
Bronchoscopy Findings during Percutaneous Dilation Tracheostomy: A Single Tertiary Medical Center Experience

Abstract
:1. Introduction
2. Materials and Methods
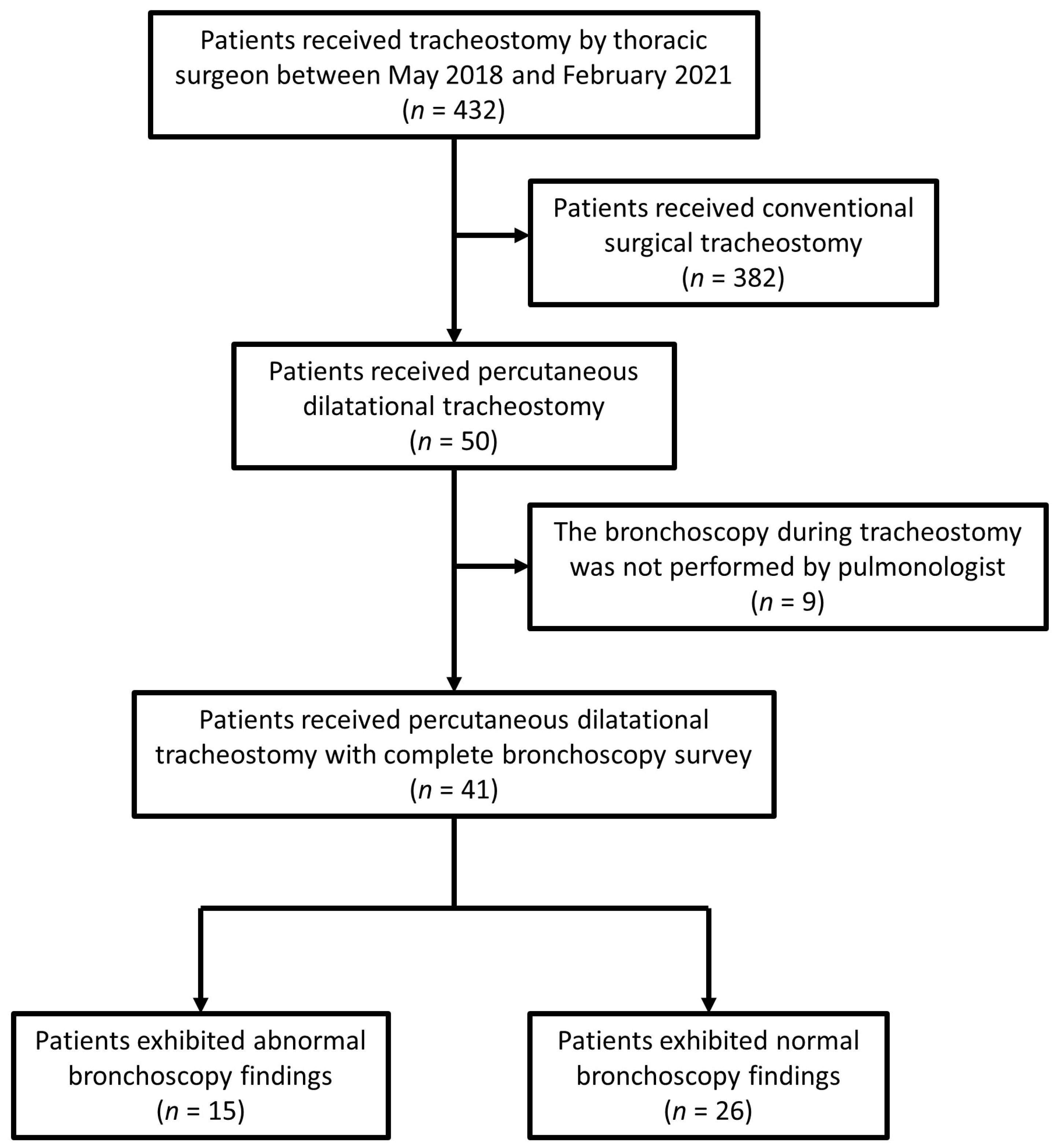
2.1. Patient Population
2.2. PDT
2.3. Arterial Blood Gas and Ventilator Setting Data
2.4. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Clinical Outcomes
3.3. Comparison of Gas Exchange and Ventilator Parameters before and after Tracheostomy
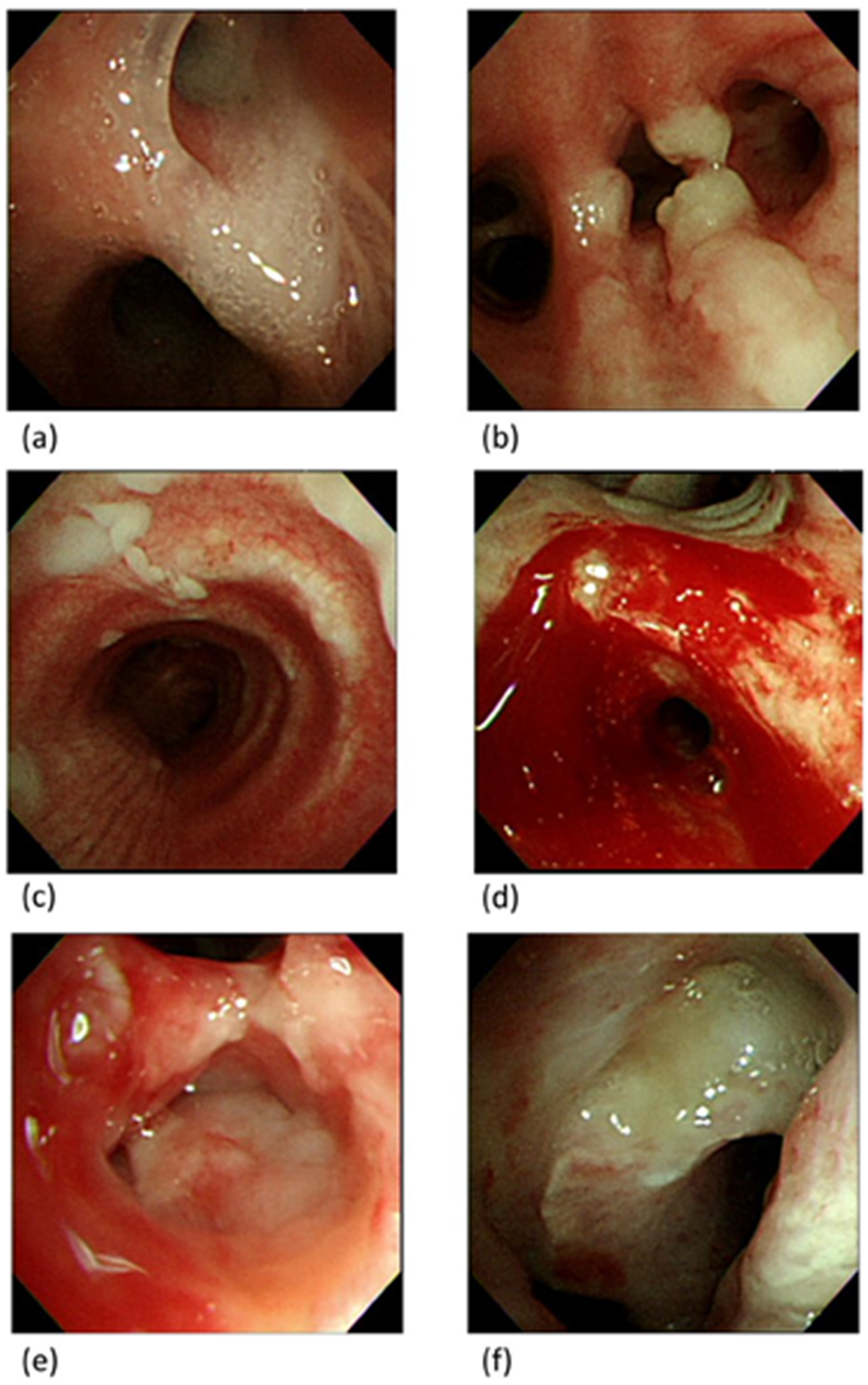
3.4. Bronchoscopy Findings
3.4.1. Case 1
3.4.2. Case 2
3.5. Bronchoscopy Findings and Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trouillet, J.L.; Collange, O.; Belafia, F.; Blot, F.; Capellier, G.; Cesareo, E.; Constantin, J.-M.; Demoule, A.; Diehl, J.-L.; Guinot, P.-G.; et al. Tracheotomy in the intensive care unit: Guidelines from a French expert panel. Ann. Intensiv. Care 2018, 8, 37. [Google Scholar] [CrossRef]
- De Leyn, P.; Bedert, L.; Delcroix, M.; Depuydt, P.; Lauwers, G.; Sokolov, Y.; Van Meerhaeghe, A.; Van Schil, P. Tracheotomy: Clinical review and guidelines. Eur. J. Cardio-Thoracic Surg. 2007, 32, 412–421. [Google Scholar] [CrossRef]
- Susarla, S.M.; Peacock, Z.S.; Alam, H.B. Percutaneous Dilatational Tracheostomy: Review of Technique and Evidence for Its Use. J. Oral Maxillofac. Surg. 2012, 70, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Delaney, A.; Bagshaw, S.M.; Nalos, M. Percutaneous dilatational tracheostomy versus surgical tracheostomy in critically ill patients: A systematic review and meta-analysis. Crit. Care 2006, 10, R55. [Google Scholar] [CrossRef] [PubMed]
- Putensen, C.; Theuerkauf, N.; Guenther, U.; Vargas, M.; Pelosi, P. Percutaneous and surgical tracheostomy in critically ill adult patients: A meta-analysis. Crit. Care 2014, 18, 544. [Google Scholar] [CrossRef]
