
Oncologic Outcome after Pulmonary Metastasectomy as Part of Multidisciplinary Treatment in a Tertiary Oncological Center

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
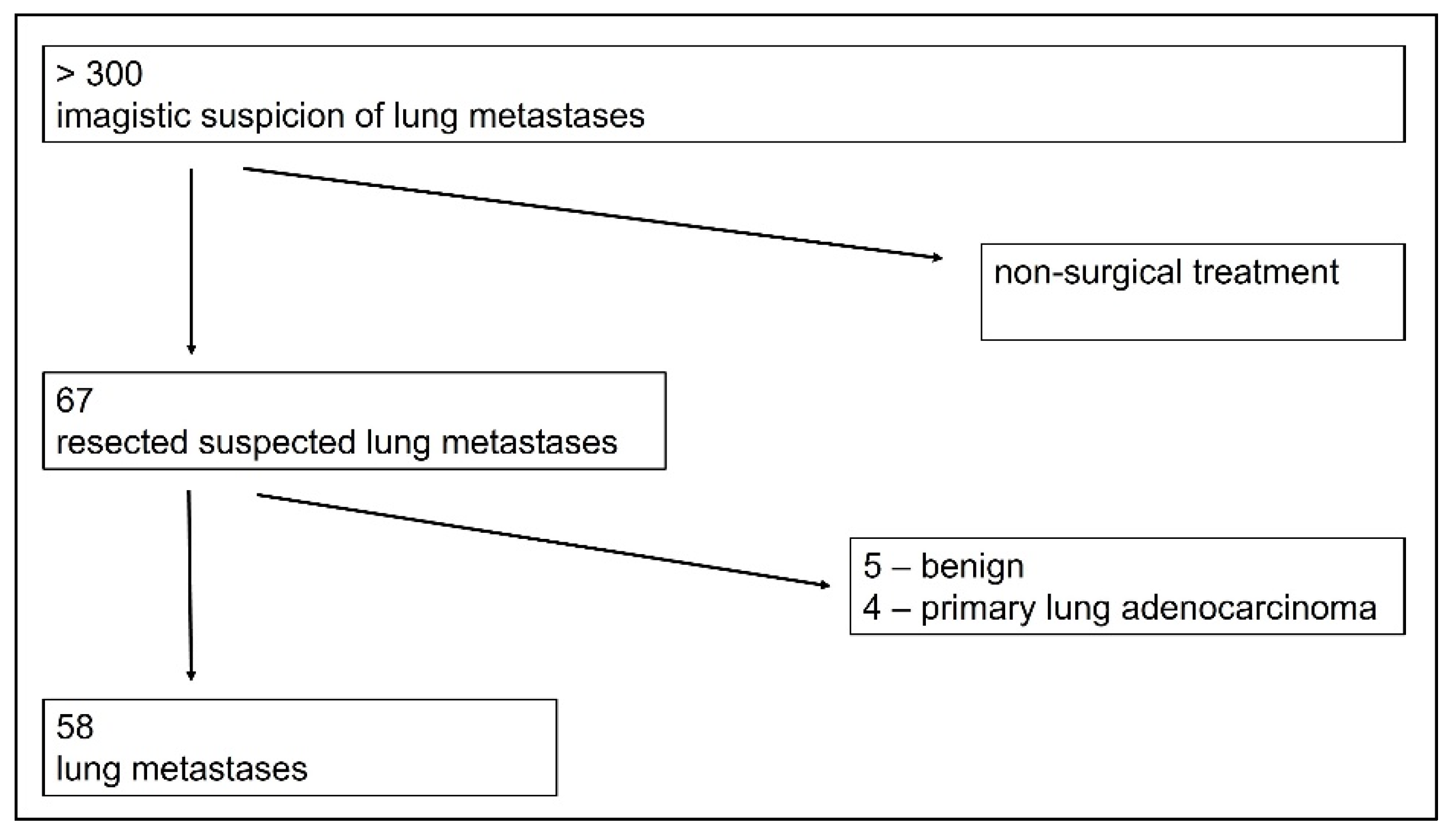
3. Results
3.1. Patient Characteristics
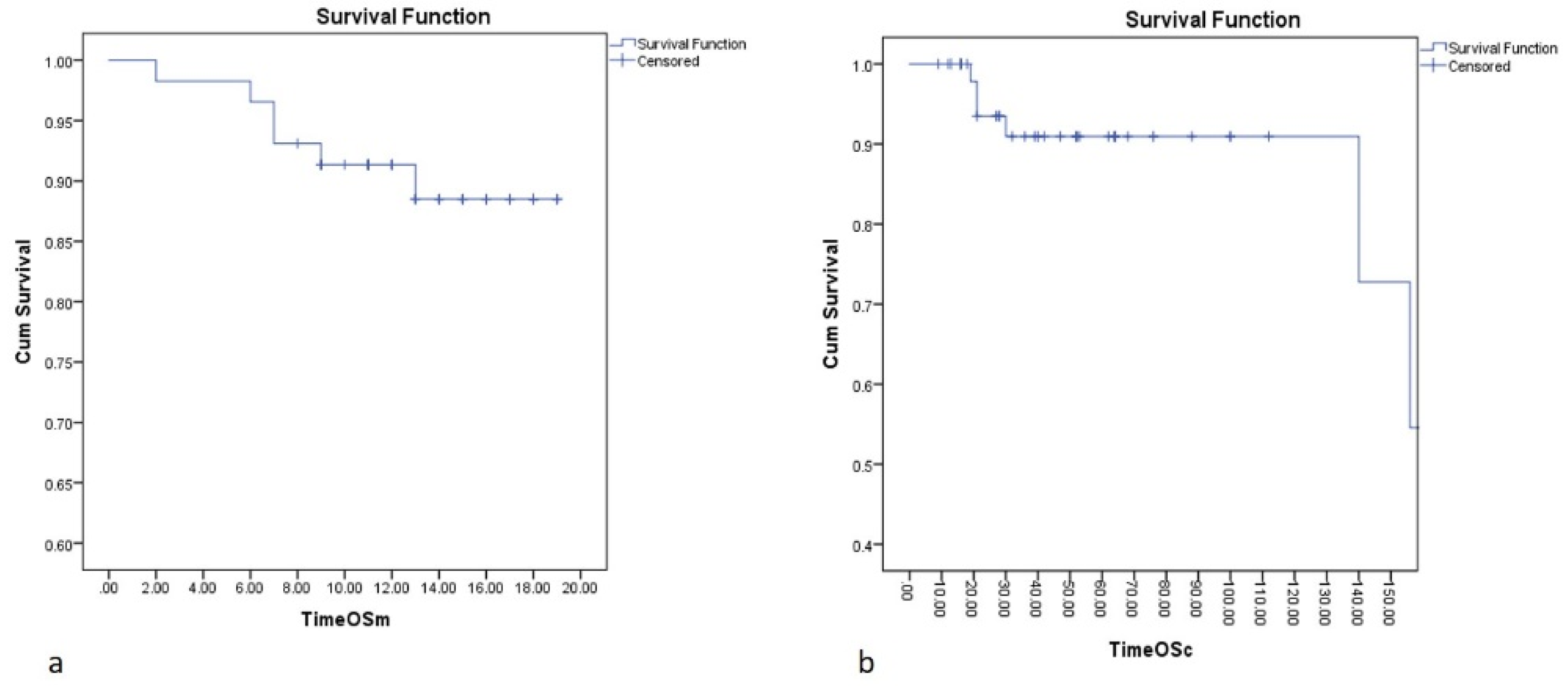
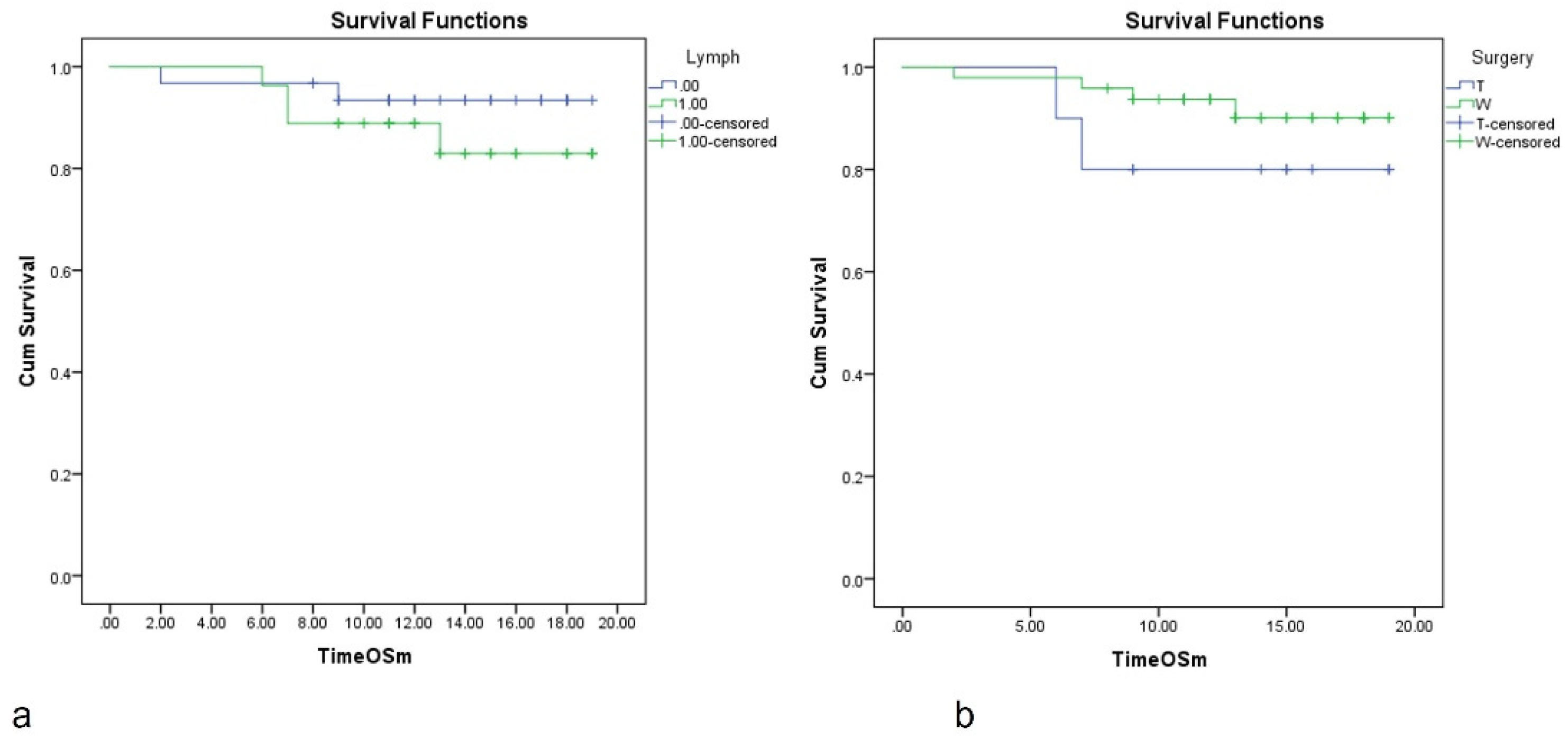
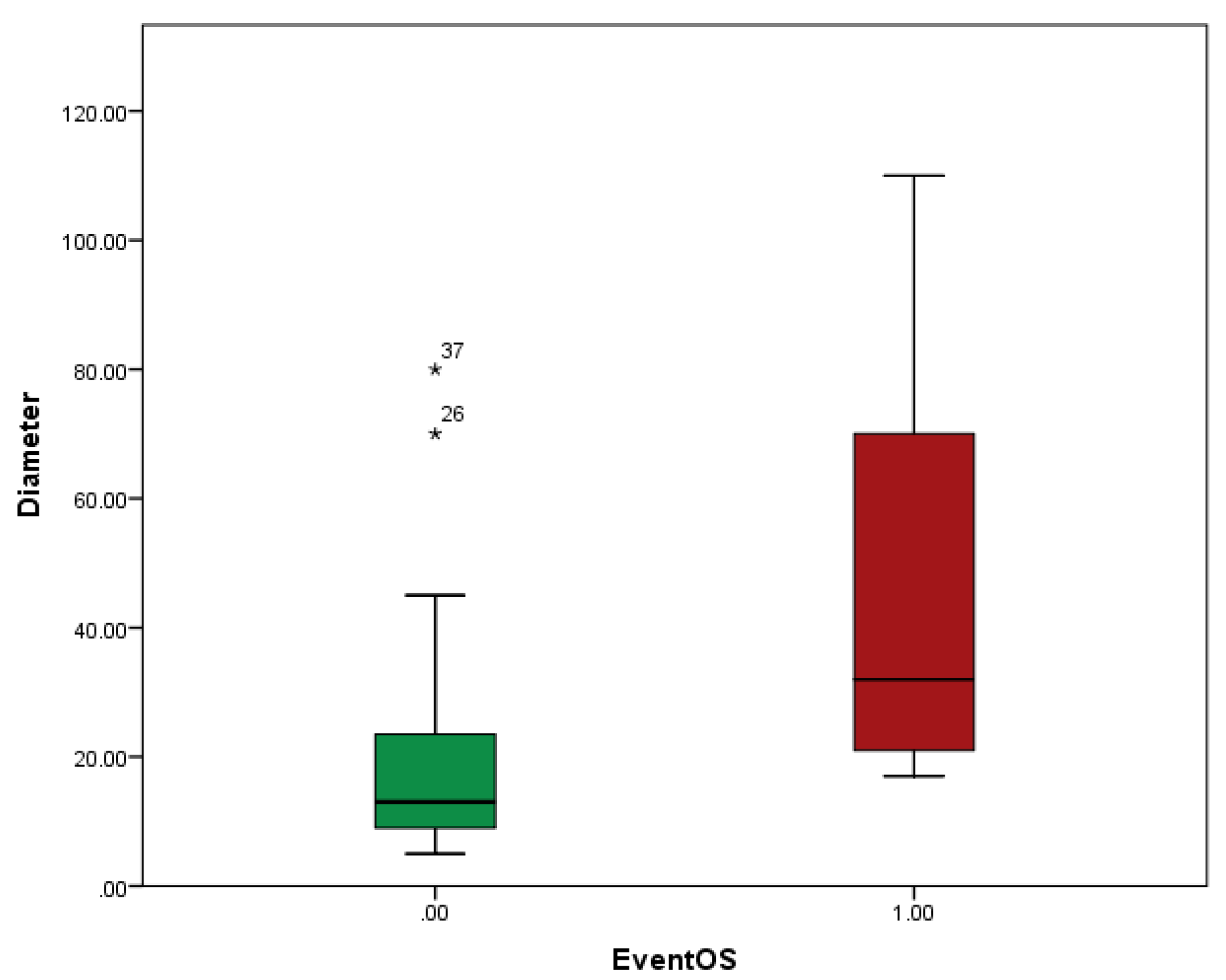
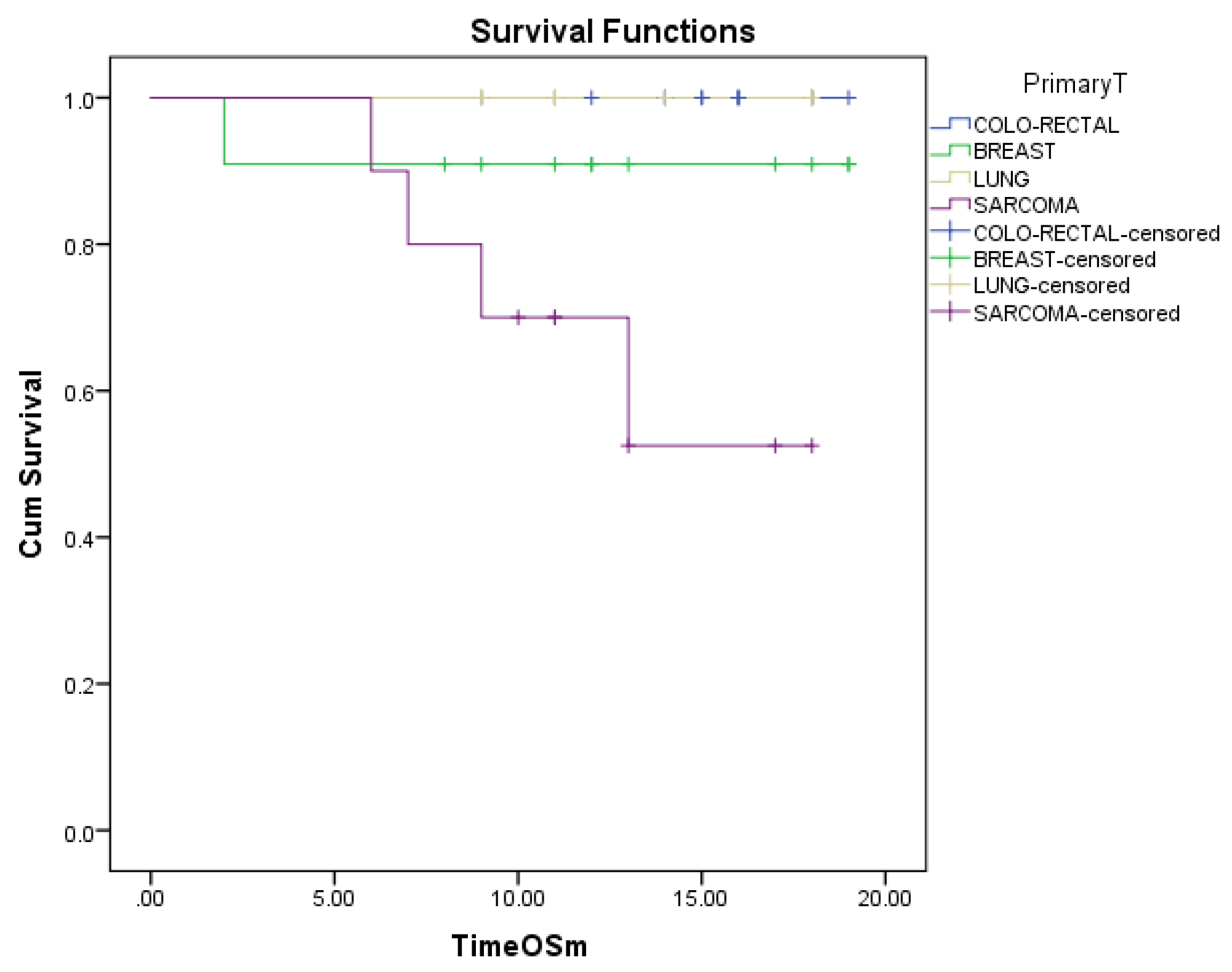
3.2. Overall Survival (OS) after Metastasectomy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mangiameli, G.; Cioffi, U.; Alloisio, M.; Testori, A. Lung Metastases: Current Surgical Indications and New Perspectives. Front. Surg. 2022, 9, 884915. [Google Scholar] [CrossRef] [PubMed]
- Forster, C.; Ojanguren, A.; Perentes, J.Y.; Zellweger, M.; Krueger, T.; Abdelnour-Berchtold, E.; Gonzalez, M. Survival prognostic and recurrence risk factors after single pulmonary metastasectomy. J. Cardiothorac. Surg. 2021, 16, 357. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; MacManus, M.; Ball, D. Stereotactic radiotherapy for pulmonary oligometastases: A systematic review. J. Thorac. Oncol. 2010, 5, 1091–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Database Annual Report. 2021. The European Society of Thoracic Surgeons. Available online: https://www.ests.org/_userfiles/pages/files/database_reports/ests_2021_silver_book.pdf (accessed on 28 November 2022).
- Handy, J.R.; Bremner, R.M.; Crocenzi, T.S.; Detterbeck, F.C.; Fernando, H.C.; Fidias, P.M.; Firestone, S.; Johnstone, C.A.; Lanuti, M.; Litle, V.R.; et al. Expert consensus document on pulmonary metastasectomy. Ann. Thorac. Surg. 2019, 107, 631–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastorino, U.; Buyse, M.; Friedel, G.; Ginsberg, R.J.; Girard, P.; Goldstraw, P.; Johnston, M.; McCormack, P.; Pass, H.; Putnam, J.B., Jr.; et al. Long-term results of lung metastasectomy: Prognostic analyses based on 5206 cases. J. Thorac. Cardiovasc. Surg. 1997, 113, 37–49. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.Y.; Lau, J.; Siew, B.E.; Chua, Y.K.; Lim, Y.X.; Lim, X.Y.; Chong, C.S.; Tan, K.K. Does pulmonary metastasectomy of colorectal metastases translate to better survival? A systematic review. Ann. Acad. Med. Singap. 2021, 50, 773–781. [Google Scholar] [CrossRef]
- Treasure, T.; PulMiCC Trial Group; Farewell, V.; Macbeth, F.; Monson, K.; Williams, N.R.; Brew-Graves, C.; Lees, B.; Grigg, O.; Fallowfield, L. Pulmonary metastasectomy versus continued active monitoring in colorectal cancer (PulMiCC): A multicentre randomised clinical trial. Trials 2019, 20, 718. [Google Scholar] [CrossRef] [Green Version]
- Higashiyama, M.; Tokunaga, T.; Nakagiri, T.; Ishida, D.; Kuno, H.; Okami, J. Pulmonary metastasectomy: Outcomes and issues according to the type of surgical resection. Gen. Thorac. Cardiovasc. Surg. 2015, 63, 320–330. [Google Scholar] [CrossRef]
- Chung, J.H.; Lee, S.H.; Yi, E.; Lim, J.Y.; Jung, J.S.; Son, H.S.; Sun, K. Impact of resection margin length and tumor depth on the local recurrence after thoracoscopic pulmonary wedge resection of a single colorectal metastasis. J. Thorac. Dis. 2019, 11, 1879–1887. [Google Scholar] [CrossRef]
- Shiono, S.; Metastatic Lung Tumor Study Group of Japan; Matsutani, N.; Hashimoto, H.; Yamauchi, Y.; Matsuguma, H.; Mun, M.; Kuroda, H.; Funai, K.; Nakajima, J.; et al. Metastatic Lung Tumor Study Group of Japan. Prospective study of recurrence at the surgical margin after wedge resection of pulmonary metastases. Gen. Thorac. Cardiovasc. Surg. 2021, 69, 950–959. [Google Scholar] [CrossRef]
