
Fetal Health State Detection Using Interval Type-2 Fuzzy Neural Networks

Abstract
:1. Introduction
2. Related Research Works
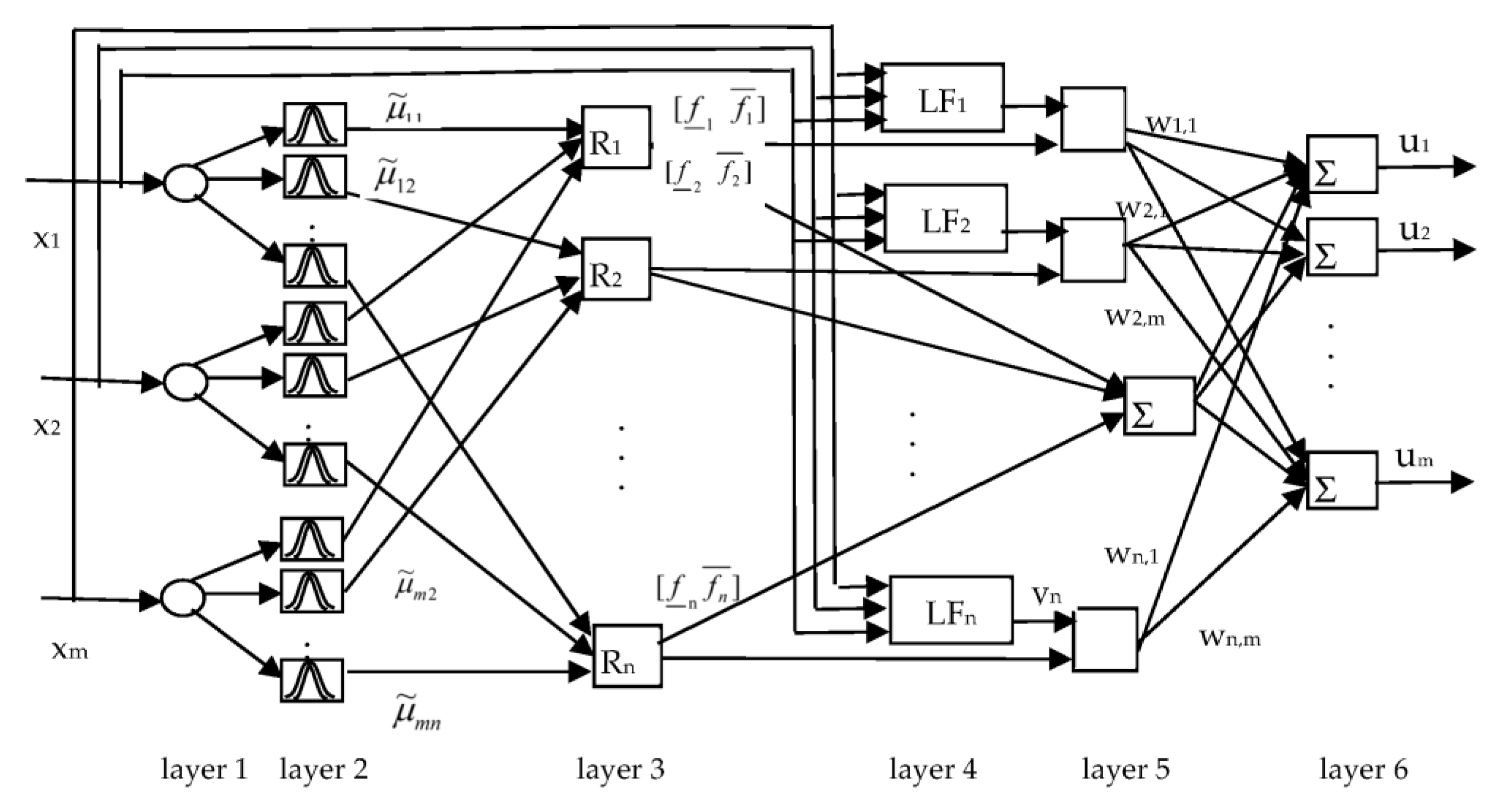
- The T2-FNN system based on the integration of type-2 fuzzy system and neural networks is proposed for the detection of fetal health status.
- The structure of type-2 fuzzy neural networks (T2-FNN) is proposed and the design algorithm of T2-FNN is presented.
- The presented system is implemented for the detection of the fetal health status of pregnant women. The simulation of the proposed system is implemented using statistical data.
- Based on the input–output relationship, novel data preprocessing algorithm is designed and tested on the dataset.
