
Predictive Value of Cervical Shear Wave Elastography in the Induction of Labor in Late-Term Pregnancy Nulliparous Women: Preliminary Results
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
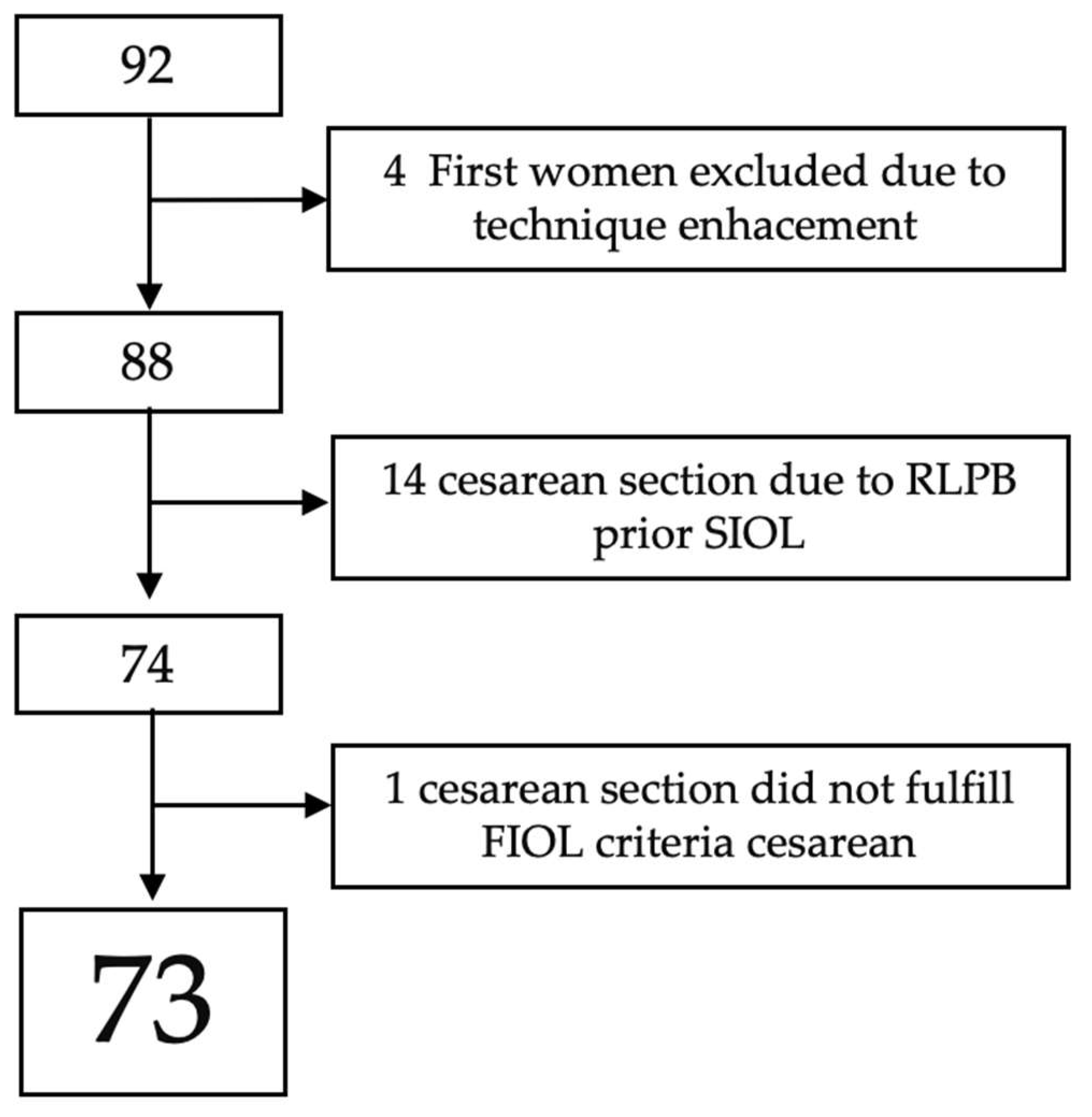
2.1. Study Design
2.2. Sample Size
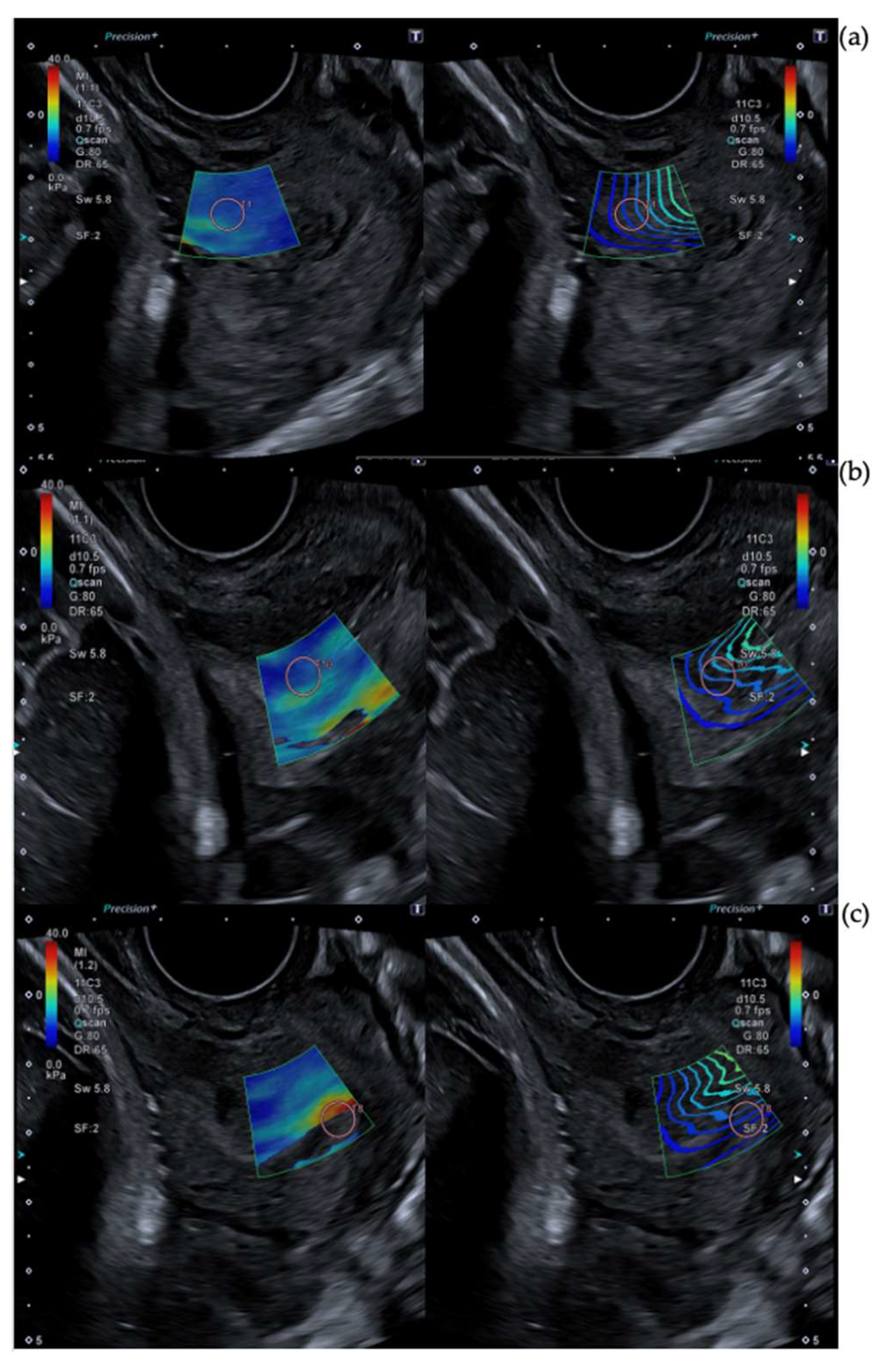
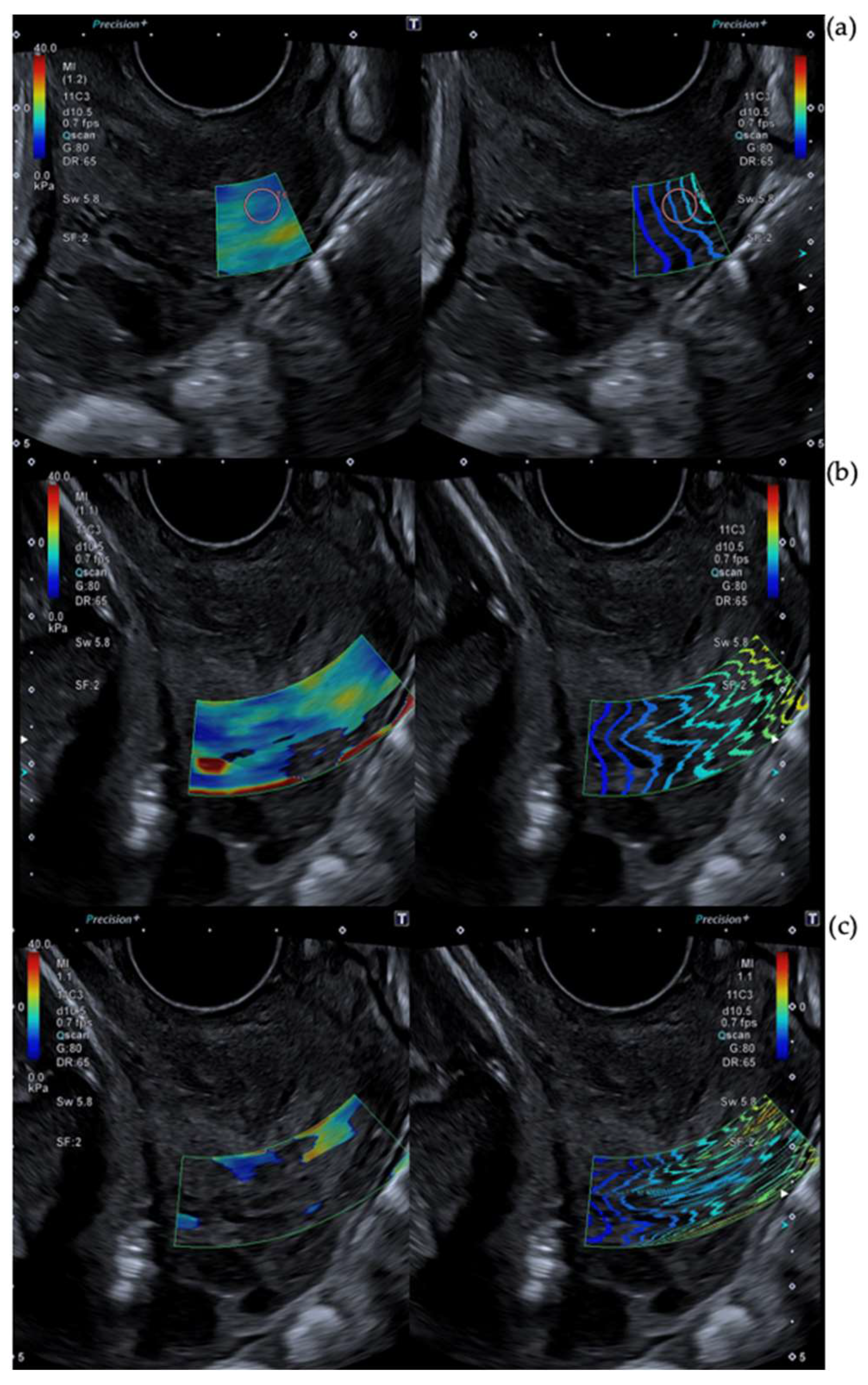
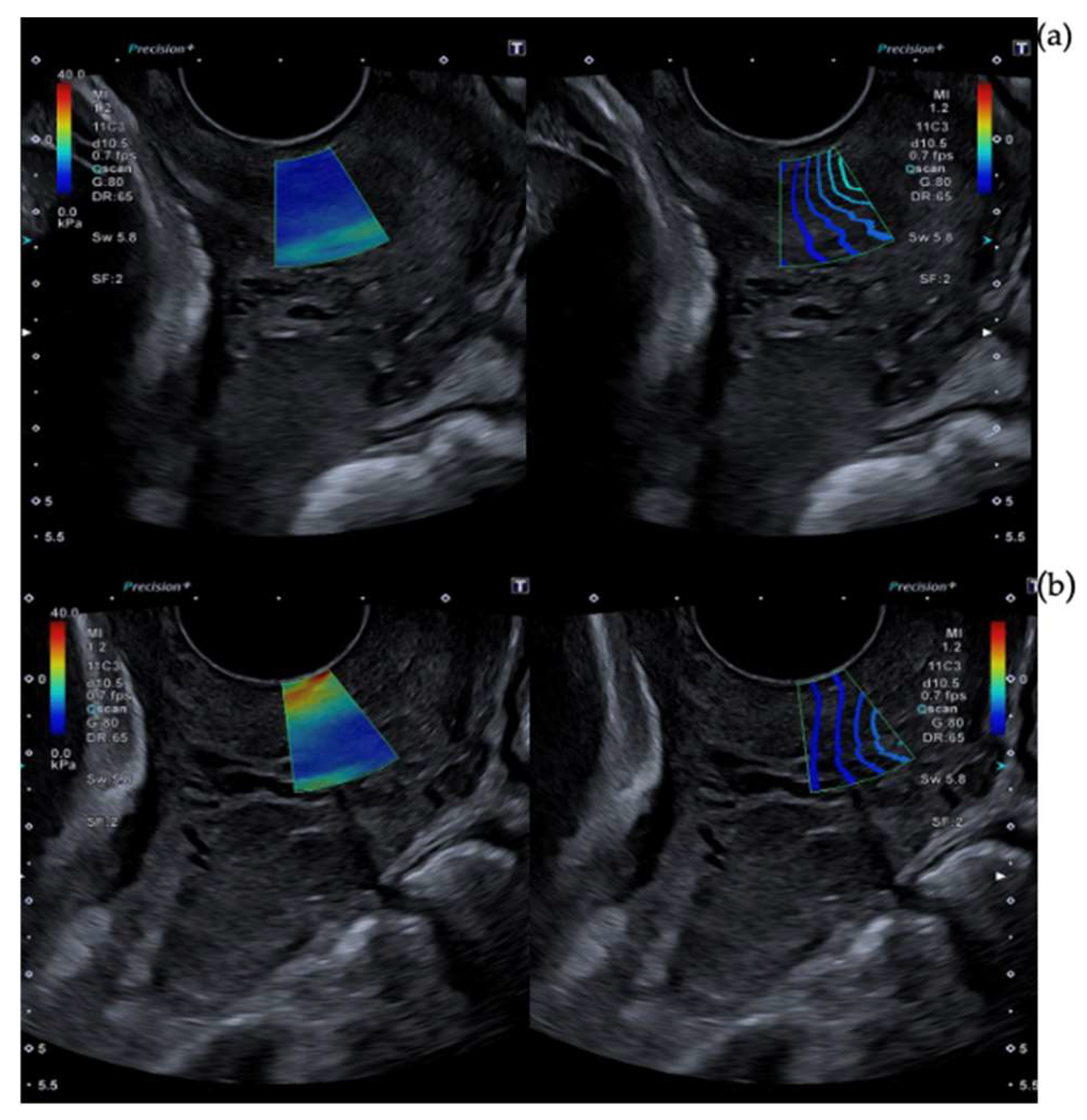
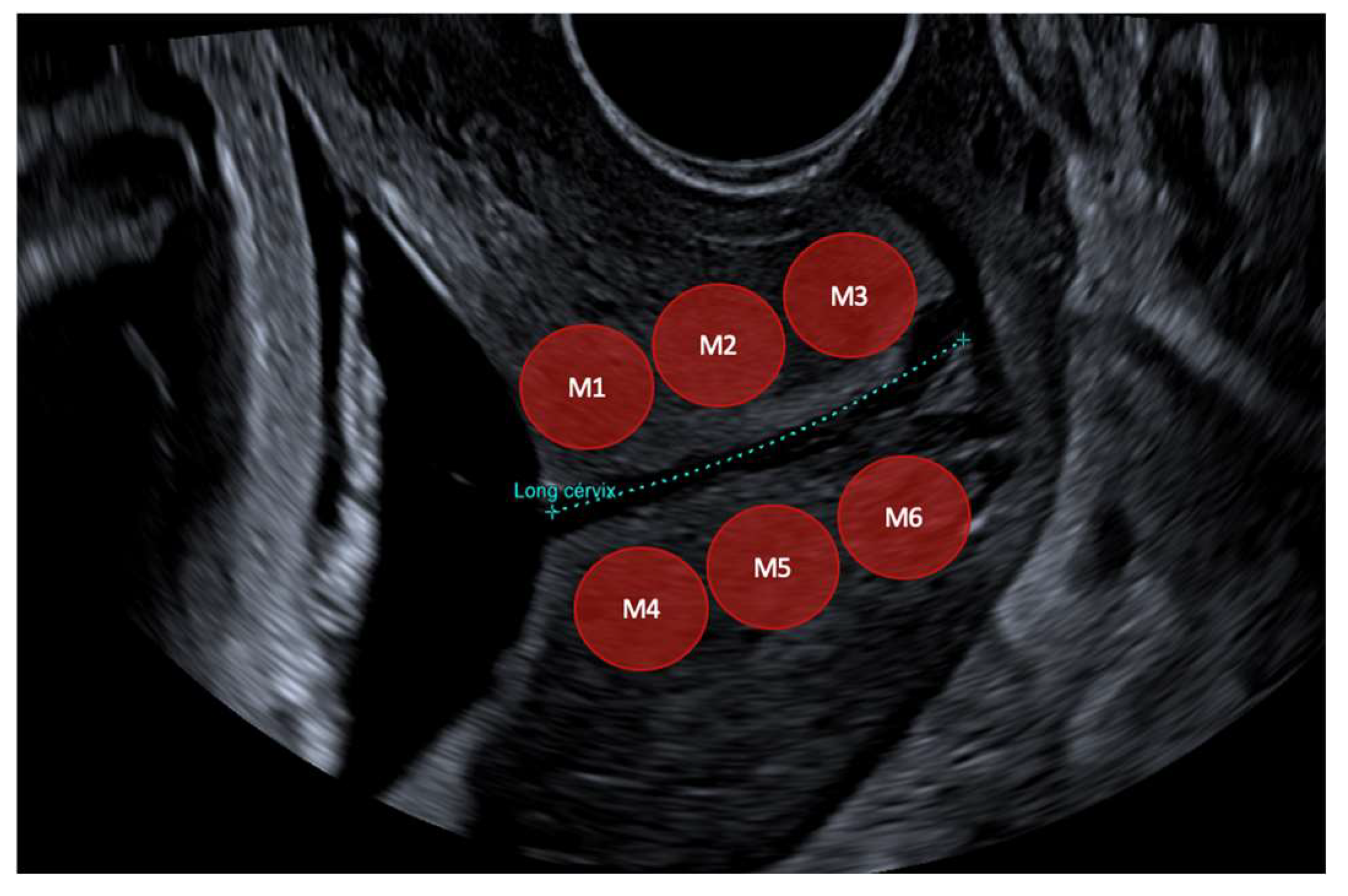
2.3. Cervical Shear Wave Elastography Measurement
2.4. Induction of Labor
2.5. Failure to Progress, Cesarean Indications
2.6. Statistical Analyses
3. Results
3.1. Population Characteristics
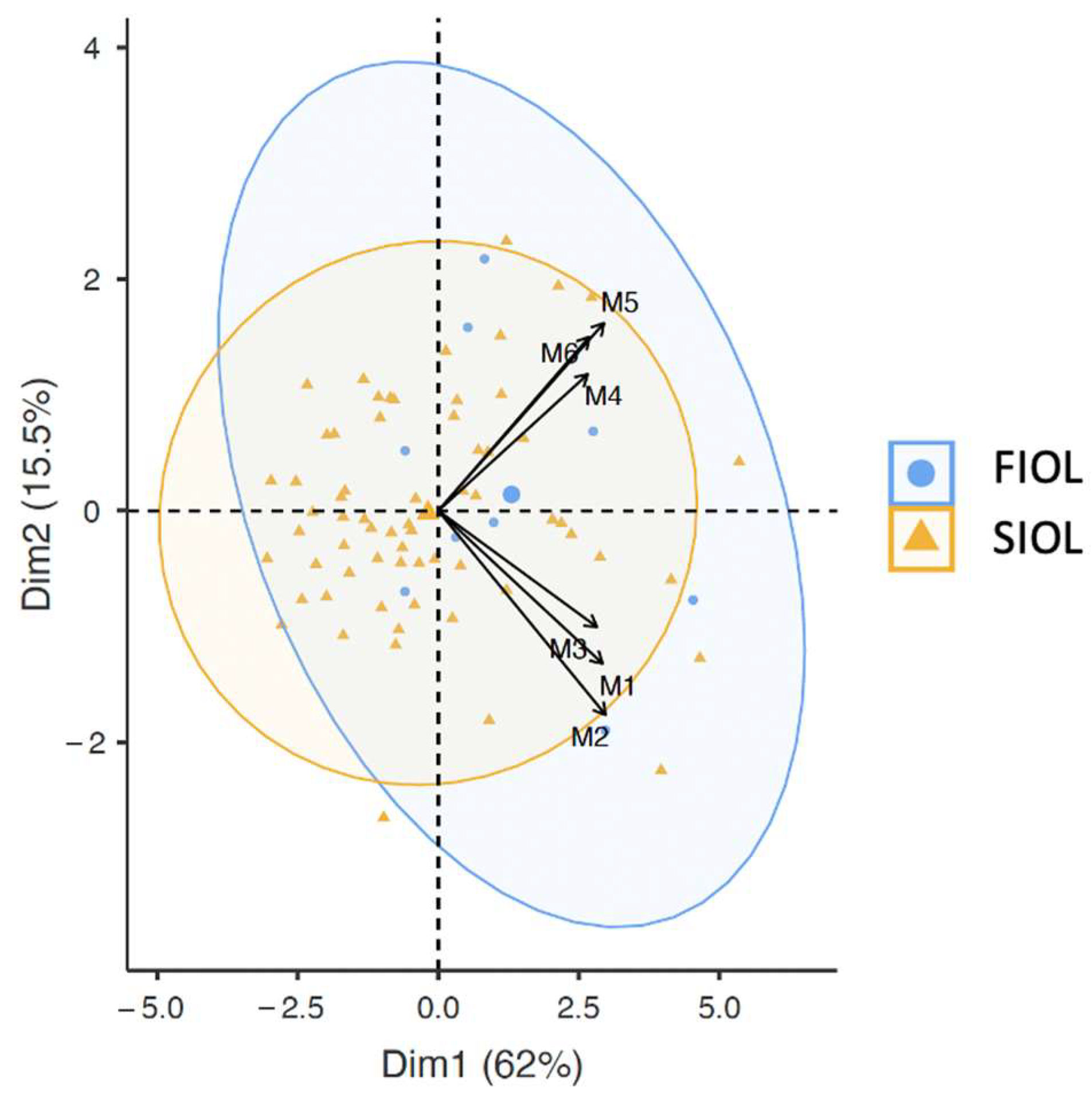
3.2. SWE Measurements
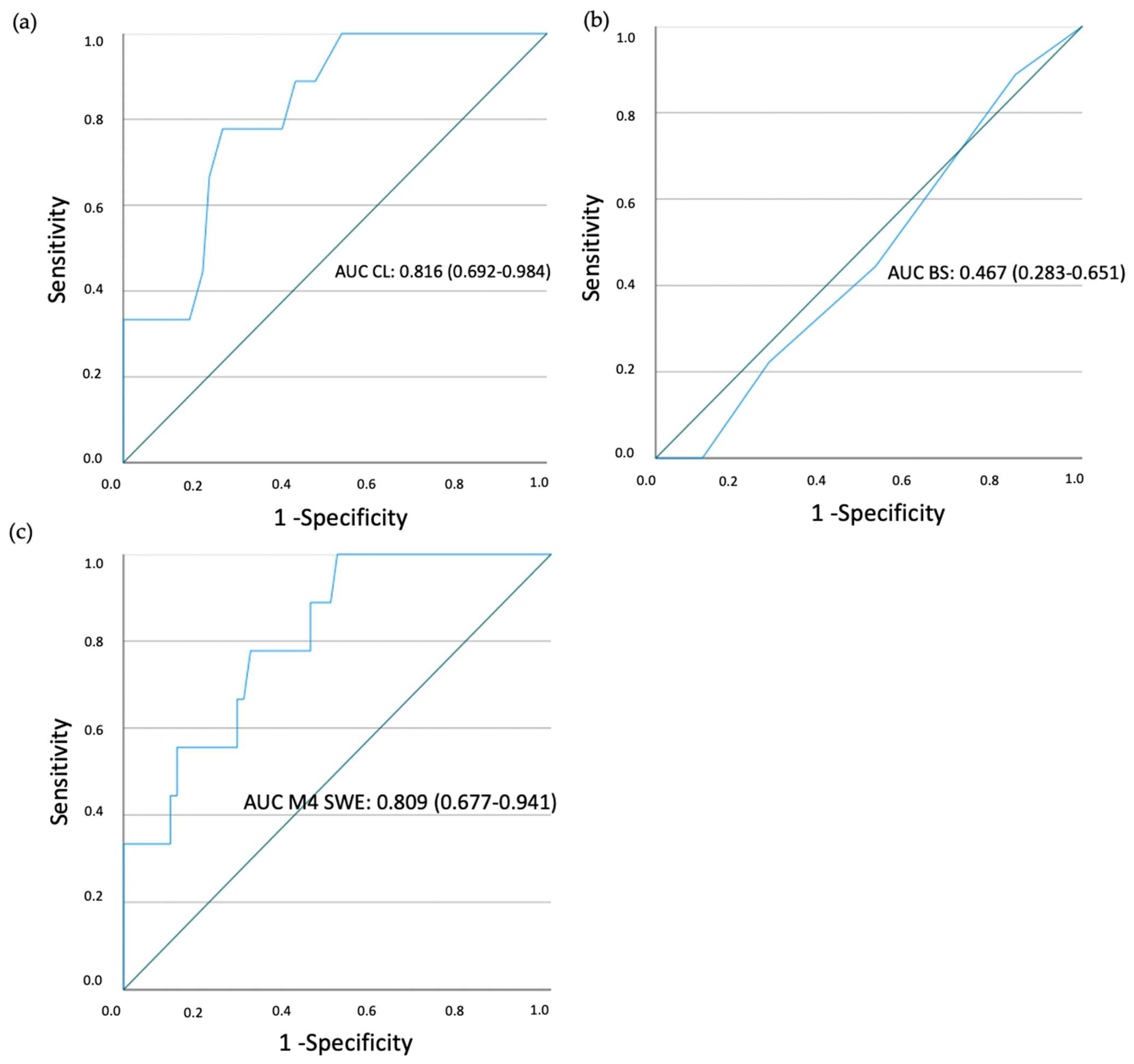
3.3. ROC Curves
3.4. Univariate and Multivariate Analysis
3.5. Correlation with Hours of Delivery
4. Discussion
5. Drawbacks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AC | Abdominal Circumference |
| AUC | Area Under Curve |
| BPD | Biparietal Diameter |
| BS | Bishop Score |
| CL | Cervical Length |
| CM | Centimeters |
| CPD | Cephalo Pelvic Disproportion |
| FIOL | Failure Induction of Labor |
| FTP | Failure to Progress |
| HC | Head Circumference |
| ICC | Intraclass Correlation Coefficient |
| IOL | Induction of Labor |
| Kpa | Kilopascals |
| RLFB | Risk of Loss Fetal well-Being |
| ROC | Receiver Operator Characteristics |
| ROI | Region of Interest |
| SIOL | Successful Induction of Labor |
| SWE | Shear Wave Elastography |
References
- Spanish Society of Obstetrics and Gynecology. Labor induction. Guideline. Prog. Obs. Ginecol. 2015, 58, 54–64. [Google Scholar]
