
Immunological Aspects of Von Hippel-Lindau Disease: A Focus on Neuro-Oncology and Myasthenia Gravis
 , , ,
, , ,  , , , , ,
, , , , , 
Abstract
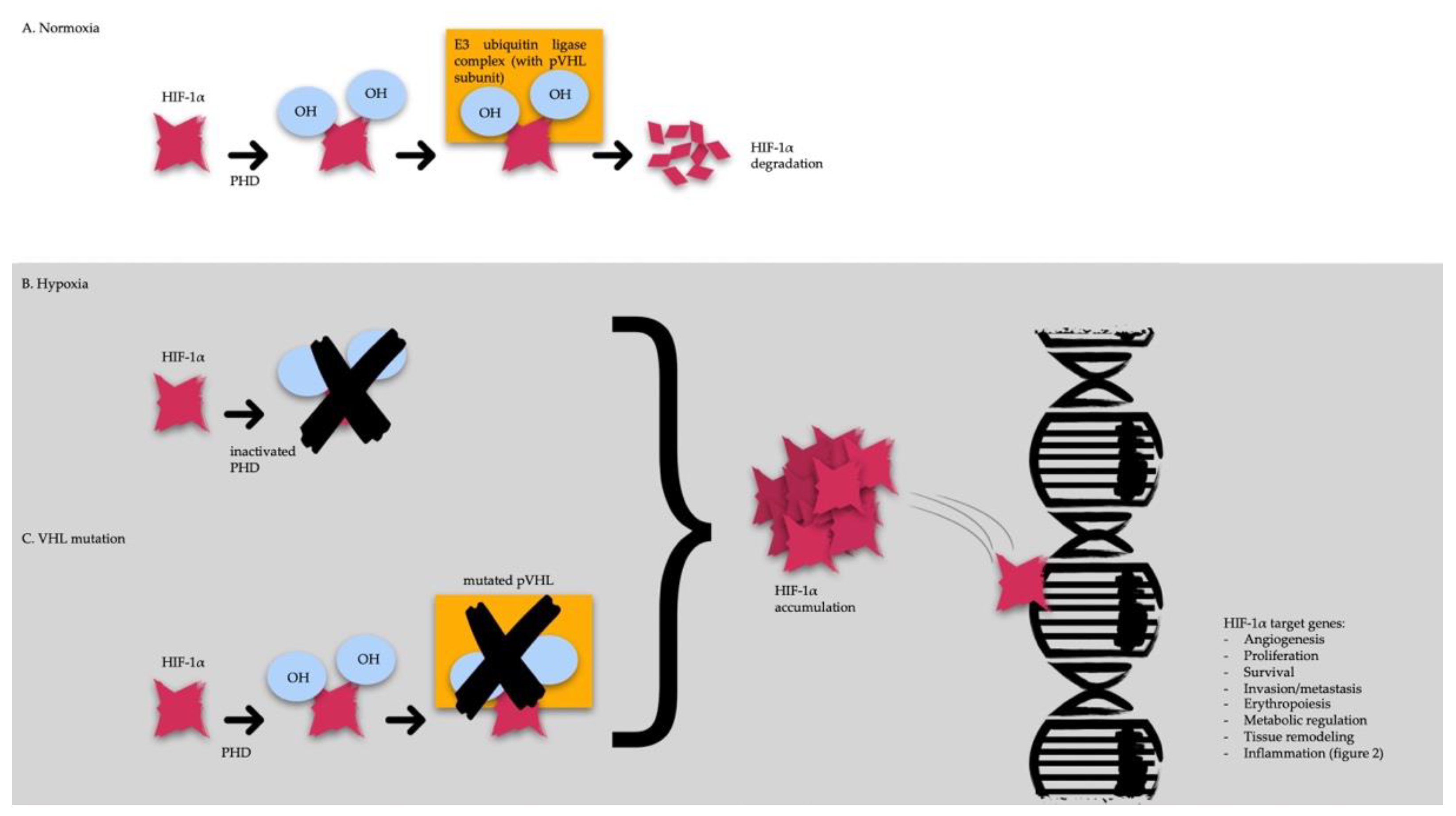
:1. VHL Disease: Definition and Pathogenesis
2. Influence of VHL/HIF Pathway Alterations on Tumor Immune Microenvironment
3. Oncological Therapeutical Aspect in VHL Disease
4. Neurosurgery’s Perspective on Patients with VHL Disease
5. Multidisciplinary Approach for Diagnosis and Surveillance in VHL Disease
6. VHL/HIF Axis in Inflammation and Autoimmunity
6.1. The Innate Immune System
6.2. The Adaptive Cell-Mediated Response
6.3. The Adaptive Humoral Response: B Cells
6.4. The Adaptive Humoral Response: CD4+ T Cells
7. VHL Disease and Myasthenia Gravis
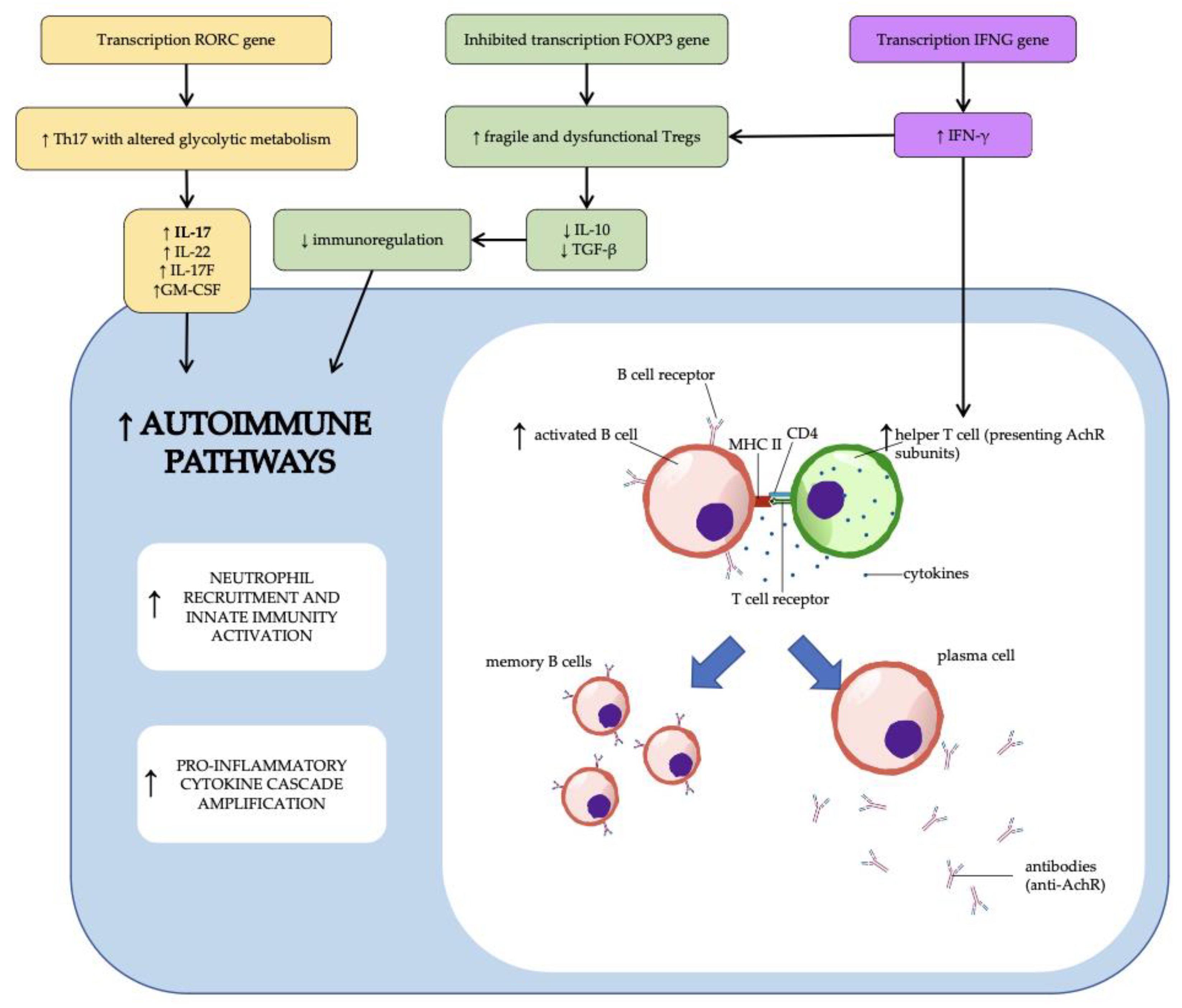
7.1. Myasthenia Gravis Autoimmune Pathways
7.2. Possible Interactions between Myasthenia Gravis and Von Hippel-Lindau Disease Immunological Pathways
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maher, E.R.; Iselius, L.; Yates, J.R.; Littler, M.; Benjamin, C.; Harris, R.; Sampson, J.; Williams, A.; Ferguson-Smith, M.A.; Morton, N. Von Hippel-Lindau Disease: A Genetic Study. J. Med. Genet. 1991, 28, 443–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binderup, M.L.M.; Galanakis, M.; Budtz-Jørgensen, E.; Kosteljanetz, M.; Luise Bisgaard, M. Prevalence, Birth Incidence, and Penetrance of von Hippel-Lindau Disease (VHL) in Denmark. Eur. J. Hum. Genet. EJHG 2017, 25, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.; Howard, E.; Giblin, C.; Clancy, T.; Spencer, H.; Huson, S.M.; Lalloo, F. Birth Incidence and Prevalence of Tumor-Prone Syndromes: Estimates from a UK Family Genetic Register Service. Am. J. Med. Genet. A. 2010, 152A, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Neumann, H.P.; Wiestler, O.D. Clustering of Features of von Hippel-Lindau Syndrome: Evidence for a Complex Genetic Locus. Lancet 1991, 337, 1052–1054. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, M.L.M.; Budtz-Jørgensen, E.; Bisgaard, M.L. Surveillance in von Hippel-Lindau Disease (VHL). Clin. Genet. 2010, 77, 49–59. [Google Scholar] [CrossRef]
- PDQ Cancer Genetics Editorial Board. Von Hippel-Lindau Disease (PDQ®): Health Professional Version. In PDQ Cancer Information Summaries; National Cancer Institute (US): Bethesda, MD, USA, 2002. [Google Scholar]
- Latif, F.; Tory, K.; Gnarra, J.; Yao, M.; Duh, F.M.; Orcutt, M.L.; Stackhouse, T.; Kuzmin, I.; Modi, W.; Geil, L. Identification of the von Hippel-Lindau Disease Tumor Suppressor Gene. Science 1993, 260, 1317–1320. [Google Scholar] [CrossRef]
- Knudson, A.G. Genetics of Human Cancer. Annu. Rev. Genet. 1986, 20, 231–251. [Google Scholar] [CrossRef]
- Knudson, A.G.; Strong, L.C. Mutation and Cancer: Neuroblastoma and Pheochromocytoma. Am. J. Hum. Genet. 1972, 24, 514–532. [Google Scholar]
- Maxwell, P.H.; Wiesener, M.S.; Chang, G.W.; Clifford, S.C.; Vaux, E.C.; Cockman, M.E.; Wykoff, C.C.; Pugh, C.W.; Maher, E.R.; Ratcliffe, P.J. The Tumour Suppressor Protein VHL Targets Hypoxia-Inducible Factors for Oxygen-Dependent Proteolysis. Nature 1999, 399, 271–275. [Google Scholar] [CrossRef]
- Ivan, M.; Kondo, K.; Yang, H.; Kim, W.; Valiando, J.; Ohh, M.; Salic, A.; Asara, J.M.; Lane, W.S.; Kaelin, W.G. HIFalpha Targeted for VHL-Mediated Destruction by Proline Hydroxylation: Implications for O2 Sensing. Science 2001, 292, 464–468. [Google Scholar] [CrossRef]