- Saritas, A.; Saritas, P.U.; Kurnaz, M.M.; Beyaz, S.G.; Ergönenç, T. The role of fiberoptic bronchoscopy monitoring during percutaneous dilatational tracheostomy and its routine use into tracheotomy practice. J. Pak. Med. Assoc. 2016, 66, 83–89. [Google Scholar] [PubMed]
- Su, J.; Lin, C.-Y.; Chen, P.-J.; Lin, F.J.; Chen, S.-K.; Kuo, H.-T. Experience with a step-down respiratory care center at a tertiary referral medical center in Taiwan. J. Crit. Care 2006, 21, 156–161. [Google Scholar] [CrossRef]
- Wu, Y.-K.; Tsai, Y.-H.; Lan, C.-C.; Huang, C.-Y.; Lee, C.-H.; Kao, K.-C.; Fu, J.-Y. Prolonged mechanical ventilation in a respiratory-care setting: A comparison of outcome between tracheostomized and translaryngeal intubated patients. Crit. Care 2010, 14, R26. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Yurasakpong, L.; Nantasenamat, C.; Janta, S.; Eiamratchanee, P.; Coey, J.; Chaiyamoon, A.; Kruepunga, N.; Senarai, T.; Langer, M.F.; Meemon, K.; et al. The decreasing prevalence of the thyroid ima artery: A systematic review and machine learning assisted meta-analysis. Ann. Anat. Anat. Anz. 2021, 239, 151803. [Google Scholar] [CrossRef]
- Winkler, W.-B.; Karnik, R.; Seelmann, O.; Havlicek, J.; Slany, J. Bedside percutaneous dilational tracheostomy with endoscopic guidance: Experience with 71 ICU patients. Intensive Care Med. 1994, 20, 476–479. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.S.M.; Davis, J.W.; Kaups, K.L.; Sue, L.P.; Wolfe, M.M.; Bilello, J.F.; Lemaster, D. Percutaneous Tracheostomy: To Bronch or Not to Bronch—That Is the Question. J. Trauma: Inj. Infect. Crit. Care 2011, 71, 1553–1556. [Google Scholar] [CrossRef] [PubMed]
