
Determining HER2 Status by Artificial Intelligence: An Investigation of Primary, Metastatic, and HER2 Low Breast Tumors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Ethics
2.2. Cohort Selection, Tissue Staining and Interpretation
2.3. AI Analysis of Immunohistochemistry Slides
2.4. AI Analysis of In Situ Hybridization Slides
2.5. Manual Assessment of Slides
2.6. Statistical Analysis
3. Results
3.1. Clinicopathological Features
3.2. Preliminary Cohort
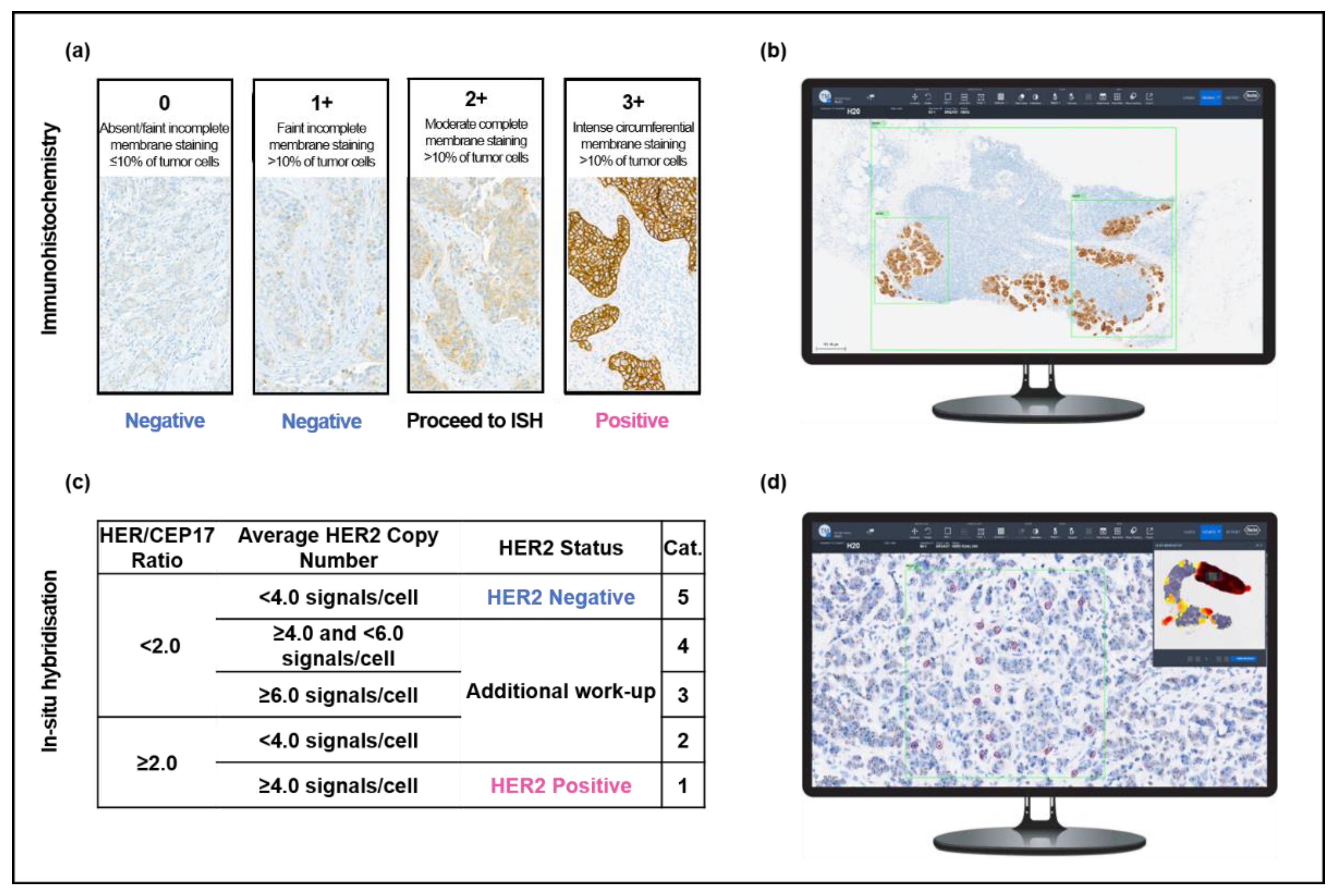
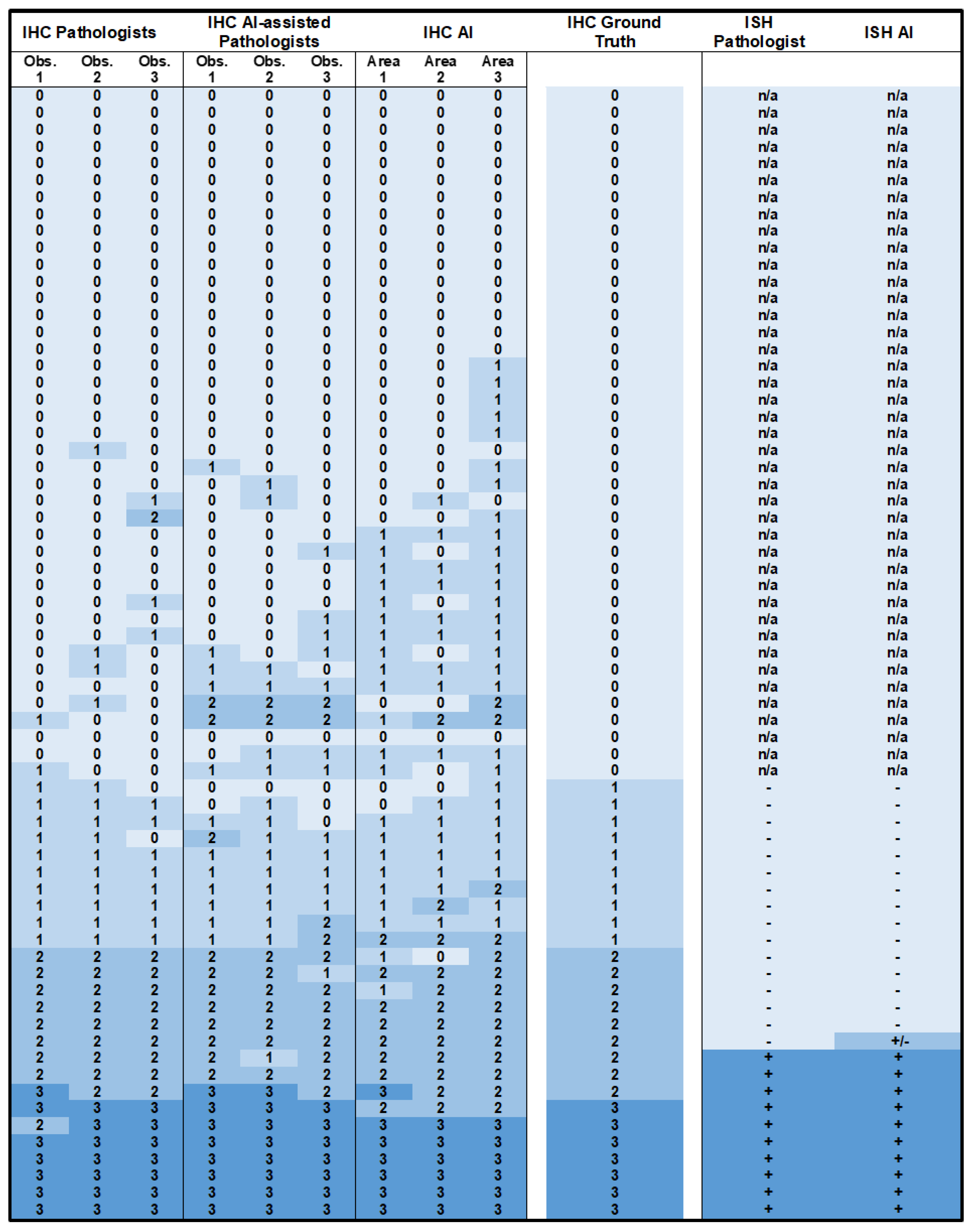
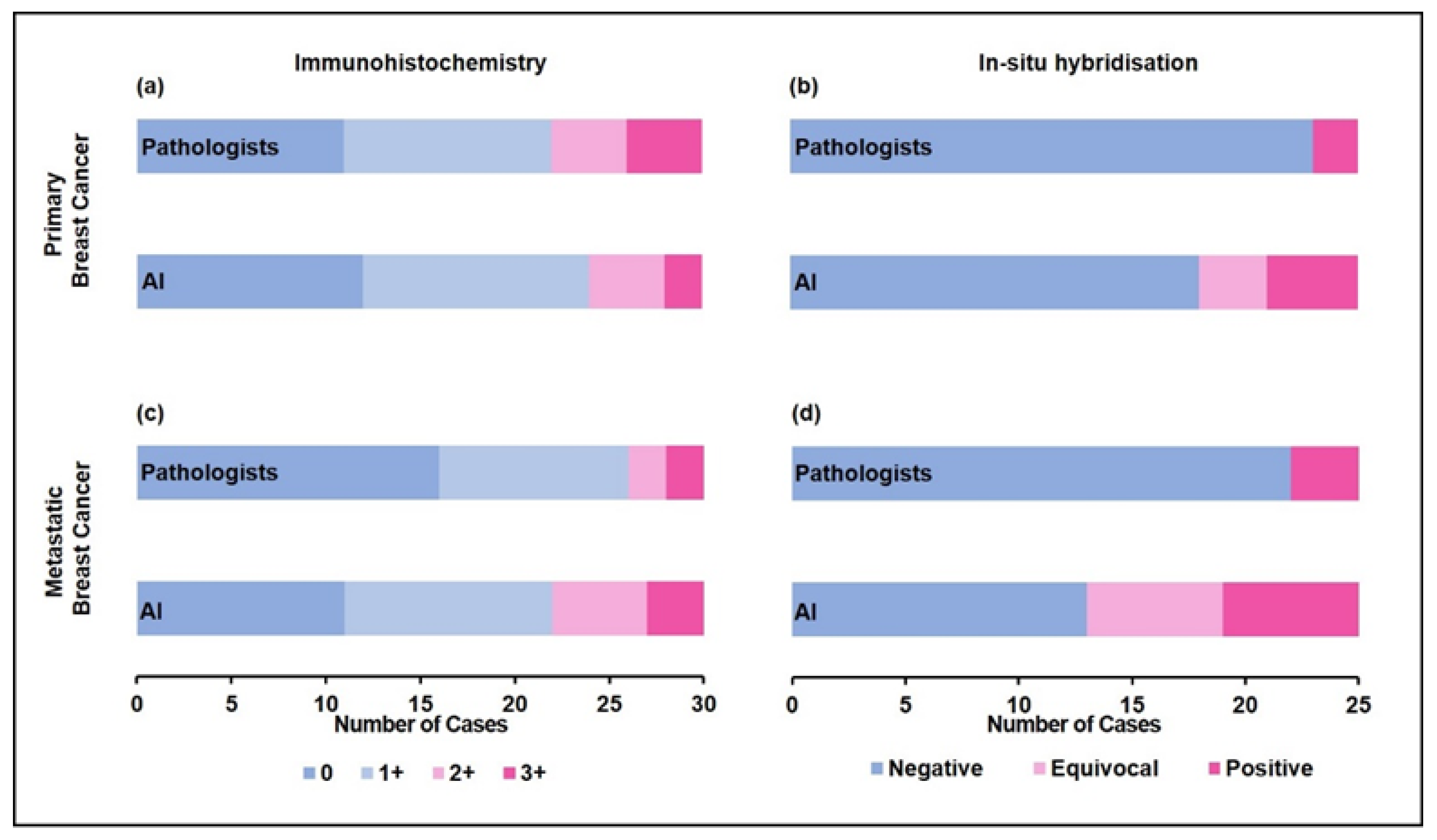
3.3. Primary B5b IBC: Immunohistochemistry
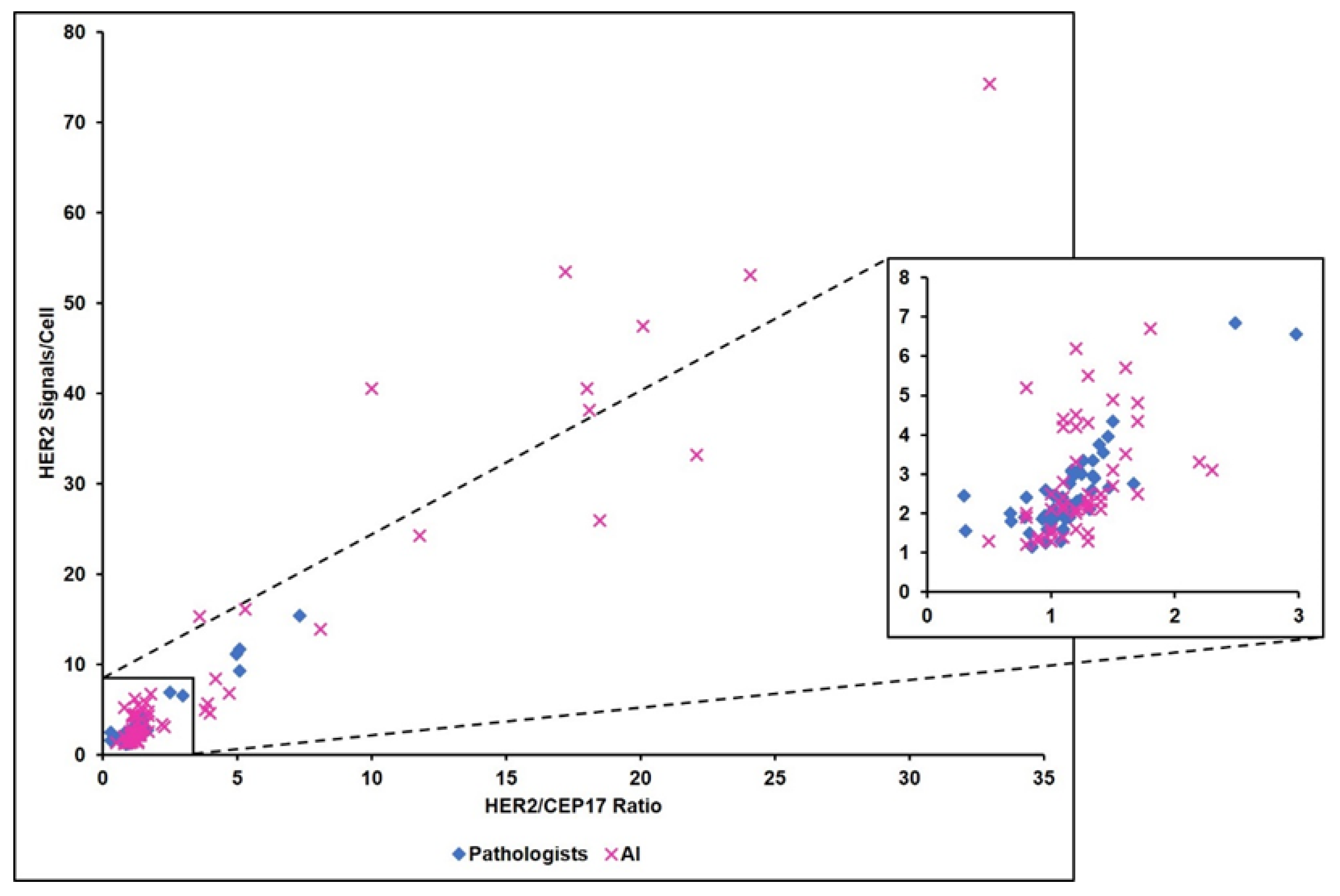
3.4. Primary B5b IBC: In Situ Hybridization
3.5. Primary B5b IBC: HER2 Low Tumors
3.6. Primary B5b IBC: Metastatic Breast Cancer
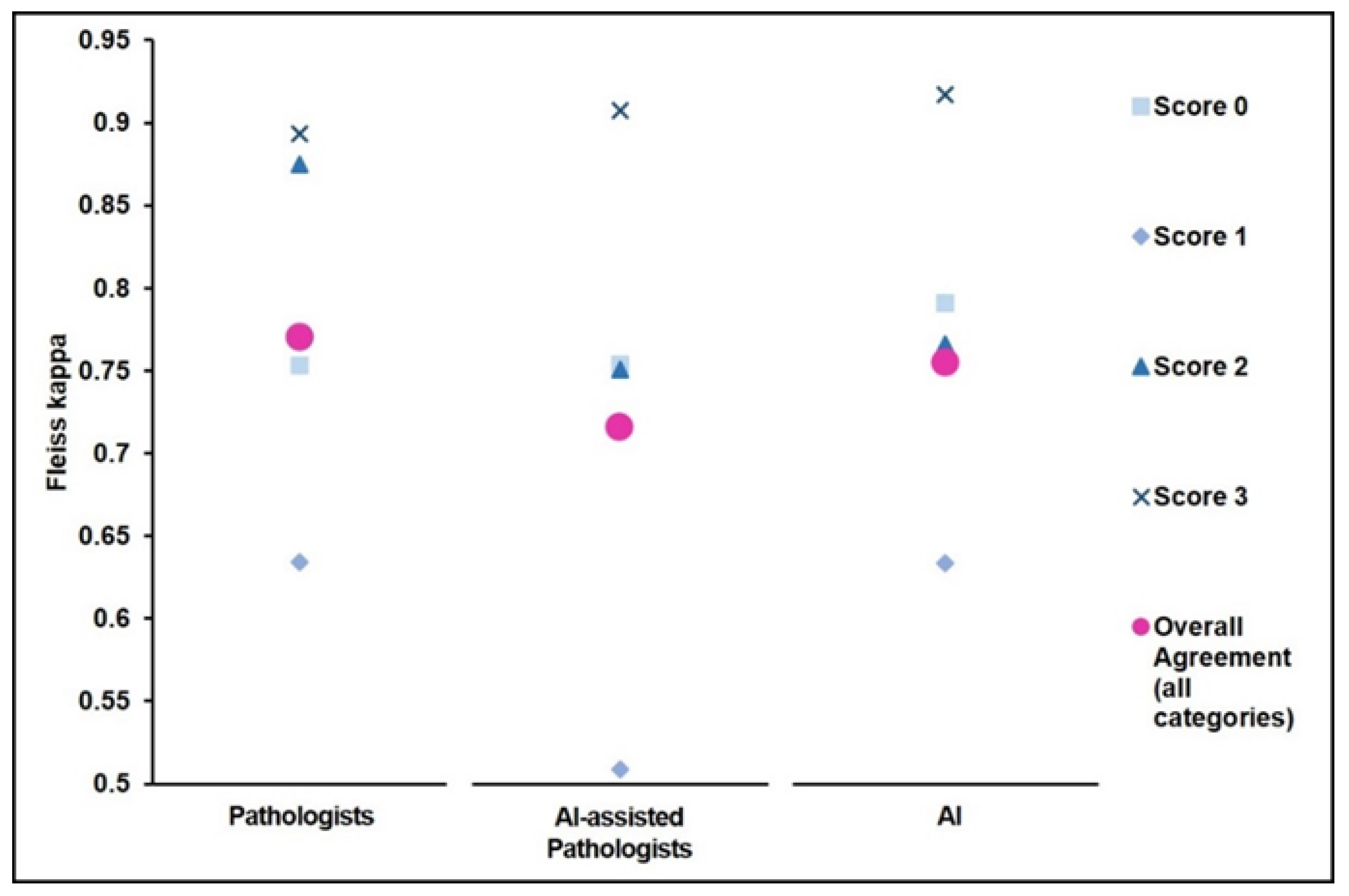
3.7. Primary B5b IBC: Accuracy of AI-Assisted Digitalized Workflow
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Konecny, G.E.; Meng, Y.G.; Untch, M.; Wang, H.-J.; Bauerfeind, I.; Epstein, M.; Stieber, P.; Vernes, J.-M.; Gutierrez, J.; Hong, K.; et al. Association between HER-2/neu and Vascular Endothelial Growth Factor Expression Predicts Clinical Outcome in Primary Breast Cancer Patients. Clin. Cancer Res. 2004, 10, 