- American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 107: Induction of labor. Obs. Gynecol. 2009, 114, 386–397. [Google Scholar] [CrossRef]
- Spanish Society of Obstetrics and Gynecology. Management post-term pregnancy. Guideline. Prog. Obs. Ginecol. 2011, 54, 38–49. [Google Scholar]
- ACOJ. Practice bulletin no. 146: Management of late-term and postterm pregnancies. Obs. Gynecol. 2014, 124, 390–396. [Google Scholar] [CrossRef]
- Gagnon, J.; Corlin, T.; Berghella, V.; Hoffman, M.K.; Sciscione, A.; Marie, P.S.; Schoen, C.N. Intracervical Foley catheter with and without oxytocin for labor induction with Bishop score ≤3: A secondary analysis. Am. J. Obs. Gynecol. MFM 2021, 3, 100350. [Google Scholar] [CrossRef]
- Leduc, D.; Biringer, A.; Lee, L.; Dy, J.; Corbett, T.; Duperron, L.; Clinical Practice Obstetrics Committee. Induction of Labour. J. Obs. Gynaecol. Can. 2013, 35, 840–857. [Google Scholar] [CrossRef] [PubMed]
- Mozurkewich, E.L.; Chilimigras, J.L.; Berman, D.R.; Perni, U.C.; Romero, V.C.; King, V.J.; Keeton, K.L. Methods of induction of labour: A systematic review. BMC Pregnancy Childbirth 2011, 11, 84. [Google Scholar] [CrossRef]
- Osmundson, S.; Ou-Yang, R.J.; Grobman, W.A. Elective induction compared with expectant management in nulliparous women with an unfavorable cervix. Obs. Gynecol. 2011, 117, 583. [Google Scholar] [CrossRef] [PubMed]
- Coates, R.; Cupples, G.; Scamell, A.; McCourt, C. Women’s experiences of induction of labour: Qualitative systematic review and thematic synthesis. Midwifery 2019, 69, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Friedman, E.A.; Niswander, K.R.; Bayonet-Rivera, N.P.; Sachtleben, M.R. Relation of prelabour evaluation to inducibility and the course of labour. Obs. Gynecol. 1966, 28, 495–501. [Google Scholar]