- Gadkaree, S.K.; Schwartz, D.; Gerold, K.; Kim, Y. Use of Bronchoscopy in Percutaneous Dilational Tracheostomy. JAMA Head Otolaryngol. Neck Surg. 2016, 142, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Reilly, P.M.; Sing, R.F.; Giberson, F.A.; Anderson, H.L., III; Rotondo, M.F.; Tinkoff, G.H.; Schwab, C.W. Hypercarbia during tracheostomy: A comparison of percutaneous endoscopic, percutaneous Doppler, and standard surgical tracheostomy. Intensive Care Med. 1997, 23, 859–864. [Google Scholar] [CrossRef] [PubMed]
- Dollner, R.; Verch, M.; Schweiger, P.; Deluigi, C.; Graf, B.; Wallner, F. Laryngotracheoscopic Findings in Long-term Follow-up After Griggs Tracheostomy. Chest 2002, 122, 206–212. [Google Scholar] [CrossRef]
- Gobatto, A.L.N.; Besen, B.; Tierno, P.F.G.M.M.; Mendes, P.V.; Cadamuro, F.; Joelsons, D.; Melro, L.; Carmona, M.J.C.; Santori, G.; Pelosi, P.; et al. Ultrasound-guided percutaneous dilational tracheostomy versus bronchoscopy-guided percutaneous dilational tracheostomy in critically ill patients (TRACHUS): A randomized noninferiority controlled trial. Intensive Care Med. 2016, 42, 342–351. [Google Scholar] [CrossRef]
- Gobatto, A.L.N.; Besen, B.A.M.P.; Cestari, M.; Pelosi, P.; Malbouisson, L.M.S. Ultrasound-Guided Percutaneous Dilational Tracheostomy: A Systematic Review of Randomized Controlled Trials and Meta-Analysis. J. Intensive Care Med. 2018, 35, 445–452. [Google Scholar] [CrossRef]
- Bellani, G.; El, S.A.; Pradella, A.; Mauri, T.; Citerio, G.; Foti, G.; Pesenti, A. Effect of Percutaneous Tracheostomy on Gas Exchange in Hypoxemic and Nonhypoxemic Mechanically Ventilated Patients. Respir. Care 2013, 58, 482–486. [Google Scholar] [CrossRef]
- Gergin, O.; Adil, E.; Kawai, K.; Watters, K.; Moritz, E.; Rahbar, R. Routine airway surveillance in pediatric tracheostomy patients. Int. J. Pediatr. Otorhinolaryngol. 2017, 97, 1–4. [Google Scholar] [CrossRef]
- Ernst, A.; Feller-Kopman, D.; Becker, H.D.; Mehta, A.C. Central Airway Obstruction. Am. J. Respir. Crit. Care Med. 2004, 169, 1278–1297. [Google Scholar] [CrossRef]
