
Brain Volume Changes after COVID-19 Compared to Healthy Controls by Artificial Intelligence-Based MRI Volumetry
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- aged 25 to 75 years
- Cohort I: asymptomatic course (MILD) of COVID-19 (SARS-CoV-2–positive) or mild course (i.e., declaration of no symptoms other than anosmia or ageusia)
- Cohort II: severely affected course (SEV) of COVID-19 (SARS-CoV-2–positive) according to simplified WHO classification, defined as having been admitted to hospital (any ward type) for at least 24 h due to SARS-CoV-2 infection at any timepoint during the course of the disease
- Cohort III: healthy controls (CTL) will only be included in the study if they also meet all of the following criteria:
- must perform > –1.0 SD on the Hopkins Verbal Learning Test
- no substance abuse
- no known history of or current diagnosed psychiatric illness
- negative nCoV IgG/IgM Rapid Test before inclusion, indicative of no recent COVID-19 infection
- general contraindication for MRI
- severe or unstable medical condition
- current major depressive episode
- psychotic disorder, bipolar disorder, substance abuse at present or in the past
- known neurodegenerative disorder (Alzheimer’s disease, Parkinson’s disease, frontotemporal dementia, Huntington’s disease, amyotrophic lateral sclerosis)
- vascular dementia or history of stroke
- history of malignant disease
2.2. Magnetic Resonance Imaging
2.3. Image Analysis
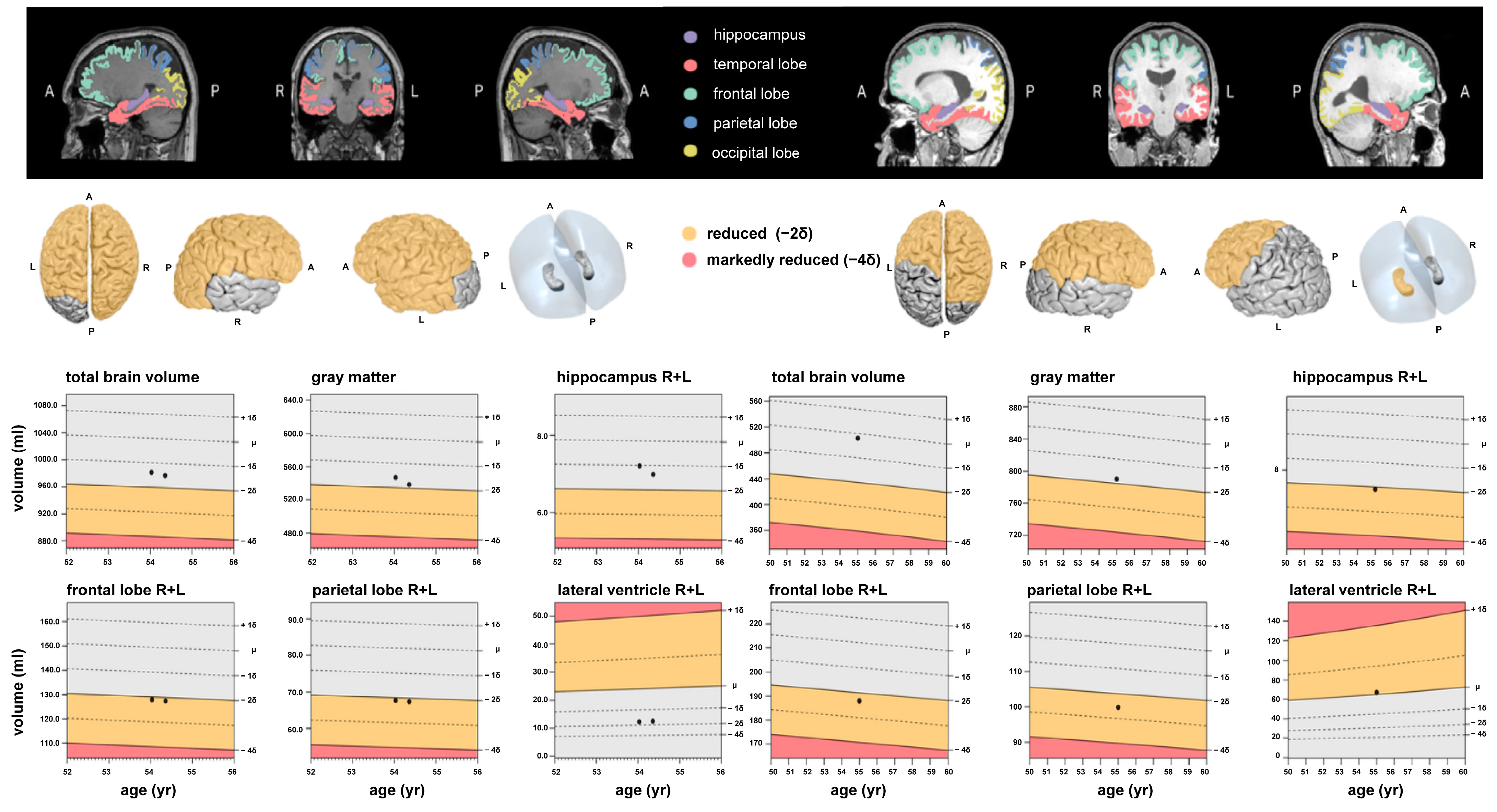
2.4. Post-Processing and Artificial Intelligence (AI)-Based Volumetry
2.5. Statistical Analysis
3. Results
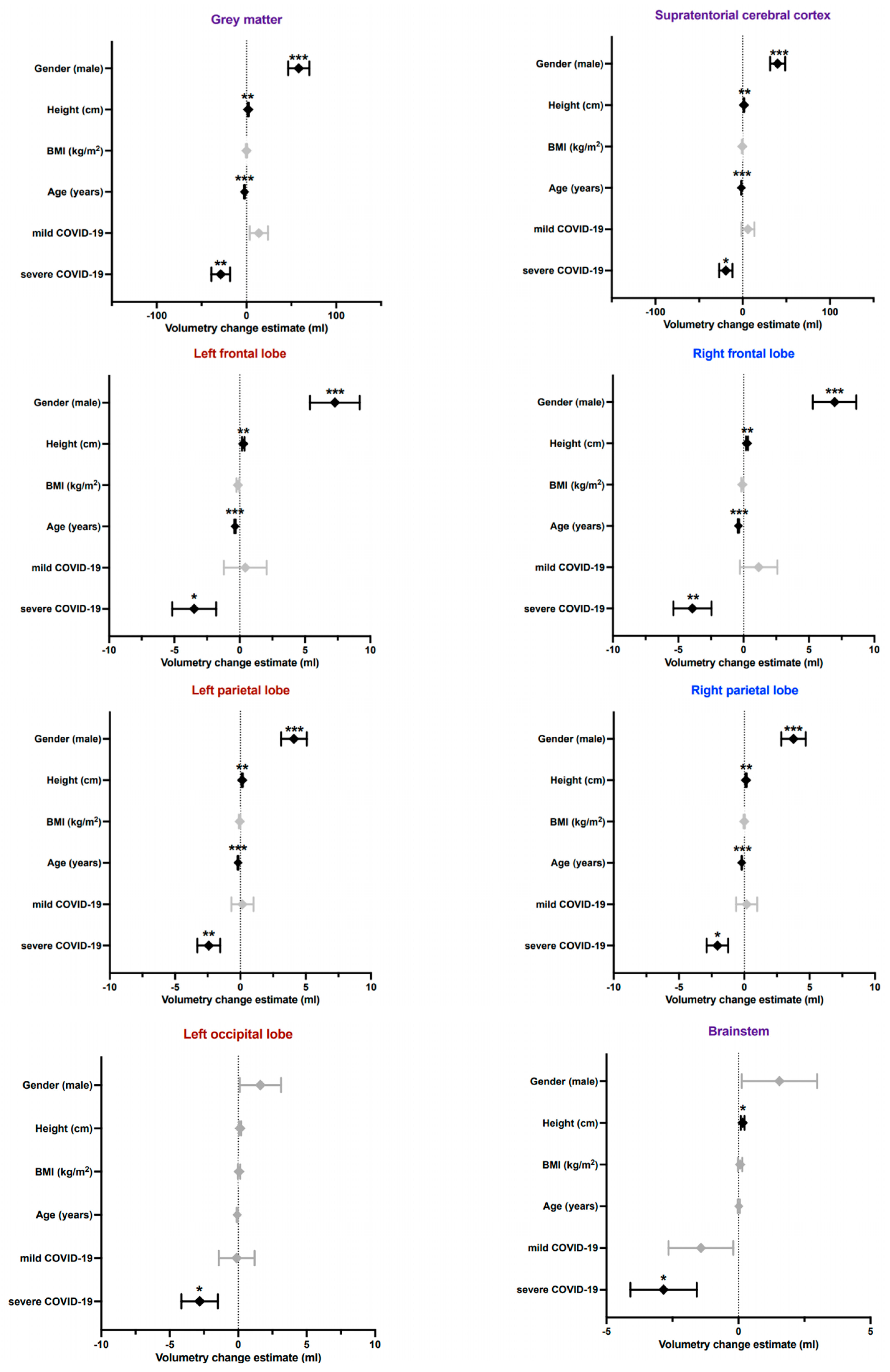
Volumetric Brain Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aghagoli, G.; Gallo Marin, B.; Katchur, N.J.; Chaves-Sell, F.; Asaad, W.F.; Murphy, S.A. Neurological Involvement in COVID-19 and Potential Mechanisms: A Review. Neurocritcal Care 2021, 34, 1062–1071. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef] [PubMed]
- Ortelli, P.; Ferrazzoli, D.; Sebastianelli, L.; Engl, M.; Romanello, R.; Nardone, R.; Bonini, I.; Koch, G.; Saltuari, L.; Quartarone, A.; et al. Neuropsychological and neurophysiological correlates of fatigue in post-acute patients with neurological manifestations of COVID-19: Insights into a challenging symptom. J. Neurol. Sci. 2021, 420, 117271. [Google Scholar] [CrossRef]
- Romagnolo, A.; Balestrino, R.; Imbalzano, G.; Ciccone, G.; Riccardini, F.; Artusi, C.A.; Bozzali, M.; Ferrero, B.; Montalenti, E.; Montanaro, E.; et al. Neurological comorbidity and severity of COVID-19. J. Neurol. 2021, 268, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Herman, C.; Mayer, K.; Sarwal, A. Scoping review of prevalence of neurologic comorbidities in patients hospitalized for COVID-19. Neurology 2020, 95, 77–84. [Google Scholar] [CrossRef]
- Heneka, M.T.; Golenbock, D.; Latz, E.; Morgan, D.; Brown, R. Immediate and long-term consequences of COVID-19 infections for the development of neurological disease. Alzheimer’s Res. Ther. 2020, 12, 69. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef]
