
Performance of Deauville Criteria in [18F]FDG-PET/CT Diagnostics of Giant Cell Arteritis
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. PET/CT Imaging
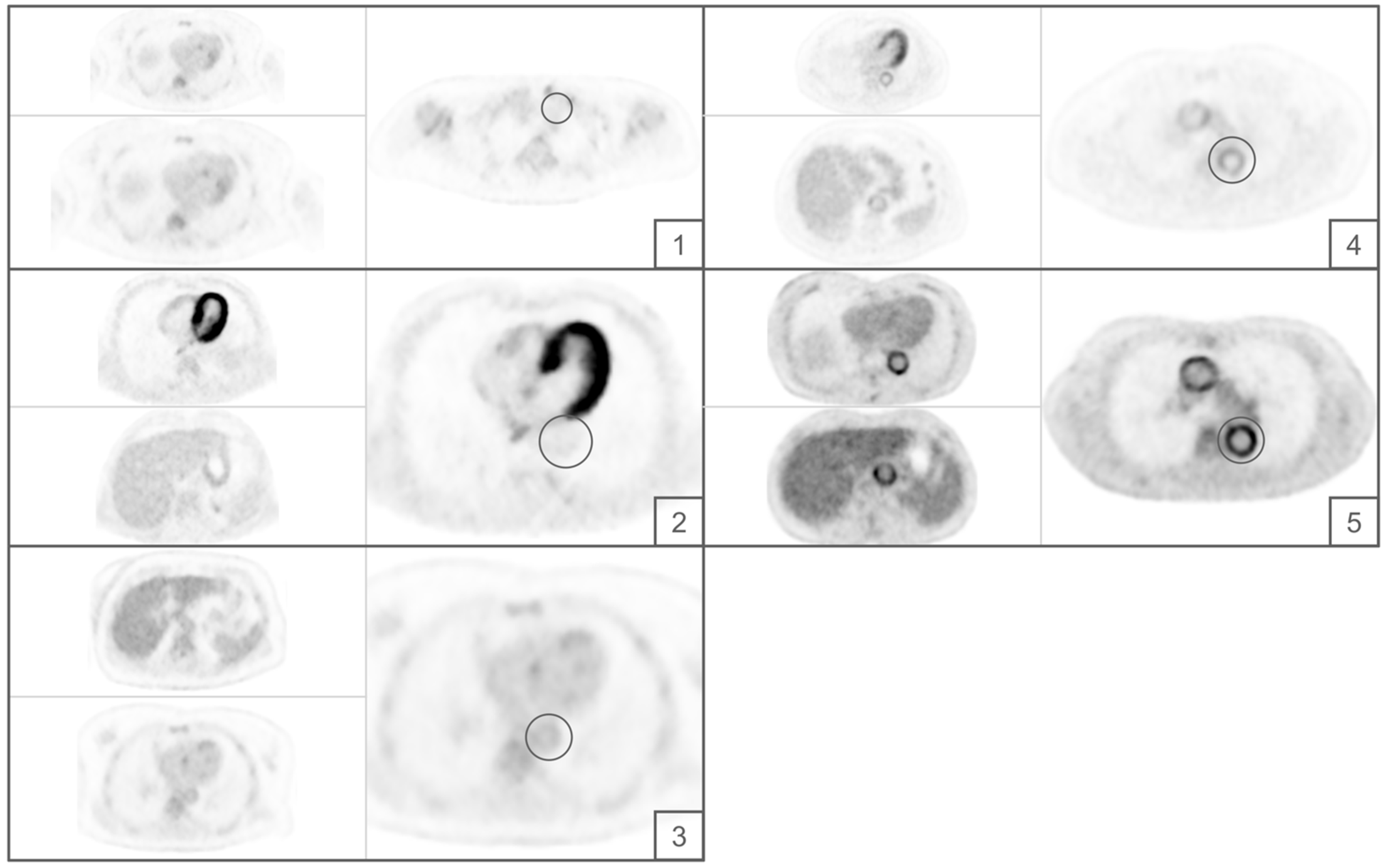
2.3. Image Assessment
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Diagnostic Performance
3.3. Comparison with Cut-Off ≥3
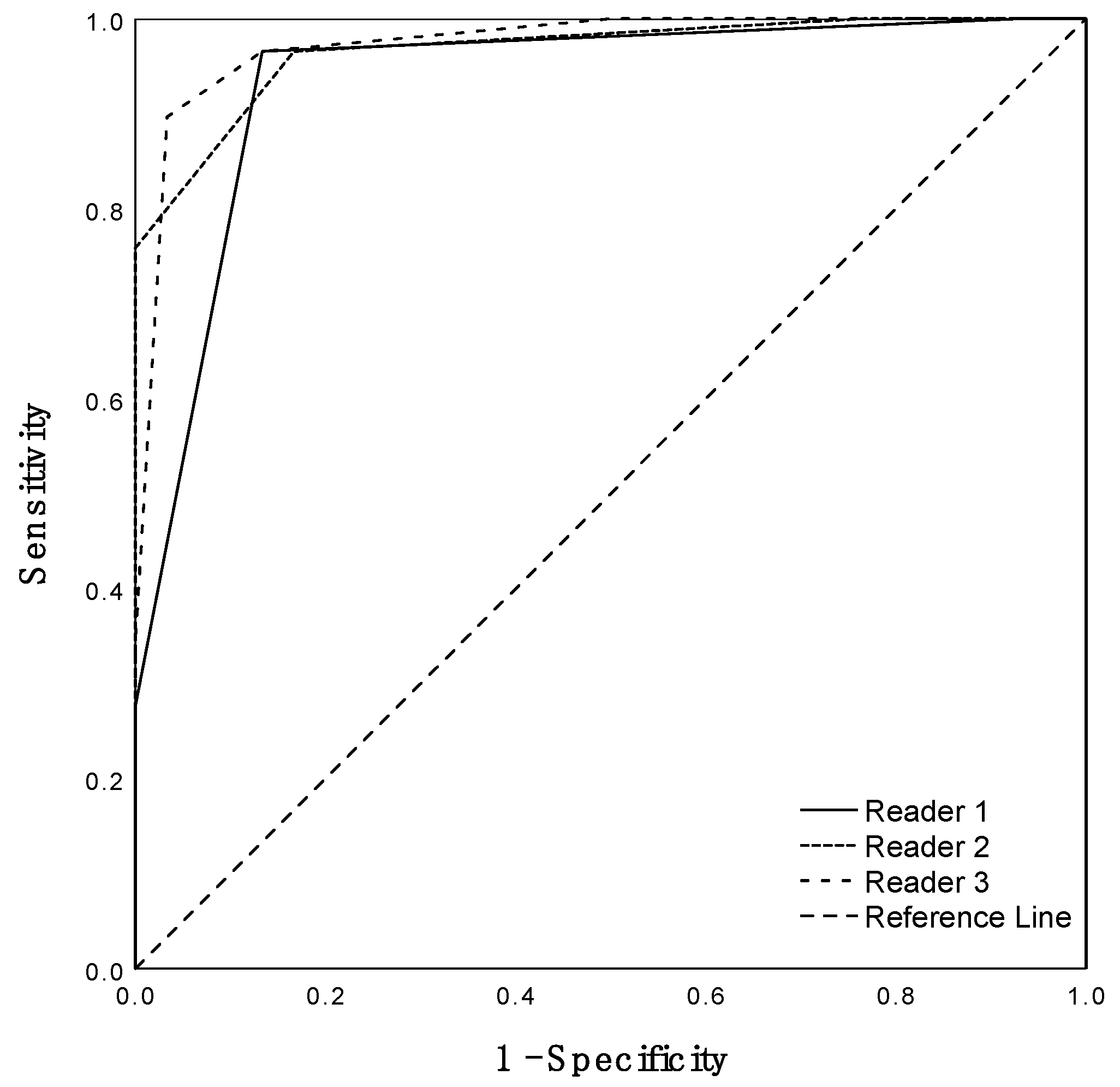
3.4. Inter-Rater Agreement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sai, K.K.S.; Zachar, Z.; Bingham, P.M.; Mintz, A. Metabolic PET Imaging in Oncology. Am. J. Roentgenol. 2017, 209, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, Y.; Gutowski, T.D.; Fisher, S.J.; Brown, R.S.; Wahl, R.L. Uptake of positron emission tomography tracers in experimental bacterial infections: A comparative biodistribution study of radiolabeled FDG, thymidine, L-methionine, 67Ga-citrate, and 125I-HSA. Eur. J. Nucl. Med. 1999, 26, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Kung, B.T.; Seraj, S.M.; Zadeh, M.Z.; Rojulpote, C.; Kothekar, E.; Ayubcha, C.; Ng, K.S.; Ng, K.K.; Au-Yong, T.K.; Werner, T.J.; et al. An update on the role of 18F-FDG-PET/CT in major infectious and inflammatory diseases. Am. J. Nucl. Med. Mol. Imaging 2019, 9, 255–273. [Google Scholar] [PubMed]
- Blockmans, D.; Maes, A.; Stroobants, S.; Nuyts, J.; Bormans, G.; Knockaert, D.; Bobbaers, H.; Mortelmans, L. New arguments for a vasculitic nature of polymyalgia rheumatica using positron emission tomography. Rheumatology 1999, 38, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Tatò, F.; Hoffmann, U. Giant cell arteritis: A systemic vascular disease. Vasc. Med. 2008, 13, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Brack, A.; Martinez-Taboada, V.; Stanson, A.; Goronzy, J.J.; Weyand, C.M. Disease pattern in cranial and large-vessel giant cell arteritis. Arthritis Rheum. 1999, 42, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Barraclough, K.; Mallen, C.D.; Helliwell, T.; Hider, S.L.; Dasgupta, B. Diagnosis and management of giant cell arteritis. Br. J. Gen. Pract. 2012, 62, 329–330. [Google Scholar] [CrossRef]
- Soussan, M.; Nicolas, P.; Schramm, C.; Katsahian, S.; Pop, G.; Fain, O.; Mekinian, A. Management of Large-Vessel Vasculitis With FDG-PET: A Systematic Literature Review and Meta-Analysis. Medicine 2015, 94, e622. [Google Scholar] [CrossRef]
