonization is unlikely to play important role in Helicobacter pylori infection in children. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 585–590. [Google Scholar] [CrossRef]
- Toros, S.Z.; Toros, A.B.; Kaya, K.S.; Deveci, I.; Özel, L.; Naiboğlu, B.; Habeşoğlu, T.; Egeli, E. A study to detect Helicobacter pylori in adenotonsillar tissue. Ear Nose Throat J. 2011, 90, E32. [Google Scholar] [CrossRef]
- Kourieh, A.; Gheit, T.; Tommasino, M.; Dalstein, V.; Clifford, G.M.; Lacau St Guily, J.; Clavel, C.; Franceschi, S.; Combes, J.D. SPLIT study group. Prevalence of human herpesviruses infections in nonmalignant tonsils: The SPLIT study. J. Med. Virol. 2019, 91, 687–697. [Google Scholar] [CrossRef]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and Neck cancers-major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef]
- Ahmed, S.; Jafarey, N.A. Association of herpes simplex virus type-I and human papilloma virus with carcinoma of the oral cavity and oropharynx. J. Environ. Pathol. Toxicol. Oncol. 1995, 14, 193–196. [Google Scholar]
- Parker, T.M.; Smith, E.M.; Ritchie, J.M.; Haugen, T.H.; Vonka, V.; Turek, L.P.; Hamsikova, E. Head and neck cancer associated with herpes simplex virus 1 and 2 and other risk factors. Oral Oncol. 2006, 42, 288–296. [Google Scholar] [CrossRef]
- Hanon, E.; Hoornaert, S.; Dequiedt, F.; Vanderplasschen, A.; Lyaku, J.; Willems, L.; Pastoret, P.P. Bovine herpesvirus 1-induced apoptosis occurs at the G0/G1 phase of the cell cycle. Virology 1997, 232, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Kather, A.; Raftery, M.J.; Devi-Rao, G.; Lippmann, J.; Giese, T.; Sandri-Goldin, R.M.; Schönrich, G. Herpes simplex virus type 1 (HSV-1)-induced apoptosis in human dendritic cells as a result of downregulation of cellular FLICE-inhibitory protein and reduced expression of HSV-1 antiapoptotic latency-associated transcript sequences. J. Virol. 2010, 84, 1034–1046. [Google Scholar] [CrossRef] [PubMed]
- Lilley, C.E.; Carson, C.T.; Muotri, A.R.; Gage, F.H.; Weitzman, M.D. DNA repair proteins affect the lifecycle of herpes simplex virus 1. Proc. Natl. Acad. Sci. USA 2005, 102, 5844–5849. [Google Scholar] [CrossRef]
- Brown, S.H.; States, V.; Afghan, A.K.; Satyanarayana, G. Herpes simplex virus-infected squamous cell carcinoma: A case report. BMC Infect. Dis. 2022, 22, 25. [Google Scholar] [CrossRef] [PubMed]
- Hagglund, R.; Munger, J.; Poon, A.P.; Roizman, B. U(S)3 protein kinase of herpes simplex virus 1 blocks caspase 3 activation induced by the products of U(S)1.5 and U(L)13 genes and modulates expression of transduced U(S)1.5 open reading frame in a cell type-specific manner. J. Virol. 2002, 76, 743–754. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Patenode, C.; Roizman, B. US3 protein kinase of HSV-1 cycles between the cytoplasm and nucleus and interacts with programmed cell death protein 4 (PDCD4) to block apoptosis. Proc. Natl. Acad. Sci. USA 2011, 108, 14632–14636. [Google Scholar] [CrossRef] [PubMed]
- Turunen, A.; Hukkanen, V.; Kulmala, J.; Syrjanen, S. HSV-1 Infection Modulates the Radioresponse of a HPV16-positive Head and Neck Cancer Cell Line. Anticancer Res. 2016, 36, 565–574. [Google Scholar]
- Giacobbe, D.R.; Di Bella, S.; Lovecchio, A.; Ball, L.; De Maria, A.; Vena, A.; Bruzzone, B.; Icardi, G.; Pelosi, P.; Luzzati, R.; et al. Herpes Simplex Virus 1 (HSV-1) Reactivation in Critically Ill COVID-19 Patients: A Brief Narrative Review. Infect. Dis. Ther. 2022, 11, 1779–1791. [Google Scholar] [CrossRef]
- Jalouli, J.; Jalouli, M.M.; Sapkota, D.; Ibrahim, S.O.; Larsson, P.A.; Sand, L. Human papilloma virus, herpes simplex virus and epstein barr virus in oral squamous cell carcinoma from eight different countries. Anticancer Res. 2012, 32, 571–580. [Google Scholar]
- Dabouian, A.; Tabibzadeh, A.; Salimi-Jeda, A.; Torkashvand, S.; Panahi, M.; Tameshkel, F.S.; Zamani, F.; Keyvani, H.; Niya, M.H.K. The Molecular Epidemiology of Herpes Simplex Virus Type 1 and 2 (HSV-1 and HSV-2) in Head and Neck Cancer (HNC). Int. J. Cancer Manag. 2020, 13, e105916. [Google Scholar] [CrossRef]