- Paterson, R.W.; Brown, R.L.; Benjamin, L.; Nortley, R.; Wiethoff, S.; Bharucha, T.; Jayaseelan, D.L.; Kumar, G.; Raftopoulos, R.E.; Zambreanu, L.; et al. The emerging spectrum of COVID-19 neurology: Clinical, radiological and laboratory findings. Brain 2020, 143, 3104–3120. [Google Scholar] [CrossRef]
- Widmann, C.N.; Wieberneit, M.; Bieler, L.; Bernsen, S.; Grafenkamper, R.; Brosseron, F.; Schmeel, C.; Tacik, P.; Skowasch, D.; Radbruch, A.; et al. Longitudinal Neurocognitive and Pulmonological Profile of Long COVID-19: Protocol for the COVIMMUNE-Clin Study. JMIR Res. Protoc. 2021, 10, e30259. [Google Scholar] [CrossRef] [PubMed]
- Dieckmeyer, M.; Roy, A.G.; Senapati, J.; Wachinger, C.; Grundl, L.; Dopfert, J.; Bertran, P.F.; Lemke, A.; Zimmer, C.; Kirschke, J.S.; et al. Effect of MRI acquisition acceleration via compressed sensing and parallel imaging on brain volumetry. Magn. Reson. Mater. Phys. Biol. Med. 2021, 34, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Suchyta, M.R.; Jephson, A.; Hopkins, R.O. Neurologic changes during critical illness: Brain imaging findings and neurobehavioral outcomes. Brain Imaging Behav. 2010, 4, 22–34. [Google Scholar] [CrossRef]
- Gunther, M.L.; Morandi, A.; Krauskopf, E.; Pandharipande, P.; Girard, T.D.; Jackson, J.C.; Thompson, J.; Shintani, A.K.; Geevarghese, S.; Miller, R.R., 3rd; et al. The association between brain volumes, delirium duration, and cognitive outcomes in intensive care unit survivors: The VISIONS cohort magnetic resonance imaging study*. Crit. Care Med. 2012, 40, 2022–2032. [Google Scholar] [CrossRef] [PubMed]
- Manca, R.; De Marco, M.; Ince, P.G.; Venneri, A. Heterogeneity in Regional Damage Detected by Neuroimaging and Neuropathological Studies in Older Adults With COVID-19: A Cognitive-Neuroscience Systematic Review to Inform the Long-Term Impact of the Virus on Neurocognitive Trajectories. Front. Aging Neurosci. 2021, 13, 646908. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; McCarthy, P.; Lange, F.; Andersson, J.L.R.; Griffanti, L.; Duff, E.; et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Hosp, J.A.; Dressing, A.; Blazhenets, G.; Bormann, T.; Rau, A.; Schwabenland, M.; Thurow, J.; Wagner, D.; Waller, C.; Niesen, W.D.; et al. Cognitive impairment and altered cerebral glucose metabolism in the subacute stage of COVID-19. Brain 2021, 144, 1263–1276. [Google Scholar] [CrossRef]
- Guedj, E.; Million, M.; Dudouet, P.; Tissot-Dupont, H.; Bregeon, F.; Cammilleri, S.; Raoult, D. (18)F-FDG brain PET hypometabolism in post-SARS-CoV-2 infection: Substrate for persistent/delayed disorders? Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 592–595. [Google Scholar] [CrossRef] [PubMed]
- Duan, K.; Premi, E.; Pilotto, A.; Cristillo, V.; Benussi, A.; Libri, I.; Giunta, M.; Bockholt, H.J.; Liu, J.; Campora, R.; et al. Alterations of frontal-temporal gray matter volume associate with clinical measures of older adults with COVID-19. Neurobiol. Stress 2021, 14, 100326. [Google Scholar] [CrossRef]