- Jaakkola, P.; Mole, D.R.; Tian, Y.M.; Wilson, M.I.; Gielbert, J.; Gaskell, S.J.; von Kriegsheim, A.; Hebestreit, H.F.; Mukherji, M.; Schofield, C.J.; et al. Targeting of HIF-Alpha to the von Hippel-Lindau Ubiquitylation Complex by O2-Regulated Prolyl Hydroxylation. Science 2001, 292, 468–472. [Google Scholar] [CrossRef]
- Keith, B.; Johnson, R.S.; Simon, M.C. HIF1α and HIF2α: Sibling Rivalry in Hypoxic Tumour Growth and Progression. Nat. Rev. Cancer 2011, 12, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Fanale, D.; Bazan, V.; Caruso, S.; Castiglia, M.; Bronte, G.; Rolfo, C.; Cicero, G.; Russo, A. Hypoxia and Human Genome Stability: Downregulation of BRCA2 Expression in Breast Cancer Cell Lines. BioMed Res. Int. 2013, 2013, 746858. [Google Scholar] [CrossRef]
- Gläsker, S.; Neumann, H.P.H.; Koch, C.A.; Vortmeyer, A. Von Hippel-Lindau Disease. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Chen, Y.; Gaber, T. Hypoxia/HIF Modulates Immune Responses. Biomedicines 2021, 9, 260. [Google Scholar] [CrossRef]
- Lee, J.H.; Elly, C.; Park, Y.; Liu, Y.-C. E3 Ubiquitin Ligase VHL Regulates Hypoxia-Inducible Factor-1α to Maintain Regulatory T Cell Stability and Suppressive Capacity. Immunity 2015, 42, 1062–1074. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Shim, B.Y.; Lee, S.-J.; Lee, J.Y.; Lee, H.-J.; Kim, I.-H. Loss of Von Hippel–Lindau (VHL) Tumor Suppressor Gene Function: VHL–HIF Pathway and Advances in Treatments for Metastatic Renal Cell Carcinoma (RCC). Int. J. Mol. Sci. 2021, 22, 9795. [Google Scholar] [CrossRef]
- Zhang, J.; Yan, A.; Cao, W.; Shi, H.; Cao, K.; Liu, X. Development and Validation of a VHL-Associated Immune Prognostic Signature for Clear Cell Renal Cell Carcinoma. Cancer Cell Int. 2020, 20, 584. [Google Scholar] [CrossRef]
- Jonasch, E.; Donskov, F.; Iliopoulos, O.; Rathmell, W.K.; Narayan, V.K.; Maughan, B.L.; Oudard, S.; Else, T.; Maranchie, J.K.; Welsh, S.J.; et al. Belzutifan for Renal Cell Carcinoma in von Hippel–Lindau Disease. N. Engl. J. Med. 2021, 385, 2036–2046. [Google Scholar] [CrossRef]
- Jonasch, E.; McCutcheon, I.E.; Gombos, D.S.; Ahrar, K.; Perrier, N.D.; Liu, D.; Robichaux, C.C.; Villarreal, M.F.; Weldon, J.A.; Woodson, A.H.; et al. Pazopanib in Patients with von Hippel-Lindau Disease: A Single-Arm, Single-Centre, Phase 2 Trial. Lancet Oncol. 2018, 19, 1351–1359. [Google Scholar] [CrossRef]
- Klingler, J.-H.; Gläsker, S.; Bausch, B.; Urbach, H.; Krauss, T.; Jilg, C.A.; Steiert, C.; Puzik, A.; Neumann-Haefelin, E.; Kotsis, F.; et al. Hemangioblastoma and von Hippel-Lindau Disease: Genetic Background, Spectrum of Disease, and Neurosurgical Treatment. Childs Nerv. Syst. 2020, 36, 2537–2552. [Google Scholar] [CrossRef]
- Pavesi, G.; Feletti, A.; Berlucchi, S.; Opocher, G.; Martella, M.; Murgia, A.; Scienza, R. Neurosurgical Treatment of von Hippel-Lindau-Associated Hemangioblastomas: Benefits, Risks and Outcome. J. Neurosurg. Sci. 2008, 52, 29–36. [Google Scholar] [PubMed]