- Dhall, K.; Mittal, S.C.; Kumar, A. Evaluation of preinduction scoring systems. Aust. N. Z. J. Obs. Gynaecol. 1987, 27, 309–311. [Google Scholar] [CrossRef]
- Kolkman, D.G.E.; Verhoeven, C.J.M.; Brinkhorst, S.J.; Van Der Post, J.A.M.; Pajkrt, E.; Opmeer, B.C.; Mol, B.W.J. The Bishop score as a predictor of labor induction success: A systematic review. Am. J. Perinatol. 2013, 30, 625–630. [Google Scholar] [CrossRef]
- Laencina, A.M.G.; Sánchez, F.G.; Gimenez, J.H.; Martínez, M.S.; Martínez, J.A.V.; Vizcaíno, V.M. Comparison of ultrasonographic cervical length and the Bishop score in predicting successful labor induction. Acta Obs. Gynecol. Scand. 2007, 86, 799–804. [Google Scholar] [CrossRef]
- Verhoeven, C.J.M.; Opmeer, B.C.; Oei, S.G.; Latour, V.; Van Der Post, J.A.M.; Mol, B.W.J. Transvaginal sonographic assessment of cervical length and wedging for predicting outcome of labor induction at term: A systematic review and meta-analysis. Ultrasound Obs. Gynecol. 2013, 42, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Molina, F.S.; Gómez, L.F.; Florido, J.; Padilla, M.C.; Nicolaides, K.H. Quantification of cervical elastography: A reproducibility study. Ultrasound Obs. Gynecol. 2012, 39, 685–689. [Google Scholar] [CrossRef]
- Swiatkowska-Freund, M.; Preis, K. Elastography of the uterine cervix: Implications for success of induction of labor. Ultrasound Obs. Gynecol. 