- Besson, F.L.; Parienti, J.-J.; Bienvenu, B.; Prior, J.O.; Costo, S.; Bouvard, G.; Agostini, D. Diagnostic performance of 18F-fluorodeoxyglucose positron emission tomography in giant cell arteritis: A systematic review and meta-analysis. Eur. J. Nucl. Med. 2011, 38, 1764–1772. [Google Scholar] [CrossRef]
- Slart, R.H.J.A.; Writing Group. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: Joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1250–1269. [Google Scholar] [CrossRef]
- Meignan, M.; Gallamini, A.; Haioun, C. Report on the First International Workshop on interim-PET scan in lymphoma. Leuk. Lymphoma 2009, 50, 1257–1260. [Google Scholar] [CrossRef]
- Biggi, A.; Gallamini, A.; Chauvie, S.; Hutchings, M.; Kostakoglu, L.; Gregianin, M.; Meignan, M.; Malkowski, B.; Hofman, M.S.; Barrington, S.F. International Validation Study for Interim PET in ABVD-Treated, Advanced-Stage Hodgkin Lymphoma: Interpretation Criteria and Concordance Rate Among Reviewers. J. Nucl. Med. 2013, 54, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Furth, C.; Amthauer, H.; Hautzel, H.; Steffen, I.; Ruf, J.; Schiefer, J.; Schönberger, S.; Henze, G.; Grandt, R.; Hundsdoerfer, P.; et al. Evaluation of interim PET response criteria in paediatric Hodgkin’s lymphoma—Results for dedicated assessment criteria in a blinded dual-centre read. Ann. Oncol. 2011, 22, 1198–1203. [Google Scholar] [CrossRef]
- Dejaco, C.; Duftner, C.; Buttgereit, F.; Matteson, E.L.; Dasgupta, B. The spectrum of giant cell arteritis and polymyalgia rheumatica: Revisiting the concept of the disease. Rheumatology 2017, 56, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Watts, R.A.; Hatemi, G.; Burns, J.C.; Mohammad, A.J. Global epidemiology of vasculitis. Nat. Rev. Rheumatol. 2022, 18, 22–34. [Google Scholar] [CrossRef]
- Prior, J.A.; Ranjbar, H.; Belcher, J.; Mackie, S.L.; Helliwell, T.; Liddle, J.; Mallen, C.D. Diagnostic delay for giant cell arteritis—A systematic review and meta-analysis. BMC Med. 2017, 15, 120. [Google Scholar] [CrossRef]
- Ponte, C.; Martins-Martinho, J.; Luqmani, R.A. Diagnosis of giant cell arteritis. Rheumatology 2020, 59, iii5–iii16. [Google Scholar] [CrossRef]
- Koster, M.J.; Matteson, E.L.; Warrington, K.J. Large-vessel giant cell arteritis: Diagnosis, monitoring and management. Rheumatology 2018, 57, ii32–ii42. [Google Scholar] [CrossRef]