- Miyagami, M.; Katayama, Y.; Nakamura, S. Clinicopathological Study of Vascular Endothelial Growth Factor (VEGF), P53, and Proliferative Potential in Familial von Hippel-Lindau Disease and Sporadic Hemangioblastomas. Brain Tumor Pathol. 2000, 17, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Wanebo, J.E.; Lonser, R.R.; Glenn, G.M.; Oldfield, E.H. The Natural History of Hemangioblastomas of the Central Nervous System in Patients with von Hippel-Lindau Disease. J. Neurosurg. 2003, 98, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Harati, A.; Satopää, J.; Mahler, L.; Billon-Grand, R.; Elsharkawy, A.; Niemelä, M.; Hernesniemi, J. Early Microsurgical Treatment for Spinal Hemangioblastomas Improves Outcome in Patients with von Hippel-Lindau Disease. Surg. Neurol. Int. 2012, 3, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siller, S.; Szelényi, A.; Herlitz, L.; Tonn, J.C.; Zausinger, S. Spinal Cord Hemangioblastomas: Significance of Intraoperative Neurophysiological Monitoring for Resection and Long-Term Outcome. J. Neurosurg. Spine 2017, 26, 483–493. [Google Scholar] [CrossRef] [Green Version]
- Ammerman, J.M.; Lonser, R.R.; Dambrosia, J.; Butman, J.A.; Oldfield, E.H. Long-Term Natural History of Hemangioblastomas in Patients with von Hippel-Lindau Disease: Implications for Treatment. J. Neurosurg. 2006, 105, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Louise, M.; Binderup, M.; Smerdel, M.; Borgwadt, L.; Beck Nielsen, S.S.; Madsen, M.G.; Møller, H.U.; Kiilgaard, J.F.; Friis-Hansen, L.; Harbud, V.; et al. Von Hippel-Lindau Disease: Updated Guideline for Diagnosis and Surveillance. Eur. J. Med. Genet. 2022, 65, 104538. [Google Scholar] [CrossRef]
- Peyssonnaux, C.; Cejudo-Martin, P.; Doedens, A.; Zinkernagel, A.S.; Johnson, R.S.; Nizet, V. Cutting Edge: Essential Role of Hypoxia Inducible Factor-1alpha in Development of Lipopolysaccharide-Induced Sepsis. J. Immunol. 2007, 178, 7516–7519. [Google Scholar] [CrossRef] [Green Version]
- Thiel, M.; Caldwell, C.C.; Kreth, S.; Kuboki, S.; Chen, P.; Smith, P.; Ohta, A.; Lentsch, A.B.; Lukashev, D.; Sitkovsky, M.V. Targeted Deletion of HIF-1alpha Gene in T Cells Prevents Their Inhibition in Hypoxic Inflamed Tissues and Improves Septic Mice Survival. PloS ONE 2007, 2, e853. [Google Scholar] [CrossRef] [Green Version]
- Cramer, T.; Yamanishi, Y.; Clausen, B.E.; Förster, I.; Pawlinski, R.; Mackman, N.; Haase, V.H.; Jaenisch, R.; Corr, M.; Nizet, V.; et al. HIF-1alpha Is Essential for Myeloid Cell-Mediated Inflammation. Cell 2003, 112, 645–657. [Google Scholar] [CrossRef] [Green Version]
- Weidemann, A.; Kerdiles, Y.M.; Knaup, K.X.; Rafie, C.A.; Boutin, A.T.; Stockmann, C.; Takeda, N.; Scadeng, M.; Shih, A.Y.; Haase, V.H.; et al. The Glial Cell Response Is an Essential Component of Hypoxia-Induced Erythropoiesis in Mice. J. Clin. Investig. 2009, 119, 3373–3383. [Google Scholar] [CrossRef]
- Tenner, S.; Roston, A.; Lichtenstein, D.; Sica, G.; Carr-Locke, D.; Banks, P.A. Von Hippel-Lindau Disease Complicated by Acute Pancreatitis and Evan’s Syndrome. Int. J. Pancreatol. 1995, 18, 271–275. [Google Scholar] [CrossRef]
- Nath, S.R.; Grewal, P.; Cho, T.; Mao-Draayer, Y. Familial Multiple Sclerosis in Patients with Von Hippel-Lindau Disease. BMC Neurol. 2022, 22, 80. [Google Scholar] [CrossRef]
- Le Moan, N.; Baeten, K.M.; Rafalski, V.A.; Kyu Ryu, J.; Rios Coronado, P.E.; Bedard, C.; Syme, C.; Davalos, D.; Akassoglou, K. Hypoxia Inducible Factor-1α in Astrocytes and/or Myeloid Cells Is Not Required for the Development of Autoimmune Demyelinating Disease. eNeuro 2015, 2. [Google Scholar] [CrossRef]
- Ding, X.; Jo, J.; Wang, C.-Y.; Cristobal, C.D.; Zuo, Z.; Ye, Q.; Wirianto, M.; Lindeke-Myers, A.; Choi, J.M.; Mohila, C.A.; et al. The Daam2-VHL-Nedd4 Axis Governs Developmental and Regenerative Oligodendrocyte Differentiation. Genes Dev. 2020, 34, 1177–1189. [Google Scholar] [CrossRef]