1706–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, S.; Woo, J.W.; Lee, K.; Park, S.Y. HER2 status in breast cancer: Changes in guidelines and complicating factors for interpretation. J. Pathol. Transl. Med. 2020, 54, 34–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: Correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.; Unni, N.; Peng, Y. The Changing Paradigm for the Treatment of HER2-Positive Breast Cancer. Cancers 2020, 12, 2081. [Google Scholar] [CrossRef]
- Cameron, D.; Piccart-Gebhart, M.J.; Gelber, R.D.; Procter, M.; Goldhirsch, A.; de Azambuja, E.; Castro, G., Jr.; Untch, M.; Smith, I.; Gianni, L.; et al. 11 years’ follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive early breast cancer: Final analysis of the HERceptin Adjuvant (HERA) trial. Lancet 2017, 389, 1195–1205. [Google Scholar] [CrossRef] [Green Version]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef] [Green Version]
- Layfield, L.J.; Frazier, S.; Esebua, M.; Schmidt, R.L. Interobserver reproducibility for HER2/neu immunohistochemistry: A comparison of reproducibility for the HercepTest™ and the 4B5 antibody clone. Pathol. Res. Pract. 2016, 212, 190–195. [Google Scholar] [CrossRef]
- Thomson, T.A.; Hayes, M.M.; Spinelli, J.J.; Hilland, E.; Sawrenko, C.; Phillips, D.; Dupuis, B.; Parker, R.L. HER-2/neu in Breast Cancer: Interobserver Variability and Performance of Immunohistochemistry with 4 Antibodies Compared with Fluorescent In Situ Hybridization. Mod. Pathol. 2001, 14, 1079–1086. [Google Scholar] [CrossRef] [Green Version]
- Moelans, C.; de Weger, R.; Van der Wall, E.; van Diest, P. Current technologies for HER2 testing in breast cancer. Crit. Rev. Oncol. 2011, 80, 380–392. [Google Scholar] [CrossRef]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef]
- Hurvitz, S.A. DESTINY-Changing Results for Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Turashvili, G.; Leung, S.; Turbin, D.; Montgomery, K.; Gilks, B.; West, R.; Carrier, M.; Huntsman, D.; Aparicio, S. Inter-observer reproducibility of HER2 immunohistochemical assessment and concordance with fluorescent in situhybridization (FISH): Pathologist assessment compared to quantitative image analysis. BMC Cancer 2009, 9, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, C.M.; Dyson, M.J.; Stephenson, T.J.; Maltby, E.L. HER2 amplification status in breast cancer: A comparison between immunohistochemical staining and fluorescence in situ hybridisation using manual and automated quantitative image analysis scoring techniques. J. Clin. Pathol. 