
Morphological and Compositional Features of Chronic Internal Carotid Artery Occlusion in MR Vessel Wall Imaging Predict Successful Endovascular Recanalization

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Carotid MR-VWI
2.2. DSA Assessment
2.3. Endovascular Recanalization
2.4. Statistical Analysis
3. Results
3.1. Imaging Characteristics
3.2. Association between MR-VWI Characteristics of CICAO and Successful Recanalization
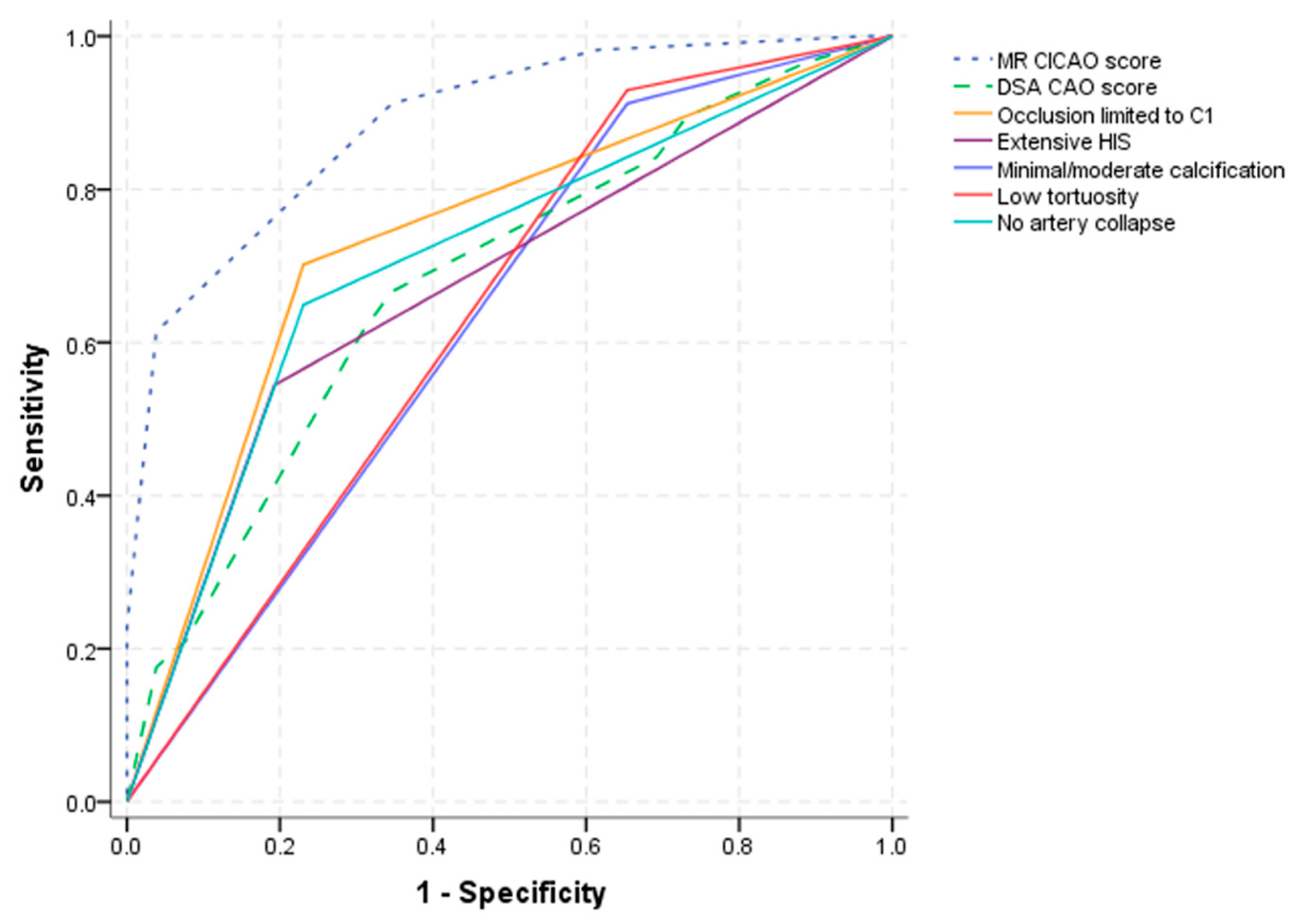
3.3. The MR-VWI ICAO Score
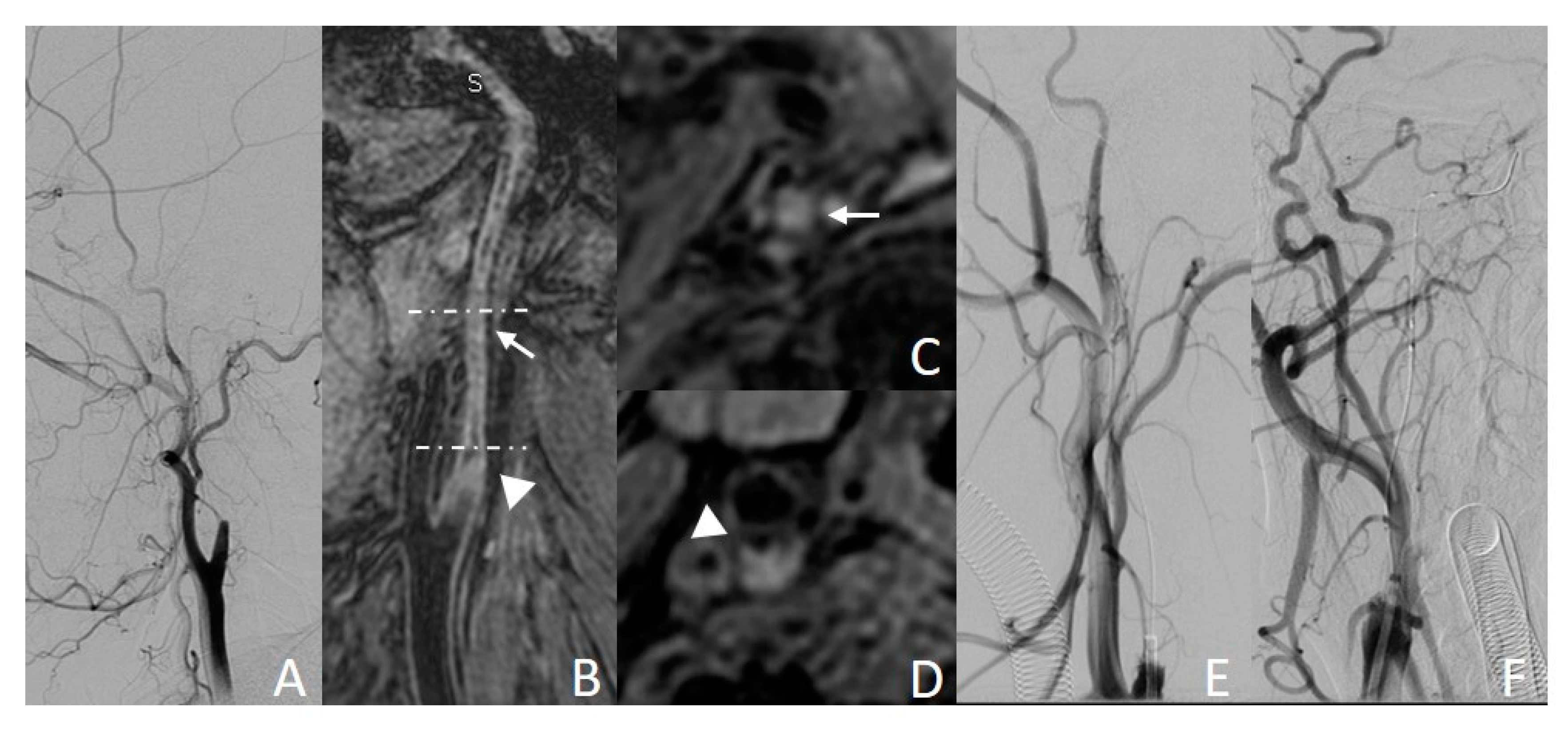
3.3.1. Example Case 1
3.3.2. Example Case 2
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CICAO | chronic internal carotid artery occlusion |
| MR-VWI | MR vessel wall imaging |
| CAO | carotid artery occlusion |
| MERGE | motion-sensitized driven equilibrium prepared rapid gradient echo |
| SNAP | simultaneous non-contrast angiography and intraplaque hemorrhage |
| MPR | multi-planar reconstruction |
References
- Poorthuis, M.H.; Sherliker, P.; Morris, D.R.; Massa, M.S.; Clarke, R.; Staplin, N.; Lewington, S.; de Borst, G.J.; Bulbulia, R.; Halliday, A. Development and Internal Validation of a Risk Score to Detect Asymptomatic Carotid Stenosis. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, M.L.; Flemming, K.D.; McClelland, R.; Jorgensen, N.W.; Brown, R.D., Jr. Population-based study of symptomatic internal carotid artery occlusion: Incidence and long-term follow-up. Stroke 2004, 35, e349–e352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hause, S.; Oldag, A.; Breja, A.; Neumann, J.; Wilcke, J.; Schreiber, S.; Heinze, H.-J.; Skalej, M.; Halloul, Z.; Goertler, M. Acute symptomatic extracranial internal carotid occlusion—Natural course and clinical impact. Vasa 2020, 49, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-S.; Chiu, M.-J.; Wu, Y.-W.; Huang, C.-C.; Chao, C.-C.; Chen, Y.-H.; Lin, H.-J.; Li, H.-Y.; Chen, Y.-F.; Lin, L.-C.; et al. Neurocognitive improvement after carotid artery stenting in patients with chronic internal carotid artery occlusion and cerebral ischemia. Stroke 2011, 42, 2850–2854. [Google Scholar] [CrossRef] [Green Version]