- Wheeler, M.A.; Clark, I.C.; Tjon, E.C.; Li, Z.; Zandee, S.E.J.; Couturier, C.P.; Watson, B.R.; Scalisi, G.; Alkwai, S.; Rothhammer, V.; et al. MAFG-Driven Astrocytes Promote CNS Inflammation. Nature 2020, 578, 593–599. [Google Scholar] [CrossRef]
- Hedegaard Jensen, G.; Mortensen, M.B.; Klöppel, G.; Nielsen, M.F.B.; Nielsen, O.; Detlefsen, S. Utility of PVHL, Maspin, IMP3, S100P and Ki67 in the Distinction of Autoimmune Pancreatitis from Pancreatic Ductal Adenocarcinoma. Pathol. Res. Pract. 2020, 216, 152925. [Google Scholar] [CrossRef]
- Aki, D.; Li, Q.; Li, H.; Liu, Y.-C.; Lee, J.H. Immune Regulation by Protein Ubiquitination: Roles of the E3 Ligases VHL and Itch. Protein Cell 2019, 10, 395–404. [Google Scholar] [CrossRef]
- Cho, S.H.; Raybuck, A.L.; Stengel, K.; Wei, M.; Beck, T.C.; Volanakis, E.; Thomas, J.W.; Hiebert, S.; Haase, V.H.; Boothby, M.R. Germinal Centre Hypoxia and Regulation of Antibody Qualities by a Hypoxia Response System. Nature 2016, 537, 234–238. [Google Scholar] [CrossRef] [Green Version]
- Jellusova, J.; Cato, M.H.; Apgar, J.R.; Ramezani-Rad, P.; Leung, C.R.; Chen, C.; Richardson, A.D.; Conner, E.M.; Benschop, R.J.; Woodgett, J.R.; et al. Gsk3 Is a Metabolic Checkpoint Regulator in B Cells. Nat. Immunol. 2017, 18, 303–312. [Google Scholar] [CrossRef] [Green Version]
- Abbott, R.K.; Thayer, M.; Labuda, J.; Silva, M.; Philbrook, P.; Cain, D.W.; Kojima, H.; Hatfield, S.; Sethumadhavan, S.; Ohta, A.; et al. Germinal Center Hypoxia Potentiates Immunoglobulin Class Switch Recombination. J. Immunol. 2016, 197, 4014–4020. [Google Scholar] [CrossRef] [PubMed]
- Rius, J.; Guma, M.; Schachtrup, C.; Akassoglou, K.; Zinkernagel, A.S.; Nizet, V.; Johnson, R.S.; Haddad, G.G.; Karin, M. NF-KappaB Links Innate Immunity to the Hypoxic Response through Transcriptional Regulation of HIF-1alpha. Nature 2008, 453, 807–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palazon, A.; Goldrath, A.W.; Nizet, V.; Johnson, R.S. HIF Transcription Factors, Inflammation, and Immunity. Immunity 2014, 41, 518–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corzo, C.A.; Condamine, T.; Lu, L.; Cotter, M.J.; Youn, J.-I.; Cheng, P.; Cho, H.-I.; Celis, E.; Quiceno, D.G.; Padhya, T.; et al. HIF-1α Regulates Function and Differentiation of Myeloid-Derived Suppressor Cells in the Tumor Microenvironment. J. Exp. Med. 2010, 207, 2439–2453. [Google Scholar] [CrossRef] [PubMed]
- Walmsley, S.R.; Print, C.; Farahi, N.; Peyssonnaux, C.; Johnson, R.S.; Cramer, T.; Sobolewski, A.; Condliffe, A.M.; Cowburn, A.S.; Johnson, N.; et al. Hypoxia-Induced Neutrophil Survival Is Mediated by HIF-1alpha-Dependent NF-KappaB Activity. J. Exp. Med. 2005, 201, 105–115. [Google Scholar] [CrossRef] [Green Version]
- Izquierdo, H.M.; Brandi, P.; Gómez, M.-J.; Conde-Garrosa, R.; Priego, E.; Enamorado, M.; Martínez-Cano, S.; Sánchez, I.; Conejero, L.; Jimenez-Carretero, D.; et al. Von Hippel-Lindau Protein Is Required for Optimal Alveolar Macrophage Terminal Differentiation, Self-Renewal, and Function. Cell Rep. 2018, 24, 1738–1746. [Google Scholar] [CrossRef] [Green Version]
- Doedens, A.L.; Stockmann, C.; Rubinstein, M.P.; Liao, D.; Zhang, N.; DeNardo, D.G.; Coussens, L.M.; Karin, M.; Goldrath, A.W.; Johnson, R.S. Macrophage Expression of HIF-1α Suppresses T Cell Function and Promotes Tumor Progression. Cancer Res. 2010, 70, 7465–7475. [Google Scholar] [CrossRef] [Green Version]
