
Point-of-Care Thoracic Ultrasound in Children: New Advances in Pediatric Emergency Setting
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Examination Technique and Ultrasound Characteristics in Healthy Subjects
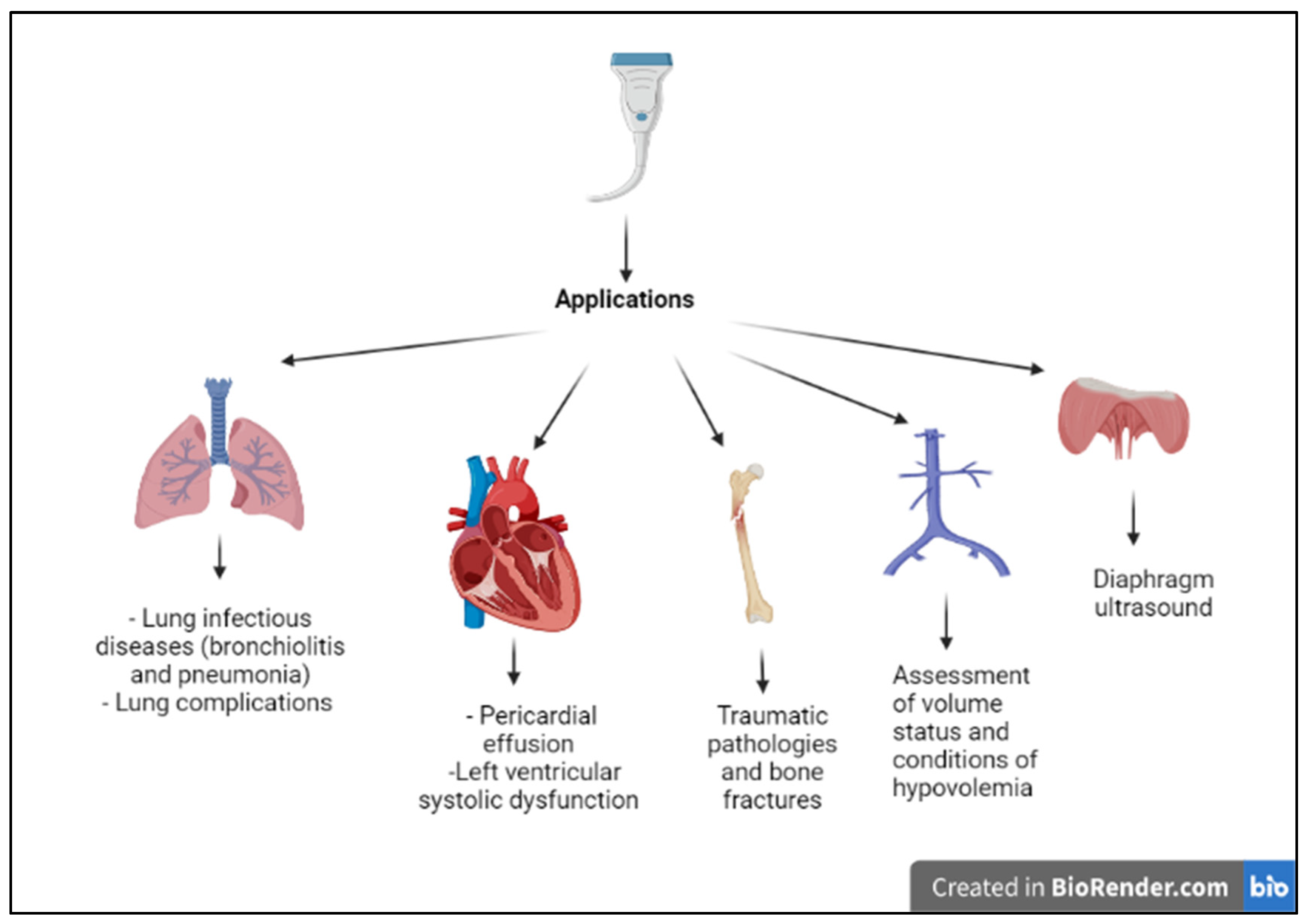
3. Applications of Point-of-Care Thoracic Ultrasound in Pediatric Emergency Department
4. Respiratory Diseases
4.1. Bronchiolitis
4.2. Pneumonia
4.3. Lung Abscess
4.4. Asthma
4.5. Pulmonary Edema
4.6. Pleural Pathologies and Complications of Pneumonia
5. Thoracic Ultrasound and Other Applications
5.1. Acute Heart Diseases
5.2. Assessment of Volume Status and Conditions of Hypovolemia
5.3. Traumatic Diseases and Early Detection of Signs of Child Abuse
5.4. Assessment of Drowning Victims
5.5. Diaphragm Ultrasound
5.6. Foreign Body Identification
6. Limitations of the Exam
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [PubMed]
- Bledsoe, A.; Zimmerman, J. Ultrasound: The New Stethoscope (Point-of-Care Ultrasound). Anesthesiol. Clin. 2021, 39, 537–553. [Google Scholar] [CrossRef] [PubMed]
- Iovine, E.; Nenna, R.; Bloise, S.; La Regina, D.P.; Pepino, D.; Petrarca, L.; Frassanito, A.; Lubrano, R.; Midulla, F. Lung Ultrasound: Its Findings and New Applications in Neonatology and Pediatric Diseases. Diagnostics 2021, 11, 652. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Choi, H. High-efficiency high-voltage class F amplifier for high-frequency wireless ultrasound systems. PLoS ONE 2021, 16, e0249034. [Google Scholar] [CrossRef] [PubMed]
- Copetti, R.; Cattarossi, L. Ultrasound diagnosis of pneumonia in children. Radiol. Med. 2008, 113, 190. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.E.; Parnell-Parmley, J.E.; Haidar, S.; Moineddin, R.; Charkot, E.; Bendavid, G.; Krajewski, C. Assessment of radiation dose awareness among pediatricians. Pediatr. Radiol. 2006, 36, 823–832. [Google Scholar] [CrossRef]
- Narula, J.; Chandrashekhar, Y.; Braunwald, E. Time to Add a Fifth Pillar to Bedside Physical Examination: Inspection, Palpation, Percussion, Auscultation, and Insonation. JAMA Cardiol. 2018, 3, 346–350. [Google Scholar] [CrossRef]
- La Regina, D.P.; Bloise, S.; Pepino, D.; Iovine, E.; Laudisa, M.; Cristiani, L.; Nicolai, A.; Nenna, R.; Mancino, E.; Di Mattia, G.; et al. Lung ultrasound in bronchiolitis. Pediatr. Pulmonol. 2021, 56, 234–239. [Google Scholar] [CrossRef]
- Buonsenso, D.; Musolino, A.M.; Gatto, A.; Lazzareschi, I.; Curatola, A.; Valentini, P. Lung ultrasound in infants with bronchiolitis. BMC Pulm. Med. 2019, 19, 159. [Google Scholar] [CrossRef]
- Supino, M.C.; Buonsenso, D.; Scateni, S.; Scialanga, B.; Mesturino, M.A.; Bock, C.; Chiaretti, A.; Giglioni, E.; Reale, A.; Musolino, A.M. Point-of-care lung ultrasound in infants with bronchiolitis in the pediatric emergency department: A prospective study. Eur. J. Pediatr. 2019, 178, 623–632. [Google Scholar] [CrossRef]
- San Sebastian Ruiz, N.; Rodríguez Albarrán, I.; Gorostiza, I.; Galletebeitia Laka, I.; Delgado Lejonagoitia, C.; Samson, F. Point-of-care lung ultrasound in children with bronchiolitis in a pediatric emergency department. Arch Pediatr. 2021, 28, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Bobillo-Perez, S.; Sorribes, C.; Gebellí, P.; Lledó, N.; Castilla, M.; Ramon, M.; Rodriguez-Fanjul, J. Lung ultrasound to predict pediatric intensive care admission in infants with bronchiolitis (LUSBRO study). Eur. J. Pediatr. 2021, 180, 2065–2072. [Google Scholar] [CrossRef] [PubMed]