- Liljeqvist, J.Å.; Tunbäck, P.; Norberg, P. Asymptomatically shed recombinant herpes simplex virus type 1 strains detected in saliva. J. Gen. Virol. 2009, 90 Pt 3, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Polz-Gruszka, D.; Stec, A.; Dworzański, J.; Polz-Dacewicz, M. EBV, HSV, CMV and HPV in laryngeal and oropharyngeal carcinoma in Polish patients. Anticancer Res. 2015, 35, 1657–1661. [Google Scholar]
- Bashir, R.A.; Elhag, W.I. Molecular Detection of Herpes Simplex Virus Types [1 and 2] in Orophar yngeal Squamous Cell Carcinoma (OSCC) in Khartoum Dental Education Hospital. J. Adv. Med. Med. Res. 2018, 26, 1–6. [Google Scholar] [CrossRef]
- Delavarian, Z.; Pakfetrat, A.; Falaki, F.; Pazouki, M.; Pazouki, N. The Role of Viruses in Oral Squamous Cell Carcinoma in Young Patients in Khorasan (Northeast of Iran). J. Appl. Sci. 2010, 10, 981–985. [Google Scholar] [CrossRef]
- Maden, C.; Beckmann, A.M.; Thomas, D.B.; McKnight, B.; Sherman, K.J.; Ashley, R.L.; Corey, L.; Daling, J.R. Human papillomaviruses, herpes simplex viruses, and the risk of oral cancer in men. Am. J. Epidemiol. 1992, 135, 1093–1102. [Google Scholar] [CrossRef]
- Mokhtari, M.; Beiraghdar, M. Evaluation of the prevalence of herpes simplex-1 infection in oral squamous cell carcinoma specimens in Alzahra and Kashani Hospitals with polymerase chain reaction method in 2012-2013. Adv. Biomed. Res. 2015, 4, 173. [Google Scholar]
- Osman, S.A.; Enan, K.A.; Mohamed, E.A. Molecular detection of herpes simplex virus (1, 2) in oral squamous cell carcinoma at Khartoum. Clin. Med. J. 2017, 2, 10–14. [Google Scholar]
- Devilleres-Mendoza, D.D.; Chang, J.V. Cytopathologic Herpes Simplex Virus Features In Laryngeal Squamous Cell Carcinoma. PhiliPPine J. Otolaryngol.-Head Neck Surg. 2016, 31, 61–64. [Google Scholar] [CrossRef]
- Shillitoe, E.J.; Greenspan, D.; Greenspan, J.S.; Silverman, S., Jr. Immunoglobulin class of antibody to herpes simplex virus in patients with oral cancer. Cancer 1983, 51, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Meurman, J.H. Infectious and dietary risk factors of oral cancer. Oral Oncol. 2010, 46, 411–413. [Google Scholar] [CrossRef]
- Saravanan, M.; Kolade Omole, R.; Torimiro, N. Oncogenic virus in oral squamous cell carcinoma and the role of oncolytic HSV-1 viro-immunotherapy as an emerging treatment. Oral Oncol. 2022, 133, 106021. [Google Scholar] [CrossRef] [PubMed]
- Strojnik, T.; Duh, D.; Lah, T.T. Prevalence of Neurotropic Viruses in Malignant Glioma and Their Onco-Modulatory Potential. Vivo 2017, 31, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Saddawi-Konefka, R.; Crawford, J.R. Chronic viral infection and primary central nervous system malignancy. J. Neuroimmune Pharmacol. 2010, 5, 387–403. [Google Scholar] [CrossRef]
- Kofman, A.; Marcinkiewicz, L.; Dupart, E.; Lyshchev, A.; Martynov, B.; Ryndin, A.; Kotelevskaya, E.; Brown, J.; Schiff, D.; Abounader, R. The roles of viruses in brain tumor initiation and oncomodulation. J. Neurooncol. 2011, 105, 451–466. [Google Scholar] [CrossRef]
- Pfeffer, S.; Sewer, A.; Lagos-Quintana, M.; Sheridan, R.; Sander, C.; Grässer, F.A.; van Dyk, L.F.; Ho, C.K.; Shuman, S.; Chien, M.; et al. Identification of microRNAs of the herpesvirus family. Nat. Methods 2005, 2, 269–276. [Google Scholar] [CrossRef]
- Vassallo, J.; Camargo, L.A.; Chagas, C.A.; Pinto, G.A.; Endo, L.H. Search for Herpesvirus 1 and 2 by in situ hybridization in tonsils and adenoids. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 345–349. [Google Scholar] [CrossRef]
- Sahin, F.; Gerceker, D.; Karasartova, D.; Ozsan, T.M. Detection of herpes simplex virus type 1 in addition to Epstein-Bar virus in tonsils using a new multiplex polymerase chain reaction assay. Diagn. Microbiol. Infect. Dis. 2007, 57, 47–51. [Google Scholar] [CrossRef]
