
Correlation between Microvascular Damage and Internal Organ Involvement in Scleroderma: Focus on Lung Damage and Endothelial Dysfunction
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Nailfold Videocapillaroscopy (NVC)
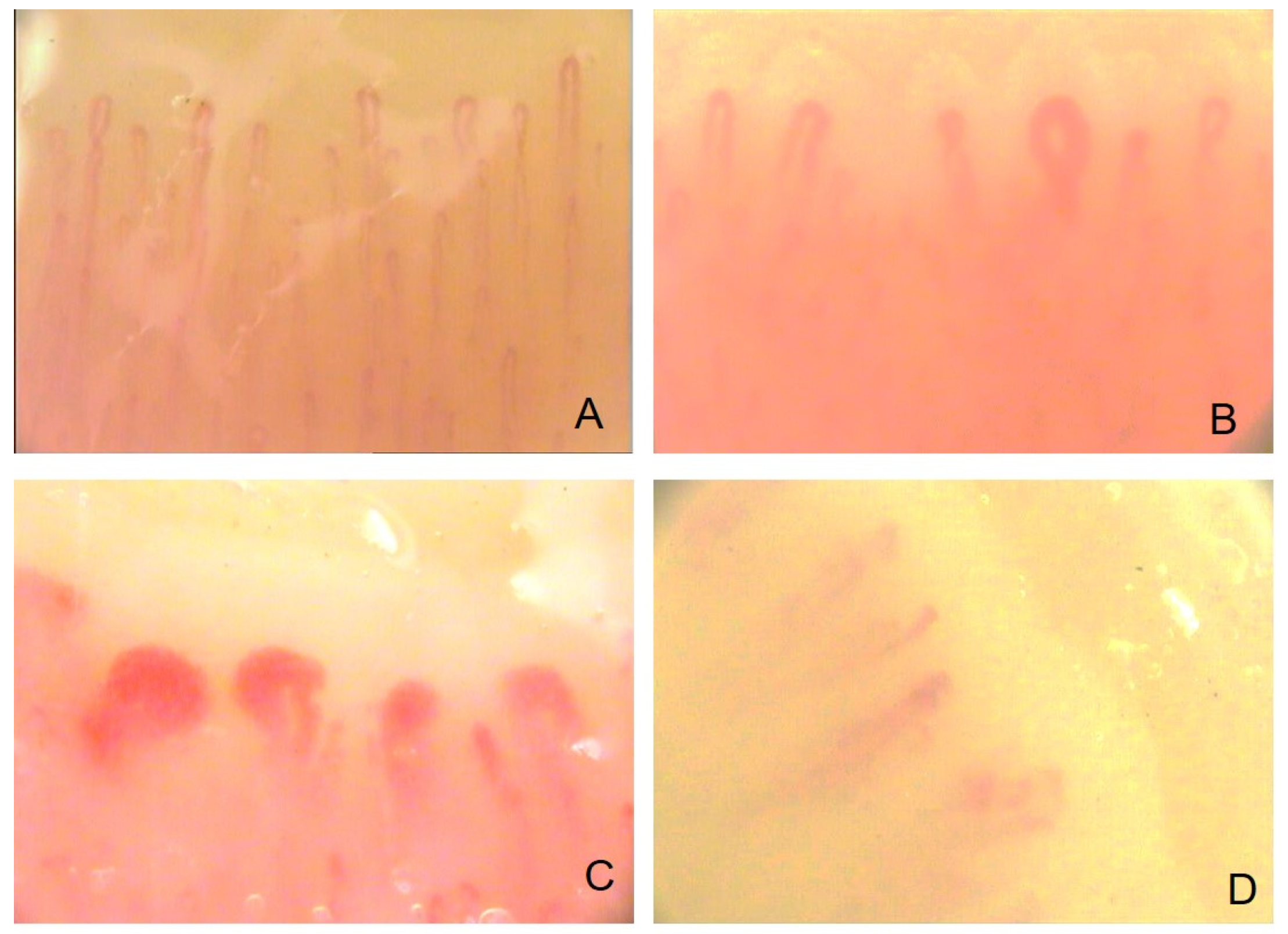
2.1. The Evaluation of Microvascular Damage by NVC
2.2. The NVC Scleroderma Patterns
2.3. The NVC in Systemic Sclerosis: Clinical Application
2.4. The NVC in Systemic Sclerosis: Clinical Application to Lung Impairment
2.5. NVC and Peripheral Blood Flow
3. An Overview of Different Functional Techniques to Evaluate Blood Perfusion
3.1. Laser Doppler Flowmetry
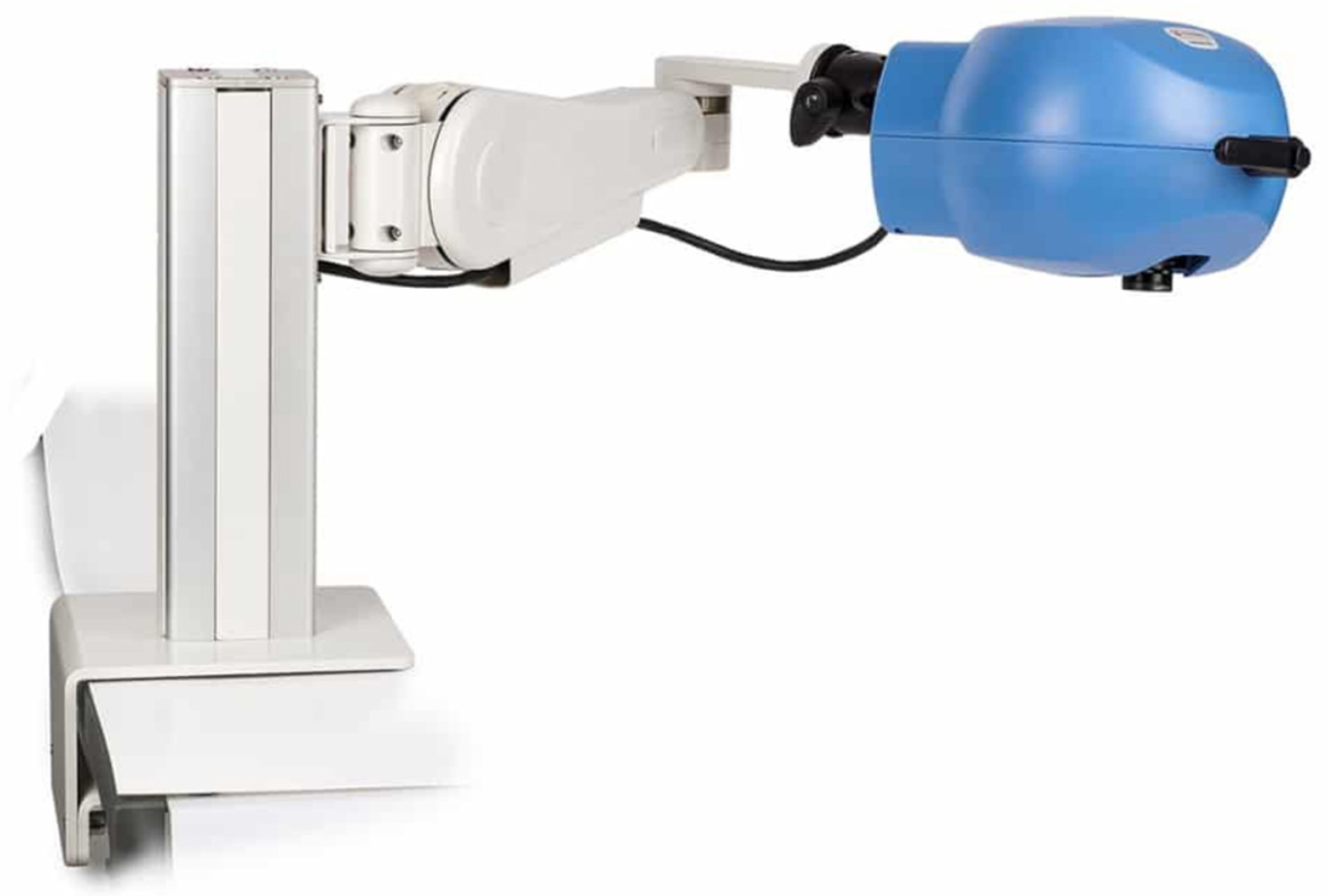
3.2. Laser Doppler Imaging
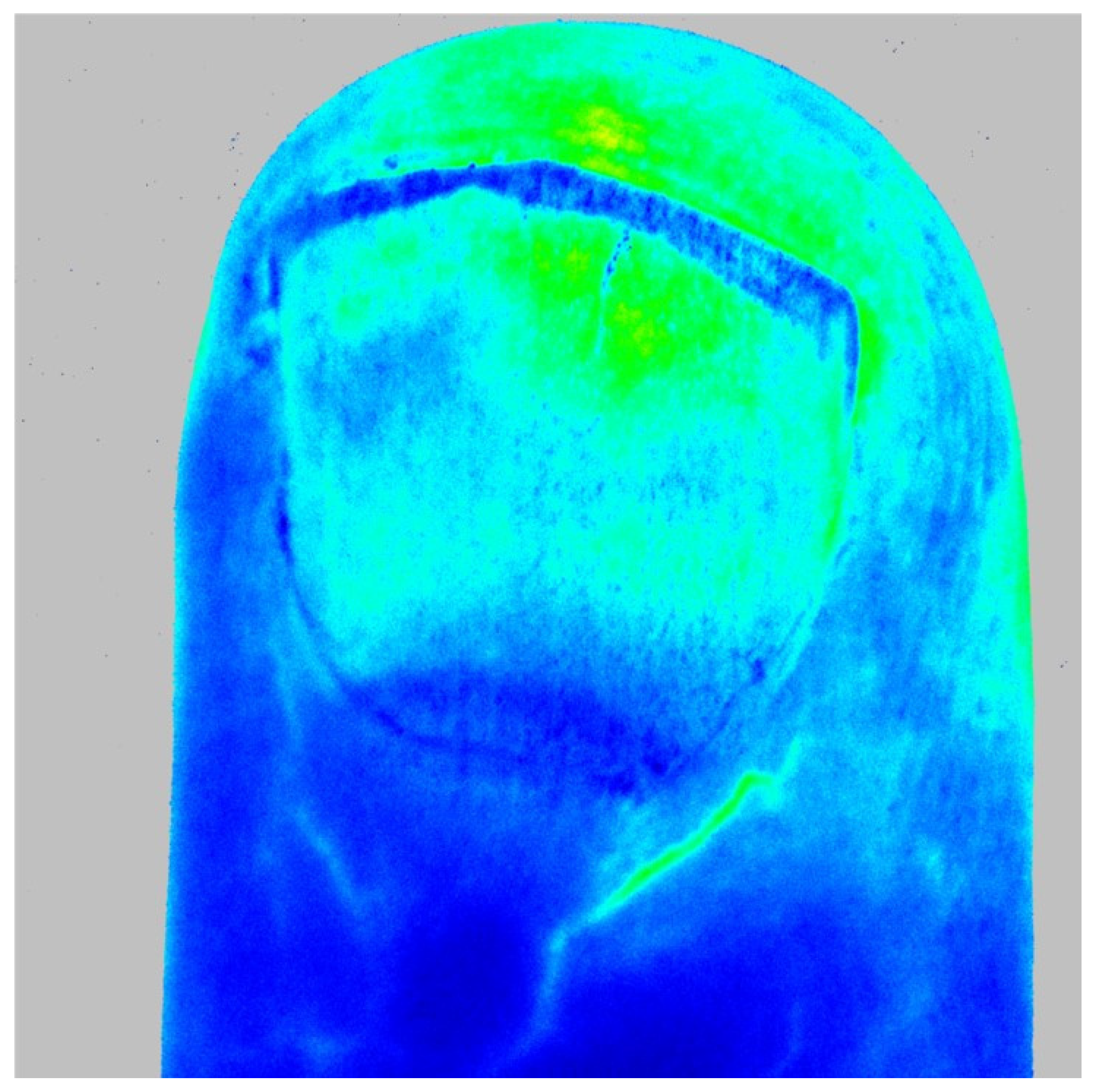
3.3. Laser Speckle Contrast Imaging
3.4. Laser Speckle Contrast Analysis
3.5. Infrared Thermography (IRT)
3.6. The Emerging Role of UltraSound
4. Correlation between NVC and Laser Techniques in the Examination of Peripheral Blood Flow
5. Flow-Mediated Dilation and Assessment of Endothelial Function
6. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Smith, V.; Scirè, C.A.; Talarico, R.; Airo, P.; Alexander, T.; Allanore, Y.; Bruni, C.; Codullo, V.; Dalm, V.; de Vries-Bouwstra, J.; et al. Systemic Sclerosis: State of the Art on Clinical Practice Guidelines. RMD Open 2018, 4, e000782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soulaidopoulos, S.; Triantafyllidou, E.; Garyfallos, A.; Kitas, G.D.; Dimitroulas, T. The Role of Nailfold Capillaroscopy in the Assessment of Internal Organ Involvement in Systemic Sclerosis: A Critical Review. Autoimmun. Rev. 2017, 16, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, M.; Landini, N.; Sambataro, G.; Nardi, C.; Tofani, L.; Bruni, C.; Bellando-Randone, S.; Blagojevic, J.; Melchiorre, D.; Hughes, M.; et al. The Role of Chest CT in Deciphering Interstitial Lung Involvement: Systemic Sclerosis versus COVID-19. Rheumatology 2022, 61, 1600–1609. [Google Scholar] [CrossRef] [PubMed]
- Lambrecht, V.; Cutolo, M.; de Keyser, F.; Decuman, S.; Ruaro, B.; Sulli, A.; Deschepper, E.; Smith, V. Reliability of the Quantitative Assessment of Peripheral Blood Perfusion by Laser Speckle Contrast Analysis in a Systemic Sclerosis Cohort. Ann. Rheum. Dis. 2016, 75, 1263–1264. [Google Scholar] [CrossRef]
- Bernero, E.; Sulli, A.; Ferrari, G.; Ravera, F.; Pizzorni, C.; Ruaro, B.; Zampogna, G.; Alessandri, E.; Cutolo, M. Prospective Capillaroscopy-Based Study on Transition from Primary to Secondary Raynaud’s Phenomenon: Preliminary Results. Reumatismo 2013, 65, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Shirazi, B.R.; Valentine, R.J.; Lang, J.A. Reproducibility and Normalization of Reactive Hyperemia Using Laser Speckle Contrast Imaging. PLoS ONE 2021, 16, e0244795. [Google Scholar] [CrossRef]
- Smith, V.; Beeckman, S.; Herrick, A.L.; Decuman, S.; Deschepper, E.; de Keyser, F.; Distler, O.; Foeldvari, I.; Ingegnoli, F.; Müller-Ladner, U.; et al. An EULAR Study Group Pilot Study on Reliability of Simple Capillaroscopic Definitions to Describe Capillary Morphology in Rheumatic Diseases. Rheumatology 2016, 55, 883–890. [Google Scholar] [CrossRef] [Green Version]
- Murray, A.K.; Moore, T.L.; Manning, J.B.; Taylor, C.; Griffiths, C.E.M.; Herrick, A.L. Noninvasive Imaging Techniques in the Assessment of Scleroderma Spectrum Disorders. Arthritis Rheum. 2009, 61, 1103–1111. [Google Scholar] [CrossRef]
- Sulli, A.; Ruaro, B.; Cutolo, M. Evaluation of Blood Perfusion by Laser Speckle Contrast Analysis in Different Areas of Hands and Face in Patients with Systemic Sclerosis. Ann. Rheum. Dis. 2014, 73, 2059–2061. [Google Scholar] [CrossRef]
- Pizzorni, C.; Sulli, A.; Smith, V.; Lladó, A.; Paolino, S.; Cutolo, M.; Ruaro, B. Capillaroscopy 2016: New Perspectives in Systemic Sclerosis. Acta Reumatol. Port. 2016, 41, 8–14. [Google Scholar]
- Mugii, N.; Hasegawa, M.; Hamaguchi, Y.; Tanaka, C.; Kaji, K.; Komura, K.; Ueda-Hayakawa, I.; Horie, S.; Ikuta, M.; Tachino, K.; et al. Reduced Red Blood Cell Velocity in Nail-Fold Capillaries as a Sensitive and Specific Indicator of Microcirculation Injury in Systemic Sclerosis. Rheumatology 2009, 48, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Distler, O.; Du Four, T.; Cutolo, M. Is There a Role for Nailfold Videocapillaroscopy in Interstitial Lung Disease? Rheumatology 2022, 61, 2217–2220. [Google Scholar] [CrossRef] [PubMed]
- Baratella, E.; Ruaro, B.; Marrocchio, C.; Starvaggi, N.; Salton, F.; Giudici, F.; Quaia, E.; Confalonieri, M.; Cova, M.A. Interstitial Lung Disease at High Resolution CT after SARS-CoV-2-Related Acute Respiratory Distress Syndrome According to Pulmonary Segmental Anatomy. J. Clin. Med. 2021, 10, 3985. [Google Scholar] [CrossRef]