- Griffanti, L.; Raman, B.; Alfaro-Almagro, F.; Filippini, N.; Cassar, M.P.; Sheerin, F.; Okell, T.W.; Kennedy McConnell, F.A.; Chappell, M.A.; Wang, C.; et al. Adapting the UK Biobank Brain Imaging Protocol and Analysis Pipeline for the C-MORE Multi-Organ Study of COVID-19 Survivors. Front. Neurol. 2021, 12, 753284. [Google Scholar] [CrossRef]
- Lee, M.H.; Perl, D.P.; Nair, G.; Li, W.; Maric, D.; Murray, H.; Dodd, S.J.; Koretsky, A.P.; Watts, J.A.; Cheung, V.; et al. Microvascular Injury in the Brains of Patients with COVID-19. N. Engl. J. Med. 2021, 384, 481–483. [Google Scholar] [CrossRef]
- Sanabria-Diaz, G.; Etter, M.M.; Melie-Garcia, L.; Lieb, J.M.; Psychogios, M.N.; Hutter, G.; Granziera, C. Brain cortical alterations in COVID-19 patients with neurological symptoms. Front. Neurosci. 2022, 16, 992165. [Google Scholar] [CrossRef] [PubMed]
- Kandemirli, S.G.; Dogan, L.; Sarikaya, Z.T.; Kara, S.; Akinci, C.; Kaya, D.; Kaya, Y.; Yildirim, D.; Tuzuner, F.; Yildirim, M.S.; et al. Brain MRI Findings in Patients in the Intensive Care Unit with COVID-19 Infection. Radiology 2020, 297, E232–E235. [Google Scholar] [CrossRef] [PubMed]
- Bougakov, D.; Podell, K.; Goldberg, E. Multiple Neuroinvasive Pathways in COVID-19. Mol. Neurobiol. 2021, 58, 564–575. [Google Scholar] [CrossRef]
- Romoli, M.; Jelcic, I.; Bernard-Valnet, R.; Garcia Azorin, D.; Mancinelli, L.; Akhvlediani, T.; Monaco, S.; Taba, P.; Sellner, J.; Infectious Disease Panel of the European Academy of Neurology. A systematic review of neurological manifestations of SARS-CoV-2 infection: The devil is hidden in the details. Eur. J. Neurol. 2020, 27, 1712–1726. [Google Scholar] [CrossRef] [PubMed]
- Calsavara, A.J.C.; Nobre, V.; Barichello, T.; Teixeira, A.L. Post-sepsis cognitive impairment and associated risk factors: A systematic review. Aust. Crit. Care 2018, 31, 242–253. [Google Scholar] [CrossRef]
- Jackson, J.C.; Pandharipande, P.P.; Girard, T.D.; Brummel, N.E.; Thompson, J.L.; Hughes, C.G.; Pun, B.T.; Vasilevskis, E.E.; Morandi, A.; Shintani, A.K.; et al. Depression, post-traumatic stress disorder, and functional disability in survivors of critical illness in the BRAIN-ICU study: A longitudinal cohort study. Lancet Respir. Med. 2014, 2, 369–379. [Google Scholar] [CrossRef]
- Julayanont, P.; Tangwongchai, S.; Hemrungrojn, S.; Tunvirachaisakul, C.; Phanthumchinda, K.; Hongsawat, J.; Suwichanarakul, P.; Thanasirorat, S.; Nasreddine, Z.S. The Montreal Cognitive Assessment-Basic: A Screening Tool for Mild Cognitive Impairment in Illiterate and Low-Educated Elderly Adults. J. Am. Geriatr. Soc. 2015, 63, 2550–2554. [Google Scholar] [CrossRef]
- Ibi, K.; Fujii, K.; Kobayashi, H.; Senda, M.; Kitazawa, K.; Honda, A. Anterior cingulate cortex involvement in non-paraneoplastic limbic encephalitis. Brain Dev. 2019, 41, 735–739. [Google Scholar] [CrossRef]
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.Y.; Huang, C.C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral Micro-Structural Changes in COVID-19 Patients—An MRI-based 3-month Follow-up Study. EClinicalMedicine 2020, 25, 100484. [Google Scholar] [CrossRef]