- Sahiner, F.; Gümral, R.; Yildizoğlu, Ü.; Babayiğit, M.A.; Durmaz, A.; Yiğit, N.; Saraçli, M.A.; Kubar, A. Coexistence of Epstein-Barr virus and Parvovirus B19 in tonsillar tissue samples: Quantitative measurement by real-time PCR. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 1288–1293. [Google Scholar] [CrossRef]
- Lévy, P.; Kohler, M.; McNicholas, W.T.; Barbé, F.; McEvoy, R.D.; Somers, V.K.; Lavie, L.; Pépin, J.L. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Prim. 2015, 1, 15015. [Google Scholar] [CrossRef]
- Deegan, P.C.; McNicholas, W.T. Pathophysiology of obstructive sleep apnoea. Eur. Respir. J. 1995, 8, 1161–1178. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.P.; Ayappa, I.A.; Caples, S.M.; Kimoff, R.J.; Patel, S.R.; Harrod, C.G. Treatment of Adult Obstructive Sleep Apnea With Positive Airway Pressure: An American Academy of Sleep Medicine Systematic Review, Meta-Analysis, and GRADE Assessment. J. Clin. Sleep Med. 2019, 15, 301–334. [Google Scholar] [CrossRef]
- Antonopoulos, C.N.; Sergentanis, T.N.; Daskalopoulou, S.S.; Petridou, E.T. Nasal continuous positive airway pressure (nCPAP) treatment for obstructive sleep apnea, road traffic accidents and driving simulator performance: A meta-analysis. Sleep Med. Rev. 2011, 15, 301–310. [Google Scholar] [CrossRef] [PubMed]
- van Veldhuisen, S.L.; van Boxel, M.F.; Wiezer, M.J.; van Veen, R.N.; de Castro, S.M.M.; Swank, D.J.; Demirkiran, A.; Boerma, E.G.; Greve, J.W.M.; van Dielen, F.M.H.; et al. Evaluation of CPAP adherence in bariatric patients diagnosed with obstructive sleep apnea: Outcomes of a multicenter cohort study. Sleep Breath 2022, 1–10. [Google Scholar] [CrossRef]
- Iannella, G.; Lechien, J.R.; Perrone, T.; Meccariello, G.; Cammaroto, G.; Cannavicci, A.; Burgio, L.; Maniaci, A.; Cocuzza, S.; Di Luca, M.; et al. Barbed reposition pharyngoplasty (BRP) in obstructive sleep apnea treatment: State of the art. Am. J. Otolaryngol. 2022, 43, 103197. [Google Scholar] [CrossRef]
- Verbraecken, J.; Dieltjens, M.; Op de Beeck, S.; Vroegop, A.; Braem, M.; Vanderveken, O.; Randerath, W. Non-CPAP therapy for obstructive sleep apnoea. Breathe 2022, 18, 220164. [Google Scholar] [CrossRef]
- Gambino, F.; Zammuto, M.M.; Virzì, A.; Conti, G.; Bonsignore, M.R. Treatment options in obstructive sleep apnea. Intern. Emerg. Med. 2022, 17, 971–978. [Google Scholar] [CrossRef] [PubMed]
- James, C.; Harfouche, M.; Welton, N.J.; Turner, K.M.; Abu-Raddad, L.J.; Gottlieb, S.L.; Looker, K.J. Herpes simplex virus: Global infection prevalence and incidence estimates, 2016. Bull World Health Organ. 2020, 98, 315–329. [Google Scholar] [CrossRef]
- Yousuf, W.; Ibrahim, H.; Harfouche, M.; Abu Hijleh, F.; Abu-Raddad, L. Herpes simplex virus type 1 in Europe: Systematic review, meta-analyses and meta-regressions. BMJ Glob. Health 2020, 5, e002388. [Google Scholar] [CrossRef]
- Dworzański, J.; Drop, B.; Kliszczewska, E.; Strycharz-Dudziak, M.; Polz-Dacewicz, M. Prevalence of Epstein-Barr virus, human papillomavirus, cytomegalovirus and herpes simplex virus type 1 in patients with diabetes mellitus type 2 in south-eastern Poland. PLoS ONE 2019, 14, e0222607. [Google Scholar] [CrossRef] [PubMed]
- Olsson, J.; Kok, E.; Adolfsson, R.; Lövheim, H.; Elgh, F. Herpes virus seroepidemiology in the adult Swedish population. Immun. Ageing 2017, 14, 10. [Google Scholar] [CrossRef]
- Malkin, J.E.; Morand, P.; Malvy, D.; Ly, T.D.; Chanzy, B.; de Labareyre, C.; El Hasnaoui, A.; Hercberg, S. Seroprevalence of HSV-1 and HSV-2 infection in the general French population. Sex. Transm. Infect. 2002, 78, 201–203. [Google Scholar] [CrossRef] [PubMed]
- Marchi, S.; Trombetta, C.M.; Gasparini, R.; Temperton, N.; Montomoli, E. Epidemiology of herpes simplex virus type 1 and 2 in Italy: A seroprevalence study from 2000 to 2014. J. Prev. Med. Hyg. 2017, 58, E27–E33. [Google Scholar] [PubMed]
- McQuillan, G.; Kruszon-Moran, D.; Flagg, E.W.; Paulose-Ram, R. Prevalence of Herpes Simplex Virus Type 1 and Type 2 in Persons Aged 14-49: United States, 2015-2016. NCHS Data Brief. 2018, 1–8. Available online: https://www.cdc.gov/nchs/products/databriefs/db304.htm (accessed on 25 April 2023).