- Ebbo, M.; Crinier, A.; Vély, F.; Vivier, E. Innate Lymphoid Cells: Major Players in Inflammatory Diseases. Nat. Rev. Immunol. 2017, 17, 665–678. [Google Scholar] [CrossRef]
- Li, Q.; Li, D.; Zhang, X.; Wan, Q.; Zhang, W.; Zheng, M.; Zou, L.; Elly, C.; Lee, J.H.; Liu, Y.-C. E3 Ligase VHL Promotes Group 2 Innate Lymphoid Cell Maturation and Function via Glycolysis Inhibition and Induction of Interleukin-33 Receptor. Immunity 2018, 48, 258–270.e5. [Google Scholar] [CrossRef] [Green Version]
- Doedens, A.L.; Phan, A.T.; Stradner, M.H.; Fujimoto, J.K.; Nguyen, J.V.; Yang, E.; Johnson, R.S.; Goldrath, A.W. Hypoxia-Inducible Factors Enhance the Effector Responses of CD8(+) T Cells to Persistent Antigen. Nat. Immunol. 2013, 14, 1173–1182. [Google Scholar] [CrossRef] [Green Version]
- Phan, A.T.; Doedens, A.L.; Palazon, A.; Tyrakis, P.A.; Cheung, K.P.; Johnson, R.S.; Goldrath, A.W. Constitutive Glycolytic Metabolism Supports CD8+ T Cell Effector Memory Differentiation during Viral Infection. Immunity 2016, 45, 1024–1037. [Google Scholar] [CrossRef]
- Eliasson, P.; Jönsson, J.-I. The Hematopoietic Stem Cell Niche: Low in Oxygen but a Nice Place to Be. J. Cell. Physiol. 2010, 222, 17–22. [Google Scholar] [CrossRef]
- Kojima, H.; Gu, H.; Nomura, S.; Caldwell, C.C.; Kobata, T.; Carmeliet, P.; Semenza, G.L.; Sitkovsky, M.V. Abnormal B Lymphocyte Development and Autoimmunity in Hypoxia-Inducible Factor 1α-Deficient Chimeric Mice. Proc. Natl. Acad. Sci. USA 2002, 99, 2170–2174. [Google Scholar] [CrossRef] [Green Version]
- Hale, L.P.; Braun, R.D.; Gwinn, W.M.; Greer, P.K.; Dewhirst, M.W. Hypoxia in the Thymus: Role of Oxygen Tension in Thymocyte Survival. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H1467–H1477. [Google Scholar] [CrossRef] [Green Version]
- Biju, M.P.; Neumann, A.K.; Bensinger, S.J.; Johnson, R.S.; Turka, L.A.; Haase, V.H. Vhlh Gene Deletion Induces Hif-1-Mediated Cell Death in Thymocytes. Mol. Cell. Biol. 2004, 24, 9038–9047. [Google Scholar] [CrossRef] [Green Version]
- Neumann, A.K.; Yang, J.; Biju, M.P.; Joseph, S.K.; Johnson, R.S.; Haase, V.H.; Freedman, B.D.; Turka, L.A. Hypoxia Inducible Factor 1α Regulates T Cell Receptor Signal Transduction. Proc. Natl. Acad. Sci. USA 2005, 102, 17071–17076. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Perea, A.L.; Arcia, E.D.; Rueda, C.M.; Velilla, P.A. Phenotypical Characterization of Regulatory T Cells in Humans and Rodents. Clin. Exp. Immunol. 2016, 185, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Tsuji-Takayama, K.; Suzuki, M.; Yamamoto, M.; Harashima, A.; Okochi, A.; Otani, T.; Inoue, T.; Sugimoto, A.; Toraya, T.; Takeuchi, M.; et al. The Production of IL-10 by Human Regulatory T Cells Is Enhanced by IL-2 through a STAT5-Responsive Intronic Enhancer in the IL-10 Locus. J. Immunol. 2008, 181, 3897–3905. [Google Scholar] [CrossRef] [Green Version]
- Overacre-Delgoffe, A.E.; Chikina, M.; Dadey, R.E.; Yano, H.; Brunazzi, E.A.; Shayan, G.; Horne, W.; Moskovitz, J.M.; Kolls, J.K.; Sander, C.; et al. Interferon-γ Drives Treg Fragility to Promote Anti-Tumor Immunity. Cell 2017, 169, 1130–1141.e11. [Google Scholar] [CrossRef] [Green Version]
- Bettelli, E.; Carrier, Y.; Gao, W.; Korn, T.; Strom, T.B.; Oukka, M.; Weiner, H.L.; Kuchroo, V.K. Reciprocal Developmental Pathways for the Generation of Pathogenic Effector TH17 and Regulatory T Cells. Nature 2006, 441, 235–238. [Google Scholar] [CrossRef]