- Seidenberg, M.; Hermann, B.; Pulsipher, D.; Morton, J.; Parrish, J.; Geary, E.; Guidotti, L. Thalamic atrophy and cognition in unilateral temporal lobe epilepsy. J. Int. Neuropsychol. Soc. 2008, 14, 384–393. [Google Scholar] [CrossRef]
- Yang, A.C.; Kern, F.; Losada, P.M.; Agam, M.R.; Maat, C.A.; Schmartz, G.P.; Fehlmann, T.; Stein, J.A.; Schaum, N.; Lee, D.P.; et al. Dysregulation of brain and choroid plexus cell types in severe COVID-19. Nature 2021, 595, 565–571. [Google Scholar] [CrossRef] [PubMed]
- de Erausquin, G.A.; Snyder, H.; Carrillo, M.; Hosseini, A.A.; Brugha, T.S.; Seshadri, S.; CNS SARS-CoV-2 Consortium. The chronic neuropsychiatric sequelae of COVID-19: The need for a prospective study of viral impact on brain functioning. Alzheimer’s Dement. 2021, 17, 1056–1065. [Google Scholar] [CrossRef]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brunink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Butowt, R.; Meunier, N.; Bryche, B.; von Bartheld, C.S. The olfactory nerve is not a likely route to brain infection in COVID-19: A critical review of data from humans and animal models. Acta Neuropathol. 2021, 141, 809–822. [Google Scholar] [CrossRef] [PubMed]
- Butowt, R.; Bilinska, K.; von Bartheld, C.S. Olfactory dysfunction in COVID-19: New insights into the underlying mechanisms. Trends Neurosci. 2023, 46, 75–90. [Google Scholar] [CrossRef]
- Postma, E.M.; Smeets, P.A.M.; Boek, W.M.; Boesveldt, S. Investigating morphological changes in the brain in relation to etiology and duration of olfactory dysfunction with voxel-based morphometry. Sci. Rep. 2021, 11, 12704. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, X.; Lin, J.; Sun, Y.; Huang, Y.; Yang, T.; Zheng, S.; Fan, M.; Zhang, J. Reduced regional gray matter volume in patients with chronic obstructive pulmonary disease: A voxel-based morphometry study. AJNR Am. J. Neuroradiol. 2013, 34, 334–339. [Google Scholar] [CrossRef]
- Harch, P.G.; Fogarty, E.F. Subacute normobaric oxygen and hyperbaric oxygen therapy in drowning, reversal of brain volume loss: A case report. Med. Gas Res. 2017, 7, 144–149. [Google Scholar] [CrossRef]
- Wilcox, M.E.; Brummel, N.E.; Archer, K.; Ely, E.W.; Jackson, J.C.; Hopkins, R.O. Cognitive dysfunction in ICU patients: Risk factors, predictors, and rehabilitation interventions. Crit. Care Med. 2013, 41, S81–S98. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sequence | Pulse Type | Orientation | TR (ms) | TE (ms) | Reconstructed Voxel Size (mm) | Matrix (mm) | Slices |
|---|---|---|---|---|---|---|---|
| T2w | Turbo spin echo | axial | 13.257 | 90 | 0.94 × 0.94 × 1 | 240 × 174 | 140 |
| SWI | 3D fast field echo | axial | 31 | 0 | 0.6 × 0.6 × 2 | 384 × 316 | 145 |
| DWI | b values (0, 500, 1000 s/mm2) | axial | 2725 | 41 | 1 × 1 × 5 | 128 × 127 | 24 |
| T1w | MPRAGE | sagittal | 7.3 | 3.9 | 1 × 1 × 1 | 256 × 256 | 180 |
| FLAIR | 3D gradient echo | sagittal | 4800 | 275 | 1.12 × 1.12 × 1.12 | 240 × 240 | 321 |