- Yao, Y.-D.; Liu, A.-F.; Qiu, H.-C.; Zhou, J.; Li, C.; Wang, Q.; Lv, J.; Jiang, W.-J. Outcomes of late endovascular recanalization for symptomatic non-acute atherosclerotic intracranial large artery occlusion. Clin. Neurol. Neurosurg. 2019, 187, 105567. [Google Scholar] [CrossRef]
- Zanaty, M.; Howard, S.; Roa, J.A.; Alvarez, C.M.; Kung, D.K.; McCarthy, D.J.; Samaniego, E.A.; Nakagawa, D.; Starke, R.M.; Limaye, K.; et al. Cognitive and cerebral hemodynamic effects of endovascular recanalization of chronically occluded cervical internal carotid artery: Single-center study and review of the literature. J. Neurosurg. 2019, 132, 1158–1166. [Google Scholar] [CrossRef]
- Saini, H.; Cerejo, R.; Williamson, R.; Malhotra, K. Internal Carotid Artery Occlusion: Management. Curr. Neurol. Neurosci. Rep. 2022, 22, 383–388. [Google Scholar] [CrossRef]
- Terada, T.; Okada, H.; Nanto, M.; Shintani, A.; Yoshimura, R.; Kakishita, K.; Masuo, O.; Matsumoto, H.; Itakura, T.; Ohshima, K.; et al. Endovascular recanalization of the completely occluded internal carotid artery using a flow reversal system at the subacute to chronic stage. J. Neurosurg. 2010, 112, 563–571. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-H.; Leong, W.-S.; Lin, M.-S.; Huang, C.-C.; Hung, C.-S.; Li, H.-Y.; Chan, K.-K.; Yeh, C.-F.; Chiu, M.-J.; Kao, H.-L. Predictors for Successful Endovascular Intervention in Chronic Carotid Artery Total Occlusion. JACC Cardiovasc. Interv. 2016, 9, 1825–1832. [Google Scholar] [CrossRef]
- Lee, C.W.; Lin, Y.H.; Liu, H.M.; Wang, Y.F.; Chen, Y.F.; Wang, J.L. Predicting procedure successful rate and 1-year patency after endovascular recanalization for chronic carotid artery occlusion by CT angiography. Int. J. Cardiol. 2016, 221, 772–776. [Google Scholar] [CrossRef]