- Pugh, D.; Karabayas, M.; Basu, N.; Cid, M.C.; Goel, R.; Goodyear, C.S.; Grayson, P.C.; McAdoo, S.P.; Mason, J.C.; Owen, C.; et al. Large-vessel vasculitis. Nat. Rev. Dis. Prim. 2022, 7, 93. [Google Scholar] [CrossRef] [PubMed]
- Kluge, R.; Chavdarova, L.; Hoffmann, M.; Kobe, C.; Malkowski, B.; Montravers, F.; Kurch, L.; Georgi, T.; Dietlein, M.; Wallace, W.H.; et al. Inter-Reader Reliability of Early FDG-PET/CT Response Assessment Using the Deauville Scale after 2 Cycles of Intensive Chemotherapy (OEPA) in Hodgkin’s Lymphoma. PLoS ONE 2016, 11, e0149072. [Google Scholar] [CrossRef] [PubMed]
- Furth, C.; Erdrich, A.S.; Steffen, I.G.; Stiebler, R.M.; Kahraman, D.; Kobe, C.; Schonberger, S.; Grandt, R.; Hundsdoerfer, P.; Hauptmann, K.; et al. Interim PET response criteria in paediatric non-Hodgkin’s lymphoma. Nuklearmedizin 2013, 52, 148–156. [Google Scholar] [CrossRef]
- Kobe, C.; Goergen, H.; Baues, C.; Kuhnert, G.; Voltin, C.-A.; Zijlstra, J.; Hoekstra, O.; Mettler, J.; Drzezga, A.; Engert, A.; et al. Outcome-based interpretation of early interim PET in advanced-stage Hodgkin lymphoma. Blood 2018, 132, 2273–2279. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.; Federico, M.; Kirkwood, A.; Fosså, A.; Berkahn, L.; Carella, A.; D’Amore, F.; Enblad, G.; Franceschetto, A.; Fulham, M.; et al. Adapted Treatment Guided by Interim PET-CT Scan in Advanced Hodgkin’s Lymphoma. N. Engl. J. Med. 2016, 374, 2419–2429. [Google Scholar] [CrossRef] [PubMed]
- Radford, J.; Illidge, T.; Counsell, N.; Hancock, B.; Pettengell, R.; Johnson, P.; Wimperis, J.; Culligan, D.; Popova, B.; Smith, P.; et al. Results of a Trial of PET-Directed Therapy for Early-Stage Hodgkin’s Lymphoma. N. Engl. J. Med. 2015, 372, 1598–1607. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, stag-ing, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Lee, Y.; Choi, S.; Ji, J.; Song, G. Diagnostic accuracy of 18F-FDG PET or PET/CT for large vessel vasculitis: A meta-analysis. Z. Für Rheumatol. 2016, 75, 924–931. [Google Scholar] [CrossRef]
- Besson, F.L.; de Boysson, H.; Parienti, J.-J.; Bouvard, G.; Bienvenu, B.; Agostini, D. Towards an optimal semiquantitative approach in giant cell arteritis: An 18F-FDG PET/CT case-control study. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 155–166. [Google Scholar] [CrossRef]