2005, 58, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Brügmann, A.; Eld, M.; Lelkaitis, G.; Nielsen, S.; Grunkin, M.; Hansen, J.D.; Foged, N.T.; Vyberg, M. Digital image analysis of membrane connectivity is a robust measure of HER2 immunostains. Breast Cancer Res. Treat. 2011, 132, 41–49. [Google Scholar] [CrossRef]
- Masmoudi, H.; Hewitt, S.M.; Petrick, N.; Myers, K.J.; Gavrielides, M.A. Automated Quantitative Assessment of HER-2/neu Immunohistochemical Expression in Breast Cancer. IEEE Trans. Med. Imaging 2009, 28, 916–925. [Google Scholar] [CrossRef]
- Yousif, M.; Huang, Y.; Sciallis, A.; Kleer, C.G.; Pang, J.; Smola, B.; Naik, K.; McClintock, D.S.; Zhao, L.; Kunju, L.P.; et al. Quantitative Image Analysis as an Adjunct to Manual Scoring of ER, PgR, and HER2 in Invasive Breast Carcinoma. Am. J. Clin. Pathol. 2021, 157, 899–907. [Google Scholar] [CrossRef]
- Yue, M.; Zhang, J.; Wang, X.; Yan, K.; Cai, L.; Tian, K.; Niu, S.; Han, X.; Yu, Y.; Huang, J.; et al. Can AI-assisted microscope facilitate breast HER2 interpretation? A multi-institutional ring study. Virchows Arch. 2021, 479, 443–449. [Google Scholar] [CrossRef]
- Shamai, G.; Binenbaum, Y.; Slossberg, R.; Duek, I.; Gil, Z.; Kimmel, R. Artificial Intelligence Algorithms to Assess Hormonal Status From Tissue Microarrays in Patients With Breast Cancer. JAMA Netw. Open 2019, 2, e197700. [Google Scholar] [CrossRef] [Green Version]