- The proposed T2-FNN system shows better accuracy performance in comparison with other models, which enhanced the effectiveness of the fetal health status detection system.
3. T2-FNN for Detection of Fetal Health Status
| Algorithm 1 The design stages of T2-FNN system |
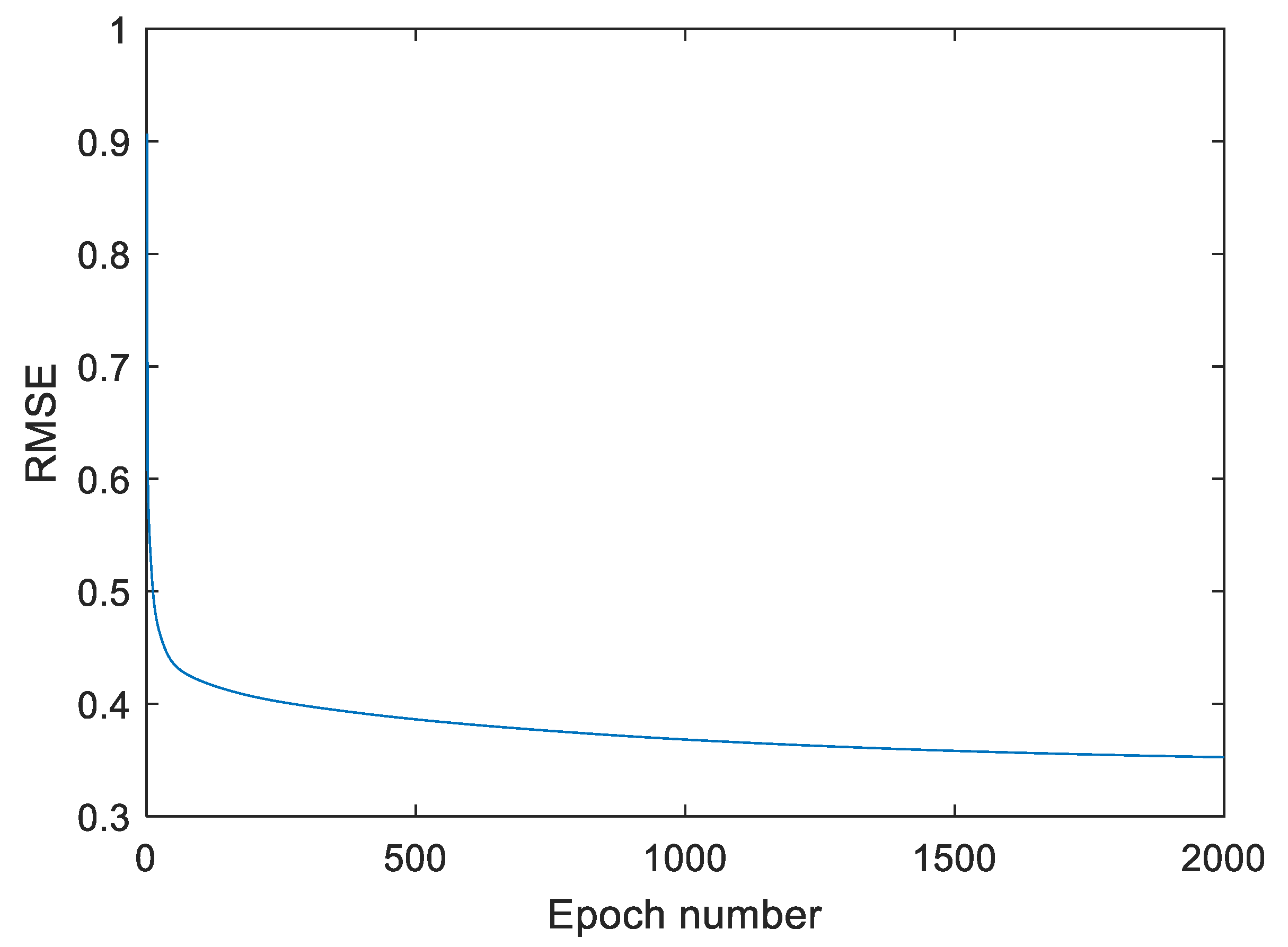
| Input datasets X. Randomly generate initial values of the c1, c2, o parameters of the antecedent part and w1 and w2 parameters of the consequent part of T2FNN. Set maximum epoch number max_epoch, learning rate, momentum rate, number of inputs, hidden and output neurons and learning coefficients. Set fold number K = 10, current epoch number equal epoch = 1. Set initial values of the parameters p = 0.5 and q = 0.5. While epch <= maximum_epoch, do Partition datasets into K groups. For each fold, do Determine training and validation (testing) samples. Determine input–output training pairs. For each input–output training pairs, do For each input data using Formulas (2)–(6), determine the output of the T2-FNN. Using UT2FNN current and Ud desired output signals, calculate the output error e(t) = Ud − UT2FNN of the network. If abs(e(t) > Δ), Then Update c1, c2, o, w1 and w2 parameters of the network. Here (Δ is an acceptable small value). endIf endFor Calculate the mean of square errors (SSE) and root mean square errors (RMSE) for the training data. According to gradient of error, adjust the learning rate Determine input–output validation (testing) pairs For each input–output validation pairs, do For each input validation data using Formulas (2)–(6), determine the output of the T2-FNN. Calculate the output error e(t) = Ud − UT2-FNN of the network. endFor Determine MSE and RMSE values for validation data (evaluation). endFor If the current RMSE value for training data is less than the one obtained in the previous epoch, save the T2FNN parameters in the file. endWhile. |
4. Simulation of the T2-FNN System for Determination of the Fetal Status
4.1. Data Preprocessing
- 1.