- Veldhoen, M.; Hocking, R.J.; Atkins, C.J.; Locksley, R.M.; Stockinger, B. TGFbeta in the Context of an Inflammatory Cytokine Milieu Supports de Novo Differentiation of IL-17-Producing T Cells. Immunity 2006, 24, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Dang, E.V.; Barbi, J.; Yang, H.-Y.; Jinasena, D.; Yu, H.; Zheng, Y.; Bordman, Z.; Fu, J.; Kim, Y.; Yen, H.-R.; et al. Control of T(H)17/T(Reg) Balance by Hypoxia-Inducible Factor 1. Cell 2011, 146, 772–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivanov, I.I.; McKenzie, B.S.; Zhou, L.; Tadokoro, C.E.; Lepelley, A.; Lafaille, J.J.; Cua, D.J.; Littman, D.R. The Orphan Nuclear Receptor RORgammat Directs the Differentiation Program of Proinflammatory IL-17+ T Helper Cells. Cell 2006, 126, 1121–1133. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.O.; Panopoulos, A.D.; Nurieva, R.; Chang, S.H.; Wang, D.; Watowich, S.S.; Dong, C. STAT3 Regulates Cytokine-Mediated Generation of Inflammatory Helper T Cells. J. Biol. Chem. 2007, 282, 9358–9363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peck, A.; Mellins, E.D. Precarious Balance: Th17 Cells in Host Defense. Infect. Immun. 2010, 78, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Dong, C. Genetic Controls of Th17 Cell Differentiation and Plasticity. Exp. Mol. Med. 2011, 43, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Patel, D.D.; Kuchroo, V.K. Th17 Cell Pathway in Human Immunity: Lessons from Genetics and Therapeutic Interventions. Immunity 2015, 43, 1040–1051. [Google Scholar] [CrossRef] [Green Version]
- Burkett, P.R.; Meyer zu Horste, G.; Kuchroo, V.K. Pouring Fuel on the Fire: Th17 Cells, the Environment, and Autoimmunity. J. Clin. Investig. 2015, 125, 2211–2219. [Google Scholar] [CrossRef]
- Liang, S.C.; Tan, X.-Y.; Luxenberg, D.P.; Karim, R.; Dunussi-Joannopoulos, K.; Collins, M.; Fouser, L.A. Interleukin (IL)-22 and IL-17 Are Coexpressed by Th17 Cells and Cooperatively Enhance Expression of Antimicrobial Peptides. J. Exp. Med. 2006, 203, 2271–2279. [Google Scholar] [CrossRef] [Green Version]
- Ishigame, H.; Kakuta, S.; Nagai, T.; Kadoki, M.; Nambu, A.; Komiyama, Y.; Fujikado, N.; Tanahashi, Y.; Akitsu, A.; Kotaki, H.; et al. Differential Roles of Interleukin-17A and -17F in Host Defense against Mucoepithelial Bacterial Infection and Allergic Responses. Immunity 2009, 30, 108–119. [Google Scholar] [CrossRef] [Green Version]
- El-Behi, M.; Ciric, B.; Dai, H.; Yan, Y.; Cullimore, M.; Safavi, F.; Zhang, G.-X.; Dittel, B.N.; Rostami, A. The Encephalitogenicity of T(H)17 Cells Is Dependent on IL-1- and IL-23-Induced Production of the Cytokine GM-CSF. Nat. Immunol. 2011, 12, 568–575. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, W.; Zenewicz, L.A.; Flavell, R.A. The Dual Nature of T(H)17 Cells: Shifting the Focus to Function. Nat. Immunol. 2010, 11, 471–476. [Google Scholar] [CrossRef] [PubMed]
- McGeachy, M.J.; Cua, D.J.; Gaffen, S.L. The IL-17 Family of Cytokines in Health and Disease. Immunity 2019, 50, 892–906. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.Z.; Wang, R.; Huang, G.; Vogel, P.; Neale, G.; Green, D.R.; Chi, H. HIF1alpha-Dependent Glycolytic Pathway Orchestrates a Metabolic Checkpoint for the Differentiation of TH17 and Treg Cells. J. Exp. Med. 2011, 208, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chitrakar, A.; Budda, S.A.; Henderson, J.G.; Axtell, R.C.; Zenewicz, L.A. E3 Ubiquitin Ligase Von Hippel–Lindau Protein Promotes Th17 Differentiation. J. Immunol. 2020, 205, 1009–1023. [Google Scholar] [CrossRef]