- Zhang, G.S.; Xu, Z.H.; Cui, W.; Zhou, F.; Xia, Y.; Li, W.; Li, L.B.; Shen, H.H. A case with lethal endobronchial lymphoma pre-senting with respiratory failure requiring intubation and mechanical ventilation. Chin. Med. J. 2008, 121, 280–282. [Google Scholar] [CrossRef] [PubMed]
- Ivanick, N.M.; Moh, M.; Seeley, E.J.; Benn, B.S. Bilateral Endobronchial Masses and Severe Hypoxemic Respiratory Failure. J. Bronchol. Interv. Pulmonol. 2019, 26, e65–e67. [Google Scholar] [CrossRef]
- Uchida, R.; Masugi, Y.; Nishizawa, T.; Kimura, T.; Yamada, T. Extensive endobronchial growth of metastatic hepatocellular carcinoma resulting in respiratory failure: A case report. Pathol. Res. Pract. 2010, 206, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.C.; Yang, M.C.; Lee, C.H.; Huang, S.F.; Wu, Y.K. Solitary primary tracheal small-cell lung cancer causing acute respir-atory failure: Diagnosis and treatment. Respir. Care 2010, 55, 929–932. [Google Scholar] [PubMed]
- Qiao, Z.; Yu, J.; Yu, K.; Zhang, M. The benefit of daily sputum suction via bronchoscopy in patients of chronic obstructive pulmonary disease with ventilators. Medicine 2018, 97, e11631. [Google Scholar] [CrossRef]
- Liu, Y.; Lu, H.-W.; Gu, S.-Y.; Wang, W.-W.; Ge, J.; Jie, Z.-J.; Jia, J.-G.; Gao, Z.-T.; Li, J.; Shi, J.-Y.; et al. Bronchoscopic airway clearance therapy for acute exacerbations of bronchiectasis. Ebiomedicine 2021, 72, 103587. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total Patients (n = 41) | Intraairway Abnormality (n = 15) | No Intraairway Abnormality (n = 26) | p Value |
|---|---|---|---|---|
| Sex (female/male) | 22/19 | 7/8 | 15/11 | 0.495 |
| Age (years) | 70.3 ± 13.1 | 69.8 ± 10.7 | 70.5 ± 14.5 | 0.758 |
| BMI (kg/m2) | 22.7 ± 4.1 | 23.0 ± 4.0 | 22.5 ± 4.2 | 0.799 |