- Bueno-Campaña, M.; Sainz, T.; Alba, M.; Del Rosal, T.; Mendez-Echevarría, A.; Echevarria, R.; Tagarro, A.; Ruperez-Lucas, M.; Herrreros, M.L.; Latorre, L.; et al. Lung ultrasound for prediction of respiratory support in infants with acute bronchiolitis: A cohort study. Pediatr. Pulmonol. 2019, 54, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Taveira, M.; Yousef, N.; Miatello, J.; Roy, C.; Claude, C.; Boutillier, B.; Dubois, C.; Pierre, A.F.; Tissières, P.; Durand, P. Can a simple lung ultrasound score predict length of ventilation for infants with severe acute viral bronchiolitis? Arch. Pediatr. 2018, 25, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Biagi, C.; Pierantoni, L.; Baldazzi, M.; Greco, L.; Dormi, A.; Dondi, A.; Faldella, G.; Lanari, M. Lung ultrasound for the diagnosis of pneumonia in children with acute bronchiolitis. BMC Pulm. Med. 2018, 18, 191. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Clark, J.; Coote, N.; Fletcher, P.; Harnden, A.; Mckean, M.; Thomson, A.; on behalf of the British Thoracic Society. Standards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in children: Update 2011. Thorax 2011, 66 (Suppl. S2), ii1–ii23. [Google Scholar] [CrossRef]
- Bradley, J.S.; Byington, C.L.; Shah, S.S. The management of community-acquired pneumonia ininfants and children older than 3 months of age: Clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin. Infect. Dis. 2011, 53, 617–630. [Google Scholar] [CrossRef]
- Yan, J.H.; Yu, N.; Wang, Y.H.; Gao, Y.B.; Pan, L. Lung ultrasound vs. chest radiography in the diagnosis of children pneumonia: Systematic evidence. Medicine 2020, 99, e23671. [Google Scholar] [CrossRef]
- Stadler, J.A.M.; Andronikou, S.; Zar, H.J. Lung ultrasound for the diagnosis of community-acquired pneumonia in children. Pediatr. Radiol. 2017, 47, 1412–1419. [Google Scholar] [CrossRef]
- Pereda, M.A.; Chavez, M.A.; Hooper-Miele, C.C.; Gilman, R.H.; Steinhoff, M.C.; Ellington, L.E.; Gross, M.; Price, C.; Tielsch, J.M.; Checkley, W. Lung ultrasound for the diagnosis of pneumonia in children: A meta-analysis. Pediatrics 2015, 135, 714–722. [Google Scholar] [CrossRef]
- Balk, D.S.; Lee, C.; Schafer, J.; Welwarth, J.; Hardin, J.; Novack, V.; Yarza, S.; Hoffmann, B. Lung ultrasound compared to chest-X-ray for diagnosis of pediatric pneumonia: A meta-analysis. Pediatr. Pulmonol. 2018, 53, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Jaworska, J.; Komorowska-Piotrowska, A.; Pomiećko, A.; Wiśniewski, J.; Woźniak, M.; Littwin, B.; Kryger, M.; Kwaśniewicz, P.; Szczyrski, J.; Kulińska-Szukalska, K.; et al. Consensus on the Application of Lung Ultrasound in Pneumonia and Bronchiolitis in Children. Diagnostics 2020, 10, 935. [Google Scholar] [CrossRef] [PubMed]
- Principi, N.; Esposito, A.; Giannitto, C.; Esposito, S. Lung ultrasonography to diagnose community-acquired pneumonia in children. BMC Pulm. Med. 2017, 17, 212. [Google Scholar] [CrossRef] [PubMed]
- Bloise, S.; La Regina, D.P.; Pepino, D.; Iovine, E.; Laudisa, M.; Di Mattia, G.; Nicolai, A.; Nenna, R.; Petrarca, L.; Mancino, E.; et al. Lung ultrasound compared to chest X-ray for the diagnosis of CAP in children. Pediatr. Int. 2021, 63, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Iorio, G.; Capasso, M.; Prisco, S.; De Luca, G.; Mancusi, C.; Laganà, B.; Piscopo, M.A.; Comune, V. Lung Ultrasound Findings Undetectable by Chest Radiography in Children with Community-Acquired Pneumonia. Ultrasound Med. Biol. 2018, 44, 1687–1693. [Google Scholar] [CrossRef] [PubMed]
- Long, L.; Zhao, H.T.; Zhang, Z.Y.; Wang, G.Y.; Zhao, H.L. Lung ultrasound for the diagnosis of pneumonia in adults: A meta-analysis. Medicine 2017, 96, e5713. [Google Scholar] [CrossRef] [PubMed]
- Staub, L.J.; Biscaro, R.R.M.; Maurici, R. Accuracy and Applications of Lung Ultrasound to Diagnose Ventilator-Associated Pneumonia: A Systematic Review. J. Intensive Care Med. 2018, 33, 447–455. [Google Scholar] [CrossRef]
- Adler, A.C.; von Ungern-Sternberg, B.S.; Matava, C.T. Lung ultrasound and atelectasis-The devil is in the details. Paediatr. Anaesth. 2021, 31, 1269–1270. [Google Scholar] [CrossRef]