2011, 38, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Londero, A.P.; Schmitz, R.; Bertozzi, S.; Driul, L.; Fruscalzo, A. Diagnostic accuracy of cervical elastography in predicting labor induction success: A systematic review and meta-analysis. J. Perinat. Med. 2016, 44, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.S.; Sohn, I.S.; Kwon, H.S. Imaging analysis of cervical elastography for prediction of successful induction of labor at term. J. Ultrasound Med. 2013, 32, 937–946. [Google Scholar] [CrossRef]
- Muscatello, A.; Di Nicola, M.; Accurti, V.; Mastrocola, N.; Franchi, V.; Colagrande, I.; Carta, G. Sonoelastography as method for preliminary evaluation of uterine cervix to predict success of induction of labor. Fetal Diagn. Ther. 2014, 35, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Fruscalzo, A.; Londero, A.P.; Fröhlich, C.; Meyer-Wittkopf, M.; Schmitz, R. Quantitative Elastography of the Cervix for Predicting Labor Induction Success. Ultraschall der Medizin Eur. J. Ultrasound 2015, 36, 65–73. [Google Scholar] [CrossRef]
- Hee, L.; Rasmussen, C.K.; Schlütter, J.M.; Sandager, P.; Uldbjerg, N. Quantitative sonoelastography of the uterine cervix prior to induction of labor as a predictor of cervical dilation time. Acta Obs. Gynecol. Scand. 2014, 93, 684–690. [Google Scholar] [CrossRef]
- Wozniak, S.; Czuczwar, P.; Szkodziak, P.; Paszkowski, T. Usefulness of elastography in predicting the outcome of Foley catheter labour induction. Aust. N. Z. J. Obs. Gynaecol. 2015, 55, 245–250. [Google Scholar] [CrossRef]
- Pereira, S.; Frick, A.P.; Poon, L.C.; Zamprakou, A.; Nicolaides, K.H. Successful induction of labor: Prediction by preinduction cervical length, angle of progression and cervical elastography. Ultrasound Obs. Gynecol. 2014, 44, 468–475. [Google Scholar] [CrossRef]