- Find a number of output classes nc.
- 2.
- Read the values of input–output variables from the dataset.
- 3.
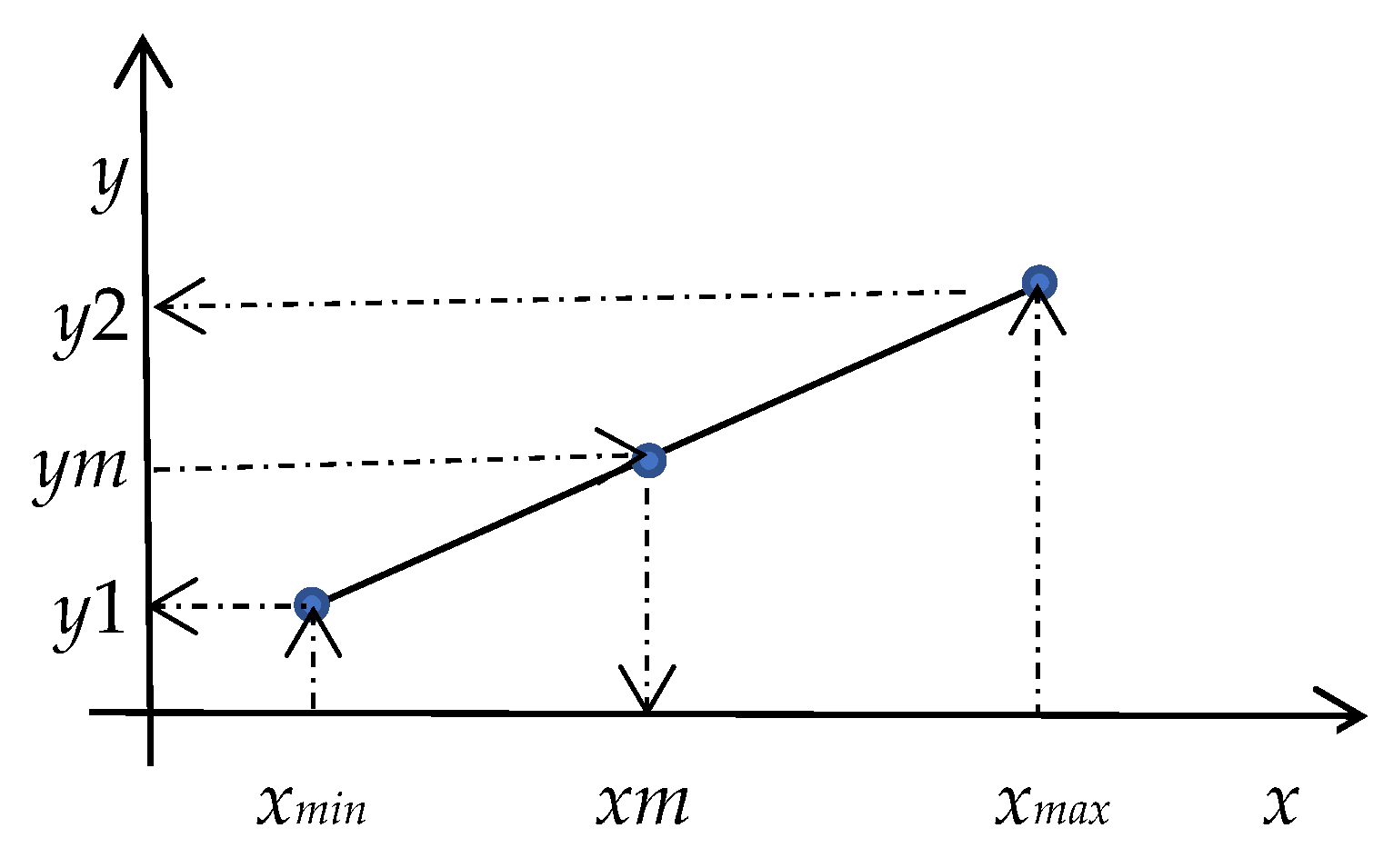
- Find the missing input variable xm and determine its minimum xmin = min(xm) and maximum xmax = max(xm) values.