- Hautzel, H.; Sander, O.; Heinzel, A.; Schneider, M.; Müller, H.-W. Assessment of Large-Vessel Involvement in Giant Cell Arteritis with 18F-FDG PET: Introducing an ROC-Analysis–Based Cutoff Ratio. J. Nucl. Med. 2008, 49, 1107–1113. [Google Scholar] [CrossRef]
- Walter, M.A.; Melzer, R.A.; Schindler, C.; Müller-Brand, J.; Tyndall, A.; Nitzsche, E.U. The value of [18F]FDG-PET in the diagnosis of large-vessel vasculitis and the assessment of activity and extent of disease. Eur. J. Nucl. Med. 2005, 32, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, M.; Briel, M.; Daikeler, T.; Walker, U.A.; Rasch, H.; Berg, S.; Ng, Q.K.T.; Raatz, H.; Jayne, D.; Kötter, I.; et al. The impact of 18F-FDG PET on the management of patients with suspected large vessel vasculitis. Eur. J. Nucl. Med. 2012, 39, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Koenigkam-Santos, M.; Sharma, P.; Kalb, B.; Oshinski, J.N.; Weyand, C.M.; Goronzy, J.J.; Martin, D.R. Magnetic Resonance Angiography in Extracranial Giant Cell Arteritis. JCR J. Clin. Rheumatol. 2011, 17, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Meller, J.; Strutz, F.; Siefker, U.; Scheel, A.; Sahlmann, C.O.; Lehmann, K.; Conrad, M.; Vosshenrich, R. Early diagnosis and follow-up of aortitis with [18F]FDG PET and MRI. Eur. J. Nucl. Med. 2003, 30, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Lensen, K.D.F.; Comans, E.F.I.; Voskuyl, A.E.; van der Laken, C.J.; Brouwer, E.; Zwijnenburg, A.T.; Arias-Bouda, L.M.P.; Glaudemans, A.W.J.M.; Slart, R.H.J.A.; Smulders, Y.M. Large-Vessel Vasculitis: Interobserver Agreement and Diagnostic Accuracy of18F-FDG-PET/CT. BioMed Res. Int. 2015, 2015, 914692. [Google Scholar] [CrossRef]
- van der Geest, K.S.M.; Treglia, G.; Glaudemans, A.W.J.M.; Brouwer, E.; Sandovici, M.; Jamar, F.; Gheysens, O.; Slart, R.H.J.A. Diagnostic value of [18F]FDG-PET/CT for treatment monitoring in large vessel vasculitis: A systematic review and meta-analysis. Eur. J. Nucl. Med. 2021, 48, 3886–3902. [Google Scholar] [CrossRef]
- Mach, E. Über die Wirkung der räumlichen Verteilung des Lichtreizes auf die Netzhaut (I). In Sitzungsberichte der Kaiserlichen Akademie der Wissenschaften; Mathematisch-Naturwissenschaftliche Classe 52, K. k. Hof- und Staatsdruckerei: Vienna, Austria, 1865; pp. 303–322. [Google Scholar]