- van Dorp, M.; Bousema, J.E.; Torensma, B.; Dickhoff, C.; Broek, F.J.C.V.D.; Schreurs, W.H.; Gonzalez, M.; Kazemier, G.; Heineman, D.J. Pulmonary metastasectomy with lymphadenectomy for colorectal pulmonary metastases: A systematic review. Eur. J. Surg. Oncol. 2022, 48, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Caristo, J.M.; Tian, D.H.; Yan, T.D. Pulmonary metastasectomy: A consensus statement by thoracic surgeons. J. Thorac. Dis. 2018, 10, 3757–3766. [Google Scholar] [CrossRef] [PubMed]
- Cariboni, U.; De Sanctis, R.; Giaretta, M.; Voulaz, E.; Morenghi, E.; Colombo, P.; Novellis, P.; Bottoni, E.; Errico, V.; Crepaldi, A.; et al. Survival outcome and prognostic factors after pulmonary metastasectomy in sarcoma patients: A 18-year experience at a single high-volume referral center. Am. J. Clin. Oncol. 2019, 42, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Beckers, P.; Berzenji, L.; Yogeswaran, S.K.; Lauwers, P.; Bilotta, G.; Shkarpa, N.; Hendriks, J.; Van Schil, P.E. Pulmonary metastasectomy in colorectal carcinoma. J. Thorac. Dis. 2021, 13, 2628–2635. [Google Scholar] [CrossRef] [PubMed]
- Shiono, S. The role of pulmonary metastasectomy for pulmonary metastasis from head and neck cancer. J. Thorac Dis. 2021, 13, 2643–2648. [Google Scholar] [CrossRef]
- Kanzaki, R.; Fukui, E.; Kanou, T.; Ose, N.; Funaki, S.; Minami, M.; Shintani, Y.; Okumura, M. Preoperative evaluation and indications for pulmonary metastasectomy. J. Thorac. Dis. 2021, 13, 2590–2602. [Google Scholar] [CrossRef]
- Ambrogi, V.; Tamburrini, A.; Tajé, R. Results of redo pulmonary metastasectomy. J. Thorac. Dis. 2021, 13, 2669–2685. [Google Scholar] [CrossRef]