- Gilhus, N.E. Myasthenia Gravis. N. Engl. J. Med. 2016, 375, 2570–2581. [Google Scholar] [CrossRef]
- Gilhus, N.E.; Tzartos, S.; Evoli, A.; Palace, J.; Burns, T.M.; Verschuuren, J.J.G.M. Myasthenia Gravis. Nat. Rev. Dis. Primers 2019, 5, 30. [Google Scholar] [CrossRef]
- Dalakas, M.C. Immunotherapy in Myasthenia Gravis in the Era of Biologics. Nat. Rev. Neurol. 2019, 15, 113–124. [Google Scholar] [CrossRef]
- Lazaridis, K.; Tzartos, S.J. Autoantibody Specificities in Myasthenia Gravis; Implications for Improved Diagnostics and Therapeutics. Front. Immunol. 2020, 11, 212. [Google Scholar] [CrossRef] [Green Version]
- Sheth, M.N.; Nations, S.P.; Wolfe, G.I.; Trivedi, J.R. Von Hippel-Lindau Disease Associated With Thymoma and Myasthenia Gravis. J. Clin. Neuromuscul. Dis. 2005, 7, 59–61. [Google Scholar] [CrossRef]
- Pozzato, P.; Sorrenti, G.; Salvi, F.; Ventrucci, M. Un caso di malattia di von Hippel-Lindau associata a miastenia gravis non correlata alla presenza di timoma Von Hippel-Lindau disease associated with myasthenia gravis not related to thymoma. Ital. J. Med. 2009, 3, 3. [Google Scholar]
- Yi, J.S.; Guptill, J.T.; Stathopoulos, P.; Nowak, R.J.; O’Connor, K.C. B Cells in the Pathophysiology of Myasthenia Gravis. Muscle Nerve 2018, 57, 172–184. [Google Scholar] [CrossRef]
- Ströbel, P.; Moritz, R.; Leite, M.I.; Willcox, N.; Chuang, W.-Y.; Gold, R.; Nix, W.; Schalke, B.; Kiefer, R.; Müller-Hermelink, H.-K.; et al. The Ageing and Myasthenic Thymus: A Morphometric Study Validating a Standard Procedure in the Histological Workup of Thymic Specimens. J. Neuroimmunol. 2008, 201, 64–73. [Google Scholar] [CrossRef]
- Le Panse, R.; Cizeron-Clairac, G.; Cuvelier, M.; Truffault, F.; Bismuth, J.; Nancy, P.; De Rosbo, N.K.; Berrih-Aknin, S. Regulatory and Pathogenic Mechanisms in Human Autoimmune Myasthenia Gravis. Ann. N. Y. Acad. Sci. 2008, 1132, 135–142. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, Y.; Gu, W.; He, L.; Sun, B. Th1/Th2 Cell’s Function in Immune System. Adv. Exp. Med. Biol. 2014, 841, 45–65. [Google Scholar] [CrossRef]
- Schaffert, H.; Pelz, A.; Saxena, A.; Losen, M.; Meisel, A.; Thiel, A.; Kohler, S. IL-17-Producing CD4(+) T Cells Contribute to the Loss of B-Cell Tolerance in Experimental Autoimmune Myasthenia Gravis. Eur. J. Immunol. 2015, 45, 1339–1347. [Google Scholar] [CrossRef]
- Aguilo-Seara, G.; Xie, Y.; Sheehan, J.; Kusner, L.L.; Kaminski, H.J. Ablation of IL-17 Expression Moderates Experimental Autoimmune Myasthenia Gravis Disease Severity. Cytokine 2017, 96, 279–285. [Google Scholar] [CrossRef]
- Masuda, M.; Matsumoto, M.; Tanaka, S.; Nakajima, K.; Yamada, N.; Ido, N.; Ohtsuka, T.; Nishida, M.; Hirano, T.; Utsumi, H. Clinical Implication of Peripheral CD4+CD25+ Regulatory T Cells and Th17 Cells in Myasthenia Gravis Patients. J. Neuroimmunol. 2010, 225, 123–131. [Google Scholar] [CrossRef]
- Roche, J.C.; Capablo, J.L.; Larrad, L.; Gervas-Arruga, J.; Ara, J.R.; Sánchez, A.; Alarcia, R. Increased Serum Interleukin-17 Levels in Patients with Myasthenia Gravis. Muscle Nerve 2011, 44, 278–280. [Google Scholar] [CrossRef]
- Xu, W.-H.; Zhang, A.-M.; Ren, M.-S.; Zhang, X.-D.; Wang, F.; Xu, X.-C.; Li, Q.; Wang, J.; Din, B.-S.; Wu, Y.-B.; et al. Changes of Treg-Associated Molecules on CD4+CD25 +Treg Cells in Myasthenia Gravis and Effects of Immunosuppressants. J. Clin. Immunol. 2012, 32, 975–983. [Google Scholar] [CrossRef]