- Kaufmann, T.J.; Kallmes, D.F. Utility of MRA and CTA in the Evaluation of Carotid Occlusive Disease. Semin. Vasc. Surg. 2005, 18, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.J.; Eliasziw, M.; Rothwell, P.M.; Schmidt, M.H.; Warlow, C.; Barnett, H.J.M. Identification, Prognosis, and Management of Patients with Carotid Artery Near Occlusion. Am. J. Neuroradiol. 2005, 26, 2086–2094. [Google Scholar] [PubMed]
- Debrey, S.M.; Yu, H.; Lynch, J.K.; Lövblad, K.O.; Wright, V.L.; Janket, S.J.D.; Baird, A.E. Diagnostic accuracy of magnetic resonance angiography for internal carotid artery disease: A systematic review and meta-analysis. Stroke 2008, 39, 2237–2248. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Choi, J.; Choe, Y.H. Coronary Artery Total Occlusion: MR Angiographic Imaging Findings and Success Rates of Percutaneous Coronary Intervention according to Intraluminal Signal Intensity Patterns. Radiology 2016, 279, 84–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasan, D.; Zanaty, M.; Starke, R.M.; Atallah, E.; Chalouhi, N.; Jabbour, P.; Singla, A.; Guerrero, W.R.; Nakagawa, D.; Samaniego, E.A.; et al. Feasibility, safety, and changes in systolic blood pressure associated with endovascular revascularization of symptomatic and chronically occluded cervical internal carotid artery using a newly suggested radiographic classification of chronically occluded cervical internal carotid artery: Pilot study. J Neurosurg. 2018, 130, 1468–1477. [Google Scholar]
- Wang, J.; Yarnykh, V.L.; Yuan, C. Enhanced image quality in black-blood MRI using the improved motion-sensitized driven-equilibrium (iMSDE) sequence. J. Magn. Reson. Imaging 2010, 31, 1256–1263. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Wang, J.; Liu, X.; Zhao, X.; Hippe, D.S.; Cao, Y.; Wan, J.; Yuan, C.; Xu, J. Assessment of Carotid Artery Atherosclerotic Disease by Using Three-dimensional Fast Black-Blood MR Imaging: Comparison with DSA. Radiology 2015, 274, 508–516. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Ding, S.; Zhao, H.; Sun, B.; Li, X.; Zhou, Y.; Wan, J.; Degnan, A.J.; Xu, J.; Zhu, C. Evaluation of chronic carotid artery occlusion by non-contrast 3D-MERGE MR vessel wall imaging: Comparison with 3D-TOF-MRA, contrast-enhanced MRA, and DSA. Eur. Radiol. 2020, 30, 5805–5814. [Google Scholar] [CrossRef]