- Trifanescu, O.G.; Gales, L.; Bacinschi, X.; Serbanescu, L.; Georgescu, M.; Sandu, A.; Michire, A.; Anghel, R. Impact of the COVID-19 Pandemic on Treatment and Oncologic Outcomes for Cancer Patients in Romania. Vivo 2022, 36, 934–941. [Google Scholar] [CrossRef]
- Panagiotopoulos, N.; Patrini, D.; Lawrence, D.; Scarci, M.; Mitsos, S. Pulmonary metastasectomy and laser-assisted resection. J. Thorac. Dis. 2018, 10 (Suppl. 17), S1930–S1933. [Google Scholar] [CrossRef]
- Cheung, P. Stereotactic body radiotherapy for oligoprogressive cancer. Br. J. Radiol. 2016, 89, 20160251. [Google Scholar] [CrossRef]
- Guida, M.; Bartolomeo, N.; De Risi, I.; Fucci, L.; Armenio, A.; Filannino, R.; Ruggieri, E.; Macina, F.; Traversa, M.; Nardone, A.; et al. The Management of Oligoprogression in the Landscape of New Therapies for Metastatic Melanoma. Cancers 2019, 11, 1559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karampinis, I.; Rathmann, N.; Kostrzewa, M.; Diehl, S.J.; Schoenberg, S.O.; Hohenberger, P.; Roessner, E.D. Computer tomography guided thoracoscopic resection of small pulmonary nodules in the hybrid theatre. PLoS ONE 2021, 16, e0258896. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Chang, W.; Wang, H.; Lin, Q.; Wei, Y.; Tang, W.; Liu, Y.; Chen, Y.; Niu, Z.; Jiang, Y.; et al. Anatomical Resection Improves Disease-Free Survival After Lung Metastasectomy of Colorectal Cancer. Cancer Manag. Res. 2021, 13, 9429–9437. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Wang, Z.; Liu, Y.; Xing, H.; Xu, J.; Xu, W.; Cai, H.; Jiang, Y. Application of Simultaneous Localization of Multiple Pulmonary Nodules in a Hybrid Operating Room for Uniportal Video-Assisted Thoracic Surgery. Int. J. Gen. Med. 2022, 15, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, J.; Licht, P.B. Thoracoscopic or open surgery for pulmonary metastasectomy: An observer blinded study. Ann. Thorac. Surg. 2014, 98, 466–469. [Google Scholar] [CrossRef] [PubMed]