- Qaiser, T.; Mukherjee, A.; Pb, C.R.; Munugoti, S.D.; Tallam, V.; Pitkäaho, T.; Lehtimäki, T.; Naughton, T.; Berseth, M.; Pedraza, A.; et al. HER2 challenge contest: A detailed assessment of automated HER2 scoring algorithms in whole slide images of breast cancer tissues. Histopathology 2017, 72, 227–238. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Koopman, T.; Buikema, H.J.; Hollema, H.; de Bock, G.H.; van der Vegt, B. What is the added value of digital image analysis of HER 2 immunohistochemistry in breast cancer in clinical practice? A study with multiple platforms. Histopathology 2018, 74, 917–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helin, H.O.; Tuominen, V.J.; Ylinen, O.; Helin, H.J.; Isola, J. Free digital image analysis software helps to resolve equivocal scores in HER2 immunohistochemistry. Virchows Arch. 2015, 468, 191–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rüschoff, J.; Lebeau, A.; Kreipe, H.; Sinn, P.; Gerharz, C.D.; Koch, W.; Morris, S.; Ammann, J.; Untch, M. Assessing HER2 testing quality in breast cancer: Variables that influence HER2 positivity rate from a large, multicenter, observational study in Germany. Mod. Pathol. 2016, 30, 217–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godoy-Ortiz, A.; Sanchez-Muñoz, A.; Parrado, M.R.C.; Álvarez, M.; Ribelles, N.; Dominguez, A.R.; Alba, E. Deciphering HER2 Breast Cancer Disease: Biological and Clinical Implications. Front. Oncol. 2019, 9, 1124. [Google Scholar] [CrossRef] [PubMed]
- Bui, M.M.; Riben, M.W.; Allison, K.H.; Chlipala, E.; Colasacco, C.; Kahn, A.G.; Lacchetti, C.; Madabhushi, A.; Pantanowitz, L.; Salama, M.E.; et al. Quantitative Image Analysis of Human Epidermal Growth Factor Receptor 2 Immunohistochemistry for Breast Cancer: Guideline From the College of American Pathologists. Arch. Pathol. Lab. Med. 2018, 143, 1180–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moutafi, M.; Robbins, C.J.; Yaghoobi, V.; Fernandez, A.I.; Martinez-Morilla, S.; Xirou, V.; Bai, Y.; Song, Y.; Gaule, P.; Krueger, J.; et al. Quantitative measurement of HER2 expression to subclassify ERBB2 unamplified breast cancer. Lab. Investig. 2022, 102, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Marchiò, C.; Annaratone, L.; Marques, A.; Casorzo, L.; Berrino, E.; Sapino, A. Evolving concepts in HER2 evaluation in breast cancer: Heterogeneity, HER2-low carcinomas and beyond. Semin. Cancer Biol. 2020, 72, 123–135. [Google Scholar] [CrossRef]