- Blancas Gómez-Casero, R.; Alonso Fernández, M.Á.; Ballesteros Ortega, D.; Martínez González, Ó. Subpleural artifact in lung pulse evidenced by M-mode ultrasound in a patient with atelectasis. Rev. Esp. Anestesiol. Reanim. 2016, 63, 127. [Google Scholar] [CrossRef]
- Montero-Yéboles, R.; Arroyo-Marin, M.J.; Jaraba-Caballero, S.; Gómez-Guzman, E.; Frías-Pérez, M.; Ruiz-Sáez, B.; Pérez-Navero, J.L. A pleural ultrasound image of a collapsed lung surrounded by pleural fluid (“jellyfish sign”) may correspond to an intrapericardial mass. J. Ultrasound 2022, 25, 387–390. [Google Scholar] [CrossRef]
- Haaksma, M.E.; Smit, J.M.; Heldeweg, M.L.A.; Nooitgedacht, J.S.; de Grooth, H.J.; Jonkman, A.H.; Girbes, A.R.J.; Heunks, L.; Tuinman, P.R. Extended Lung Ultrasound to Differentiate Between Pneumonia and Atelectasis in Critically Ill Patients: A Diagnostic Accuracy Study. Crit. Care Med. 2022, 50, 750–759. [Google Scholar] [CrossRef] [PubMed]
- Ullmann, N.; D’Andrea, M.L.; Gioachin, A.; Papia, B.; Testa, M.B.C.; Cherchi, C.; Bock, C.; Tomà, P.; Cutrera, R. Lung ultrasound: A useful additional tool in clinician’s hands to identify pulmonary atelectasis in children with neuromuscular disease. Pediatr. Pulmonol. 2020, 55, 1490–1494. [Google Scholar] [CrossRef] [PubMed]
- Lubrano, R.; Villani, A.; Berrettini, S.; Caione, P.; Chiara, A.; Costantino, A.; Formigari, R.; Franzoni, E.; Gattinara, G.C.; Giustardi, A.; et al. Point of view of the Italians pediatric scientific societies about the pediatric care during the COVID-19 lockdown: What has changed and future prospects for restarting. Ital. J. Pediatr. 2020, 46, 142. [Google Scholar] [CrossRef] [PubMed]
- Bloise, S.; Marcellino, A.; Testa, A.; Dilillo, A.; Mallardo, S.; Isoldi, S.; Martucci, V.; Sanseviero, M.T.; Del Giudice, E.; Iorfida, D.; et al. Serum IgG levels in children 6 months after SARS-CoV-2 infection and comparison with adults. Eur. J. Pediatr. 2021, 180, 3335–3342. [Google Scholar] [CrossRef]
- Isoldi, S.; Mallardo, S.; Marcellino, A.; Bloise, S.; Dilillo, A.; Iorfida, D.; Testa, A.; Del Giudice, E.; Martucci, V.; Sanseviero, M.; et al. The comprehensive clinic, laboratory, and instrumental evaluation of children with COVID-19: A 6-months prospective study. J. Med. Virol. 2021, 93, 3122–3132. [Google Scholar] [CrossRef]
- Musolino, A.M.; Supino, M.C.; Buonsenso, D.; Ferro, V.; Valentini, P.; Magistrelli, A.; Lombardi, M.H.; Romani, L.; D’Argenio, P.; Campana, A. Roman Lung Ultrasound Study Team for Pediatric COVID-19 (ROMULUS COVID Team). Lung Ultrasound in Children with COVID-19: Preliminary Findings. Ultrasound Med. Biol. 2020, 46, 2094–2098. [Google Scholar] [CrossRef]
- Musolino, A.M.; Supino, M.C.; Buonsenso, D.; Papa, R.E.; Chiurchiù, S.; Magistrelli, A.; Barbieri, M.A.; Raponi, M.; D’Argenio, P.; Villani, A.; et al. Lung ultrasound in the diagnosis and monitoring of 30 children with coronavirus disease 2019. Pediatric. Pulmonol. 2021, 6, 1045–1052. [Google Scholar] [CrossRef]
- Musolino, A.M.; Boccuzzi, E.; Supino, M.C.; Scialanga, B.; De Sanctis, F.; Buonsenso, D.; Sinibaldi, S.; Tomà, P. Point-of-care lung ultrasound in the diagnosis and monitoring of paediatric patients with spontaneous pneumothorax in SARS-CoV-2 infection. J. Paediatr. Child Health. 2021, 57, 604–606. [Google Scholar] [CrossRef]
- Norbedo, S.; Blaivas, M.; Raffaldi, I.; Caroselli, C. Lung Ultrasound Point-of-View in Pediatric and Adult COVID-19 Infection. J. Ultrasound Med. 2020, 7, 899–908. [Google Scholar] [CrossRef]
- Denina, M.; Pruccoli, G.; Scolfaro, C.; Mignone, F.; Zoppo, M.; Giraudo, I.; Silvestro, E.; Bertolotti, L.; Rosati, S.; Ramenghi, U.; et al. Sequelae of COVID-19 in Hospitalized Children: A 4-Months Follow-Up. Pediatr. Infect. Dis. J. 2020, 39, e458–e459. [Google Scholar] [CrossRef]