- Hernández, J.; Molins, L.; Fibla, J.; Heras, F.; Embún, R.; Rivas, J.; Rivas, F.; Mier, J.; de la Cruz, J.; Rubio, M.; et al. Role of major resection in pulmonary metastasectomy for colorectal cancer in the Spanish prospective multicenter study (GECMP-CCR). Ann. Oncol. 2016, 27, 850–855. [Google Scholar] [CrossRef]
- Pfannschmidt, J.; Klode, J.; Muley, T.; Dienemann, H.; Hoffmann, H. Nodal involvement at the time of pulmonary metastasectomy: Experiences in 245 patients. Ann. Thorac. Surg. 2006, 81, 448–454. [Google Scholar] [CrossRef]
- Ercan, S.; Nichols, F.C., III; Trastek, V.F.; Deschamps, C.; Allen, M.S.; Miller, D.L.; Schleck, C.D.; Pairolero, P.C. Prognostic significance of lymph node metastasis found during pulmonary metastasectomy for extrapulmonary carcinoma. Ann. Thorac. Surg. 2004, 77, 1786–1791. [Google Scholar] [CrossRef]
- Internullo, E.; Cassivi, S.D.; Van Raemdonck, D.; Friedel, G.; Treasure, T.; ESTS Pulmonary Metastasectomy Working Group. Pulmonary metastasectomy: A survey of current practice amongst members of the European Society of Thoracic Surgeons. J. Thorac. Oncol. 2008, 3, 1257–1266. [Google Scholar] [CrossRef] [Green Version]
- Abrams, H.L.; Spiro, R.; Goldstein, N. Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer 1950, 3, 74–85. [Google Scholar] [CrossRef]
- Renaud, S.; Alifano, M.; Falcoz, P.E.; Magdeleinat, P.; Santelmo, N.; Pagès, O.; Massard, G.; Régnard, J.-F. Does nodal status influence survival? Results of a 19-year systematic lymphadenectomy experience during lung metastasectomy of colorectal cancer. Interact. Cardiovasc. Thorac. Surg. 2014, 18, 482–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamaji, M.; Cassivi, S.D.; Shen, K.R.; Allen, M.S.; Nichols, F.C.; Deschamps, C.; Wigle, D.A. Is lymph node dissection required in pulmonary metastasectomy for colorectal adenocarcinoma? Ann. Thorac. Surg. 2012, 94, 1796–1800. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Yuste, M.; Cassivi, S.; Paleru, C. Thoracic lymphatic involvement in patients having pulmonary metastasectomy: Incidence and the effect on prognosis. J. Thorac. Oncol. 2010, 5 (Suppl. 2), S166–S169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dediu, M.; Ion, O.; Ion, R.; Alexandru, A.; Median, D.; Gal, C.; Horvat, T.; Motas, C.; Motas, N. Impact of adjuvant chemotherapy in stage IB non-small-cell lung cancer: An analysis of 112 consecutively treated patients. J. B.U.ON. Off. J. Balk. Union Oncol. 2012, 17, 317–322. [Google Scholar]
- Winter, H.; Meimarakis, G.; Angele, M.K.; Hummel, M.; Staehler, M.; Hoffmann, R.T.; Hatz, R.A.; Löhe, F. Tumor infiltrated hilar and mediastinal lymph nodes are an independent prognostic factor for decreased survival after pulmonary metastasectomy in patients with renal cell carcinoma. J. Urol. 2010, 184, 1888–1894. [Google Scholar] [CrossRef]
- Seebacher, G.; Decker, S.; Fischer, J.R.; Held, M.; Schäfers, H.J.; Graeter, T.P. Unexpected lymph node disease in resections for pulmonary metastases. Ann. Thorac. Surg. 2015, 99, 231–236. [Google Scholar] [CrossRef]
- Davidson, R.S.; Nwogu, C.E.; Brentjens, M.J.; Anderson, T.M. The surgical management of pulmonary metastasis: Current concepts. Surg. Oncol. 2001, 10, 35–42. [Google Scholar] [CrossRef]
- Alexander, J.; Haight, C. Pulmonary resection for solitary metastatic sarcomas and carcinomas. Surg. Gynecol. Obstet. 1947, 85, 129–146. [Google Scholar]