| Patients’ source | ||||
| Respiratory care center | 16 (39.0%) | 7 (46.7%) | 9 (34.6%) | 0.667 |
| Medical ICU | 14 (34.1%) | 4 (26.7%) | 10 (38.5%) | |
| Cardiac ICU | 2 (4.9%) | 0 (0.0%) | 2 (7.7%) | |
| Alimentary ICU | 6 (14.6%) | 3 (20.0%) | 3 (11.5%) | |
| Surgical ICU | 3 (7.3%) | 1 (6.7%) | 2 (7.7%) | |
| Indication for tracheostomy or etiology of chronic respiratory failure | ||||
| Pulmonary disease | 27 (65.9%) | 12 (80.0%) | 15 (57.7%) | 0.488 |
| Central nervous system problem | 6 (14.6%) | 1 (6.7%) | 5 (19.2%) | |
| Upper airway problem | 8 (19.5%) | 2 (13.3%) | 6 (23.1%) | |
| Duration from respiratory failure to tracheostomy (days) | 26.4 ± 19.9 | 29.8 ± 24.1 | 24.4 ± 17.3 | 0.547 |
| SOFA score | 4.6 ± 2.7 | 5.5 ± 3.3 | 4.0 ± 2.1 | 0.211 |
| Laboratory Data | ||||
| White blood cell (1000/uL) | 9.3 ± 5.8 | 8.1 ± 3.4 | 10.0 ± 6.7 | 0.659 |
| Platelet (1000/uL) | 217.2 ± 116.2 | 181.3 ± 130.0 | 237.9 ± 104.5 | 0.086 |
| PT/INR | 1.2 ± 0.1 | 1.2 ± 0.1 | 1.2 ± 0.1 | 0.565 |
| Total bilirubin (mg/dL) | 0.7 ± 0.9 | 0.7 ± 0.6 | 0.7 ± 1.0 | 0.547 |
| Creatinine (mg/dL) | 1.2 ± 1.2 | 1.1 ± 1.1 | 1.3 ± 1.3 | 0.529 |
| Blood gas data before tracheostomy | ||||
| PaO2/FIO2 ratio (mmHg) | 313.5 ± 100.4 | 294.1 ± 105.2 | 324.8 ± 97.8 | 0.277 |
| PaCO2 (mmHg) | 45.3 ± 13.1 | 48.0 ± 15.3 | 43.7 ± 11.7 | 0.445 |
| pH | 7.4 ± 0.1 | 7.4 ± 0.1 | 7.4 ± 0.1 | 0.183 |
| Ventilator settings before tracheostomy | ||||
| Positive end-expiratory pressure (cm H2O) | 8.0 ± 0.9 | 8.4 ± 0.8 | 7.8 ± 0.9 | 0.131 |
| Peak airway pressure (cm H2O) | 22.7 ± 7.0 | 22.5 ± 5.8 | 22.8 ± 7.8 | >0.999 |
| Tidal volume/predicted body weight (mL/kg) | 8.4 ± 2.0 | 8.7 ± 2.0 | 8.1 ± 1.9 | 0.283 |
| Procedure duration | ||||
| Bronchoscopy (second) | 49.8 ± 43.8 | 77.3 ± 57.3 | 33.1 ± 20.6 | 0.001 * |