| Characteristics | Healthy Control Subjects (CTL) | Mild COVID-19 Course (MILD) | Severe COVID-19 Course (SEV) | Total | p-Value a |
|---|---|---|---|---|---|
| n | 56 | 51 | 48 | 155 | |
| Age (years) | 47.0 ± 13.3 | 45.7 ± 12.4 | 50.6 ± 12.0 | 47.7 ± 12.7 | 0.612 |
| Gender (m:f) | 26:25 | 28:28 | 25:23 | 78:76 | 0.775 |
| Height (mm) | 175.0 ± 10.5 | 173.6 ± 10.7 | 172.8 ± 10.0 | 173.8 ± 9.9 | 0.316 |
| Weight (kg) | 79.6 ± 16.2 | 81.8 ± 23.5 | 84.4 ± 20.7 | 81.8 ± 20.2 | 0.315 |
| BMI | 25.9 ± 4.3 | 27.2 ± 9.1 | 27.9 ± 6.1 | 27 ± 6.7 | 0.154 |
| Brain Region | CTL | MILD | SEV | ||||
|---|---|---|---|---|---|---|---|
| Mean | ±SD | Mean | ±SD | Mean | ±SD | p-Value a | |
| Whole brain | 1264.18 | 117.28 | 1298.19 | 143.63 | 1210.70 | 113.49 | 0.003 |
| Whole brain white substance | 554.24 | 61.31 | 571.79 | 74.26 | 537.20 | 57.18 | 0.32 |
| Whole brain grey substance | 709.83 | 64.35 | 726.87 | 79.03 | 670.34 | 71.03 | ≤0.001 |
| Supratentorial gross cerebral cortex | 483.68 | 46.01 | 491.17 | 58.25 | 455.79 | 48.26 | 0.002 |
| Frontal right | 91.28 | 9.72 | 92.81 | 11.20 | 85.32 | 9.37 | 0.001 |
| Frontal left | 87.52 | 9.05 | 88.22 | 13.73 | 82.05 | 9.23 | 0.01 |
| Parietal right | 48.09 | 5.12 | 48.53 | 5.87 | 45.10 | 5.40 | 0.004 |
| Parietal left | 50.29 | 5.44 | 50.63 | 6.01 | 46.91 | 5.52 | 0.002 |
| Precuneus right | 11.44 | 1.45 | 11.66 | 1.60 | 10.77 | 1.36 | 0.008 |
| Precuneus left | 11.91 | 2.05 | 12.16 | 1.76 | 11.21 | 1.72 | 0.032 |
| Occipital right | 31.52 | 3.38 | 33.27 | 9.40 | 30.26 | 5.51 | 0.073 |
| Occipital left | 37.83 | 8.09 | 37.79 | 7.32 | 34.61 | 4.67 | 0.031 |
| Temporal right | 71.60 | 7.20 | 73.83 | 9.20 | 68.49 | 7.44 | 0.005 |
| Temporal left | 66.46 | 8.31 | 68.20 | 9.64 | 63.99 | 6.73 | 0.045 |
| Mesiotemporal right | 23.86 | 11.00 | 26.28 | 10.79 | 23.91 | 10.24 | 0.423 |
| Mesiotemporal left | 22.44 | 10.23 | 24.67 | 9.77 | 22.40 | 9.34 | 0.402 |
| Hippocampus right | 5.02 | 5.87 | 4.35 | 0.53 | 4.17 | 0.42 | 0.43 |
| Hippocampus left | 5.54 | 10.69 | 4.87 | 3.79 | 4.12 | 0.58 | 0.569 |
| Gyrus parahippocampalis right | 3.27 | 0.37 | 3.40 | 0.44 | 3.22 | 0.33 | 0.053 |
| Gyrus parahippocampalis left | 3.41 | 0.33 | 3.55 | 0.37 | 3.32 | 0.33 | 0.005 |
| Regio entorhinalis right | 2.51 | 0.31 | 2.60 | 0.32 | 2.47 | 0.24 | 0.097 |
| Regio entorhinalis left | 2.45 | 0.28 | 2.52 | 0.31 | 2.42 | 0.30 | 0.27 |
| Nucleus caudatus right | 3.30 | 0.43 | 3.49 | 0.40 | 3.19 | 0.43 | 0.002 |
| Nucleus caudatus left | 2.93 | 0.38 | 3.15 | 0.35 | 2.84 | 0.40 | ≤0.001 |
| Putamen right | 4.19 | 0.46 | 4.33 | 0.51 | 4.02 | 0.48 | 0.006 |
| Putamen left | 4.31 | 0.47 | 4.45 | 0.55 | 4.11 | 0.46 | 0.004 |
| Pallidum right | 1.43 | 0.17 | 1.47 | 0.15 | 1.38 | 0.14 | 0.014 |
| Pallidum left | 1.38 | 0.15 | 1.44 | 0.16 | 1.34 | 0.15 | 0.005 |
| Thalamus right | 8.13 | 0.76 | 8.35 | 0.81 | 7.66 | 0.77 | ≤0.001 |
| Thalamus left | 8.46 | 0.81 | 8.46 | 1.35 | 7.99 | 0.78 | 0.031 |
| Brainstem | 27.87 | 10.31 | 26.39 | 2.92 | 24.88 | 2.62 | 0.072 |