- Pacini, G.; Pogna, A.; Pendolino, M.; Pizzorni, C.; Carmisciano, L.; Gotelli, E.; Sulli, A.; Paolino, S.; Schenone, C.; Smith, V.; et al. Understanding the Value of Non-Specific Abnormal Capillary Dilations in Presence of Raynaud’s Phenomenon: A Detailed Capillaroscopic Analysis. RMD Open 2022, 8, e002449. [Google Scholar] [CrossRef]
- Smith, V.; Pizzorni, C.; Riccieri, V.; Decuman, S.; Brusselle, G.; DE Pauw, M.; Deschepper, E.; Piette, Y.; Ruaro, B.; Sulli, A.; et al. Stabilization of Microcirculation in Patients with Early Systemic Sclerosis with Diffuse Skin Involvement Following Rituximab Treatment: An Open-Label Study. J. Rheumatol. 2016, 43, 995–996. [Google Scholar] [CrossRef] [Green Version]
- Giuggioli, D.; Riccieri, V.; Cipolletta, E.; del Papa, N.; Ingegnoli, F.; Spinella, A.; Pellegrino, G.; Risa, A.M.; de Pinto, M.; Papa, S.; et al. Peripheral Microangiopathy Changes in Pulmonary Arterial Hypertension Related to Systemic Sclerosis: Data from a Multicenter Observational Study. Front. Cardiovasc. Med. 2022, 9, 924899. [Google Scholar] [CrossRef]
- Smith, V.; Vanhaecke, A.; Guerra, M.G.; Melsens, K.; Vandecasteele, E.; Paolino, S.; Cutolo, M. May Capillaroscopy Be a Candidate Tool in Future Algorithms for SSC-ILD: Are We Looking for teve Holy Grail? A Systematic Review. Autoimmun. Rev. 2020, 19, 102619. [Google Scholar] [CrossRef]
- Markusse, I.M.; Meijs, J.; de Boer, B.; Bakker, J.A.; Schippers, H.P.C.; Schouffoer, A.A.; Ajmone Marsan, N.; Kroft, L.J.M.; Ninaber, M.K.; Huizinga, T.W.J.; et al. Predicting Cardiopulmonary Involvement in Patients with Systemic Sclerosis: Complementary Value of Nailfold Videocapillaroscopy Patterns and Disease-Specific Autoantibodies. Rheumatology 2016, 56, 1081–1088. [Google Scholar] [CrossRef] [Green Version]
- Caramaschi, P.; Canestrini, S.; Martinelli, N.; Volpe, A.; Pieropan, S.; Ferrari, M.; Bambara, L.M.; Carletto, A.; Biasi, D. Scleroderma Patients Nailfold Videocapillaroscopic Patterns Are Associated with Disease Subset and Disease Severity. Rheumatology 2007, 46, 1566–1569. [Google Scholar] [CrossRef] [Green Version]
- Ruaro, B.; Smith, V.; Sulli, A.; Decuman, S.; Pizzorni, C.; Cutolo, M. Methods for the Morphological and Functional Evaluation of Microvascular Damage in Systemic Sclerosis. Korean J. Intern. Med. 2015, 30, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lescoat, A.; Coiffier, G.; Rouil, A.; Droitcourt, C.; Cazalets, C.; de Carlan, M.; Perdriger, A.; Jégo, P. Vascular Evaluation of the Hand by Power Doppler Ultrasonography and New Predictive Markers of Ischemic Digital Ulcers in Systemic Sclerosis: Results of a Prospective Pilot Study. Arthritis Care Res. 2017, 69, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Vilela, V.S.; Vanhaecke, A.; da Silva, B.R.A.; da Costa, C.H.; Lopes, A.J.; Rufino, R.; Cutolo, M.; Smith, V. Is There a Link Between Nailfold Videocapillaroscopy and Pulmonary Function Tests in Systemic Sclerosis Patients?: A 24-Month Follow-up Monocentric Study. J. Clin. Rheumatol. 2022, 28, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Ruaro, B.; Confalonieri, M.; Salton, F.; Wade, B.; Baratella, E.; Geri, P.; Confalonieri, P.; Kodric, M.; Biolo, M.; Bruni, C. The Relationship between Pulmonary Damage and Peripheral Vascular Manifestations in Systemic Sclerosis Patients. Pharmaceuticals 2021, 14, 403. [Google Scholar] [CrossRef]
- Smith, V.; Riccieri, V.; Pizzorni, C.; Decuman, S.; Deschepper, E.; Bonroy, C.; Sulli, A.; Piette, Y.; de Keyser, F.; Cutolo, M.; et al. Nailfold Capillaroscopy for Prediction of Novel Future Severe Organ Involvement in Systemic Sclerosis. J. Rheumatol. 2013, 40, 2023–2028. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Vanhaecke, A.; Vandecasteele, E.; Guerra, M.; Paolino, S.; Melsens, K.; Cutolo, M. Nailfold Videocapillaroscopy in Systemic Sclerosis–Related Pulmonary Arterial Hypertension: A Systematic Literature Review. J. Rheumatol. 2020, 47, 888–895. [Google Scholar] [CrossRef]
- Riccieri, V.; Vasile, M.; Iannace, N.; Stefanantoni, K.; Sciarra, I.; Vizza, C.D.; Badagliacca, R.; Poscia, R.; Papa, S.; Mezzapesa, M.; et al. Systemic Sclerosis Patients with and without Pulmonary Arterial Hypertension: A Nailfold Capillaroscopy Study. Rheumatology 2013, 52, 1525–1528. [Google Scholar] [CrossRef] [Green Version]
- Pigatto, E.; Peluso, D.; Zanatta, E.; Polito, P.; Miatton, P.; Bourji, K.; Badano, L.P.; Punzi, L.; Cozzi, F. Evaluation of Right Ventricular Function Performed by 3D-Echocardiography in Scleroderma Patients. Reumatismo 2015, 66, 259–263. [Google Scholar] [CrossRef] [Green Version]