- Kraft, C.; Lasure, B.; Sharon, M.; Patel, P.; Minardi, J. Pediatric Lung Abscess: Immediate Diagnosis by Point-of-Care Ultrasound. Pediatr. Emerg. Care 2018, 34, 447–449. [Google Scholar] [CrossRef] [PubMed]
- Saoud, M.; Patil, M.; Singh Dhillon, S.; Alraiyes, A.H.; Sunar, U.; Harris, K. Image Characteristics of Lung Abscess by Convex-Probe Endobronchial Ultrasound. J. Bronchol. Interv. Pulmonol. 2017, 24, 34–35. [Google Scholar] [CrossRef] [PubMed]
- Marzook, N.; Gagnon, F.; Deragon, A.; Zielinski, D.; Shapiro, A.J.; Lands, L.C.; Dubrovsky, A.S. Lung ultrasound findings in asymptomatic healthy children with asthma. Pediatr. Pulmonol. 2022, 57, 2474–2480. [Google Scholar] [CrossRef] [PubMed]
- Dankoff, S.; Li, P.; Shapiro, A.J.; Varshney, T.; Dubrovsky, A.S. Point of care lung ultrasound of children with acute asthma exacerbations in the pediatric ED. Am. J. Emerg. Med. 2017, 35, 615–622. [Google Scholar] [CrossRef]
- Blanco, P.A.; Cianciulli, T.F. Pulmonary Edema Assessed by Ultrasound: Impact in Cardiology and Intensive Care Practice. Echocardiography 2016, 33, 778–787. [Google Scholar] [CrossRef]
- Gargani, L.; Frassi, F.; Soldati, G.; Tesorio, P.; Gheorghiade, M.; Picano, E. Ultrasound lung comets for the differential diagnosis of acute cardiogenic dyspnoea: A comparison with natriuretic peptides. Eur. J. Heart Fail. 2008, 10, 70–77. [Google Scholar] [CrossRef]
- Vitturi, N.; Soattin, M.; Allemand, E.; Simoni, F.; Realdi, G. Thoracic ultrasonography: A new method for the work-up of patients with dyspnea. J. Ultrasound 2011, 14, 147–151. [Google Scholar] [CrossRef]
- Volpicelli, G.; Mussa, A.; Garofalo, G.; Cardinale, L.; Casoli, G.; Perotto, F.; Fava, C.; Frascisco, M. Bedside lung ultrasound in the assessment of alveolar-interstitial syndrome. Am. J. Emerg. Med. 2006, 24, 689–696. [Google Scholar] [CrossRef]
- Picano, E.; Frassi, F.; Agricola, E.; Gligorova, S.; Gargani, L.; Mottola, G. Ultrasound lung comets: A clinically useful sign of extravascular lung water. J. Am. Soc. Echocardiogr. 2006, 19, 356–363. [Google Scholar] [CrossRef]
- Picano, E.; Pellikka, P. Ultrasound of extravascular lung water: A new standard for pulmonary congestion. Eur. Heart J. 2016, 37, 2097–2104. [Google Scholar] [CrossRef]
- Singh, A.K.; Mayo, P.H.; Koenig, S.; Talwar, A.; Narasimhan, M. The Use of M-Mode Ultrasonography to Differentiate the Causes of B Lines. Chest 2018, 153, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Brixey, A.G.; Luo, Y.; Skouras, V.; Awdankiewicz, A.; Light, R.W. The efficacy of chest radiographs in detecting parapneumonic effusions. Respirology 2011, 16, 1000–1004. [Google Scholar] [CrossRef] [PubMed]
- Grimberg, A.; Shigueoka, D.; Atallah, A.N.; Ajzen, S.; Iared, W. Diagnostic accuracy of sonography for pleural effusion: Systematic review. Sao Paulo Med. J. 2010, 128, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Soni, N.J.; Franco, R.; Velez, M.I.; Schnobrich, D.; Dancel, R.; Restrepo, M.I.; Mayo, P.H. Ultrasound in the diagnosis and management of pleural effusions. J. Hosp. Med. 2015, 10, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Prina, E.; Torres, A.; Carvalho, C. Lung ultrasound in the evaluation of pleural effusion. J. Bras. Pneumol. 2014, 40, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Brogi, E.; Gargani, L.; Bignami, E.; Barbariol, F.; Marra, A.; Forfori, F.; Vetrugno, L. Thoracic ultrasound for pleural effusion in the intensive care unit: A narrative review from diagnosis to treatment. Crit. Care 2017, 21, 325. [Google Scholar] [CrossRef]
- Kalokairinou-Motogna, M.; Maratou, K.; Paianid, I.; Soldatos, T.; Antipa, E.; Tsikkini, A.; Baltas, C.S. Application of color Doppler ultrasound in the study of small pleural effusion. Med. Ultrason. 2010, 12, 12–16. [Google Scholar]