- Boellaard, R.; Kobe, C.; Zijlstra, J.M.; Mikhaeel, N.G.; Johnson, P.W.; Müller, S.; Dührsen, U.; Hoekstra, O.S.; Barrington, S. Does PET Reconstruction Method Affect Deauville Scoring in Lymphoma Patients? J. Nucl. Med. 2018, 59, 1167–1169. [Google Scholar] [CrossRef]
- Kuhnert, G.; Boellaard, R.; Sterzer, S.; Kahraman, D.; Scheffler, M.; Wolf, J.; Dietlein, M.; Drzezga, A.; Kobe, C. Impact of PET/CT image reconstruction methods and liver uptake normalization strategies on quantitative image analysis. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 249–258. [Google Scholar] [CrossRef]
- Bucerius, J.; Mani, V.; Moncrieff, C.; Machac, J.; Fuster, V.; Farkouh, M.E.; Tawakol, A.; Rudd, J.H.F.; Fayad, Z.A. Optimizing 18F-FDG PET/CT imaging of vessel wall inflammation: The impact of 18F-FDG circulation time, injected dose, uptake parameters, and fasting blood glucose levels. Eur. J. Nucl. Med. Mol. Imaging 2013, 41, 369–383. [Google Scholar] [CrossRef]
- Blomberg, B.A.; Thomassen, A.; Takx, R.A.P.; Hildebrandt, M.G.; Simonsen, J.A.; Buch-Olsen, K.M.; Diederichsen, A.C.P.; Mickley, H.; Alavi, A.; Høilund-Carlsen, P.F. Delayed 18F-fluorodeoxyglucose PET/CT imaging improves quantitation of atherosclerotic plaque inflammation: Results from the CAMONA study. J. Nucl. Cardiol. 2014, 21, 588–597. [Google Scholar] [CrossRef]
- Dejaco, C.; Ramiro, S.; Duftner, C.; Besson, F.L.; Bley, T.A.; Blockmans, D.; Brouwer, E.; Cimmino, M.A.; Clark, E.; Dasgupta, B.; et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice. Ann. Rheum. Dis. 2018, 77, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Hunder, G.G.; Bloch, D.A.; Michel, B.A.; Stevens, M.B.; Arend, W.P.; Do, L.H.C.; Edworthy, S.M.; Fauci, A.S.; Leavitt, R.Y.; Lie, J.T.; et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum. 1990, 33, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.H.; Tuckwell, K.; Dimonaco, S.; Klearman, M.; Aringer, M.; Blockmans, D.; Brouwer, E.; Cid, M.C.; Dasgupta, B.; Rech, J.; et al. Trial of Tocilizumab in Giant-Cell Arteritis. N. Engl. J. Med. 2017, 377, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.L.; Ngam, P.I.; Tan, K.M.; Ng, D.C.E.; Lim, S.T.; Chan, J.Y. The exact Deauville score, NABS score and high SUVmax predicts outcome in extranodal natural killer/T-cell lymphoma. Ann. Nucl. Med. 2021, 35, 557–568. [Google Scholar] [CrossRef]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Patient Cohort | Control Cohort |