- Sukik, L.; Alyafei, M.; Harfouche, M.; Abu-Raddad, L.J. Herpes simplex virus type 1 epidemiology in Latin America and the Caribbean: Systematic review and meta-analytics. PLoS ONE 2019, 14, e0215487. [Google Scholar] [CrossRef] [PubMed]
- Doi, Y.; Ninomiya, T.; Hata, J.; Yonemoto, K.; Tanizaki, Y.; Arima, H.; Liu, Y.; Rahman, M.; Iida, M.; Kiyohara, Y. Seroprevalence of herpes simplex virus 1 and 2 in a population-based cohort in Japan. J. Epidemiol. 2009, 19, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Malary, M.; Abedi, G.; Hamzehgardeshi, Z.; Afshari, M.; Moosazadeh, M. The prevalence of herpes simplex virus type 1 and 2 infection in Iran: A meta-analysis. Int. J. Reprod. Biomed. 2016, 14, 615–624. [Google Scholar] [CrossRef]
- Harfouche, M.; Chemaitelly, H.; Abu-Raddad, L.J. Herpes simplex virus type 1 epidemiology in Africa: Systematic review, meta-analyses, and meta-regressions. J. Infect. 2019, 79, 289–299. [Google Scholar] [CrossRef]
- Katz, I.; De Luca, F.; Dzudzor, B.; Sarpong, B.K.; Osei-Appiah, B.; Azoulay, D.; Katz, D.; Dey, D.; Gilburd, B.; Amital, H.; et al. Seroprevalences of autoantibodies and anti- infectious antibodies among Ghana's healthy population. Sci. Rep. 2020, 10, 2814. [Google Scholar]
- Palacios-Pedrero, M.Á.; Osterhaus, A.D.M.E.; Becker, T.; Elbahesh, H.; Rimmelzwaan, G.F.; Saletti, G. Aging and Options to Halt Declining Immunity to Virus Infections. Front. Immunol. 2021, 12, 681449. [Google Scholar] [CrossRef]
- Wald, A.; Ashley-Morrow, R. Serological testing for herpes simplex virus (HSV)-1 and HSV-2 infection. Clin. Infect. Dis. 2002, 35 (Suppl. 2), S173–S182. [Google Scholar] [CrossRef]
- Miller, C.S.; Danaher, R.J. Asymptomatic shedding of herpes simplex virus (HSV) in the oral cavity. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, 43–50. [Google Scholar] [CrossRef]
- Koelle, D.M.; Magaret, A.; Warren, T.; Schellenberg, G.D.; Wald, A. APOE genotype is associated with oral herpetic lesions but not genital or oral herpes simplex virus shedding. Sex. Transm. Infect. 2010, 86, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Mark, K.E.; Wald, A.; Magaret, A.S.; Selke, S.; Olin, L.; Huang, M.L.; Corey, L. Rapidly cleared episodes of herpes simplex virus reactivation in immunocompetent adults. J. Infect. Dis. 2008, 198, 1141–1149. [Google Scholar] [CrossRef]
- Ramchandani, M.S.; Jing, L.; Russell, R.M.; Tran, T.; Laing, K.J.; Magaret, A.S.; Selke, S.; Cheng, A.; Huang, M.L.; Xie, H.; et al. Viral Genetics Modulate Orolabial Herpes Simplex Virus Type 1 Shedding in Humans. J. Infect. Dis. 2019, 219, 1058–1066. [Google Scholar] [CrossRef]
- Yap, T.; Khor, S.; Kim, J.S.; Kim, J.; Kim, S.Y.; Kern, J.S.; Martyres, R.; Varigos, G.; Chan, H.T.; McCullough, M.J.; et al. Intraoral human herpes viruses detectable by PCR in majority of patients. Oral Dis. 2021, 27, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Margolis, T.P.; Imai, Y.; Yang, L.; Vallas, V.; Krause, P.R. Herpes simplex virus type 2 (HSV-2) establishes latent infection in a different population of ganglionic neurons than HSV-1: Role of latency-associated transcripts. J. Virol. 2007, 81, 1872–1878. [Google Scholar] [CrossRef]
- Kizilay, A.; Saydam, L.; Aydin, A.; Kalcioglu, M.T.; Ozturan, O.; Aydin, N.E. Histopathologic examination for Helicobacter pylori as a possible etiopathogenic factor in laryngeal carcinoma. Chemotherapy 2006, 52, 80–82. [Google Scholar] [CrossRef]
- Fernando, N.; Jayakumar, G.; Perera, N.; Amarasingha, I.; Meedin, F.; Holton, J. Presence of Helicobacter pylori in betel chewers and non betel chewers with and without oral cancers. BMC Oral Health 2009, 9, 23. [Google Scholar] [CrossRef] [PubMed]
- Gong, H.; Shi, Y.; Zhou, L.; Tao, L.; Shi, Y.; Cao, W.; Cheng, L. Helicobacter pylori infection of the larynx may be an emerging risk factor for laryngeal squamous cell carcinoma. Clin. Transl. Oncol. 2012, 14, 905–910. [Google Scholar] [CrossRef]
- Ozdek, A.; Cirak, M.Y.; Samim, E.; Bayiz, U.; Safak, M.A.; Turet, S. A possible role of Helicobacter pylori in chronic rhinosinusitis: A preliminary report. Laryngoscope 2003, 113, 679–682. [Google Scholar]