- Del Guillén-Castillo, A.; Simeón-Aznar, C.P.; Callejas-Moraga, E.L.; Tolosa-Vilella, C.; Alonso-Vila, S.; Fonollosa-Pla, V.; Selva-O’Callaghan, A. Quantitative Videocapillaroscopy Correlates with Functional Respiratory Parameters: A Clue for Vasculopathy as a Pathogenic Mechanism for Lung Injury in Systemic Sclerosis. Arthritis Res. Ther. 2018, 20, 281. [Google Scholar] [CrossRef] [Green Version]
- Caetano, J.; Paula, F.S.; Amaral, M.; Oliveira, S.; Alves, J.D. Nailfold Videocapillaroscopy Changes Are Associated with the Presence and Severity of Systemic Sclerosis-Related Interstitial Lung Disease. J. Clin. Rheumatol. 2019, 25, e12–e15. [Google Scholar] [CrossRef]
- Xia, Z.; Wang, G.; Xiao, H.; Guo, S.; Liu, Y.; Meng, F.; Liu, D.; Li, G.; Zong, L. Diagnostic Value of Nailfold Videocapillaroscopy in Systemic Sclerosis Secondary Pulmonary Arterial Hypertension: A Meta-Analysis. Intern. Med. J. 2018, 48, 1355–1359. [Google Scholar] [CrossRef]
- Meier, F.; Geyer, M.; Tiede, H.; Rieth, A.; Ghofrani, H.A.; Müller-Ladner, U.; Dinser, R.; Hermann, W. Is Nailfold Videocapillaroscopy a Valuable Diagnostic Tool in Pulmonary Hypertension? Eur. Respir. J. 2012, 40, 972. [Google Scholar] [CrossRef]
- Avouac, J.; Lepri, G.; Smith, V.; Toniolo, E.; Hurabielle, C.; Vallet, A.; Amrouche, F.; Kahan, A.; Cutolo, M.; Allanore, Y.; et al. Sequential Nailfold Videocapillaroscopy Examinations Have Responsiveness to Detect Organ Progression in Systemic Sclerosis. Semin. Arthritis Rheum. 2017, 47, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Hofstee, H.M.A.; Vonk Noordegraaf, A.; Voskuyl, A.E.; Dijkmans, B.A.C.; Postmus, P.E.; Smulders, Y.M.; Serné, E.H. Nailfold Capillary Density Is Associated with the Presence and Severity of Pulmonary Arterial Hypertension in Systemic Sclerosis. Ann. Rheum. Dis. 2009, 68, 191–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrado, A.; Correale, M.; Mansueto, N.; Monaco, I.; Carriero, A.; Mele, A.; Colia, R.; Di Biase, M.; Cantatore, F.P. Nailfold Capillaroscopic Changes in Patients with Idiopathic Pulmonary Arterial Hypertension and Systemic Sclerosis-Related Pulmonary Arterial Hypertension. Microvasc. Res. 2017, 114, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.E.; Allen, P.D.; Moore, T.; Hillier, V.; Taylor, C.J.; Herrick, A.L. Computerized Nailfold Video Capillaroscopy--a New Tool for Assessment of Raynaud’s Phenomenon. J. Rheumatol. 2005, 32, 841–848. [Google Scholar] [PubMed]
- Smith, V.; Decuman, S.; Sulli, A.; Bonroy, C.; Piettte, Y.; Deschepper, E.; de Keyser, F.; Cutolo, M. Do Worsening Scleroderma Capillaroscopic Patterns Predict Future Severe Organ Involvement? A Pilot Study. Ann. Rheum. Dis. 2012, 71, 1636–1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaisson, N.F.; Hassoun, P.M. Systemic Sclerosis-Associated Pulmonary Arterial Hypertension. Chest 2013, 144, 1346–1356. [Google Scholar] [CrossRef] [Green Version]
- Hax, V.; Bredemeier, M.; Didonet Moro, A.L.; Pavan, T.R.; Vieira, M.V.; Pitrez, E.H.; da Silva Chakr, R.M.; Xavier, R.M. Clinical Algorithms for the Diagnosis and Prognosis of Interstitial Lung Disease in Systemic Sclerosis. Semin. Arthritis Rheum. 2017, 47, 228–234. [Google Scholar] [CrossRef]
- Karayusuf, L.; Akdoğan, A.; Kılıç, L.; Karadağ, Ö.; Kalyoncu, U.; Apraş Bilgen, Ş.; Ertenli, İ.; Kiraz, S. Evaluation of Association between Capillaroscopic Findings and Organ Involvements in Turkish Systemic Sclerosis Patients. Ulus. Romatoloji Derg. 2014, 6, 48–52. [Google Scholar] [CrossRef]
- Ong, Y.Y.; Nikoloutsopoulos, T.; Bond, C.P.; Smith, M.D.; Ahern, M.J.; Roberts-Thomson, P.J. Decreased Nailfold Capillary Density in Limited Scleroderma with Pulmonary Hypertension. Asian Pac. J. Allergy Immunol. 1998, 16, 81–86. [Google Scholar]
- Hurabielle, C.; Avouac, J.; Lepri, G.; de Risi, T.; Kahan, A.; Allanore, Y. Skin Telangiectasia and the Identification of a Subset of Systemic Sclerosis Patients with Severe Vascular Disease. Arthritis Care Res. 2016, 68, 1021–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dababneh, L.; Cikach, F.; Alkukhun, L.; Dweik, R.A.; Tonelli, A.R. Sublingual Microcirculation in Pulmonary Arterial Hypertension. Ann. Am. Thorac. Soc. 2014, 11, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Ruaro, B.; Casabella, A.; Paolino, S.; Pizzorni, C.; Alessandri, E.; Seriolo, C.; Botticella, G.; Molfetta, L.; Odetti, P.; Smith, V.; et al. Correlation between Bone Quality and Microvascular Damage in Systemic Sclerosis Patients. Rheumatology 2018, 57, 1548–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trombetta, A.C.; Smith, V.; Gotelli, E.; Ghio, M.; Paolino, S.; Pizzorni, C.; Vanhaecke, A.; Ruaro, B.; Sulli, A.; Cutolo, M. Vitamin D Deficiency and Clinical Correlations in Systemic Sclerosis Patients: A Retrospective Analysis for Possible Future Developments. PLoS ONE 2017, 12, e0179062. [Google Scholar] [CrossRef]