- Yang, P.C.; Luh, K.T.; Chang, D.B.; Wu, H.D.; Yu, C.J.; Kuo, S.H. Value of sonography in determining the nature of pleural effusion: Analysis of 320 cases. AJR. Am. J. Roentgenol. 1992, 159, 29–33. [Google Scholar] [CrossRef]
- Diacon, A.H.; Brutsche, M.H.; Solèr, M. Accuracy of pleural puncture sites: A prospective comparison of clinical examination with ultrasound. Chest 2003, 123, 436–441. [Google Scholar] [CrossRef]
- Gordon, C.E.; Feller-Kopman, D.; Balk, E.M.; Smetana, G.W. Pneumothorax following thoracentesis: A systematic review and meta-analysis. Arch. Intern. Med. 2010, 170, 332–339. [Google Scholar] [CrossRef]
- Lichtenstein, D.; Mezière, G.; Biderman, P.; Gepner, A. The "lung point": An ultrasound sign specific to pneumothorax. Intensiv. Care Med. 2000, 26, 1434–1440. [Google Scholar] [CrossRef]
- Bhoil, R.; Ahluwalia, A.; Chopra, R.; Surya, M.; Bhoil, S. Signs and lines in lung ultrasound. J. Ultrason. 2021, 21, e225–e233. [Google Scholar] [CrossRef] [PubMed]
- Dahmarde, H.; Parooie, F.; Salarzaei, M. Accuracy of Ultrasound in Diagnosis of Pneumothorax: A Comparison between Neonates and Adults-A Systematic Review and Meta-Analysis. Can. Respir. J. 2019, 2019, 5271982. [Google Scholar] [CrossRef] [PubMed]
- Fei, Q.; Lin, Y.; Yuan, T.M. Lung Ultrasound, a Better Choice for Neonatal Pneumothorax: A Systematic Review and Meta-analysis. Ultrasound Med. Biol. 2021, 47, 359–369. [Google Scholar] [CrossRef]
- Chan, K.K.; Joo, D.A.; McRae, A.D.; Takwoingi, Y.; Premji, Z.A.; Lang, E.; Wakai, A. Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department. Cochrane Database Syst. Rev. 2020, 7, CD013031. [Google Scholar] [CrossRef]
- Cattarossi, L.; Copetti, R.; Brusa, G.; Pintaldi, S. Lung Ultrasound Diagnostic Accuracy in Neonatal Pneumothorax. Can. Respir. J. 2016, 2016, 6515069. [Google Scholar] [CrossRef] [PubMed]
- Addala, D.N.; Bedawi, E.O.; Rahman, N.M. Parapneumonic Effusion and Empyema. Clin. Chest Med. 2021, 42, 637–647. [Google Scholar] [CrossRef]
- Lin, F.; Chou, C.; Chang, S. Differentiating pyopneumothorax and peripheral lung abscess: Chest ultrasonography. Am. J. Med. Sci. 2004, 327, 330–335. [Google Scholar] [CrossRef]
- Calder, A.; Owens, C.M. Imaging of parapneumonic pleural effusions and empyema in children. Pediatr. Radiol. 2009, 39, 527–537. [Google Scholar] [CrossRef]
- Svigals, P.; Chopra, A.; Ravenel, J.; Nietert, P.J.; Huggins, J.T. The accuracy of pleural ultrasonography in diagnosing complicated parapneumonic pleural effusions. Thorax 2017, 72, 94–95. [Google Scholar] [CrossRef]
- Chen, H.J.; Yu, Y.H.; Tu, C.Y.; Chen, C.H.; Hsia, T.C.; Tsai, K.D.; Shih, C.M.; Hsu, W.H. Ultrasound in peripheral pulmonary air-fluid lesions. Color Doppler imaging as an aid in differentiating empyema and abscess. Chest 2009, 135, 1426–1432. [Google Scholar] [CrossRef] [PubMed]
- Elyashiv, D.; Alpert, E.A.; Granat, N. Empyema Necessitans Diagnosed by Point-of-Care Ultrasound. J. Emerg. Med. 2020, 59, e221–e223. [Google Scholar] [CrossRef] [PubMed]
- Alerhand, S.; Choi, A.; Varga, P. Cardiac Ultrasound for Pediatric Emergencies. Pediatr. Ann. 2021, 50, e424–e431. [Google Scholar] [CrossRef] [PubMed]
- Hamad, A.; Ng, C.; Alade, K.; D’Amico, B.; Morales-Perez, L.; Price, J.; Leung, S.K. Diagnosing Acute Heart Failure in the Pediatric Emergency Department Using Point-of-Care Ultrasound. J. Emerg. Med. 2021, 61, e18–e25. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.F.; Arichai, P.; Gravel, C.A.; Vieira, R.L.; Neal, J.T.; Neuman, M.I.; Monuteaux, M.C.; Levy, J.A. Use of Cardiac Point-of-Care Ultrasound in the Pediatric Emergency Department. Pediatr. Emerg. Care. 2022, 38, e300–e305. [Google Scholar] [CrossRef]