- Wang, J.; Börnert, P.; Zhao, H.; Hippe, D.; Zhao, X.; Balu, N.; Ferguson, M.S.; Hatsukami, T.S.; Xu, J.; Yuan, C.; et al. Simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) imaging for carotid atherosclerotic disease evaluation. Magn. Reson. Med. 2013, 69, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Zhao, H.; Li, J.; Zhou, Z.; Li, R.; Balu, N.; Yuan, C.; Chen, H.; Zhao, X. Evaluation of carotid atherosclerotic plaque surface characteristics utilizing simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) technique. J. Magn. Reson. Imaging 2018, 47, 634–639. [Google Scholar] [CrossRef] [Green Version]
- Corti, R.; Osende, J.I.; Fayad, Z.A.; Fallon, J.T.; Fuster, V.; Mizsei, G.; Dickstein, E.; Drayer, B.; Badimon, J.J. In vivo noninvasive detection and age definition of arterial thrombus by MRI. J. Am. Coll. Cardiol. 2002, 39, 1366–1373. [Google Scholar] [CrossRef] [PubMed]
- Lettau, M.; Laible, M.; Barrows, R.J.; Heiland, S.; Bendszus, M.; Hahnel, S. 3-T contrast-enhanced MR angiography with parallel imaging in cerebral venous and sinus thrombosis. J. Neuroradiol. 2011, 38, 275–282. [Google Scholar] [CrossRef]
- Liu, J.; Balu, N.; Hippe, D.S.; Ferguson, M.S.; Martinez-Malo, V.; DeMarco, J.K.; Zhu, D.C.; Ota, H.; Sun, J.; Xu, D.; et al. Semi-automatic carotid intraplaque hemorrhage detection and quantification on Magnetization-Prepared Rapid Acquisition Gradient-Echo (MP-RAGE) with optimized threshold selection. J. Cardiovasc. Magn. Reson. 2016, 18, 41. [Google Scholar] [CrossRef] [Green Version]