- Morinaka, S.; Tominaga, M.; Nakamura, H. Detection of Helicobacter pylori in the middle ear fluid of patients with otitis media with effusion. Otolaryngol.-Head Neck Surg. 2005, 133, 791–794. [Google Scholar] [CrossRef]
- Burduk, P.K.; Kaczmarek, A.; Budzynska, A.; Kazmierczak, W.; Gospodarek, E. Detection of Helicobacter pylori and cagA gene in nasal polyps and benign laryngeal diseases. Arch. Med. Res. 2011, 42, 686–689. [Google Scholar] [CrossRef]
- Cekin, E.; Ozyurt, M.; Erkul, E.; Ergunay, K.; Cincik, H.; Kapucu, B.; Gungor, A. The association between Helicobacter pylori and laryngopharyngeal reflux in laryngeal pathologies. Ear Nose Throat J. 2012, 91, E6–E9. [Google Scholar] [CrossRef] [PubMed]
- Jelavic, B.; Petricevic, J.; Marijanović, I.; Bevanda, M. Helicobacter pylori in Otorhinolaryngology: Cause or Bystander. Eurasian J. Med. 2019, 51, 196–202. [Google Scholar]
- Meng, X.; Wang, Q.; He, C.; Chen, M.; Liu, J.; Liu, W.; Yuan, Y. An inverse association of Helicobacter pylori infection with oral squamous cell carcinoma. J. Oral Pathol. Med. 2016, 45, 17–22. [Google Scholar] [CrossRef]
- Zhou, J.; Zhang, D.; Yang, Y.; Zhou, L.; Tao, L. Association between helicobacter pylori infection and carcinoma of the larynx or pharynx. Head Neck. 2016, 38 (Suppl. 1), E2291–E2296. [Google Scholar] [CrossRef]
- Lukeš, P.; Pavlík, E.; Potuznikova, B.; Nartova, E.; Foltynova, E.; Plzak, J.; Katra, R.; Sterzl, I.; Bartunkova, J.; Betka, J.; et al. Detection of Helicobacter pylori in oropharyngeal lymphatic tissue with real-time PCR and assessment of its carcinogenic potential. Eur. Arch. Otorhinolaryngol. 2014, 271, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Meng, W.P.; Wang, Z.Q.; Deng, J.Q.; Liu, Y.; Deng, M.M.; Lü, M.H. The Role of H. pylori CagA in Regulating Hormones of Functional Dyspepsia Patients. Gastroenterol. Res. Pract. 2016, 2016, 7150959. [Google Scholar] [CrossRef]
- Yilmaz, T.; Ceylan, M.; Akyön, Y.; Özçakýr, O.; Gürsel, B. Helicobacter pylori: A possible association with otitis media with effusion. Otolaryngol. Head Neck Surg. 2006, 134, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Mohtasham, N.; Saghravanian, N.; Zare, R.; Saghafi, S.; Ghazi, N.; Mohajertehran, F.; Shahabinejad, M. Tumor tissue Helicobacter pylori and human papillomavirus infection in head and neck squamous cell carcinoma patients and association with clinicopathological indices: A cross-sectional medical survey. Dent. Res. J. 2022, 19, 8. [Google Scholar]
- Akbayir, N.; Başak, T.; Seven, H.; Sungun, A.; Erdem, L. Investigation of Helicobacter pylori colonization in laryngeal neoplasia. Eur. Arch. Oto-Rhino-Laryngol. 2005, 262, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Morand, G.B.; Fellmann, J.; Laske, R.D.; Weisert, J.U.; Soltermann, A.; Zbinden, R.; Probst, R.; Huber, G.F. Detection of Helicobacter pylori in patients with head and neck cancer: Results from a prospective comparative study combining serology, polymerase chain reaction, and rapid urease test. Head Neck 2016, 38, 769–774. [Google Scholar] [CrossRef]
- Masoud, N.; Manouchehr, K.; Najmeh, D.; Monireh, H. Lack of association between Helicobacter pylori and laryngeal carcinoma. Asian Pac. J. Cancer Prev. 2008, 9, 81–82. [Google Scholar] [PubMed]
- Pandey, S.; Jha, H.C.; Shukla, S.K.; Shirley, M.K.; Robertson, E.S. Epigenetic Regulation of Tumor Suppressors by Helicobacter pylori Enhances EBV-Induced Proliferation of Gastric Epithelial Cells. mBio 2018, 9, e00649-18. [Google Scholar] [CrossRef] [PubMed]
- Burduk, P.K. Rola infekcji helicobacter pylori w patogenezie raka krtani [The role of helicobacter pylori infection in carcinoma of the larynx]. Otolaryngol. Pol. 2006, 60, 521–523. (In Polish) [Google Scholar] [PubMed]
- Burduk, P.K. Association between infection of virulence cagA gene Helicobacter pylori and laryngeal squamous cell carcinoma. Med. Sci. Monit. 2013, 19, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Aygenc, E.; Selcuk, A.; Celikkanat, S.; Ozbek, C.; Ozdem, C. The role of Helicobacter pylori infection in the cause of squamous cell carcinoma of the larynx. Otolaryngol. Head Neck Surg. 2001, 125, 520–521. [Google Scholar] [CrossRef]