- Thomford, N.R.; Woolner, L.B.; Clagett, O.T. The surgical treament of metastatic tumors in the lungs. J. Thorac. Cardiovasc. Surg. 1965, 49, 357–363. [Google Scholar] [CrossRef]
- Hornbech, K.; Ravn, J.; Steinbrüchel, D.A. Current status of pulmonary metastasectomy. Eur. J. Cardio-Thorac. Surg. 2011, 39, 955–962. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Soria, J.C.; Michiels, S.; Grunenwald, D.; Validire, P.; Caliandro, R.; Girard, P.; Le Chevalier, T. Uncertain benefit from surgery in patients with lung metastases from breast carcinoma. Cancer 2004, 100, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Bilani, N.; Yaghi, M.; Main, O.; Naik, M.; Jabbal, I.; Rivera, C.; Elson, L.; Liang, H.; Saravia, D.; Nahleh, Z. Metastasectomy versus radiation of secondary sites in stage IV breast cancer: Analysis from a national cancer registry. Breast 2021, 60, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.H.; Park, S.Y.; Kim, H.E.; Park, B.J.; Lee, C.Y.; Lee, J.G.; Kim, D.J.; Paik, H.C. Effects of mediastinal lymph node dissection in colorectal cancer-related pulmonary metastasectomy. Thorac. Cancer 2021, 12, 3248–3254. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Stoltzfus, K.C.; Lehrer, E.J.; Horn, S.R.; Siva, S.; Trifiletti, D.M.; Meng, M.B.; Verma, V.; Louie, A.V.; Zaorsky, N.G. The Epidemiology of Lung Metastases. Front. Med. 2021, 8, 723396. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Cancer | Number of Cases | Percent from Total (%) |
|---|---|---|
| colon | 14 | 24.14 |
| breast | 10 | 17.24 |
| lung | 8 | 13.79 |
| sarcomas | 8 | 13.79 |
| cervix | 5 | 8.62 |
| renal | 4 | 6.9 |
| endometrium | 3 | 5.17 |
| GIST | 2 | 3.45 |
| pharynx | 1 | 1.72 |
| pancreas | 1 | 1.72 |
| hepatic | 1 | 1.72 |
| urothelium | 1 | 1.72 |
| Total | 58 | 100 |