- Hamza, A.; Radosa, J.; Gerlinger, C.; Solomayer, E.F.; Ströder, R.M.-S.G. Cervical and Lower Uterine Parameter Ultrasound and Elastographic Parameters for the Prediction of a Successful Induction of Labor. Ultraschall Med. 2021, 42, 520–528. [Google Scholar] [CrossRef]
- Doherty, J.R.; Trahey, G.E.; Nightingale, K.R.; Palmeri, M.L. Acoustic Radiation Force Elasticity Imaging in Diagnostic Ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2013, 60, 685–701. [Google Scholar] [CrossRef]
- Peralta, L.; Molina, F.S.; Melchor, J.; Gómez, L.F.; Massó, P.; Florido, J.; Rus, G. Transient Elastography to Assess the Cervical Ripening during Pregnancy: A Preliminary Study. Ultraschall Med. 2017, 38, 395–402. [Google Scholar] [CrossRef]
- Duan, H.; Chaemsaithong, P.; Ju, X.; Ho, S.Y.S.; Sun, Q.; Tai, Y.Y.; Poon, L.C. Shear-wave sonoelastographic assessment of cervix in pregnancy. Acta Obs. Gynecol. Scand. 2020, 99, 1458–1468. [Google Scholar] [CrossRef]
- Lu, J.; Cheng, Y.K.Y.; Ho, S.Y.S.; Sahota, D.S.; Hui, L.L.; Poon, L.C.; Leung, T.Y. The predictive value of cervical shear wave elastography in the outcome of labor induction. Acta Obs. Gynecol. Scand. 2020, 99, 59–68. [Google Scholar] [CrossRef]
- Fetal Medicine Foundation. Cervical Assesment. FMF Certification. Available online: https://fetalmedicine.org/fmf-certification-2/cervical-assessment-1 (accessed on 1 February 2020).
- Shiina, T.; Nightingale, K.R.; Palmeri, M.L.; Hall, T.J.; Bamber, J.C.; Barr, R.G.; Castera, L.; Choi, B.I.; Chou, Y.-H.; Cosgrove, D.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 1: Basic principles and terminology. Ultrasound Med. Biol. 2015, 41, 1126–1147. [Google Scholar] [CrossRef]