|---|---|---|
| Total (n) | 29 | 30 |
| Female (n) | 16/29 | 18/30 |
| Male (n) | 13/29 | 12/30 |
| Age (years) | 66 (range, 51–83) | 66 (range, 49–79) |
| Activity (MBq) | 269 (IQR, 245–302.5) | 274.5 (IQR, 251–300.25) |
| Uptake time (min) | 67 (IQR, 64–80) | 71.5 (IQR, 65–84) |
| Blood glucose (mmol/L) | 5.4 (IQR, 4.9–6) | 5.6 (IQR, 5–6.3) |
| CRP (mg/L) | 36.9 (IQR, 18.95–65.1) | 38.15 (IQR, 3.8–84.9) * |
| Reader | TP | TN | FP | FN | Accuracy | Sensitivity | Specificity | PPV | NPV | AUC | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | 95%-CI | % | 95%-CI | % | 95%-CI | % | 95%-CI | % | 95%-CI | % | 95%-CI | |||||
| 1 | 28 | 26 | 4 | 1 | 91.5 | 81.3–97.2 | 96.6 | 82.2–99.9 | 86.7 | 69.3–96.2 | 87.5 | 71.0–96.5 | 96.3 | 81.0–99.9 | 0.94 | 0.87–1.00 |
| 2 | 28 | 25 | 5 | 1 | 89.8 | 79.2–96.2 | 96.6 | 82.2–99.9 | 83.3 | 65.3–94.4 | 84.9 | 68.1–94.9 | 96.2 | 80.4–99.9 | 0.97 | 0.93–1.01 |
| 3 | 26 | 29 | 1 | 3 | 93.2 | 83.5–98.1 | 89.7 | 72.7–97.8 | 96.7 | 82.8–99.9 | 96.3 | 81.0–99.9 | 90.6 | 75.0–98.0 | 0.97 | 0.94–1.01 |
| Average | 91.5 | 94.3 | 88.9 | 89.6 | 94.3 | 0.96 | ||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siefert, J.; Kaufmann, J.; Thiele, F.; Walter-Rittel, T.; Rogasch, J.; Biesen, R.; Burmester, G.R.; Amthauer, H.; Schneider, U.; Furth, C. Performance of Deauville Criteria in [18F]FDG-PET/CT Diagnostics of Giant Cell Arteritis. Diagnostics 2023, 13, 157. https://doi.org/10.3390/diagnostics13010157
Siefert J, Kaufmann J, Thiele F, Walter-Rittel T, Rogasch J, Biesen R, Burmester GR, Amthauer H, Schneider U, Furth C. Performance of Deauville Criteria in [18F]FDG-PET/CT Diagnostics of Giant Cell Arteritis. Diagnostics. 2023; 13(1):157. https://doi.org/10.3390/diagnostics13010157
Chicago/Turabian StyleSiefert, Jeffrey, Jonas Kaufmann, Felix Thiele, Thula Walter-Rittel, Julian Rogasch, Robert Biesen, Gerd R. Burmester, Holger Amthauer, Udo Schneider, and Christian Furth. 2023. "Performance of Deauville Criteria in [18F]FDG-PET/CT Diagnostics of Giant Cell Arteritis" Diagnostics 13, no. 1: 157. https://doi.org/10.3390/diagnostics13010157