- Titiz, A.; Ozcakir, O.; Ceyhan, S.; Yilmaz, Y.F.; Unal, A.; Akyon, Y. The presence of Helicobacter pylori in the larynx pathologies. Auris Nasus Larynx 2008, 35, 534–538. [Google Scholar] [CrossRef]
- Shi, Y.; Gong, H.; Zhou, L.; Tao, L.; Shi, Y.; Cao, W.; Cheng, L. Association between Helicobacter pylori infection and laryngeal squamous cell carcinoma in a Chinese male population. ORL J. Otorhinolaryngol. Relat. Spec. 2011, 73, 295–300. [Google Scholar] [CrossRef]
- Astl, J.; Holy, R.; Maute, E.; Rotnágl, J.; Kalfeřt, D.; Drnková, B.; Younus, T.; Pavlík, E. Genome of Helicobacter pylori and Serotype of HPV Detected in Oropharyngeal and Laryngeal Cancer and Chronic Inflammation Patients. Int. J. Environ. Res. Public Health 2021, 18, 9545. [Google Scholar] [CrossRef]
- Pajić Matić, I.; Matić, I.; Maslovara, S.; Veselski, K.; Stojadinović, T.; Vučković, I. Helicobacter pylori gastric infection in patients with laryngeal cancer and chronic laryngitis. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 135–139. [Google Scholar] [CrossRef]
- Rezaii, J.; Tavakoli, H.; Esfandiari, K.; Ashegh, H.; Hasibi, M.; Ghanei, G.; Khosh-Batn, M.; Rashidi, A. Association between Helicobacter pylori infection and laryngohypopharyngeal carcinoma: A case-control study and review of the literature. Head Neck 2008, 30, 1624–1627. [Google Scholar] [CrossRef]
- Kariya, S.; Okano, M.; Nishizaki, K. An association between Helicobacter pylori and upper respiratory tract disease: Fact or fiction? World J. Gastroenterol. 2014, 20, 1470–1484. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Jakubovics, N.S.; Bächle, M.; Buchalla, W.; Hiller, K.A.; Maisch, T.; Hellwig, E.; Kirschneck, C.; Gessner, A.; Al-Ahmad, A.; et al. Colonization of Helicobacter pylori in the oral cavity—An endless controversy? Crit. Rev. Microbiol. 2021, 47, 612–629. [Google Scholar] [CrossRef] [PubMed]
- Aslan, S.; Yilmaz, I.; Bal, N.; Sener, M.; Butros, R.; Demirhan, B.; Ozluoglu, L.N. Investigation of Helicobacter pylori in tonsillary tissue with Pronto Dry test and pathologic examination. Auris Nasus Larynx 2007, 34, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; Wu, P.Y.; Friedman, M.; Chang, H.W.; Wilson, M. Difference of Helicobacter pylori colonization in recurrent inflammatory and simple hyperplastic tonsil tissues. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 468–470. [Google Scholar] [CrossRef]
- Güçlü, O.; Akçalı, A.; Sahin, E.M.; Tekin, K.; Barutçu, O.; Otkun, M.T.; Dereköy, F.S. Relationship between Helicobacter pylori Adenotonsillar Colonization and Frequency of Adenotonsillitis in Children. Balk. Med. J. 2013, 30, 301–304. [Google Scholar] [CrossRef]
- Nártová, E.; Kraus, J.; Pavlík, E.; Lukeš, P.; Katra, R.; Plzák, J.; Kolářová, L.; Sterzl, I.; Betka, J.; Astl, J. Presence of different genotypes of Helicobacter pylori in patients with chronic tonsillitis and sleep apnoea syndrome. Eur. Arch. Otorhinolaryngol. 2014, 271, 607–613. [Google Scholar] [CrossRef]
- Siupsinskiene, N.; Katutiene, I.; Jonikiene, V.; Janciauskas, D.; Vaitkus, S. Helicobacter pylori in the tonsillar tissue: A possible association with chronic tonsillitis and laryngopharyngeal reflux. J. Laryngol. Otol. 2017, 131, 549–556. [Google Scholar] [CrossRef]
- Wu, X.; Wang, W.; Fang, L.; Shi, L.; Rao, X. Is Helicobacter pylori colonization associated with chronic tonsillitis? - A meta-analysis and systematic review. Am. J. Otolaryngol. 2022, 43, 103515. [Google Scholar] [CrossRef]
- Burne, R.A.; Chen, Y.Y. Bacterial ureases in infectious diseases. Microbes. Infect. 2000, 2, 533–542. [Google Scholar] [CrossRef]
- Celiński, K.; Kurzeja-Mirosław, A.; Słomka, M.; Cichoz-Lach, H.; Madro, A.; Kasztelan-Szczerbińska, B. The effects of environmental factors on the prevalence of Helicobacter pylori infection in inhabitants of Lublin Province. Ann. Agric. Env. Med. 2006, 13, 185–191. [Google Scholar]
- Szczepanik, A.B.; Zaleska, M.; Wiszniewski, A.; Wislawski, S.; Misiak, A.; Maryniak, R.; Windyga, J. Helicobacter pylori infection in patients with haemophilia in Poland: Prevalence and risk of upper gastrointestinal bleeding. Haemophilia. 2005, 11, 376–379. [Google Scholar] [CrossRef]