- Sakamoto, T.; Furukawa, T.; Lami, K.; Pham, H.H.N.; Uegami, W.; Kuroda, K.; Kawai, M.; Sakanashi, H.; Cooper, L.A.D.; Bychkov, A.; et al. A narrative review of digital pathology and artificial intelligence: Focusing on lung cancer. Transl. Lung Cancer Res. 2020, 9, 2255–2276. [Google Scholar] [CrossRef]
- Jahn, S.; Plass, M.; Moinfar, F. Digital Pathology: Advantages, Limitations and Emerging Perspectives. J. Clin. Med. 2020, 9, 3697. [Google Scholar] [CrossRef]
- Ahmad, Z.; Rahim, S.; Zubair, M.; Abdul-Ghafar, J. Artificial intelligence (AI) in medicine, current applications and future role with special emphasis on its potential and promise in pathology: Present and future impact, obstacles including costs and acceptance among pathologists, practical and philosophical considerations. A comprehensive review. Diagn. Pathol. 2021, 16, 24. [Google Scholar] [CrossRef]
- Varga, Z.; Noske, A.; Ramach, C.; Padberg, B.; Moch, H. Assessment of HER2 status in breast cancer: Overall positivity rate and accuracy by fluorescence in situ hybridization and immunohistochemistry in a single institution over 12 years: A quality control study. BMC Cancer 2013, 13, 615. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preliminary Cohort | Study Cohort | |
|---|---|---|
| No. of Cases | 495 | 97 (67 *) |
| Average Patient Age, yrs | 61 | 60 |
| Range | 29–95 | 30–80 |
| Tumor Type, No. (%) | ||
| Ductal | 394 (80) | 55 (82) |