- 4.
- Determine minimum y1 and maximum y2 values of output classes corresponding to missing input xm variables.
- 5.
- Determine the steps for the missing input and corresponding output variables using formulas and .
- 6.
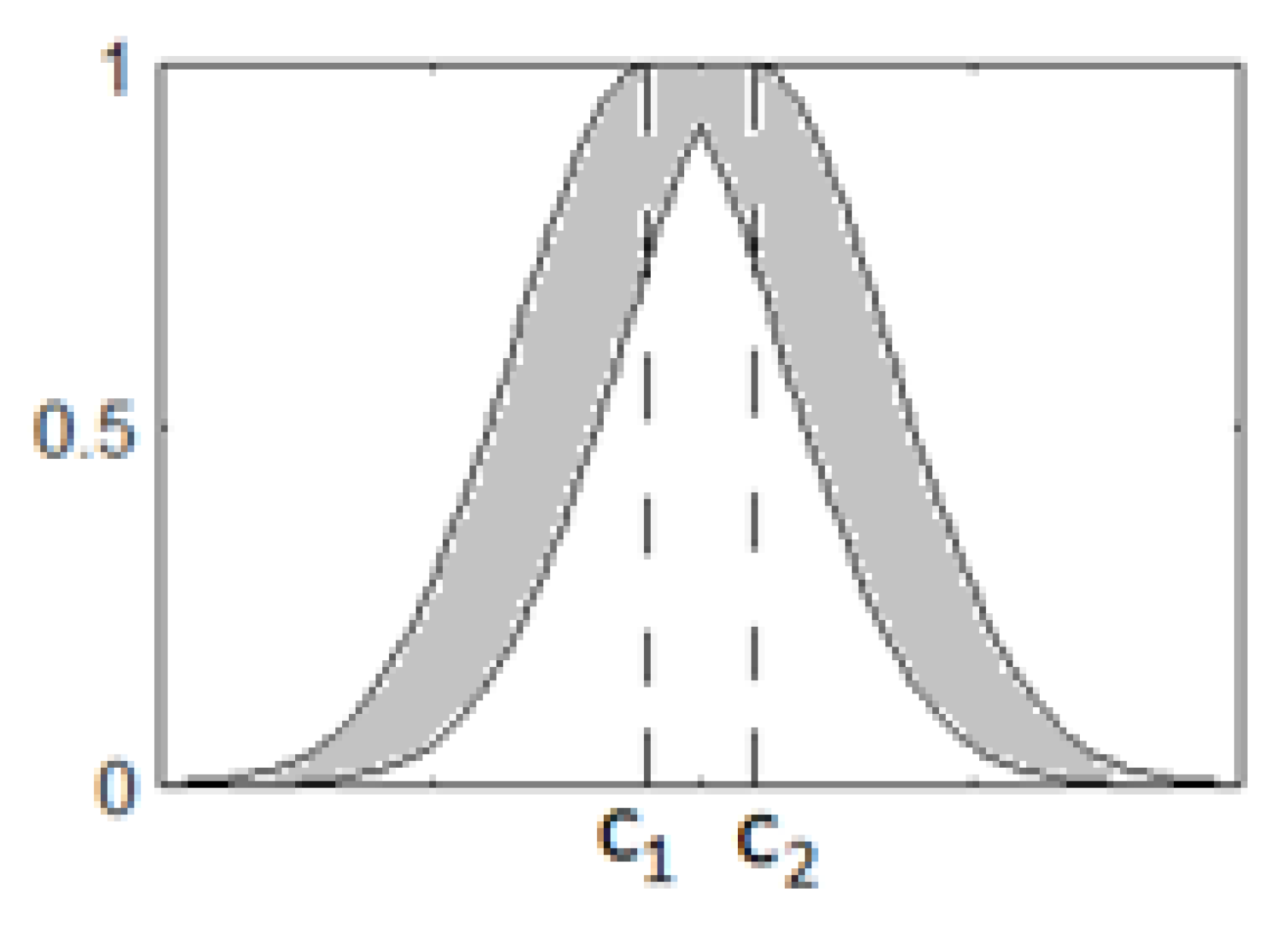
- Using minimum and maximum values, determine cluster centers for the missing input and corresponding output variables using formulasand . Here, k = 1, …, nc, c = 1, …, C. nc is the number of output classes, C is the number of input variables.