- Saam, T.; Ferguson, M.; Yarnykh, V.; Takaya, N.; Xu, D.; Polissar, N.; Hatsukami, T.; Yuan, C. Quantitative evaluation of carotid plaque composition by in vivo MRI. Arter. Thromb. Vasc. Biol. 2005, 25, 234–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morino, Y.; Abe, M.; Morimoto, T.; Kimura, T.; Hayashi, Y.; Muramatsu, T.; Ochiai, M.; Noguchi, Y.; Kato, K.; Shibata, Y.; et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: The J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc. Interv. 2011, 4, 213–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, F.; Sun, X.; Zhang, H.; Ma, N.; Mo, D.; Miao, Z. Endovascular Recanalization for Nonacute Intracranial Vertebral Artery Occlusion According to a New Classification. Stroke 2020, 51, 3340–3343. [Google Scholar] [CrossRef]
- Gao, F.; Sun, X.; Guo, X.; Li, D.; Xu, G.D.; Miao, Z.R. Endovascular Recanalization of Symptomatic Nonacute Intracranial Internal Carotid Artery Occlusion: Proposal of a New Angiographic Classification. Am. J. Neuroradiol. 2021, 42, 299–305. [Google Scholar] [CrossRef]
- Myrcha, P.; Gloviczki, P. A systematic review of endovascular treatment for chronic total occlusion of the internal carotid artery. Ann. Transl. Med. 2021, 9, 1203. [Google Scholar] [CrossRef]
- Li, J.; Wang, C.; Zou, S.; Liu, Y.; Qu, L. Hybrid Surgery for Nontaper or Nonstump Lesions in Symptomatic Subacute or Chronic Internal Carotid Occlusion: A Better Solution. World Neurosurg. 2019, 122, e1416–e1425. [Google Scholar] [CrossRef]
- Zanaty, M.; Roa, J.A.; Jabbour, P.M.; Samaniego, E.A.; Hasan, D.M. Recanalization of the Chronically Occluded Internal Carotid Artery: Review of the Literature. World Neurosurg. X 2020, 5, 100067. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 83) | Success Group (n = 57) | Failure Group (n = 26) | p Value | |
|---|---|---|---|---|
| Age (years) | 62.6 ± 7.0 | 62.6 ± 7.1 | 62.5 ± 6.8 | 0.945 |
| Male sex | 73 (88.0) | 53 (93.0) | 20 (76.9) | 0.064 |
| Smoking | 32 (38.6) | 26 (45.6) | 6 (23.1) | 0.057 |
| Alcohol drinking | 17 (20.5) | 14 (24.6) | 3 (11.5) | 0.244 |
| Hypertension | 59 (71.1) | 44 (77.2) | 15 (57.7) | 0.116 |