- O’Hara, S.; Zelesco, M.; Sun, Z. Shear Wave Elastography on the Uterine Cervix: Technical Development for the Transvaginal Approach. J. Ultrasound Med. 2019, 38, 1049–1060. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; Friedrich-Rust, M.; Gilja, O.H.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Liver Ultrasound Elastography, Update 2017 (Long Version). Ultraschall Med. 2017, 38, e16–e47. [Google Scholar]
- Thiele, M.; Detlefsen, S.; Sevelsted Møller, L.; Madsen, B.S.; Fuglsang Hansen, J.; Fialla, A.D.; Trebicka, J.; Krag, A. Transient and 2-Dimensional Shear-Wave Elastography Provide Comparable Assessment of Alcoholic Liver Fibrosis and Cirrhosis. Gastroenterology 2016, 150, 123–133. [Google Scholar] [CrossRef]
- Torres, J.; Muñoz, M.; Porcel, M.D.C.; Contreras, S.; Molina, F.S.; Rus, G.; Ocón-Hernández, O.; Melchor, J. Preliminary Results on the Preinduction Cervix Status by Shear Wave Elastography. Mathematics 2022, 10, 3164. [Google Scholar] [CrossRef]
- Carlson, C.; Romero, S.; Palmeri, M.; del Rio, A.M.; Esplin, S.M.; Rotemberg, V.M.; Hall, T.J.; Feltovich, H. Changes in Shear Wave Speed Pre and Post Induction of Labor: A Feasibility Study. Ultrasound Obs. Gynecol. 2015, 46, 93–98. [Google Scholar] [CrossRef]
- Hernández, S.; Peguero, A. Protocolo de maduración cervical e inducción de parto. Clin. Med. Fetal. Barc. 2013. Available online: https://portal.medicinafetalbarcelona.org/protocolos/es/obstetricia/induccion-del-parto.pdf (accessed on 31 January 2023).