- Ruaro, B.; Sulli, A.; Pizzorni, C.; Paolino, S.; Smith, V.; Alessandri, E.; Trombetta, A.C.; Alsheyyab, J.; Cutolo, M. Correlations between blood perfusion and dermal thickness in different skin areas of systemic sclerosis patients. Microvasc. Res. 2018, 115, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Thevissen, K.; Trombetta, A.C.; Pizzorni, C.; Ruaro, B.; Piette, Y.; Paolino, S.; de Keyser, F.; Sulli, A.; Melsens, K.; et al. Nailfold Capillaroscopy and Clinical Applications in Systemic Sclerosis. Microcirculation 2016, 23, 364–372. [Google Scholar] [CrossRef]
- Vanhaecke, A.; Debusschere, C.; Cutolo, M.; Smith, V. The EULAR Study Group on Microcirculation in Rheumatic Diseases Predictive Value of Laser Speckle Contrast Analysis in Systemic Sclerosis. A Systematic Review and Pilot Study. Eur. J. Clin. Investig. 2022, 52, e13672. [Google Scholar] [CrossRef]
- Cutolo, M.; Ferrone, C.; Pizzorni, C.; Soldano, S.; Seriolo, B.; Sulli, A. Peripheral Blood Perfusion Correlates with Microvascular Abnormalities in Systemic Sclerosis: A Laser-Doppler and Nailfold Videocapillaroscopy Study. J. Rheumatol. 2010, 37, 1174–1180. [Google Scholar] [CrossRef]
- Cutolo, M.; Zampogna, G.; Vremis, L.; Smith, V.; Pizzorni, C.; Sulli, A. Longterm Effects of Endothelin Receptor Antagonism on Microvascular Damage Evaluated by Nailfold Capillaroscopic Analysis in Systemic Sclerosis. J. Rheumatol. 2013, 40, 40–45. [Google Scholar] [CrossRef]
- Cutolo, M.; Ruaro, B.; Pizzorni, C.; Ravera, F.; Smith, V.; Zampogna, G.; Paolino, S.; Seriolo, B.; Cimmino, M.; Sulli, A.; et al. Longterm Treatment with Endothelin Receptor Antagonist Bosentan and Iloprost Improves Fingertip Blood Perfusion in Systemic Sclerosis. J. Rheumatol. 2014, 41, 881–886. [Google Scholar] [CrossRef]
- Trombetta, A.C.; Pizzorni, C.; Ruaro, B.; Paolino, S.; Sulli, A.; Smith, V.; Cutolo, M. Effects of Longterm Treatment with Bosentan and Iloprost on Nailfold Absolute Capillary Number, Fingertip Blood Perfusion, and Clinical Status in Systemic Sclerosis. J. Rheumatol. 2016, 43, 2033–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauling, J.D.; Hackett, N.; Guida, A.; Merkel, P.A. Performance of Laser-Derived Imaging for Assessing Digital Perfusion in Clinical Trials of Systemic Sclerosis-Related Digital Vasculopathy: A Systematic Literature Review. Semin. Arthritis Rheum. 2020, 50, 1114–1130. [Google Scholar] [CrossRef] [PubMed]
- Ruaro, B.; Bruni, C.; Wade, B.; Baratella, E.; Confalonieri, P.; Antonaglia, C.; Geri, P.; Biolo, M.; Confalonieri, M.; Salton, F.; et al. Laser Speckle Contrast Analysis: Functional Evaluation of Microvascular Damage in Connective Tissue Diseases. Is There Evidence of Correlations with Organ Involvement, Such as Pulmonary Damage? Front. Physiol. 2021, 12, 710298. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.; Wilkinson, J.; Moore, T.; Manning, J.; New, P.; Dinsdale, G.; Murray, A.; Herrick, A.L. Thermographic Abnormalities Are Associated with Future Digital Ulcers and Death in Patients with Systemic Sclerosis. J. Rheumatol. 2016, 43, 1519–1522. [Google Scholar] [CrossRef]
- Dinsdale, G.; Wilkinson, S.; Wilkinson, J.; Moore, T.L.; Manning, J.B.; Berks, M.; Marjanovic, E.; Dickinson, M.; Herrick, A.L.; Murray, A.K.; et al. State-of-the-Art Technologies Provide New Insights Linking Skin and Blood Vessel Abnormalities in SSc-Related Disorders. Microvasc. Res. 2020, 130, 104006. [Google Scholar] [CrossRef]
- Trombetta, A.C.; Smith, V.; Pizzorni, C.; Meroni, M.; Paolino, S.; Cariti, C.; Ruaro, B.; Sulli, A.; Cutolo, M. Quantitative Alterations of Capillary Diameter Have a Predictive Value for Development of the Capillaroscopic Systemic Sclerosis Pattern. J. Rheumatol. 2016, 43, 599–606. [Google Scholar] [CrossRef]
- Sulli, A.; Ruaro, B.; Smith, V.; Pizzorni, C.; Zampogna, G.; Gallo, M.; Cutolo, M. Progression of Nailfold Microvascular Damage and Antinuclear Antibody Pattern in Systemic Sclerosis. J. Rheumatol. 2013, 40, 634–639. [Google Scholar] [CrossRef]
- Sebastiani, M.; Manfredi, A.; Colaci, M.; D’amico, R.; Malagoli, V.; Giuggioli, D.; Ferri, C. Capillaroscopic Skin Ulcer Risk Index: A New Prognostic Tool for Digital Skin Ulcer Development in Systemic Sclerosis Patients. Arthritis Rheum. 2009, 61, 688–694. [Google Scholar] [CrossRef]
- Smith, V.; de Keyser, F.; Pizzorni, C.; Van Praet, J.T.; Decuman, S.; Sulli, A.; Deschepper, E.; Cutolo, M. Nailfold Capillaroscopy for Day-to-Day Clinical Use: Construction of a Simple Scoring Modality as a Clinical Prognostic Index for Digital Trophic Lesions. Ann. Rheum. Dis. 2011, 70, 180–183. [Google Scholar] [CrossRef]