| Diabetes | 36 (43.4) | 28 (49.1) | 8 (30.8) | 0.154 |
| Dyslipidemia | 24 (28.9) | 16 (28.1) | 8 (30.8) | 0.800 |
| Symptom status | 0.073 | |||
| Ischemic event ≤3 months | 57 (68.7) | 43 (75.4) | 14 (53.8) | |
| Ischemic event >3 months | 26 (31.3) | 14 (24.6) | 12 (46.2) | |
| Perioperative complication | 9 (10.8) | 2 (3.5) | 7 (26.9) | 0.003 |
| Perforation | 2 (2.4) | 0 (0.0) | 2 (7.7) | 0.096 |
| Dissection | 6 (7.2) | 1 (1.8) | 5 (19.2) | 0.011 |
| Thrombosis | 1 (1.2) | 1 (1.8) | 0 (0.0) | 1.000 |
| Stroke within 30 days after procedure | 2 (2.4) | 1 (1.8) | 1 (3.8) | 0.531 |
| MR-VWI characteristics | ||||
| Occlusion length in C1 | 62.8 ± 23.8 | 61.7 ± 26.1 | 65.1 ± 18 | 0.552 |
| Proximal stump morphology | 0.619 | |||
| Tapered | 32 (38.6) | 20 (35.1) | 12 (46.2) | |
| Blunt | 28 (33.7) | 20 (35.1) | 8 (30.8) | |
| Absent | 23 (27.7) | 17 (29.8) | 6 (23.1) | |
| Occlusions limited to C1 | 46 (55.4) | 40 (70.2) | 6 (23.1) | 0.001 |
| Extensive HIS | 36 (43.4) | 31 (54.4) | 5 (19.2) | 0.004 |
| Extensive calcification | 14 (16.9) | 5 (8.8) | 9 (34.6) | 0.009 |
| High tortuosity | 13 (15.7) | 4 (7.0) | 9 (34.6) | 0.003 |
| Artery collapse | 40 (48.2) | 20 (35.1) | 20 (76.9) | 0.001 |
| DSA characteristics * | ||||
| Proximal stump morphology | 0.519 | |||
| Tapered | 35 (42.2) | 22 (38.6) | 13 (50.0) | |
| Blunt | 26 (31.3) | 18 (31.6) | 8 (30.8) | |
| Absent | 22 (26.5) | 17 (29.8) | 5 (19.2) | |
| Distal ICA reconstitution with contralateral injection | 29 (34.9) | 14 (24.6) | 15 (57.7) | 0.006 |
| Level of distal ICA reconstitution at or before clinoid segment | 45 (54.2) | 38 (66.7) | 7 (26.9) | 0.001 |
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Occlusions limited to C1 | 13.84 | 3.44–55.76 | <0.001 | 9.14 | 2.12–39.34 | 0.003 |
| Extensive HIS | 3.99 | 1.20–13.22 | 0.024 | 4.02 | 1.09–14.90 | 0.037 |
| Extensive calcification | 0.19 | 0.05–0.72 | 0.014 | 0.31 | 0.07–1.33 | 0.115 |
| High tortuosity | 0.12 | 0.03–0.51 | 0.004 | 0.18 | 0.04–0.82 | 0.027 |