- Klugman, D.; Berger, J.T. Echocardiography and Focused Cardiac Ultrasound. Pediatr. Crit. Care Med. 2016, 17 (Suppl. S1), S222–S224. [Google Scholar] [CrossRef]
- Yıldızdaş, D.; Aslan, N. A new stethoscope for pediatric intensivists: Point-of-care ultrasound. Turk. Arch. Pediatr. 2020, 55, 345–353. [Google Scholar] [CrossRef]
- Nelson, B.P.; Sanghvi, A. Point-of-Care Cardiac Ultrasound: Feasibility of Performance by Noncardiologists. Glob. Heart. 2013, 8, 293–297. [Google Scholar] [CrossRef]
- Adler, A.C.; Matisoff, A.J.; DiNardo, J.A.; Miller-Hance, W.C. Point-of-care ultrasound in pediatric anesthesia: Perioperative considerations. Curr. Opin. Anaesthesiol. 2020, 33, 343–353. [Google Scholar] [CrossRef]
- Leviter, J.I.; Walsh, S.; Riera, A. Point-of-Care Ultrasound for Pulse Checks in Pediatric Cardiac Arrest: Two Illustrative Cases. Pediatr. Emerg. Care 2022, 39, 60–61. [Google Scholar] [CrossRef]
- Doniger, S.J.; Ng, N. Cardiac point-of-care ultrasound reveals unexpected, life-threatening findings in two children. Ultrasound J. 2020, 12, 4. [Google Scholar] [CrossRef] [PubMed]
- Song, I.; Kim, E.; Lee, J.; Kang, P.; Kim, H.S.; Kim, J.T. Utility of perioperative lung ultrasound in pediatric cardiac surgery: A randomized controlled trial. Anesthesiology 2018, 128, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Townsley, M. Lung Ultrasound in Pediatric Cardiac Surgery: A Complementary Tool for Predicting and Identifying Postoperative Pulmonary Complications. J. Cardiothorac. Vasc. Anesth. 2020, 35, 1369–1370. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, F.; Migliaro, F.; Sodano, A.; Umbaldo, A.; Romano, A.; Vallone, G.; Capasso, L. Can neonatal ultrasound monitor fluid clearence and preditc the need of respiratory support? Crit. Care 2012, 16, 220. [Google Scholar] [CrossRef] [PubMed]
- Delmonaco, A.G.; Carpino, A.; Raffaldi, I.; Pruccoli, G.; Garrone, E.; Del Monte, F.; Riboldi, L.; Licciardi, F.; Urbino, A.F.; Parodi, E. First diagnosis of multisystem inflammatory syndrome in children (MIS-C): An analysis of PoCUS findings in the ED. Ultrasound J. 2021, 13, 41. [Google Scholar] [CrossRef]
- Chen, L.; Kim, Y.; Santucci, K.A. Use of ultrasound measurement of the inferior vena cava diameter as an objective tool in the assessment of children with clinical dehydration. Acad. Emerg. Med. 2007, 14, 841–845. [Google Scholar] [CrossRef]
- Levine, A.C.; Shah, S.P.; Umulisa, I.; Munyaneza, R.B.; Dushimiyimana, J.M.; Stegmann, K.; Musavuli, J.; Ngabitsinze, P.; Stulac, S.; Epino, H.M.; et al. Ultrasound assessment of severe dehydration in children with diarrhea and vomiting. Acad. Emerg. Med. 2010, 17, 1035–1041. [Google Scholar] [CrossRef]
- Zengin, S.; Al, B.; Genc, S.; Yildirim, C.; Ercan, S.; Dogan, M.; Altunbas, G. Role of inferior vena cava and right ventricular diameter in assessment of volume status: A comparative study: Ultrasound and hypovolemia. Am. J. Emerg. Med. 2013, 31, 763–767. [Google Scholar] [CrossRef]
- Zhang, X.; Luan, H.; Zhu, P.; Feng, J.; Cui, J.; Zhao, Z. Does ultrasonographic measurement of the inferior vena cava diameter correlate with central venous pressure in the assessment of intravascular volume in patients undergoing gastrointestinal surgery? J. Surg. Res. 2014, 191, 339–343. [Google Scholar] [CrossRef]
- Loomba, R.S.; Villarreal, E.G.; Farias, J.S.; Flores, S.; Bronicki, R.A. Fluid bolus administration in children, who responds and how? A systematic review and meta-analysis. Paediatr. Anaesth. 2022, 32, 993–999. [Google Scholar] [CrossRef]
- Levitov, A.; Marik, P.E. Echocardiographic assessment of preload responsiveness in critically ill patients. Cardiol. Res. Pract. 2012, 2012, 819696. [Google Scholar] [CrossRef] [PubMed]