- Ministerio De Sanidad y Política Social. Guía de Práctica Clínica sobre la Atención al Parto Normal Versión resumida; Guías de practica clínica en el SNS; Eusko Jaurlaritzaren Argitalpen Zerbitzu Nagusia: Urduliz, Spain, 2010; 173p. [Google Scholar]
- Yang, X.; Ding, Y.; Mei, J.; Xiong, W.; Wang, J.; Huang, Z.; Li, R. Second-Trimester Cervical Shear Wave Elastography Combined With Cervical Length for the Prediction of Spontaneous Preterm Birth. Ultrasound Med. Biol. 2022, 48, 820–829. [Google Scholar] [CrossRef]
- Peralta, L.; Mourier, E.; Richard, C.; Charpigny, G.; Larcher, T.; Aït-Belkacem, D.; Balla, N.K.; Brasselet, S.; Tanter, M.; Muller, M.; et al. In vivo evaluation of cervical stiffness evolution during induced ripening using Shear Wave Elastography, histology and 2 photon excitation microscopy: Insight from an animal model. PLoS ONE 2015, 10, e0133377. [Google Scholar] [CrossRef]
- Hernandez-Andrade, E.; Aurioles-Garibay, A.; Garcia, M.; Korzeniewski, S.J.; Schwartz, A.G.; Ahn, H.; Martinez-Varea, A.; Yeo, L.; Chaiworapongsa, T.; Hassan, S.S.; et al. Effect of depth on shear-wave elastography estimated in the internal and external cervical os during pregnancy. J. Perinat. Med. 2014, 42, 549–557. [Google Scholar] [CrossRef]
- Carlson, L.C.; Feltovich, H.; Palmeri, M.L.; Dahl, J.J.; Munoz Del Rio, A.; Hall, T.J. Estimation of shear wave speed in the human uterine cervix. Ultrasound Obs. Gynecol. 2014, 43, 452–458. [Google Scholar] [CrossRef]
- Nott, J.P.; Bonney, E.A.; Pickering, J.D.; Simpson, N.A.B. The structure and function of the cervix during pregnancy. Transl. Res. Anat. 2016, 2, 1–7. [Google Scholar] [CrossRef]
- Vink, J.Y.; Qin, S.; Brock, C.O.; Zork, N.M.; Feltovich, H.M.; Chen, X.; Urie, P.; Myers, K.M.; Hall, T.J.; Wapner, R. A new paradigm for the role of smooth muscle cells in the human cervix. Am. J. Obs. Gynecol. 2016, 215, 478.e1–478.e11. [Google Scholar] [CrossRef]
- Noelia, M.Z.; Myers, K.M.; Yoshida, M.K.; Cremers, S.; Jiang, H.; Ananth, C.V.; Wapner, R.J.; Kitajewski, J.; Vink, J. A Systematic Evaluation of Collagen Crosslinks in the Human Cervix. Physiol. Behav. 2016, 92, 135–140. [Google Scholar]
- Zhou, Y.; Jin, N.; Chen, Q.; Lv, M.; Jiang, Y.; Chen, Y.; Xi, F.; Yang, M.; Zhao, B.; Huang, H.; et al. Predictive value of cervical length by ultrasound and cervical strain elastography in labor induction at term. J. Int. Med. Res. 2021, 49, 300060520985338. [Google Scholar] [CrossRef] [PubMed]
- Fruscalzo, A.; Mazza, E.; Feltovich, H.; Schmitz, R. Cervical elastography during pregnancy: A critical review of current approaches with a focus on controversies and limitations. J. Med. Ultrason. 2016, 43, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Feltovich, H. Elastography applications in pregnancy. Tissue Elast. Imaging 2020, 1, 181–196. [Google Scholar]
- Palmeri, M.L.; Feltovich, H.; Homyk, A.; Carlson, L.C.; Hall, T.J. Evaluating the feasibility of acoustic radiation force impulse shear wave elasticity imaging of the uterine cervix with an intracavity array: A simulation study. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2013, 60, 2053–2064. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Maternal age (y) | 33 (18–44) |
| Maternal height (cm) | 164 (150–175) |
| BMI before pregnancy (kg/m2) | 24.13 (16.5–43.3) |
| BMI at delivery (kg/m2) | 28.82 (20.8–44.4) |
| Smokers | 7 (15.8%) |
| Reproduction techniques | 14 (19.2%) (In vitro 13, artificial insemination 1) |
| Cervical surgery or manipulation | 10 (13.7%) (9 curettages) |
| Prior cesarean section | 8 (10.9%) |
| Gestational age induction (wk) | 41.3 (41.0–41.5) |
| EFW in 3rd trimester (gr) | 2589 (2079–3253) |
| Birthweight (gr) | 3461 (2795–4405) |
| Newborn pH | 7.2 (6.47–7.36) |
| Characteristics | SIOL (n = 64) | FIOL (n = 9) | p |
|---|---|---|---|
| Maternal age (y) | 33 (30.20–36.0) | 31.8 (29.0–36.0) | 0.602 |
| Maternal height (cm) | 164 (161–170) | 163 (160–166) | 0.432 |
| BMI before pregnancy (kg/m2) | 23.95 (21.51–25.76) | 25.42 (21.03–27.21) | 0.657 |
| BMI at delivery (kg/m2) | 28.53 (25.56–31.12) | 30.90 (26.38–32.92) | 0.257 |
| EFW in 3rd trimester (gr) | 2578 (2411–1752) | 2667 (2442–2893) | 0.319 |
| Fetal percentile 3rd trimester | 40.88 (27.0–51.0) | 52.89 (37.50–68.50) | 0.077 |
| EFW prior delivery (gr) | 3573 (3295–3602) | 4033 (3683–4335) | 0.030 |
| Fetal percentile prior delivery | 33.0 (14.0–44.0) | 61.0 (37.50–83.50) | 0.020 |
| BPD (mm) | 94.11 (91.0–98.0) | 96.56 (92.20–101.0) | 0.152 |
| HC (mm) | 336.31 (326.25–347.0) | 348.0 (335.0–358.0) | 0.030 |