- Cutolo, M.; Herrick, A.L.; Distler, O.; Becker, M.O.; Beltran, E.; Carpentier, P.; Ferri, C.; Inanç, M.; Vlachoyiannopoulos, P.; Chadha-Boreham, H.; et al. Nailfold Videocapillaroscopic Features and Other Clinical Risk Factors for Digital Ulcers in Systemic Sclerosis: A Multicenter, Prospective Cohort Study. Arthritis Rheumatol. 2016, 68, 2527–2539. [Google Scholar] [CrossRef] [Green Version]
- Cutolo, M. Disease Modification in Systemic Sclerosis. Do Integrated Approaches Offer New Challenges? Z. Rheumatol. 2013, 72, 326–328. [Google Scholar] [CrossRef]
- Cutolo, M.; Sulli, A. Therapy. Optimized Treatment Algorithms for Digital Vasculopathy in SSc. Nat. Rev. Rheumatol. 2015, 11, 569–571. [Google Scholar] [CrossRef]
- Catarsi, E.; Doveri, M.; Tavoni, A. Bosentan and Sildenafil: Successful Treatment in a Sclerodermic Patient with Refractory Ulcers. Reumatismo 2013, 65, 79–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soldano, S.; Montagna, P.; Brizzolara, R.; Ferrone, C.; Parodio, A.; Sulli, A.; Seriolo, B.; Villaggio, B.; Cutolo, M. Endothelin Receptor Antagonists: Effects on Extracellular Matrix Synthesis in Primary Cultures of Skin Fibroblasts from Systemic Sclerosis Patients. Reumatismo 2012, 64, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Casigliani Rabl, S.; Della Rossa, A.; Pepe, P.; D’Ascanio, A.; Mosca, M.; di Vita, A.; Bombardieri, S. Long-Term Cyclic Intravenous Iloprost in Systemic Sclerosis: Clinical Experience from a Single Center. Reumatismo 2012, 64, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Miniati, I.; Guiducci, S.; Conforti, M.L.; Rogai, V.; Fiori, G.; Cinelli, M.; Saccardi, R.; Guidi, S.; Bosi, A.; Tyndall, A.; et al. Autologous Stem Cell Transplantation Improves Microcirculation in Systemic Sclerosis. Ann. Rheum. Dis. 2009, 68, 94–98. [Google Scholar] [CrossRef]
- Guiducci, S.; Bellando Randone, S.; Bruni, C.; Carnesecchi, G.; Maresta, A.; Iannone, F.; Lapadula, G.; Matucci Cerinic, M. Bosentan Fosters Microvascular De-Remodelling in Systemic Sclerosis. Clin. Rheumatol. 2012, 31, 1723–1725. [Google Scholar] [CrossRef] [PubMed]
- Filaci, G.; Cutolo, M.; Scudeletti, M.; Castagneto, C.; Derchi, L.; Gianrossi, R.; Ropolo, F.; Zentilin, P.; Sulli, A.; Murdaca, G.; et al. Cyclosporin A and Iloprost Treatment of Systemic Sclerosis: Clinical Results and Interleukin-6 Serum Changes after 12 Months of Therapy. Rheumatology 1999, 38, 992–996. [Google Scholar] [CrossRef] [Green Version]
- Aschwanden, M.; Daikeler, T.; Jaeger, K.A.; Thalhammer, C.; Gratwohl, A.; Matucci-Cerinic, M.; Tyndall, A. Rapid Improvement of Nailfold Capillaroscopy after Intense Immunosuppression for Systemic Sclerosis and Mixed Connective Tissue Disease. Ann. Rheum. Dis. 2008, 67, 1057–1059. [Google Scholar] [CrossRef]
- Avouac, J.; Fransen, J.; Walker, U.A.; Riccieri, V.; Smith, V.; Muller, C.; Miniati, I.; Tarner, I.H.; Randone, S.B.; Cutolo, M.; et al. Preliminary Criteria for the Very Early Diagnosis of Systemic Sclerosis: Results of a Delphi Consensus Study from EULAR Scleroderma Trials and Research Group. Ann. Rheum. Dis. 2011, 70, 476–481. [Google Scholar] [CrossRef]
- Van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A.; Carreira, P.E.; et al. 2013 Classification Criteria for Systemic Sclerosis: An American College of Rheumatology/European League against Rheumatism Collaborative Initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maverakis, E.; Patel, F.; Kronenberg, D.G.; Chung, L.; Fiorentino, D.; Allanore, Y.; Guiducci, S.; Hesselstrand, R.; Hummers, L.K.; Duong, C.; et al. International Consensus Criteria for the Diagnosis of Raynaud’s Phenomenon. J. Autoimmun. 2014, 48–49, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Medsger, T.A.; Silman, A.J.; Steen, V.D.; Black, C.M.; Akesson, A.; Bacon, P.A.; Harris, C.A.; Jablonska, S.; Jayson, M.I.; Jimenez, S.A.; et al. A Disease Severity Scale for Systemic Sclerosis: Development and Testing. J. Rheumatol. 1999, 26, 2159–2167. [Google Scholar]
- Smith, V.; Vanhaecke, A.; Guerra, M.; Ruaro, B.; Sulli, A.; Vandecasteele, E.; Cutolo, M. Fri0345 Capillaroscopy. In Systemic Sclerosis Related Pulmonary Arterial Hypertension; BMJ Publishing Group Ltd.: London, UK, 2019; ISBN 0003-4967. [Google Scholar]
- Jehangir, M.; Qayoom, S.; Jeelani, S.; Yousuf, R. Nail Fold Capillaroscopy in Patients of Systemic Sclerosis and Its Association with Disease Severity as Evidenced by High Resolution Computed Tomography Lung: A Hospital Based Cross Sectional Study. Int. J. Res. Med. Sci. 2015, 3, 3485–3489. [Google Scholar] [CrossRef] [Green Version]
- Pizzorni, C.; Ruaro, B.; Paolino, S.; Camellino, D.; Cimmino, M.A.; Cutolo, M.; Sulli, A. SAT0215 Twelve Year Follow-Up on Progression of Nailfold Microangiopathy Detected through Transition between Different Capillaroscopic Patterns of Microvascular Damage in Systemic Sclerosis; BMJ Publishing Group Ltd.: London, UK, 2016; ISBN 0003-4967. [Google Scholar]