- Jalil, B.A.; Cavallazzi, R. Predicting fluid responsiveness: A review of literature and a guide for the clinician. Am. J. Emerg. Med. 2018, 36, 2093–2102. [Google Scholar] [CrossRef]
- Conlon, T.W.; Nishisaki, A.; Singh, Y.; Bhombal, S.; De Luca, D.; Kessler, D.O.; Su, E.R.; Chen, A.E.; Fraga, M.V. Moving Beyond the Stethoscope: Diagnostic Point-of-Care Ultrasound in Pediatric Practice. Pediatrics 2019, 144, e20191402. [Google Scholar] [CrossRef] [PubMed]
- Costantino, T.G.; Parikh, A.K.; Satz, W.A.; Fojtik, J.P. Ultrasonography-guided peripheral intravenous access versus traditional approaches in patients with difficult intravenous access. Ann. Emerg. Med. 2005, 46, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Vinograd, A.M.; Zorc, J.J.; Dean, A.J.; Abbadessa, M.K.F.; Chen, A.E. First-Attempt Success, Longevity, and Complication Rates of Ultrasound-Guided Peripheral Intravenous Catheters in Children. Pediatr. Emerg. Care 2018, 34, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Ravikanth, R. Diagnostic Accuracy and Prognostic Significance of Point-Of-Care Ultrasound (POCUS) for Traumatic Cervical Spine in Emergency care setting: A Comparison of clinical outcomes between POCUS and Computed Tomography on a Cohort of 284 Cases and Review of Literature. J. Craniovertebral Junction Spine 2021, 12, 257–262. [Google Scholar]
- Wongwaisayawan, S.; Suwannanon, R.; Prachanukool, T.; Sricharoen, P.; Saksobhavivat, N.; Kaewlai, R. Trauma Ultrasound. Ultrasound Med. Biol. 2015, 41, 2543–2561. [Google Scholar] [CrossRef]
- Flato, U.; Guimarães, H.; Lopes, R.D.; Valiatti, J.L.; Flato, E.M.; Lorenzo, R.G. Usefulness of Extended-FAST (EFAST-Extended Focused Assessment with Sonography for Trauma in critical care setting. Rev. Bras. De Ter. Intensive 2010, 22, 291–299. [Google Scholar] [CrossRef]
- Stengel, D.; Leisterer, J.; Ferrada, P.; Ekkernkamp, A.; Mutze, S.; Hoenning, A. Point-of care ultrasonography for diagnosing thoracoabdominal injuries in patients with blunt trauma. Cochrane Database Syst. Rev. 2018, 12, CD012669. [Google Scholar] [CrossRef]
- Yousefifard, M.; Baikpour, M.; Ghelichkhani, P.; Asady, H.; Darafarin, A.; Esfahani, M.R.A.; Hosseini, M.; Yaseri, M.; Safari, S. Comparison of Ultrasonography and Radiography in Detection of Thoracic Bone Fractures; A Systematic Review and Meta-Analysis. Emergency 2016, 4, 55–64. [Google Scholar]
- Battle, C.; Hayward, S.; Eggert, S.; Evans, P.A. Comparison of the use of lung ultrasound and chest radiography in the diagnosis of rib fracture:a systematic review. Emerg. Med. J. 2019, 36, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Pishbin, E.; Ahmadi, K.; Foogardi, M.; Salehi, M.; Seilanian Toosi, F.; Rahimi-Movaghar, V. Comparison of ultrasonography and radiography in diagnosis of rib fractures. Chin. J. Traumatol. 2017, 20, 226–228. [Google Scholar] [CrossRef] [PubMed]
- Bloise, S.; Martucci, V.; Marcellino, A.; Mallardo, S.; Lubrano, R. Possible Role of Thoracic Ultrasound in the Diagnostic Pathway of Infant Abuse in the Pediatric Emergency Department. J. Ultrasound Med. 2021, 40, 1705–1707. [Google Scholar] [CrossRef] [PubMed]
- Laursen, C.B.; Davidsen, J.R.; Madsen, P.H. Utility of lung ultrasound in near-drowning victims. BMJ Case Rep. 2012, 2012, bcr0120125687. [Google Scholar] [CrossRef]
- Bloise, S.; Martucci, V.; Marcellino, A.; Sanseviero, M.; Lubrano, R. Lung ultrasound in children drowning victims in pediatric emergency department. Pediatr. Int. 2022, 64, e15095. [Google Scholar] [CrossRef]
- Zambon, M.; Greco, M.; Bocchino, S.; Cabrini, L.; Beccaria, P.F.; Zangrillo, A. Assessment of diaphragmatic dysfunction in the critically ill patient with ultrasound: A systematic review. Intensive Care Med. 2017, 43, 29–38. [Google Scholar] [CrossRef]