- 7.
- Save the and .
- 8.
- Repeat Steps 3–7 for all missing variables.
- 9.
- Read the dataset, find the row that has missing input value xm in the dataset and fix the corresponding output class of this row.
- 10.
- Use (Step 9) and the stored input–output data (Step 7) to find the corresponding input data.
- 11.
- Replace the missing value of xm in the dataset with the value of determined in Step 10.
- 12.
- Repeat Steps 9–11 for all missing values.
4.2. Simulation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Maternal Mortality. Available online: http://www.who.int/mediacentre/factsheets/fs348/en/ (accessed on 24 January 2023).
- What Are Some Common Complications of Pregnancy? National Institutes of Health, US Department of Health and Human Services. Available online: https://www.nichd.nih.gov/health/topics/pregnancy/conditioninfo/complications (accessed on 24 January 2023).
- Ingemarsson, I. Fetal monitoring during labor. Neonatology 2009, 95, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Jezewski, M.; Czabanski, R.; Wrobel, J.; Horoba, K. Analysis of extracted cardiotocographic signal features to improve automated prediction of fetal outcome. Biocybern. Biomed. Eng. 2010, 30, 29–47. [Google Scholar]
- Zadeh, L.A. Fuzzy sets. Inf. Control 1965, 8, 338–353. [Google Scholar] [CrossRef] [Green Version]
- Ghesu, F.C.; Krubasik, E.; Georgescu, B.; Singh, V.; Zheng, Y.; Hornegger, J.; Comaniciu, D. Marginal space deep learning: Efficient architecture for volumetric image parsing. IEEE Trans. Med. Imaging 2016, 35, 1217–1228. [Google Scholar] [CrossRef]
- Deepika, P.; Suresh, R.M.; Pabitha, P. Defending against child death: Deep learning-based diagnosis method for abnormal identification of fetus ultrasound Images. Comput. Intell. 2020, 37, 128–154. [Google Scholar] [CrossRef]
- Lin, Z.; Li, S.; Ni, D.; Liao, Y.; Wen, H.; Du, J.; Chen, S.; Wang, T.; Lei, B. Multi-task learning for quality assessment of fetal head ultrasound images. Med. Image Anal. 2019, 58, 101548. [Google Scholar] [CrossRef]
- Arif, M. Classification of cardiotocograms using random forest classifier and selection of important features from cardiotocogram signal. Biomater. Biomech. Bioeng. 2015, 2, 173–183. [Google Scholar] [CrossRef]
- Signorini, M.G.; Pini, N.; Malovini, A.; Bellazzi, R.; Magenes, G. Integrating machine learning techniques and physiology-based heart rate features for antepartum fetal monitoring. Comput. Methods Programs Biomed. 2020, 185, 105015. [Google Scholar] [CrossRef]
- Sharanya, S.; Venkataraman, R. An intelligent context-based multi-layered Bayesian inferential, predictive analytic framework for classifying machine states. J. Ambient. Intell. Humaniz. Comput. 2020, 12, 7353–7361. [Google Scholar]
- Cömert, Z.; S¸engür, A.; Budak, Ü.; Kocamaz, A.F. Prediction of intrapartum fetal hypoxia considering feature selection algorithms and machine learning models. Health Inf. Sci. Syst. 2019, 7, 17. [Google Scholar] [CrossRef]
- Sharma, P.; Sharma, K. Fetal state health monitoring using novel Enhanced Binary Bat Algorithm. Comput. Electr. Eng. 2022, 101, 108035. [Google Scholar] [CrossRef]
- Subasia, A.; Kadasa, B.; Kremic, E. Classification of the Cardiotocogram Data for Anticipation of Fetal Risks using Bagging Ensemble Classifier. Procedia Comput. Sci. 2020, 168, 34–39. [Google Scholar] [CrossRef]