| Mesencephalon | 8.91 | 12.29 | 7.23 | 0.90 | 6.81 | 0.84 | 0.307 |
| Pons | 15.86 | 11.18 | 14.36 | 1.77 | 13.59 | 1.47 | 0.228 |
| Cerebellar grey matter | 109.62 | 25.60 | 112.52 | 11.18 | 105.98 | 11.48 | 0.017 |
| Left ventricle | 10.09 | 7.46 | 8.51 | 5.92 | 8.83 | 5.14 | 0.389 |
| Right ventricle | 9.91 | 6.21 | 9.01 | 5.55 | 9.56 | 5.44 | 0.723 |
| Third ventricle | 0.69 | 0.41 | 0.76 | 0.39 | 0.78 | 0.35 | 0.423 |
| Fourth ventricle | 1.16 | 0.37 | 1.20 | 0.42 | 1.10 | 0.36 | 0.378 |
| Brain Region | CTL | MILD | SEV | ||||
|---|---|---|---|---|---|---|---|
| Mean | ±SD | Mean | ±SD | Mean | ±SD | p-Value a | |
| Whole brain | 82.09 | 17.40 | 80.56 | 21.51 | 71.09 | 27.13 | 0.029 |
| Whole brain white substance | 85.82 | 16.02 | 85.84 | 16.67 | 82.55 | 24.63 | 0.619 |
| Whole brain grey substance | 56.14 | 24.23 | 53.18 | 26.60 | 43.65 | 26.24 | 0.041 |
| Supratentorial gross cerebral cortex | 46.49 | 25.98 | 40.35 | 26.02 | 35.05 | 26.77 | 0.088 |
| Frontal right | 55.31 | 26.81 | 46.84 | 27.67 | 39.85 | 27.97 | 0.018 |
| Frontal left | 48.41 | 25.53 | 43.48 | 27.30 | 35.83 | 27.84 | 0.061 |
| Parietal right | 34.16 | 21.89 | 26.27 | 21.09 | 28.87 | 24.10 | 0.178 |
| Parietal left | 46.44 | 25.26 | 36.91 | 23.87 | 36.26 | 26.09 | 0.066 |
| Precuneus right | 47.78 | 29.91 | 45.68 | 26.00 | 42.65 | 26.69 | 0.641 |
| Precuneus left | 70.30 | 23.34 | 64.93 | 25.74 | 60.31 | 31.78 | 0.171 |
| Occipital right | 23.70 | 24.08 | 21.92 | 23.72 | 19.84 | 23.36 | 0.711 |
| Occipital left | 40.51 | 27.27 | 38.06 | 28.98 | 34.79 | 28.45 | 0.589 |
| Temporal right | 56.31 | 28.07 | 57.84 | 27.54 | 51.79 | 28.19 | 0.536 |
| Temporal left | 56.83 | 30.13 | 59.44 | 27.70 | 49.30 | 28.46 | 0.197 |
| Mesiotemporal right | 48.95 | 32.89 | 53.54 | 28.83 | 48.34 | 32.17 | 0.66 |
| Mesiotemporal left | 48.21 | 33.66 | 52.61 | 28.19 | 48.02 | 31.52 | 0.703 |
| Hippocampus right | 56.14 | 26.79 | 57.43 | 28.65 | 56.09 | 26.77 | 0.962 |
| Hippocampus left | 58.86 | 26.41 | 59.19 | 27.21 | 58.84 | 24.98 | 0.997 |
| Gyrus parahippocampalis right | 62.83 | 28.41 | 69.88 | 28.61 | 67.68 | 22.35 | 0.378 |
| Gyrus parahippocampalis left | 60.66 | 27.73 | 71.51 | 23.27 | 60.91 | 26.97 | 0.058 |
| Regio entorhinalis right | 70.46 | 26.90 | 75.37 | 21.56 | 72.13 | 19.83 | 0.543 |
| Regio entorhinalis left | 59.11 | 26.74 | 63.99 | 26.23 | 58.62 | 26.94 | 0.532 |
| Nucleus caudatus right | 40.50 | 25.82 | 52.19 | 24.97 | 40.37 | 27.25 | 0.033 |
| Nucleus caudatus left | 27.37 | 22.08 | 39.51 | 23.31 | 27.90 | 24.42 | ≤0.001 |
| Putamen right | 27.69 | 22.36 | 31.95 | 24.28 | 25.74 | 25.12 | 0.415 |
| Putamen left | 29.71 | 24.42 | 33.84 | 25.37 | 25.11 | 22.97 | 0.207 |
| Pallidum right | 36.65 | 27.64 | 40.73 | 25.44 | 36.08 | 29.20 | 0.648 |
| Pallidum left | 27.09 | 23.85 | 28.51 | 22.19 | 25.08 | 25.64 | 0.773 |
| Thalamus right | 44.43 | 30.43 | 44.14 | 28.17 | 31.93 | 27.93 | 0.052 |
| Thalamus left | 56.73 | 29.84 | 54.33 | 26.68 | 42.83 | 29.39 | 0.037 |
| Brainstem | 55.91 | 24.97 | 56.35 | 28.32 | 46.25 | 26.65 | 0.106 |