- Bureš, J.; Kopáčová, M.; Koupil, I.; Seifert, B.; Skodová Fendrichová, M.; Spirková, J.; Voříšek, V.; Rejchrt, S.; Douda, T.; Král, N.; et al. Significant decrease in prevalence of Helicobacter pylori in the Czech Republic. World J. Gastroenterol. 2012, 18, 4412–4418. [Google Scholar] [CrossRef]
- Bálint, L.; Tiszai, A.; Kozák, G.; Dóczi, I.; Szekeres, V.; Inczefi, O.; Ollé, G.; Helle, K.; Róka, R.; Rosztóczy, A. Epidemiologic characteristics of Helicobacter pylori infection in southeast Hungary. World J. Gastroenterol. 2019, 25, 6365–6372. [Google Scholar] [CrossRef] [PubMed]
- van Blankenstein, M.; van Vuuren, A.J.; Looman, C.W.; Ouwendijk, M.; Kuipers, E.J. The prevalence of Helicobacter pylori infection in the Netherlands. Scand. J. Gastroenterol. 2013, 48, 794–800. [Google Scholar] [CrossRef]
- Lorenzo, I.; Fernández-de-Larrea, N.; Michel, A.; Romero, B.; Lope, V.; Bessa, X.; Moreno, V.; Martín, V.; Amiano, P.; Castilla, J.; et al. Helicobacter pylori seroprevalence in Spain: Influence of adult and childhood sociodemographic factors. Eur. J. Cancer Prev. 2019, 28, 294–303. [Google Scholar] [CrossRef]
- Roberts, S.E.; Morrison-Rees, S.; Samuel, D.G.; Thorne, K.; Akbari, A.; Williams, J.G. Review article: The prevalence of Helicobacter pylori and the incidence of gastric cancer across Europe. Aliment. Pharmacol. Ther. 2016, 43, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Wang, X.; Liu, K.; Chen, K. Association between Helicobacter pylori infection and the risk of type 2 diabetes mellitus based on a middle-aged and elderly Chinese population. Endocr. J. 2022, 69, 839–846. [Google Scholar] [CrossRef]
- Ito, M.; Sugiyama, A.; Mino, M.; Kodama, M.; Nagaoki, Y.; Abe, K.; Imada, H.; Ouoba, S.E.B.; Ko, K.; Akita, T.; et al. Prevalence of Helicobacter pylori infection in the general population evaluated by a resident-register-based epidemiological study. J. Gastroenterol. 2022, 57, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Mežmale, L.; Polaka, I.; Rudzite, D.; Vangravs, R.; Kikuste, I.; Parshutin, S.; Daugule, I.; Tazhedinov, A.; Belikhina, T.; Igissinov, N.; et al. Prevalence and Potential Risk Factors of Helicobacter pylori Infection among Asymptomatic Individuals in Kazakhstan. Asian Pac. J. Cancer Prev. 2021, 22, 597–602. [Google Scholar] [CrossRef]
- Zaterka, S.; Eisig, J.N.; Chinzon, D.; Rothstein, W. Factors related to Helicobacter pylori prevalence in an adult population in Brazil. Helicobacter 2007, 12, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Willems, P.; de Repentigny, J.; Hassan, G.M.; Sidani, S.; Soucy, G.; Bouin, M. The Prevalence of Helicobacter pylori Infection in a Quaternary Hospital in Canada. J. Clin. Med. Res. 2020, 12, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Kadota, T.; Hamada, M.; Nomura, R.; Ogaya, Y.; Okawa, R.; Uzawa, N.; Nakano, K. Distribution of Helicobacter pylori and Periodontopathic Bacterial Species in the Oral Cavity. Biomedicines 2020, 8, 161. [Google Scholar] [CrossRef]
- Šeligová, B.; Lukáč, Ľ.; Bábelová, M.; Vávrová, S.; Sulo, P. Diagnostic reliability of nested PCR depends on the primer design and threshold abundance of Helicobacter pylori in biopsy, stool, and saliva samples. Helicobacter 2020, 25, e12680. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All | HNSCC | Chronic Tonsillitis | Control | |||||
|---|---|---|---|---|---|---|---|---|
| Median | Range | Median | Range | Median | Range | Median | Range | |
| Age | 41 | 29–57.5 | 60 | 52–65 | 33 | 24–41 | 33 | 24–49.25 |
| N | % | N | % | N | % | N | % | |
| Age ≥ 40 | 153 | 51.86 | 84 | 93.33 | 26 | 27.96 | 43 | 38.39 |
| Age < 40 | 142 | 48.14 | 6 | 6.67 | 67 | 72.04 | 69 | 61.61 |
| Female | 140 | 47.46 | 26 | 28.89 | 51 | 54.84 | 63 | 56.25 |
| Male | 155 | 52.54 | 64 | 71.11 | 42 | 45.16 | 49 | 43.75 |
| Smoking | 109 | 36.95 | 65 | 72.22 | 14 | 15.05 | 31 | 27.68 |
| Not smoking | 186 | 63.05 | 25 | 27.78 | 79 | 84.95 | 81 | 72.32 |
| Drinking | 182 | 61.69 | 61 | 67.78 | 29 | 31.18 | 92 | 82.14 |
| Regular drinking | 22 | 7.46 | 11 | 12.22 | 3 | 3.23 | 8 | 7.14 |
| Occasional drinking | 160 | 54.24 | 50 | 55.56 | 26 | 27.96 | 84 | 75.00 |
| Not drinking | 113 | 38.31 | 29 | 32.22 | 64 | 68.82 | 20 | 17.86 |
| Smoking and drinking | 85 | 28.81 | 50 | 55.56 | 8 | 8.60 | 27 | 24.11 |