- Agrawal, K.; Mohan, H. Cardiotocography Analysis for Fetal State Classification Using Machine Learning Algorithms. In Proceedings of the 2019 International Conference on Computer Communication and Informatics (ICCCI-2019), Coimbatore, India, 23–25 January 2019. [Google Scholar]
- Mehbodniya, A.; Lazar, A.J.P.; Webber, J.; Sengan, S. Fetal health classification from cardiotocographic data using machine learning. Expert Syst. 2022, 39, 3. [Google Scholar] [CrossRef]
- Hoodbhoy, Z.; Noman, M.; Shafique, A.; Nasim, A.; Chowdhury, D.; Hasan, B. Use of Machine Learning Algorithms for Prediction of Fetal Risk using Cardiotocographic Data. Int. J. Appl. Basic Med. Res. 2019, 9, 226–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akbulut, A.; Ertugrul, E.; Topcu, V. Fetal health status prediction based on maternal clinical history using machine learning techniques. Comput. Methods Programs Biomed. 2018, 163, 87–100. [Google Scholar] [CrossRef] [PubMed]
- Spilka, J.; Georgoulas, G.; Karvelis, P.; Oikonomou, V.P.; Chudacek, V.; Stylios, C.; Lhostka, L.; Janku, P. Automatic Evaluation of FHR Recordings from CTU-UHB CTG Database. In Information Technology in Bio- and Medical Informatics, ITBAM 2013; Lecture Notes in Computer Science; Bursa, M., Khuri, S., Renda, M.E., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; Volume 8060. [Google Scholar] [CrossRef]
- Oikonomou, V.P.; Spilka, J.; Stylios, C.; Lhostka, L. An adaptive method for the recovery of missing samples from FHR time series. In Proceedings of the 26th IEEE International Symposium on Computer-Based Medical Systems, Porto, Portugal, 20–22 June 2013; pp. 337–342. [Google Scholar] [CrossRef]
- Azeez, N.; Towolawi, T.; Vyver, C.V.D.; Misra, S.; Adewumi, A.; Damaševičius, R.; Ahuja, R. A Fuzzy Expert System for Diagnosing and Analyzing Human Diseases. In Innovations in Bio-Inspired Computing and Applications. IBICA 2018. Advances in Intelligent Systems and Computing; Abraham, A., Gandhi, N., Pant, M., Eds.; Springer: Cham, Switzerland, 2018; Volume 939. [Google Scholar] [CrossRef]
- Bressan, G.M.; Flamia De Azevedo, B.C.; Molina De Souza, R. A Fuzzy Approach for Diabetes Mellitus Type 2 Classification. Brazilian Arch. Biol. Technol. 2020, 63, e20180742. [Google Scholar] [CrossRef]
- Thandra, J.; Sharief Basha, S. Artificial Intelligence (AI) Model: Adaptive Neuro-Fuzzy Inference System (ANFIS) for Diagnosis of COVID-19 Influenza. Comput. Inform. 2022, 41, 1114–1135. [Google Scholar] [CrossRef]
- Feng, T.C.; Li TH, S.; Kuo, P.H. Variable coded hierarchical fuzzy classification model using DNA coding and evolutionary programming. Appl. Math. Model. 2015, 39, 7401–7419. [Google Scholar] [CrossRef]
- Ejegwa, P.A.; Onyeke, I.C.; Adah, V. A pythagorean fuzzy algorithm embedded with a new correlation measure and its application in diagnostic processes. Granul. Comput. 2021, 6, 1037–1046. [Google Scholar] [CrossRef]
- Mendel, J.M. Uncertain Rule-Based Fuzzy Systems. In Introduction and New Directions, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar] [CrossRef]
- Abiyev, R.; Abizada, S. Type-2 fuzzy wavelet neural network for estimation energy performance of residential buildings. Soft Comput. 2021, 25, 11175–11190. [Google Scholar] [CrossRef]
- Castillo, O.; Melin, P. Type-2 Fuzzy Logic: Theory and Applications. Stud. Fuzziness Soft Comput. 2008, 223, 241. [Google Scholar] [CrossRef]