- Kim, H.S.; Park, M.K.; Kim, H.Y.; Park, S.H. Capillary Dimension Measured by Computer-Based Digitalized Image Correlated with Plasma Endothelin-1 Levels in Patients with Systemic Sclerosis. Clin. Rheumatol. 2010, 29, 247–254. [Google Scholar] [CrossRef]
- D’Angelo, W.A.; Fries, J.F.; Masi, A.T.; Shulman, L.E. Pathologic Observations in Systemic Sclerosis (Scleroderma). A Study of Fifty-Eight Autopsy Cases and Fifty-Eight Matched Controls. Am. J. Med. 1969, 46, 428–440. [Google Scholar] [CrossRef]
- Frech, T.M. Imaging Techniques for Assessment of Vascular Involvement in Systemic Sclerosis. Curr. Opin. Rheumatol. 2022, 34, 311–318. [Google Scholar] [CrossRef]
- Briers, D.; Duncan, D.D.; Hirst, E.; Kirkpatrick, S.J.; Larsson, M.; Steenbergen, W.; Stromberg, T.; Thompson, O.B. Laser Speckle Contrast Imaging: Theoretical and Practical Limitations. J. Biomed. Opt. 2013, 18, 066018. [Google Scholar] [CrossRef] [Green Version]
- Hellmann, M.; Kalinowski, L.; Cracowski, J.L. Laser Speckle Contrast Imaging to Assess Microcirculation. Cardiol. J. 2022, 29, 1028–1030. [Google Scholar] [CrossRef]
- Ruaro, B.; Sulli, A.; Alessandri, E.; Pizzorni, C.; Ferrari, G.; Cutolo, M. Laser Speckle Contrast Analysis: A New Method to Evaluate Peripheral Blood Perfusion in Systemic Sclerosis Patients. Ann. Rheum. Dis. 2014, 73, 1181–1185. [Google Scholar] [CrossRef]
- Ruaro, B.; Sulli, A.; Pizzorni, C.; Paolino, S.; Smith, V.; Cutolo, M. Correlations between Skin Blood Perfusion Values and Nailfold Capillaroscopy Scores in Systemic Sclerosis Patients. Microvasc. Res. 2016, 105, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Ickinger, C.; Lambrecht, V.; Tikly, M.; Vanhaecke, A.; Cutolo, M.; Smith, V. Laser Speckle Contrast Analysis Is a Reliable Measure of Digital Blood Perfusion in Black Africans with Systemic Sclerosis. Clin. Exp. Rheumatol. 2021, 131, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, J.D.; Leggett, S.A.; Marjanovic, E.J.; Moore, T.L.; Allen, J.; Anderson, M.E.; Britton, J.; Buch, M.H.; Del Galdo, F.; Denton, C.P.; et al. A Multicenter Study of the Validity and Reliability of Responses to Hand Cold Challenge as Measured by Laser Speckle Contrast Imaging and Thermography: Outcome Measures for Systemic Sclerosis-Related Raynaud’s Phenomenon. Arthritis Rheumatol. 2018, 70, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Pauling, J.D.; Shipley, J.A.; Raper, S.; Watson, M.L.; Ward, S.G.; Harris, N.D.; McHugh, N.J. Comparison of Infrared Thermography and Laser Speckle Contrast Imaging for the Dynamic Assessment of Digital Microvascular Function. Microvasc. Res. 2012, 83, 162–167. [Google Scholar] [CrossRef]
- Branco, J.H.L.; Branco, R.L.L.; Siqueira, T.C.; de Souza, L.C.; Dalago, K.M.S.; Andrade, A. Clinical Applicability of Infrared Thermography in Rheumatic Diseases: A Systematic Review. J. Therm. Biol. 2022, 104, 103172. [Google Scholar] [CrossRef]
- Wilson, A.C.; Jungbauer, W.N.; Hussain, F.T.; Lindgren, B.R.; Lassig, A.A.D. Characterization of Baseline Temperature Characteristics Using Thermography in The Clinical Setting. J. Surg. Res. 2022, 272, 26–36. [Google Scholar] [CrossRef]
- Pauling, J.D.; Shipley, J.A.; Hart, D.J.; McGrogan, A.; McHugh, N.J. Use of Laser Speckle Contrast Imaging to Assess Digital Microvascular Function in Primary Raynaud Phenomenon and Systemic Sclerosis: A Comparison Using the Raynaud Condition Score Diary. J. Rheumatol. 2015, 42, 1163–1168. [Google Scholar] [CrossRef] [Green Version]
- Miziołek, B.; Lis-Święty, A.; Skrzypek-Salamon, A.; Brzezińska-Wcisło, L. Correlation between the Infrared Thermogram and Microvascular Abnormalities of the Nailfold in Patients with Systemic Sclerosis. Adv. Dermatol. Allergol. Postępy Dermatol. Alergol. 2021, 38, 115–122. [Google Scholar] [CrossRef]
- Staffa, E.; Bernard, V.; Kubíček, L.; Vlachovský, R.; Vlk, D.; Mornstein, V.; Staffa, R. Using Noncontact Infrared Thermography for Long-Term Monitoring of Foot Temperatures in a Patient with Diabetes Mellitus. Ostomy Wound Manag. 2016, 62, 54–61. [Google Scholar]
- Picasso, R.; Bica, P.; Pistoia, F.; Zaottini, F.; Sanguinetti, S.; Bovis, F.; Ponzano, M.; Pizzorni, C.; Paolino, S.; Sulli, A.; et al. High-resolution Doppler Ultrasound in Systemic Sclerosis: Analysis of Digital Arteries and Nailfold Microvasculature Using 18-5 MHz and 33-9 MHz Probes. Int. J. Rheum. Dis. 2022, 25, 1288–1294. [Google Scholar] [CrossRef]