| Drinking; not smoking | 96 | 32.54 | 11 | 12.22 | 20 | 21.51 | 65 | 58.04 |
| Smoking; not drinking | 26 | 8.81 | 15 | 16.67 | 7 | 7.53 | 4 | 3.57 |
| Not smoking; not drinking | 88 | 29.83 | 14 | 15.56 | 58 | 62.37 | 16 | 14.29 |
| N | (%) | ||
|---|---|---|---|
| Clinical T-classification | 90 | (100.00) | |
| T1 | 10 | 11.1 | |
| T2 | 22 | 24.4 | |
| T3 | 28 | 31.1 | |
| T4 | 30 | 33.3 | |
| T1 + T2 | 32 | 35.6 | |
| T3 + T4 | 58 | 64.4 | |
| Lymph node status | 90 | (100.00) | |
| N0 | 43 | 47.8 | |
| N1 | 22 | 24.4 | |
| N2 | 22 | 24.4 | |
| N3 | 3 | 3.3 | |
| N1 + N2 | 44 | 48.8 | |
| Histological grade | 90 | (100.00) | |
| G1 | 15 | 16.7 | |
| G2 | 56 | 62.2 | |
| G3 | 19 | 21.1 | |
| G1 + G2 | 71 | 78.9 | |
| Stage | 90 | (100.00) | |
| I | 7 | 7.78 | |
| II | 12 | 13.33 | |
| III | 21 | 23.33 | |
| IV | 50 | 55.56 |
| HSV-1 | H. pylori | |
|---|---|---|
| Control vs. HNSCC | 0.283 | 0.035 |
| Control vs. Chronic tonsillitis | 0.376 | 0.353 |
| Chronic tonsillitis vs. HNSCC | 0.841 | 0.099 |
| Study Group | Variable | Variant | HSV-1 | p | H. pylori | p | ||
|---|---|---|---|---|---|---|---|---|
| Negative | Positive | Negative | Positive | |||||
| HNSCC | Age | ≥40 | 77 | 7 | 1 | 84 | 0 | 1 |
| <40 | 6 | 0 | 6 | 0 | ||||
| Gender | Female | 23 | 3 | 0.407 | 26 | 0 | 1 | |
| Male | 60 | 4 | 64 | 0 | ||||
| Drinking | Yes | 55 | 6 | 0.422 | 61 | 0 | 1 | |
| No | 28 | 1 | 29 | 0 | ||||
| Smoking | Yes | 59 | 6 | 0.668 | 65 | 0 | 1 | |
| No | 24 | 1 | 25 | 0 | ||||
| Chronic tonsillitis | Age | ≥40 | 24 | 2 | 1 | 24 | 2 | 0.188 |
| <40 | 61 | 6 | 66 | 1 | ||||
| Gender | Female | 47 | 4 | 1 | 49 | 2 | 1 | |
| Male | 38 | 4 | 39 | 1 | ||||
| Drinking | Yes | 27 | 2 | 1 | 27 | 2 | 0.228 | |
| No | 58 | 6 | 63 | 1 | ||||
| Smoking | Yes | 11 | 3 | 0.097 | 14 | 0 | 1 | |
| No | 74 | 5 | 76 | 3 | ||||
| Control | Age | ≥40 | 34 | 9 | 0.042 | 40 | 3 | 1 |
| <40 | 64 | 5 | 65 | 4 | ||||
| Gender | Female | 57 | 6 | 0.389 | 61 | 2 | 0.237 | |
| Male | 41 | 8 | 44 | 5 | ||||
| Drinking | Yes | 82 | 10 | 0.272 | 86 | 6 | 1 | |
| No | 16 | 4 | 19 | 1 | ||||
| Smoking | Yes | 26 | 5 | 0.527 | 29 | 2 | 1 | |
| No | 72 | 9 | 76 | 5 | ||||
| Study Group | Variable | Variant | HSV-1 | p | H. pylori | p | ||
|---|---|---|---|---|---|---|---|---|
| Negative | Positive | Negative | Positive | |||||
| HNSCC | T1 | Yes | 10 | 0 | 1 | 10 | 0 | 1 |
| No | 73 | 7 | 80 | 0 | ||||
| T2 | Yes | 22 | 0 | 0.188 | 22 | 0 | 1 | |
| No | 61 | 7 | 68 | 0 | ||||
| T3 | Yes | 27 | 1 | 0.428 | 28 | 0 | 1 | |
| No | 56 | 6 | 62 | 0 | ||||
| T4 | Yes | 24 | 6 | 0.005 | 30 | 0 | 1 | |
| No | 59 | 1 | 60 | 0 | ||||
| T1 + T2 | Yes | 32 | 0 | 0.048 | 32 | 0 | 1 | |
| No | 51 | 7 | 58 | 0 | ||||
| T3 + T4 | Yes | 51 | 7 | 0.048 | 58 | 0 | 1 | |
| No | 51 | 0 | 32 | 0 | ||||
| Stage I | Yes | 7 | 0 | 1 | 7 | 0 | 1 | |
| No | 76 | 7 | 83 | 0 | ||||
| Stage II | Yes | 12 | 0 | 0.588 | 12 | 0 | 1 | |
| No | 71 | 7 | 78 | 0 | ||||
| Stage III | Yes | 21 | 0 | 0.193 | 90 | 0 | 1 | |
| No | 62 | 7 | 69 | 0 | ||||
| Stage IV | Yes | 50 | 7 | 0.044 | 50 | 0 | 1 | |
| No | 33 | 0 | 40 | 0 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strzelczyk, J.K.; Świętek, A.; Hudy, D.; Gołąbek, K.; Gaździcka, J.; Miśkiewicz-Orczyk, K.; Ścierski, W.; Strzelczyk, J.; Misiołek, M. Low Prevalence of HSV-1 and Helicobacter pylori in HNSCC and Chronic Tonsillitis Patients Compared to Healthy Individuals. Diagnostics 2023, 13, 1798. https://doi.org/10.3390/diagnostics13101798
Strzelczyk JK, Świętek A, Hudy D, Gołąbek K, Gaździcka J, Miśkiewicz-Orczyk K, Ścierski W, Strzelczyk J, Misiołek M. Low Prevalence of HSV-1 and Helicobacter pylori in HNSCC and Chronic Tonsillitis Patients Compared to Healthy Individuals. Diagnostics. 2023; 13(10):1798. https://doi.org/10.3390/diagnostics13101798
Chicago/Turabian StyleStrzelczyk, Joanna Katarzyna, Agata Świętek, Dorota Hudy, Karolina Gołąbek, Jadwiga Gaździcka, Katarzyna Miśkiewicz-Orczyk, Wojciech Ścierski, Janusz Strzelczyk, and Maciej Misiołek. 2023. "Low Prevalence of HSV-1 and Helicobacter pylori in HNSCC and Chronic Tonsillitis Patients Compared to Healthy Individuals" Diagnostics 13, no. 10: 1798. https://doi.org/10.3390/diagnostics13101798