| Lobular | 75 (15) | 6 (9) |
| Other | 26 (5) | 6 (9) |
| Tumor Grade, No. (%) | ||
| 1 | 112 (23) | 9 (14) |
| 2 | 237 (48) | 30 (45) |
| 3 | 146 (29) | 28 (42) |
| ER positive, No. (%) | 421 (85) | 58 (87) |
| PR positive, No. (%) | 371 (75) | 52 (78) |
| HER2 positive, No. (%) | 59 (12) | 10 (15) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palm, C.; Connolly, C.E.; Masser, R.; Padberg Sgier, B.; Karamitopoulou, E.; Simon, Q.; Bode, B.; Tinguely, M. Determining HER2 Status by Artificial Intelligence: An Investigation of Primary, Metastatic, and HER2 Low Breast Tumors. Diagnostics 2023, 13, 168. https://doi.org/10.3390/diagnostics13010168
Palm C, Connolly CE, Masser R, Padberg Sgier B, Karamitopoulou E, Simon Q, Bode B, Tinguely M. Determining HER2 Status by Artificial Intelligence: An Investigation of Primary, Metastatic, and HER2 Low Breast Tumors. Diagnostics. 2023; 13(1):168. https://doi.org/10.3390/diagnostics13010168
Chicago/Turabian StylePalm, Christiane, Catherine E. Connolly, Regina Masser, Barbara Padberg Sgier, Eva Karamitopoulou, Quentin Simon, Beata Bode, and Marianne Tinguely. 2023. "Determining HER2 Status by Artificial Intelligence: An Investigation of Primary, Metastatic, and HER2 Low Breast Tumors" Diagnostics 13, no. 1: 168. https://doi.org/10.3390/diagnostics13010168