| AC (mm) | 347.73 (332.50–362.75) | 365.33 (349.0–384.50) | 0.010 |
| Bishop Score | 2.73 (1.0–3.75) | 2.11 (1.0–3.0) | 0.478 |
| Cervical length (mm) | 25.12 (20.0–32.0) | 42.33 (30.5–49.0) | 0.020 |
| SWE M1 (Kpa) | 8.86 (6.63–9.98) | 10.46 (7.75–13.77) | 0.347 |
| SWE M2 (Kpa) | 7.94 (6.21–8.73) | 9.72 (7.37–12.35) | 0.062 |
| SWE M3 (Kpa) | 7.45 (5.87–8.61) | 8.31 (6.65–9.82) | 0.273 |
| SWE Mean anterior lip (Kpa) | 8.08 (6.34–8.87) | 9.49 (7.10–11.94) | 0.113 |
| SWE M4 (Kpa) | 9.13 (6.98–11.16) | 13.91 (10.0–17.900) | 0.023 |
| SWE M5 (Kpa) | 8.92 (6.71–10.88) | 10.60 (9.05–12.25) | 0.052 |
| SWE M6 (Kpa) | 8.15 (6.38–9.86) | 8.75 (7.57–9.95) | 0.288 |
| SWE Mean posterior lip (Kpa) | 8.73 (6.86–10.49) | 11.09 (9.05–13.76) | 0.022 |
| Mean SWE inner | 9.01 (7.41–10.58) | 12.18 (9.16–15.18) | 0.071 |
| Mean SWE outer | 7.81 (6.41–8.69) | 8.53 (7.83–9.30) | 0.090 |
| Birthweight (gr) | 3443 (3211–3718) | 3590 (3160–3967) | 0.292 |
| Total hours of induction (h) | 21.77 (13.75–28.0) | 29.56 (25.50–32.50) | <0.001 |
| Cervical Region | Inner | Middle | Outer | Inner vs. Middle | Middle vs. Outer |
|---|---|---|---|---|---|
| Anterior cervical lip | 8.40 (7.15–10.30) | 7.75 (6.25–9.40) | 7.45 (5.95–8.85) | p < 0.01 | p 0.06 |
| Posterior cervical lip | 9.60 (7.40–11.85) | 8.65 (7.0–11.20) | 8.40 (6.65–10.10) | p 0.06 | p 0.01 |
| Variables | Correlation | p Value |
|---|---|---|
| M1 SWE | 0.166 | 0.160 |
| M2 SWE | 0.215 | 0.067 |
| M3 SWE | 0.128 | 0.276 |
| M4 SWE | 0.437 | 0.0001 |
| M5 SWE | 0.162 | 0.168 |
| M6 SWE | 0.088 | 0.457 |
| Mean SWE anterior lip | 0.192 | 0.1024 |
| Mean SWE posterior lip | 0.289 | 0.0130 |
| Mean SWE inner | 0.369 | 0.0012 |
| Mean SWE outer | 0.131 | 0.2701 |
| Measurement Method | AUC (95% IC) | Cutoff Value | Sensitivity | Specificity | PPV | NPV | LR+ | LR− |
|---|---|---|---|---|---|---|---|---|
| Bishop | 0.467 (0.283–0.651) | >1.5 | 44% | 48% | 11% | 86% | 0.84 | 1.16 |
| Cervical length | 0.816 (0.692–0.984) | >32.5 | 78% | 77% | 32% | 96% | 3.39 | 0.28 |
| M4 SWE | 0.809 (0.677–0.941) | >10.72 | 78% | 70% | 27% | 96% | 2.6 | 0.31 |
| Univariate Analysis | |||
|---|---|---|---|
| Variables | Odds Ratio | 95% IC | p Value |
| Maternal age | 1.06 | (0.933; 1.203) | 0.372 |
| Maternal height | 135.71 | (0.01; 2.032) | 0.428 |
| BMI before pregnancy | 0.937 | (0.818; 1.107) | 0.352 |
| BMI at delivery | 0.905 | (0.788; 1.038) | 0.154 |
| EFW in 3rd trimester | 0.999 | (0.996; 1.001) | 0.316 |
| Fetal percentile 3rd trimester | 0.969 | (0.935; 1.004) | 0.085 |
| EFW prior delivery | 0.997 | (0.995; 0.999) | 0.07 |
| Fetal percentile prior delivery | 0.959 | (0.959; 0.932) | 0.005 |
| BPD | 0.872 | (0.732; 1.038) | 0.124 |
| HC | 0.947 | (0.905; 0.992) | 0.020 |
| AC | 0.939 | (0.888; 0.993) | 0.028 |
| SME M1 | 0.875 | (0.724; 1.057) | 0.166 |
| SWE M2 | 0.821 | (0.821; 0.659) | 0.079 |
| SWEM3 | 0.840 | (0.615; 1.147) | 0.272 |
| SWE M4 | 0.701 | (0.553; 0.890) | 0.04 |
| SWE M5 | 0.877 | (0.726; 1.059) | 0.172 |
| SWE M6 | 0.889 | (0.654; 1.207) | 0.449 |
| SWE Mean anterior lip | 0.810 | (0.626; 1.048) | 0.109 |
| SWE Mean posterior lip | 0.724 | (0.552; 0.950) | 0.02 |
| Mean SWE inner | 0.693 | (0.536; 0.896) | 0.05 |
| Mean SWE outer | 0.814 | (0.566; 1.170) | 0.267 |
| Cervical Length | 0.867 | (0.782; 0.962) | 0.07 |
| Bishop Score | 1.151 | (0.642; 2.063) | 0.638 |
| Multivariate Analysis | |||
|---|---|---|---|
| Variables | Adjusted Odds Ratio | 95% IC | p Value |
| SWE M4 | 1.174 | (1.055–1.305) | 0.03 |
| Fetal percentile prior delivery | 0.997 | (0.975–1.020) | 0.803 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costas, T.; Rodríguez, M.d.l.O.; Sánchez-Barba, M.; Alcázar, J.L. Predictive Value of Cervical Shear Wave Elastography in the Induction of Labor in Late-Term Pregnancy Nulliparous Women: Preliminary Results. Diagnostics 2023, 13, 1782. https://doi.org/10.3390/diagnostics13101782
Costas T, Rodríguez MdlO, Sánchez-Barba M, Alcázar JL. Predictive Value of Cervical Shear Wave Elastography in the Induction of Labor in Late-Term Pregnancy Nulliparous Women: Preliminary Results. Diagnostics. 2023; 13(10):1782. https://doi.org/10.3390/diagnostics13101782
Chicago/Turabian StyleCostas, Tatiana, María de la O Rodríguez, Mercedes Sánchez-Barba, and Juan Luis Alcázar. 2023. "Predictive Value of Cervical Shear Wave Elastography in the Induction of Labor in Late-Term Pregnancy Nulliparous Women: Preliminary Results" Diagnostics 13, no. 10: 1782. https://doi.org/10.3390/diagnostics13101782