- Biglarbegian, M.; Melek, W.W.; Mendel, J.M. On the stability of interval type-2 tsk fuzzy logic control systems. IEEE Trans. Syst. Man. Cybern. Part B Cybern. 2010, 40, 798–818. [Google Scholar] [CrossRef] [PubMed]
- Abiyev, R.H. A Type-2 Fuzzy Wavelet Neural Network for Time Series Prediction. In Trends in Applied Intelligent Systems. IEA/AIE 2010; García-Pedrajas, N., Herrera, F., Fyfe, C., Benítez, J.M., Ali, M., Eds.; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2010; Volume 6098. [Google Scholar] [CrossRef]
- Abiyev, R.H.; Altiparmak, H. Type-2 Fuzzy Neural System for Diagnosis of Diabetes. Math. Probl. Eng. 2021, 2021, 5854966. [Google Scholar] [CrossRef]
- Goharimanesh, M.; Lashkaripour, A.; Akbari, A. A Comparison of Fuzzy Types 1 and 2 in Diabetics Control, Based on Augmented Minimal Model. J. World Elec. Eng. Tech. 2015, 4, 70–75. [Google Scholar]
- Almansour, N.A.; Syed, H.F.; Khayat, N.R.; Altheeb, R.K.; Juri, R.E.; Alhiyafi, J.; Alrashed, S.; Olatunji, S.O. Neural network and support vector machine for the prediction of chronic kidney disease: A comparative study. Comput. Biol. Med. 2019, 109, 101–111. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Attribute | Description |
|---|---|
| BV | FHR baseline value—beats per min |
| AC | No. of accelerations per sec |
| FM | No. of fetal movement |
| UC | No. of uterine contractions per sec |
| LD | No. of light decelerations per sec |
| SD | No. of severe decelerations per sec |
| PD | No. of prolonged decelerations per sec |
| ASTV | Percentage of time with abnormal short-term variability |
| MSTV | Mean Value of Short-Term Variability |
| ALTV | Percentage of Time with Abnormal Long-Term Variability |
| MLTV | Mean Value of Long-Term Variability |
| HW | Histogram Width (width of FHR histogram) |
| HMax | Histogram Max (maximum of FHR histogram) |
| Hmin | Histogram Min (minimum of FHR histogram) |
| NP | Number of Histogram Peaks |
| NZ | Number of Histogram Zeroes |
| HMo | Histogram Mode |
| HMe | Histogram Mean |
| HMed | Histogram Median |
| HV | Histogram Variance |
| HT | Histogram Tendency |
| NSP | Fetal Health (Fetal state class code, N = normal, S = Suspected, P = Pathological) |
| 151.0 | … | 64.0 | 1.9 | 9.0 | 27.6 | 130.0 | 56.0 | 186.0 | 2.0 | 0.0 | 150.0 | 148.0 | 151.0 | 9.0 | 1.0 | 2.0 |
| 150.0 | … | 64.0 | 2.0 | 8.0 | 29.5 | 130.0 | 56.0 | 186.0 | 5.0 | 0.0 | 150.0 | 148.0 | 151.0 | 10.0 | 1.0 | 2.0 |
| 131.0 | … | 28.0 | 1.4 | 0.0 | 12.9 | 66.0 | 88.0 | 154.0 | 5.0 | 0.0 | 135.0 | 134.0 | 137.0 | 7.0 | 1.0 | 1.0 |
| 131.0 | … | 28.0 | 1.5 | 0.0 | 5.4 | 87.0 | 71.0 | 158.0 | 2.0 | 0.0 | 141.0 | 137.0 | 141.0 | 10.0 | 1.0 | 1.0 |
| 130.0 | … | 21.0 | 2.3 | 0.0 | 7.9 | 107.0 | 67.0 | 174.0 | 7.0 | 0.0 | 143.0 | 125.0 | 135.0 | 76.0 | 0.0 | 1.0 |
| 130.0 | … | 19.0 | 2.3 | 0.0 | 8.7 | 107.0 | 67.0 | 174.0 | 3.0 | 0.0 | 134.0 | 127.0 | 133.0 | 43.0 | 0.0 | 1.0 |
| 130.0 | … | 24.0 | 2.1 | 0.0 | 10.9 | 125.0 | 53.0 | 178.0 | 5.0 | 0.0 | 143.0 | 128.0 | 138.0 | 70.0 | 1.0 | 1.0 |
| Input Variables | Mean | Std | Min | Max |
|---|---|---|---|---|
| baseline value | 133.303857 | 9.840844 | 106.0 | 160.0 |
| accelerations | 0.003178 | 0.003866 | 0.0 | 0.019 |
| fetal_movement | 0.009481 | 0.046666 | 0.0 | 0.481 |
| uterine_contractions | 0.004366 | 0.002946 | 0.0 | 0.015 |
| light_decelerations | 0.001889 | 0.002960 | 0.0 | 0.015 |