- Weber, M.D.; Lim, J.K.B.; Glau, C.; Conlon, T.; James, R.; Lee, J.H. A narrative review of diaphragmatic ultrasound in pediatric critical care. Pediatr. Pulmonol. 2021, 56, 2471–2483. [Google Scholar] [CrossRef]
- Sferrazza Papa, G.; Pellegrino, G.; Di Marco, F.; Imeri, G.; Brochard, L.; Goligher, E.; Centanni, S. A Review of the Ultrasound Assessment of Diaphragmatic Function in Clinical Practice. Respiration 2016, 91, 403–411. [Google Scholar] [CrossRef]
- Şık, N.; Çitlenbik, H.; Öztürk, A.; Yılmaz, D.; Duman, M. Point of care diaphragm ultrasound: An objective tool to predict the severity of pneumonia and outcomes in children. Pediatr. Pulmonol. 2021, 56, 1666–1672. [Google Scholar] [CrossRef]
- Buonsenso, D.; Supino, M.C.; Giglioni, E.; Battaglia, M.; Mesturino, A.; Scateni, S.; Scialanga, B.; Reale, A.; Musolino, A.M.C. Point of care diaphragm ultrasound in infants with bronchiolitis: A prospective study. Pediatr. Pulmonol. 2018, 56, 778–786. [Google Scholar] [CrossRef]
- Tomà, P.; Granata, C.; Sperandeo, M. Diaphragm ultrasound in infants with bronchiolitis. Pediatr. Pulmonol. 2018, 53, 1177–1178. [Google Scholar] [CrossRef] [PubMed]
- Aras, M.H.; Miloglu, O.; Barutcugil, C.; Kantarci, M.; Ozcan, E.; Harorli, A. Comparison of the sensitivity for detecting foreign bodies among conventional plain radiography, computed tomography and ultrasonography. Dentomaxillofacial Radiol. 2010, 39, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, R.; Cico, S.J.; Bailitz, J. Point-of-care ultrasound: A new tool for the identification of gastric foreign bodies in children? J. Emerg. Med. 2016, 50, 99–103. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Group | Study Type | Outcome | Key Results |
|---|---|---|---|---|
| La Regina DP et al. [8] | 92 infants:
| Comparative study |
|
|
| Supino MC et al. [10] | 76 infants (from 1 to 12 months aged) with a clinical diagnosis of bronchiolitis. | Clinical trial |
|
|
| Bobillo-Perez S et al. [12] | 80 infants (median age 53 days) with a clinical diagnosis of bronchiolitis. | Observational study |
|
|
| Bueno-Campana M et al. [13] | 145 infants <6 months of age who were hospitalized for bronchiolitis. | Observational study |
|
|
| Taveira M et al. [14] | 47 infants <6 months of age who were hospitalized for severe acute viral bronchiolitis. | Observational study |
|
|
| Biagi C et al. [15] | 87 children from birth to 24 months of age who were hospitalized for acute bronchiolitis. | Clinical trial |
|
|
| Study | Study Type | Outcome | Key Results |
|---|---|---|---|
| Stadler JAM et al. [19] | Review |
|
|
| AM Pareda et al. [20] | Meta-analysis |
|
|
| DS Balk et al. [21] | Meta-analysis |
|
|
| Bloise et al. [24] | Clinical trial |
|
|
| G Iorio et al. [25] | Retrospective study |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bloise, S.; Marcellino, A.; Sanseviero, M.; Martucci, V.; Testa, A.; Leone, R.; Del Giudice, E.; Frasacco, B.; Gizzone, P.; Proietti Ciolli, C.; et al. Point-of-Care Thoracic Ultrasound in Children: New Advances in Pediatric Emergency Setting. Diagnostics 2023, 13, 1765. https://doi.org/10.3390/diagnostics13101765
Bloise S, Marcellino A, Sanseviero M, Martucci V, Testa A, Leone R, Del Giudice E, Frasacco B, Gizzone P, Proietti Ciolli C, et al. Point-of-Care Thoracic Ultrasound in Children: New Advances in Pediatric Emergency Setting. Diagnostics. 2023; 13(10):1765. https://doi.org/10.3390/diagnostics13101765
Chicago/Turabian StyleBloise, Silvia, Alessia Marcellino, Mariateresa Sanseviero, Vanessa Martucci, Alessia Testa, Rita Leone, Emanuela Del Giudice, Beatrice Frasacco, Pietro Gizzone, Claudia Proietti Ciolli, and et al. 2023. "Point-of-Care Thoracic Ultrasound in Children: New Advances in Pediatric Emergency Setting" Diagnostics 13, no. 10: 1765. https://doi.org/10.3390/diagnostics13101765