- Hu, Y.; Wang, J.; Rao, J.; Xu, X.; Cheng, Y.; Yan, L.; Wu, Y.; Wu, N.; Wu, X. Comparison of Peripheral Blood B Cell Subset Ratios and B Cell-Related Cytokine Levels between Ocular and Generalized Myasthenia Gravis. Int. Immunopharmacol. 2020, 80, 106130. [Google Scholar] [CrossRef] [PubMed]
- Thiruppathi, M.; Rowin, J.; Ganesh, B.; Sheng, J.R.; Prabhakar, B.S.; Meriggioli, M.N. Impaired Regulatory Function in Circulating CD4(+)CD25(High)CD127(Low/−) T Cells in Patients with Myasthenia Gravis. Clin. Immunol. 2012, 145, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Balandina, A.; Lécart, S.; Dartevelle, P.; Saoudi, A.; Berrih-Aknin, S. Functional Defect of Regulatory CD4(+)CD25+ T Cells in the Thymus of Patients with Autoimmune Myasthenia Gravis. Blood 2005, 105, 735–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Chen, Y.; Jia, G.; Chen, X.; Lu, J.; Yang, H.; Zhou, W.; Xiao, B.; Zhang, N.; Li, J. FOXP3 -3279 and IVS9+459 Polymorphisms Are Associated with Genetic Susceptibility to Myasthenia Gravis. Neurosci. Lett. 2013, 534, 274–278. [Google Scholar] [CrossRef]
- Huang, S.; Wang, W.; Chi, L. Feasibility of Up-Regulating CD4(+)CD25(+) Tregs by IFN-γ in Myasthenia Gravis Patients. BMC Neurol. 2015, 15, 163. [Google Scholar] [CrossRef] [Green Version]
- Baecher-Allan, C.; Brown, J.A.; Freeman, G.J.; Hafler, D.A. CD4+CD25high Regulatory Cells in Human Peripheral Blood. J. Immunol. 2001, 167, 1245–1253. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Case Report | Sex, Age (y) VHL Mutation | VHL-Related Tumors | MG Symptoms/Signs |
| Thymic Disease (Histological Diagnosis) |
|---|---|---|---|---|---|
| Sheth et al., 2005 [82] | M, 47 - | Cerebellar hemangioblastoma Retinal angioma Renal cysts RCC | Right ptosis, binocular diplopia Dysarthria, dysphagia, exertional dyspnea, mild facial weakness Proximal lower extremity bilateral weakness |
| Thymoma |
| Pozzato et al., 2009 [83] | F, 60 New VHL mutation (c279delC) + polymorphism c291C > G | Cerebellar hemangioblastoma Pancreatic cyst RCC | Left ptosis, binocular diplopia Dysarthria Bilateral upper and lower limbs weakness |
| - |
| Present case 1 | F, 17 Paternal VHL mutation | Spinal hemangioblastoma | Left ptosis, binocular diplopia Sporadic dysarthria |
| Thymic hyperplasia |
| Present case 2 | M, 51 | Cerebellar hemangioblastoma | Binocular diplopia Sporadic dysphagia Lower limbs weakness |
| - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Norata, D.; Peri, M.; Giammalva, G.R.; Lupica, A.; Paolini, F.; Incorvaia, L.; Badalamenti, G.; Gristina, V.; Galvano, A.; Russo, A.; et al. Immunological Aspects of Von Hippel-Lindau Disease: A Focus on Neuro-Oncology and Myasthenia Gravis. Diagnostics 2023, 13, 144. https://doi.org/10.3390/diagnostics13010144
Norata D, Peri M, Giammalva GR, Lupica A, Paolini F, Incorvaia L, Badalamenti G, Gristina V, Galvano A, Russo A, et al. Immunological Aspects of Von Hippel-Lindau Disease: A Focus on Neuro-Oncology and Myasthenia Gravis. Diagnostics. 2023; 13(1):144. https://doi.org/10.3390/diagnostics13010144
Chicago/Turabian StyleNorata, Davide, Marta Peri, Giuseppe Roberto Giammalva, Antonino Lupica, Federica Paolini, Lorena Incorvaia, Giuseppe Badalamenti, Valerio Gristina, Antonio Galvano, Antonio Russo, and et al. 2023. "Immunological Aspects of Von Hippel-Lindau Disease: A Focus on Neuro-Oncology and Myasthenia Gravis" Diagnostics 13, no. 1: 144. https://doi.org/10.3390/diagnostics13010144