- Schioppo, T.; Orenti, A.; Boracchi, P.; de Lucia, O.; Murgo, A.; Ingegnoli, F. Evidence of Macro- and Micro-Angiopathy in Scleroderma: An Integrated Approach Combining 22-MHz Power Doppler Ultrasonography and Video-Capillaroscopy. Microvasc. Res. 2019, 122, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Rosato, E.; Molinaro, I.; Rossi, C.; Pisarri, S.; Salsano, F. The Combination of Laser Doppler Perfusion Imaging and Photoplethysmography Is Useful in the Characterization of Scleroderma and Primary Raynaud’s Phenomenon. Scand. J. Rheumatol. 2011, 40, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Barsotti, S.; d’Ascanio, A.; Valentina, V.; Chiara, S.; Silvia, B.; Laura, A.; Mosca, M.; Della Rossa, A. Is There a Role for Laser Speckle Contrast Analysis (LASCA) in Predicting the Outcome of Digital Ulcers in Patients with Systemic Sclerosis? Clin. Rheumatol. 2020, 39, 69–75. [Google Scholar] [CrossRef]
- Della Rossa, A.; Cazzato, M.; d’Ascanio, A.; Tavoni, A.; Bencivelli, W.; Pepe, P.; Mosca, M.; Baldini, C.; Rossi, M.; Bombardieri, S. Alteration of Microcirculation Is a Hallmark of Very Early Systemic Sclerosis Patients: A Laser Speckle Contrast Analysis. Clin. Exp. Rheumatol. 2013, 31, 109–114. [Google Scholar] [PubMed]
- Gigante, A.; Villa, A.; Rosato, E. Laser Speckle Contrast Analysis Predicts Major Vascular Complications and Mortality of Patients with Systemic Sclerosis. Rheumatology 2021, 60, 1850–1857. [Google Scholar] [CrossRef]
- Gaillard-Bigot, F.; Roustit, M.; Blaise, S.; Gabin, M.; Cracowski, C.; Seinturier, C.; Imbert, B.; Carpentier, P.; Cracowski, J.L. Abnormal Amplitude and Kinetics of Digital Postocclusive Reactive Hyperemia in Systemic Sclerosis. Microvasc. Res. 2014, 94, 90–95. [Google Scholar] [CrossRef]
- Pyke, K.E.; Tschakovsky, M.E. The Relationship between Shear Stress and Flow-Mediated Dilatation: Implications for the Assessment of Endothelial Function. J. Physiol. 2005, 568, 357–369. [Google Scholar] [CrossRef]
- Tremblay, J.C.; Pyke, K.E. Flow-Mediated Dilation Stimulated by Sustained Increases in Shear Stress: A Useful Tool for Assessing Endothelial Function in Humans? Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H508–H520. [Google Scholar] [CrossRef]
- Harris, R.A.; Nishiyama, S.K.; Wray, D.W.; Richardson, R.S. Ultrasound Assessment of Flow-Mediated Dilation. Hypertension 2010, 55, 1075–1085. [Google Scholar] [CrossRef]
- Markos, F.; Ruane O’Hora, T.; Noble, M.I.M. What Is the Mechanism of Flow-Mediated Arterial Dilatation. Clin. Exp. Pharmacol. Physiol. 2013, 40, 489–494. [Google Scholar] [CrossRef]
- Aizawa, K.; Ramalli, A.; Sbragi, S.; Tortoli, P.; Casanova, F.; Morizzo, C.; Thorn, C.E.; Shore, A.C.; Gates, P.E.; Palombo, C. Arterial Wall Shear Rate Response to Reactive Hyperaemia Is Markedly Different between Young and Older Humans. J. Physiol. 2019, 597, 4151–4163. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Asano, Y.; Amiya, E.; Hatano, M.; Tamaki, Z.; Takata, M.; Ozeki, A.; Watanabe, A.; Kawarasaki, S.; Taniguchi, T.; et al. Clinical Correlation of Brachial Artery Flow-Mediated Dilation in Patients with Systemic Sclerosis. Mod. Rheumatol. 2014, 24, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Frech, T.; Walker, A.E.; Barrett-O’Keefe, Z.; Hopkins, P.N.; Richardson, R.S.; Wray, D.W.; Donato, A.J. Systemic Sclerosis Induces Pronounced Peripheral Vascular Dysfunction Characterized by Blunted Peripheral Vasoreactivity and Endothelial Dysfunction. Clin. Rheumatol. 2015, 34, 905–913. [Google Scholar] [CrossRef] [Green Version]
- Frech, T.M.; Murtaugh, M.A. Non-Invasive Digital Thermal Monitoring and Flow-Mediated Dilation in Systemic Sclerosis. Clin. Exp. Rheumatol. 2019, 37, 97–101. [Google Scholar]
- Roustit, M.; Simmons, G.H.; Baguet, J.P.; Carpentier, P.; Cracowski, J.L. Discrepancy between Simultaneous Digital Skin Microvascular and Brachial Artery Macrovascular Post-Occlusive Hyperemia in Systemic Sclerosis. J. Rheumatol. 2008, 35, 1576–1583. [Google Scholar]
- Szucs, G.; Tímár, O.; Szekanecz, Z.; Dér, H.; Kerekes, G.; Szamosi, S.; Shoenfeld, Y.; Szegedi, G.; Soltész, P. Endothelial Dysfunction Precedes Atherosclerosis in Systemic Sclerosis--Relevance for Prevention of Vascular Complications. Rheumatology 2007, 46, 759–762. [Google Scholar] [CrossRef]
- Soltész, P.; Dér, H.; Kerekes, G.; Szodoray, P.; Szücs, G.; Dankó, K.; Shoenfeld, Y.; Szegedi, G.; Szekanecz, Z. A Comparative Study of Arterial Stiffness, Flow-Mediated Vasodilation of the Brachial Artery, and the Thickness of the Carotid Artery Intima-Media in Patients with Systemic Autoimmune Diseases. Clin. Rheumatol. 2009, 28, 655–662. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Technique | Principle | Skills | Disadvantages | Linked Organ Damage |
|---|---|---|---|---|