| severe_decelerations | 0.000003 | 0.000057 | 0.0 | 0.001 |
| prolongued_decelerations | 0.000159 | 0.000590 | 0.0 | 0.005 |
| abnormal_short_term_variability | 46.990122 | 17.192814 | 12.0 | 87.000 |
| mean_value_of_short_term_variability | 1.332785 | 0.883241 | 0.2 | 7.000 |
| percentage_of_time_with_abnormal_long_term_variability | 9.846660 | 18.396880 | 0.0 | 91.000 |
| mean_value_of_long_term_variability | 8.187629 | 5.628247 | 0.0 | 50.700 |
| histogram_width | 70.445908 | 38.955693 | 3.0 | 180.000 |
| histogram_min | 93.579492 | 29.560212 | 50.0 | 159.000 |
| histogram_max | 164.025400 | 17.944183 | 122.0 | 238.000 |
| histogram_number_of_peaks | 4.068203 | 2.949386 | 0.0 | 18.000 |
| histogram_number_of_zeroes | 0.323612 | 0.706059 | 0.0 | 10.000 |
| histogram_mode | 137.452023 | 16.381289 | 60.0 | 187.000 |
| histogram_mean | 134.610536 | 15.593596 | 73.0 | 182.000 |
| histogram_median | 138.090310 | 14.466589 | 77.0 | 186.000 |
| histogram_variance | 18.80809 | 28.977636 | 0.0 | 269.000 |
| histogram_tendency | 0.320320 | 0.610829 | −1.0 | 1.000 |
| fetal_health | 1.304327 | 0.614377 | 1.0 | 3.000 |
| No | Training Error | Validation Error | Test Error | Accuracy | Precision | Recall | F1 Score |
|---|---|---|---|---|---|---|---|
| 21 | 0.393879 | 0.409894 | 0.407634 | 0.936 | 0.9036 | 0.9038 | 0.9038 |
| 42 | 0.351097 | 0.361881 | 0.361453 | 0.958 | 0.9375 | 0.9375 | 0.9375 |
| 63 | 0.318810 | 0.323347 | 0.322312 | 0.966 | 0.9518 | 0.9518 | 0.9518 |
| Method | Accuracy | Precision | Recall | F-1 Score |
|---|---|---|---|---|
| Logistic Regression | 0.89 | 0.87 | 0.88 | 0.87 |
| Gaussian Naive Bayes | 0.79 | 0.86 | 0.80 | 0.82 |
| SVC | 0.88 | 0.88 | 0.88 | 0.88 |
| RBF SVC | 0.90 | 0.91 | 0.91 | 0.91 |
| ANN | 0.91 | 0.91 | 0.92 | 0.91 |
| CART | 0.93 | 0.93 | 0.93 | 0.93 |
| Random Forest | 0.94 | 0.94 | 0.94 | 0.94 |
| CatBoost | 0.93 | 0.94 | 0.94 | 0.94 |
| RNN | 0.92 | 0.92 | 0.92 | 0.91 |
| T2-FNN (21 rules) | 0.936 | 0.904 | 0.904 | 0.904 |
| T2-FNN (42 rules) | 0.958 | 0.94 | 0.94 | 0.94 |
| T2-FNN (63 rules) | 0.966 | 0.95 | 0.95 | 0.95 |
| The Research Works | Methodology | Accuracy |
|---|---|---|
| Sharma P [12] | Decision Tree | 92.63 |
| Sharma P [12] | K-NN | 92.78 |
| Sharma P [12] | Random Forest | 93.57 |
| Agrawal [14] | Decision Tree | 91.54 |
| Agrawal [14] | SVM | 92.39 |
| Agrawal [14] | Naïve Bayes | 85.572 |
| Mehbodniya [15] | K-NN | 91.23 |
| Mehbodniya [15] | SVM | 93 |
| Mehbodniya [15] | MLP | 92.53 |
| Mehbodniya [15] | Random Forest | 94.5 |
| Current Research | T2-FNN (21 rules) | 93.6 |
| Current Research | T2-FNN (42 rules) | 95.8 |
| Current Research | T2-FNN (63 rules) | 96.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abiyev, R.; Idoko, J.B.; Altıparmak, H.; Tüzünkan, M. Fetal Health State Detection Using Interval Type-2 Fuzzy Neural Networks. Diagnostics 2023, 13, 1690. https://doi.org/10.3390/diagnostics13101690
Abiyev R, Idoko JB, Altıparmak H, Tüzünkan M. Fetal Health State Detection Using Interval Type-2 Fuzzy Neural Networks. Diagnostics. 2023; 13(10):1690. https://doi.org/10.3390/diagnostics13101690
Chicago/Turabian StyleAbiyev, Rahib, John Bush Idoko, Hamit Altıparmak, and Murat Tüzünkan. 2023. "Fetal Health State Detection Using Interval Type-2 Fuzzy Neural Networks" Diagnostics 13, no. 10: 1690. https://doi.org/10.3390/diagnostics13101690