| Tracheostomy (second) | 102.8 ± 34.6 | 98.9 ± 39.0 | 105.5 ± 31.9 | 0.334 |
| Before Tracheostomy | After Tracheostomy | p Value | |
|---|---|---|---|
| PaO2/FiO2 ratio (mmHg) | 313.5 ± 100.4 | 331.6 ± 93.8 | 0.196 |
| PaCO2 (mmHg) | 45.3 ± 13.1 | 45.4 ± 12.0 | 0.933 |
| pH | 7.4 ± 0.1 | 7.4 ± 0.1 | 0.927 |
| Positive end-expiratory pressure (cm H2O) | 8.1 ± 0.8 | 7.9 ± 1.0 | 0.183 |
| Peak airway pressure (cm H2O) | 23.4 ± 6.9 | 22.6 ± 7.8 | 0.403 |
| Tidal volume/predicted body weight (mL/kg) | 8.3 ± 1.9 | 8.3 ± 2.7 | 0.962 |
| Total | Liberated from Ventilator | Ventilator Dependent | In-Hospital Mortality | |
|---|---|---|---|---|
| No abnormality | 26 | 13 (50.0%) | 9 (34.6%) | 4 (15.4%) |
| Increased secretion | 7 | 4 (57.1%) | 1 (14.3%) | 2 (28.6%) |
| Granulation tissue without airway obstruction | 3 | 2 (66.7%) | 0 (0.0%) | 1 (33.3%) |
| Mucosal patches | 1 | 0 (0.0%) | 1 (100.0%) | 0 (0.0%) |
| Mass lesions with airway obstruction | 2 | 0 (0.0%) | 2 (100.0%) | 0 (0.0%) |
| Tumor invasion | 1 | 0 (0.0%) | 0 (0.0%) | 1 (100.0%) |
| Peripheral airway mucosal blood oozing | 1 | 0 (0.0%) | 1 (100.0%) | 0 (0.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, K.-W.; Fang, H.-Y. Bronchoscopy Findings during Percutaneous Dilation Tracheostomy: A Single Tertiary Medical Center Experience. Diagnostics 2023, 13, 1764. https://doi.org/10.3390/diagnostics13101764
Chang K-W, Fang H-Y. Bronchoscopy Findings during Percutaneous Dilation Tracheostomy: A Single Tertiary Medical Center Experience. Diagnostics. 2023; 13(10):1764. https://doi.org/10.3390/diagnostics13101764
Chicago/Turabian StyleChang, Ko-Wei, and Hsin-Yueh Fang. 2023. "Bronchoscopy Findings during Percutaneous Dilation Tracheostomy: A Single Tertiary Medical Center Experience" Diagnostics 13, no. 10: 1764. https://doi.org/10.3390/diagnostics13101764