| Laser speckle contrast analysis (LASCA) and imaging (LSCI) | When the laser light illuminates the tissue, the static areas result in a stationary speckled pattern, which fluctuates due to the movement of the red blood cells, causing them to appear blurred and thus creating an overall speckled pattern. Based on the level of blurring (contrast), the degree of blood perfusion is determined (low contrast = high perfusion). | -Fast data acquisition -Good spatial resolution (images rich in detail) -Possibility of both spatial (areas) and temporal (dynamic response) evaluations -Non-contact technique -Valid instrument in subjects of Black ethnicity -Decreased PBP at the fingertips, periungual, palmar aspect of third finger and palm areas in SSc patients -After cold test, SSc patients had a significant reduction in blood flow and a higher recovery time compared to HS and PRP -Increase in PBP during long-term therapy with the endothelin receptor antagonist bosentan (BOSE) and the synthetic analog of prostacyclin PGI2 iloprost (ILO) in a 4-years follow up in patients with Sac | Measures perfusion at tissue and skin structure levels (capillaries, arterioles, venules, and shunts). | Microvascular damage in SSc, PAH (assessment of pulmonary damage) |
| Laser Doppler Flowmetry (LDF) | Assesses skin perfusion by measuring the Doppler effect induced by coherent light scattering related to red blood cell movement. | -Heatable fiber optic probe -Can detect both tissue perfusion and skin temperature -Optimal time resolution | -Measurement of blood flow at one point -Lack of reproducibility -Contact technique, limited to probe site -Measurement of local tissue perfusion (capillaries, arterioles, venules, shunts) | Microvascular damage in SSc |
| Laser Doppler Perfusion Imaging (LDPI) | -A laser with a standard output wavelength (color) directed against a diffusion medium such as skin or blood -A Doppler shift (color change) is induced by moving objects, such as blood cells, in scattered light | -Measurement of blood flow of an entire area -Non-contact technique -Good reproducibility | -Slow data acquisition -Measurement of skin perfusion (capillaries, arterioles, venules, and shunts) -Poor temporal resolution | PRP and vascular involvement in SSc |
| Thermography | Indirect measurement of blood flow | Non-contact technique | Indirect measurement of blood flow | Microvascular damage in SSc |
| Near infrared spectroscopy 2D imaging (NIRS-2D) | -Assess regional tissue oxygenation and microvascular function, in conjunction with vascular occlusion testing | -Non-invasive technique -Evaluation of vascular function by measuring blood flow | -Indirect measurement of blood flow -Low spatial resolution and poor sensitivity | Microvascular damage in SSc |
| Photoplethysmography (PPG) | It uses infrared light to measure changes in blood volume | Non-invasive technique | Its application in Raynaud’s phenomenon to evaluate digital artery response to cold test and medications has so far been limited | Microvascular damage in SSc |
| Infrared thermography (IRT) | Through digital thermal cameras, it records and quantifies the skin thermoregulation process, evaluating digital perfusion. | Predictor of higher probability of developing DU and need of surgical debridement | It requires careful monitoring of acclimatization time, camera-to-individual distance, ambient temperature, and humidity, as well as proper subject characterization. | Evaluation of PRP in patients with SSc |
| Nailfold videocapillaroscopy (NVC) | Method for an early diagnosis and follow up of nailfold microangiopathy combining a microscope (with a 5-million-pixels system) and a digital video camera. | Noninvasive, safe, inexpensive, reproducible, and validated method to assess morphological impairment in SSc | Need for further investigation | Microvascular damage in SSc and efficacy of treatment, PAH, ILD (assessment of pulmonary damage and heart involvement) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Oria, M.; Gandin, I.; Riccardo, P.; Hughes, M.; Lepidi, S.; Salton, F.; Confalonieri, P.; Confalonieri, M.; Tavano, S.; Ruaro, B. Correlation between Microvascular Damage and Internal Organ Involvement in Scleroderma: Focus on Lung Damage and Endothelial Dysfunction. Diagnostics 2023, 13, 55. https://doi.org/10.3390/diagnostics13010055
D’Oria M, Gandin I, Riccardo P, Hughes M, Lepidi S, Salton F, Confalonieri P, Confalonieri M, Tavano S, Ruaro B. Correlation between Microvascular Damage and Internal Organ Involvement in Scleroderma: Focus on Lung Damage and Endothelial Dysfunction. Diagnostics. 2023; 13(1):55. https://doi.org/10.3390/diagnostics13010055
Chicago/Turabian StyleD’Oria, Mario, Ilaria Gandin, Pozzan Riccardo, Michael Hughes, Sandro Lepidi, Francesco Salton, Paola Confalonieri, Marco Confalonieri, Stefano Tavano, and Barbara Ruaro. 2023. "Correlation between Microvascular Damage and Internal Organ Involvement in Scleroderma: Focus on Lung Damage and Endothelial Dysfunction" Diagnostics 13, no. 1: 55. https://doi.org/10.3390/diagnostics13010055