| Mesencephalon | 49.42 | 27.37 | 49.82 | 28.56 | 40.90 | 27.23 | 0.198 |
| Pons | 54.01 | 27.01 | 51.15 | 29.24 | 44.37 | 27.23 | 0.204 |
| Cerebellar grey matter | 68.01 | 24.56 | 70.45 | 25.60 | 60.24 | 27.65 | 0.127 |
| Left ventricle | 54.37 | 31.06 | 48.48 | 29.31 | 56.07 | 27.71 | 0.401 |
| Right ventricle | 54.67 | 31.64 | 51.08 | 29.46 | 56.61 | 29.85 | 0.723 |
| Third ventricle | 48.64 | 29.01 | 43.47 | 29.44 | 59.20 | 27.78 | 0.024 |
| Fourth ventricle | 48.34 | 28.67 | 54.38 | 27.16 | 48.82 | 30.70 | 0.498 |
| Brain Region | Estimate | Standard Error | t-Value | p-Value | |
|---|---|---|---|---|---|
| Whole brain | Age (years) | −2.4107 | 0.6102 | −3.951 | <0.001 |
| Gender (male) | 97.1842 | 21.3302 | 4.556 | <0.001 | |
| COVID-19 Mild | 32.6959 | 18.3726 | 1.780 | 0.077195 | |
| COVID-19 Severe | −36.1273 | 18.8432 | −1.917 | 0.057131 | |
| Height | 4.0755 | 1.0574 | 3.854 | <0.001 | |
| BMI | −0.9211 | 1.1922 | −0.773 | 0.441023 | |
| Multiple R-squared | 0.4932 | p-value | <0.001 | ||
| Grey matter | Age (years) | −2.20669 | 0.33652 | −6.557 | <0.001 |
| Gender (male) | 58.22570 | 11.76448 | 4.949 | <0.001 | |
| COVID-19 Mild | 13.84293 | 10.13324 | 1.366 | 0.17398 | |
| COVID-19 Severe | −28.64409 | 10.39277 | −2.756 | 0.00658 | |
| Height | 1.92446 | 0.58321 | 3.300 | 0.00121 | |
| BMI | 0.05646 | 0.65757 | 0.086 | 0.93169 | |
| Multiple R-squared | 0.5367 | p-value | <0.001 | ||
| Supratentorial | Age (years) | −1.53934 | 0.24475 | −6.289 | <0.001 |
| cerebral | Gender (male) | 39.97339 | 8.55623 | 4.671 | <0.001 |
| cortex | COVID-19 Mild | 5.92185 | 7.36984 | 0.803 | 0.42295 |
| COVID-19 Severe | −19.36262 | 7.55859 | −2.561 | 0.01141 | |
| Height | 1.37947 | 0.42416 | 3.252 | 0.00141 | |
| BMI | −0.41309 | 0.47824 | −0.863 | 0.38911 | |
| Multiple R-squared | 0.5097 | p-value | <0.001 | ||
| Frontal lobe | Age (years) | −0.39890 | 0.04735 | −8.425 | <0.001 |
| right | Gender (male) | 6.96303 | 1.65526 | 4.207 | <0.001 |
| COVID-19 Mild | 1.15013 | 1.42575 | 0.807 | 0.42114 | |
| COVID-19 Severe | −3.92092 | 1.46226 | −2.681 | 0.00816 | |
| Height | 0.25741 | 0.08206 | 3.137 | 0.00206 | |
| BMI | −0.09647 | 0.09252 | −1.043 | 0.29881 | |
| Multiple R-squared | 0.5397 | p-value | <0.001 | ||
| Frontal lobe | Age (years) | −0.35550 | 0.05445 | −6.529 | <0.001 |
| left | Gender (male) | 7.28431 | 1.90364 | 3.827 | <0.001 |
| COVID-19 Mild | 0.42527 | 1.63969 | 0.259 | 0.795716 | |
| COVID-19 Severe | −3.48425 | 1.68168 | −2.072 | 0.040011 | |
| Height | 0.27121 | 0.09437 | 2.874 | 0.004651 | |
| BMI | −0.13552 | 0.10640 | −1.274 | 0.204797 | |
| Multiple R-squared | 0.4524 | p-value | <0.001 | ||
| Parietal lobe | Age (years) | −0.19783 | 0.02668 | −7.414 | <0.001 |
| right | Gender (male) | 3.76298 | 0.93281 | 4.034 | <0.001 |
| COVID-19 Mild | 0.17747 | 0.80347 | 0.221 | 0.8255 | |
| COVID-19 Severe | −2.05789 | 0.82405 | −2.497 | 0.0136 | |
| Height | 0.13298 | 0.04624 | 2.876 | 0.0046 | |
| BMI | −0.00355 | 0.05214 | −0.068 | 0.9458 | |
| Multiple R-squared | 0.4866 | p-value | <0.001 | ||