| Artery collapse | 0.20 | 0.06–0.63 | 0.006 | 0.23 | 0.07–0.80 | 0.021 |
| β Coefficient | OR | 95% CI | p Value | |
|---|---|---|---|---|
| Occlusions limited to C1 | 1.72 | 5.56 | 1.33–23.23 | 0.019 |
| Extensive HIS | 1.55 | 4.67 | 1.01–21.84 | 0.049 |
| Extensive calcification | −1.81 | 0.16 | 0.03–0.97 | 0.046 |
| High tortuosity | −2.37 | 0.09 | 0.11–0.79 | 0.029 |
| Artery collapse | −2.27 | 0.10 | 0.20–0.52 | 0.006 |
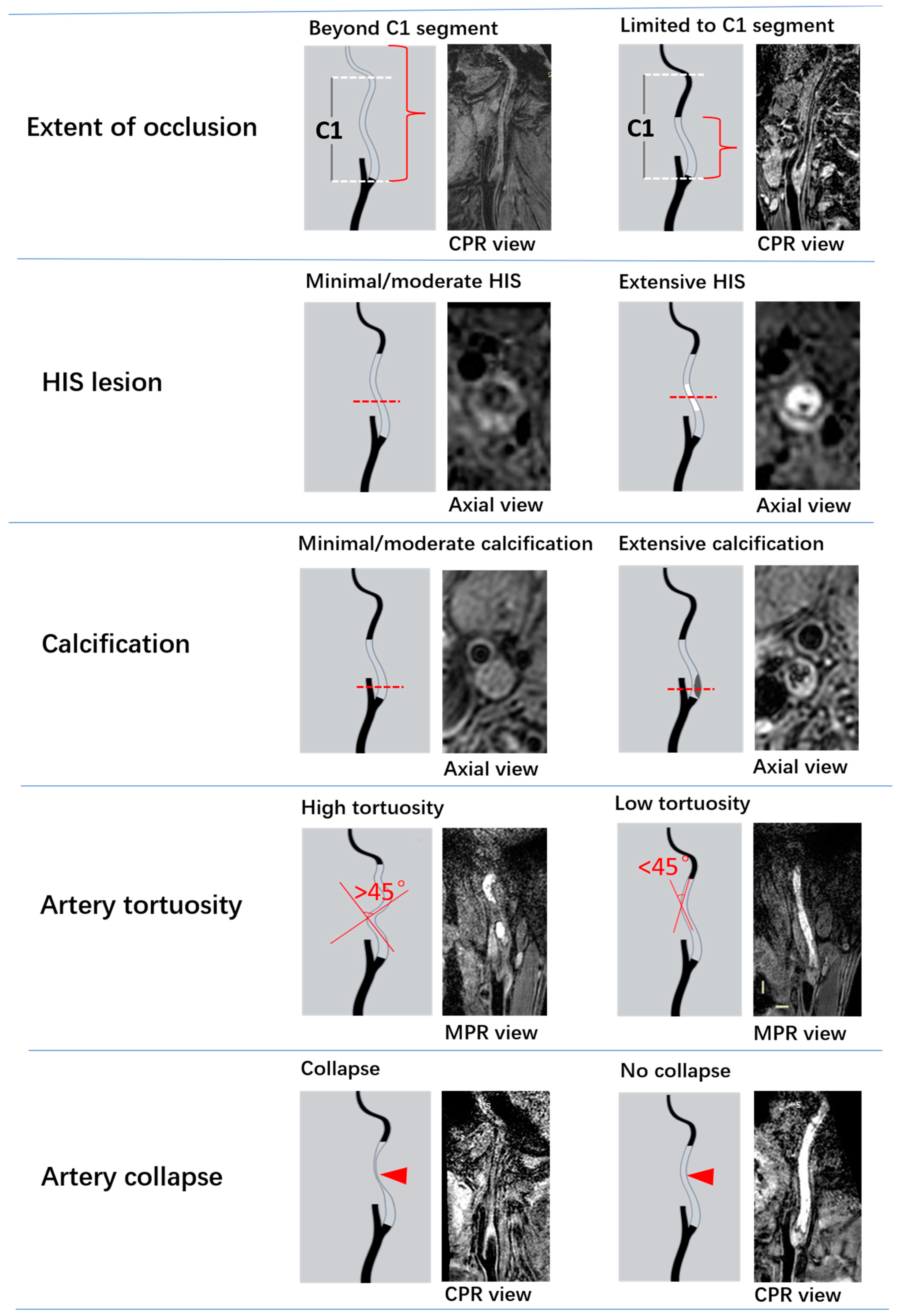
| Variable | Categories | Score Point |
|---|---|---|
| Extent of occlusion | Beyond the C1 segment | 0 |
| Limited to the C1 segment | 1 | |
| HIS | Minimal/moderate HIS | 0 |
| Extensive HIS | 1 | |
| Calcification | Extensive calcification | 0 |
| Minimal/moderate calcification | 1 | |
| Artery tortuosity | With high tortuosity | 0 |
| With low tortuosity | 1 | |
| Artery collapse | With collapse | 0 |
| Without collapse | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Ding, S.; Zhao, B.; Sun, B.; Guo, Q.; Pan, Y.; Li, X.; Wang, L.; Zhang, J.; Tian, J.; et al. Morphological and Compositional Features of Chronic Internal Carotid Artery Occlusion in MR Vessel Wall Imaging Predict Successful Endovascular Recanalization. Diagnostics 2023, 13, 147. https://doi.org/10.3390/diagnostics13010147
Zhang J, Ding S, Zhao B, Sun B, Guo Q, Pan Y, Li X, Wang L, Zhang J, Tian J, et al. Morphological and Compositional Features of Chronic Internal Carotid Artery Occlusion in MR Vessel Wall Imaging Predict Successful Endovascular Recanalization. Diagnostics. 2023; 13(1):147. https://doi.org/10.3390/diagnostics13010147
Chicago/Turabian StyleZhang, Jin, Shenghao Ding, Bing Zhao, Beibei Sun, Qinhua Guo, Yaohua Pan, Xiao Li, Lingling Wang, Jianjian Zhang, Jiaqi Tian, and et al. 2023. "Morphological and Compositional Features of Chronic Internal Carotid Artery Occlusion in MR Vessel Wall Imaging Predict Successful Endovascular Recanalization" Diagnostics 13, no. 1: 147. https://doi.org/10.3390/diagnostics13010147