| Lobe/Type of Resection | Anatomical Resections (Typical) | Associated Resections | Wedge Resection (Non-Anatomical, Atypical) | Associated Resections |
|---|---|---|---|---|
| Right upper lobe (RUL) | 2 | - | 8 | - |
| Right middle lobe (RML) | 2 | +2 wedge lung resections | - | - |
| Right lower lobe (RLL) | 4 | +Atrial resection, pericardiectomy, pericardioplasty | 21 | +Resection of diaphragm and pericardium |
| Left upper lobe (LUL) | 2 | - | 18 | - |
| +Excision of nodule of parietal pleura | ||||
| Left lower lobe (LLL) | 2 | +Parietal pleura | 15 | +Splanchnicectomy |
| +Laser vaporization of millimeric lung nodules |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Motas, N.; Davidescu, M.D.; Tanase, B.C.; Rus, O.; Burlacu, A.I.; Alexe, V.; Manolache, V.; Mizea, M.C.; Gheorghiu, N.; Trifanescu, O.G.; et al. Oncologic Outcome after Pulmonary Metastasectomy as Part of Multidisciplinary Treatment in a Tertiary Oncological Center. Diagnostics 2023, 13, 165. https://doi.org/10.3390/diagnostics13010165
Motas N, Davidescu MD, Tanase BC, Rus O, Burlacu AI, Alexe V, Manolache V, Mizea MC, Gheorghiu N, Trifanescu OG, et al. Oncologic Outcome after Pulmonary Metastasectomy as Part of Multidisciplinary Treatment in a Tertiary Oncological Center. Diagnostics. 2023; 13(1):165. https://doi.org/10.3390/diagnostics13010165
Chicago/Turabian StyleMotas, Natalia, Mihnea Dan Davidescu, Bogdan Cosmin Tanase, Ovidiu Rus, Alin Ionut Burlacu, Vlad Alexe, Veronica Manolache, Madalina Cristiana Mizea, Nicolae Gheorghiu, Oana Gabriela Trifanescu, and et al. 2023. "Oncologic Outcome after Pulmonary Metastasectomy as Part of Multidisciplinary Treatment in a Tertiary Oncological Center" Diagnostics 13, no. 1: 165. https://doi.org/10.3390/diagnostics13010165