| Parietal lobe | Age (years) | −0.18253 | 0.02821 | −6.47 | <0.001 |
| left | Gender (male) | 4.09906 | 0.98632 | 4.156 | <0.001 |
| COVID-19 Mild | 0.15045 | 0.84956 | 0.177 | 0.8597 | |
| COVID-19 Severe | −2.4184 | 0.87132 | −2.776 | 0.0062 | |
| Height | 0.13495 | 0.0489 | 2.76 | 0.0065 | |
| BMI | −0.048 | 0.05513 | −0.871 | 0.3853 | |
| Multiple R-squared | 0.4701 | p-value | <0.001 | ||
| Precuneus | Age (years) | −0.0379 | 0.00757 | −5.01 | <0.001 |
| right | Gender (male) | 1.1321 | 0.26447 | 4.281 | <0.001 |
| COVID-19 Mild | 0.16744 | 0.2278 | 0.735 | 0.4635 | |
| COVID-19 Severe | −0.4825 | 0.23363 | −2.065 | 0.0406 | |
| Height | 0.03398 | 0.01311 | 2.592 | 0.0105 | |
| BMI | 0.00059 | 0.01478 | 0.04 | 0.9682 | |
| Multiple R-squared | 0.4255 | p-value | <0.001 | ||
| Occipital lobe | Age (years) | −0.07167 | 0.04324 | −1.658 | 0.0995 |
| left | Gender (male) | 1.62171 | 1.51154 | 1.073 | 0.2851 |
| COVID-19 Mild | −0.10926 | 1.30195 | −0.084 | 0.9332 | |
| COVID-19 Severe | −2.81361 | 1.3353 | −2.107 | 0.0368 | |
| Height | 0.14092 | 0.07493 | 1.881 | 0.062 | |
| BMI | 0.05991 | 0.08449 | 0.709 | 0.4794 | |
| Multiple R-squared | 0.1398 | p-value | <0.001 | ||
| Thalamus | Age (years) | −0.02283 | 0.00425 | −5.375 | <0.001 |
| right | Gender (male) | 0.3445 | 0.14851 | 2.32 | 0.0217 |
| COVID-19 Mild | 0.20392 | 0.12792 | 1.594 | 0.113 | |
| COVID-19 Severe | −0.33729 | 0.13119 | −2.571 | 0.0111 | |
| Height | 0.0214 | 0.00736 | 2.906 | 0.0042 | |
| BMI | −0.00289 | 0.0083 | −0.348 | 0.7284 | |
| Multiple R-squared | 0.3903 | p-value | <0.001 | ||
| Brainstem | Age (years) | 0.0099 | 0.04076 | 0.243 | 0.8083 |
| Gender (male) | 1.54783 | 1.4248 | 1.086 | 0.2791 | |
| COVID-19 Mild | −1.4237 | 1.22724 | −1.16 | 0.2479 | |
| COVID-19 Severe | −2.84074 | 1.25867 | −2.257 | 0.0255 | |
| Height | 0.15566 | 0.07063 | 2.204 | 0.0291 | |
| BMI | 0.05938 | 0.07964 | 0.746 | 0.4571 | |
| Multiple R-squared | 0.1434 | p-value | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bendella, Z.; Widmann, C.N.; Layer, J.P.; Layer, Y.L.; Haase, R.; Sauer, M.; Bieler, L.; Lehnen, N.C.; Paech, D.; Heneka, M.T.; et al. Brain Volume Changes after COVID-19 Compared to Healthy Controls by Artificial Intelligence-Based MRI Volumetry. Diagnostics 2023, 13, 1716. https://doi.org/10.3390/diagnostics13101716
Bendella Z, Widmann CN, Layer JP, Layer YL, Haase R, Sauer M, Bieler L, Lehnen NC, Paech D, Heneka MT, et al. Brain Volume Changes after COVID-19 Compared to Healthy Controls by Artificial Intelligence-Based MRI Volumetry. Diagnostics. 2023; 13(10):1716. https://doi.org/10.3390/diagnostics13101716
Chicago/Turabian StyleBendella, Zeynep, Catherine Nichols Widmann, Julian Philipp Layer, Yonah Lucas Layer, Robert Haase, Malte Sauer, Luzie Bieler, Nils Christian Lehnen, Daniel Paech, Michael T. Heneka, and et al. 2023. "Brain Volume Changes after COVID-19 Compared to Healthy Controls by Artificial Intelligence-Based MRI Volumetry" Diagnostics 13, no. 10: 1716. https://doi.org/10.3390/diagnostics13101716